Essential Oils as Alternatives for Root-Canal Treatment and Infection Control against Enterococcus faecalis—A Preliminary Study


 ,
,  ,
,  ,
,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Essential Oils, Working Solutions and Bacterial Strains
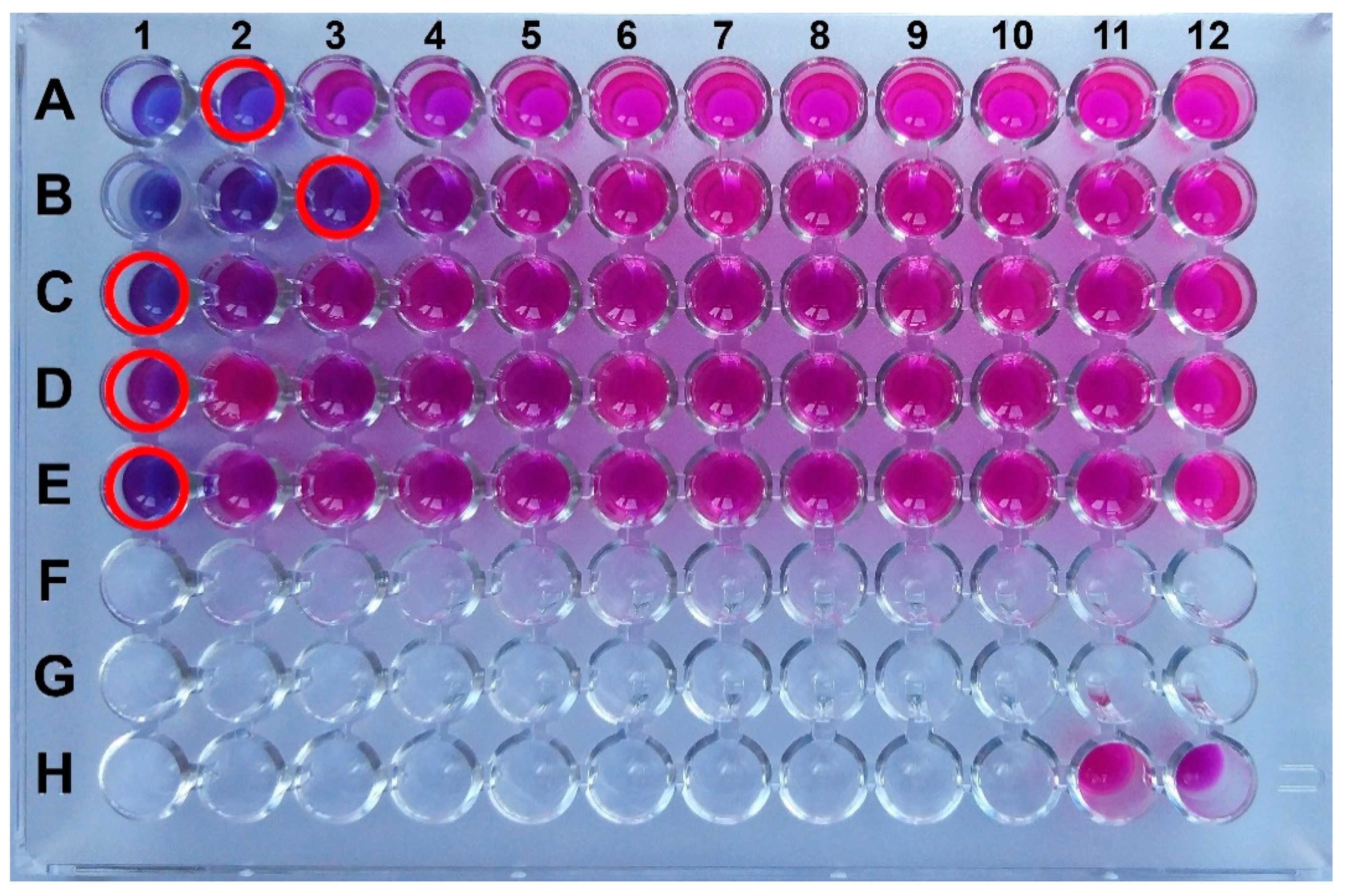
2.2. In Vitro Antibacterial Effects of Aqueous Extracts of Essential Oil (AqEO)
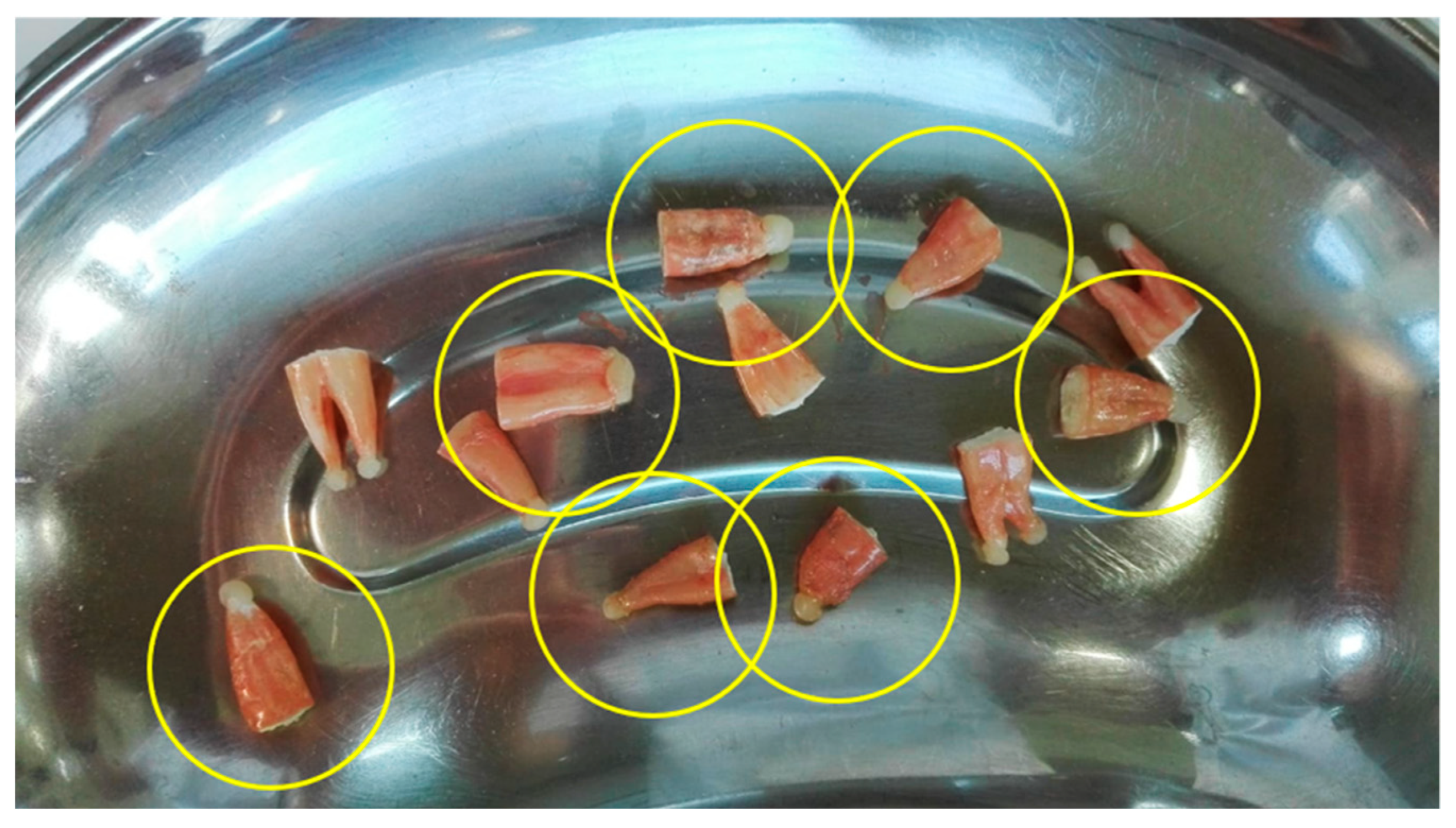
2.3. Collection and Preparation of Samples
2.4. Infection of Root Canal
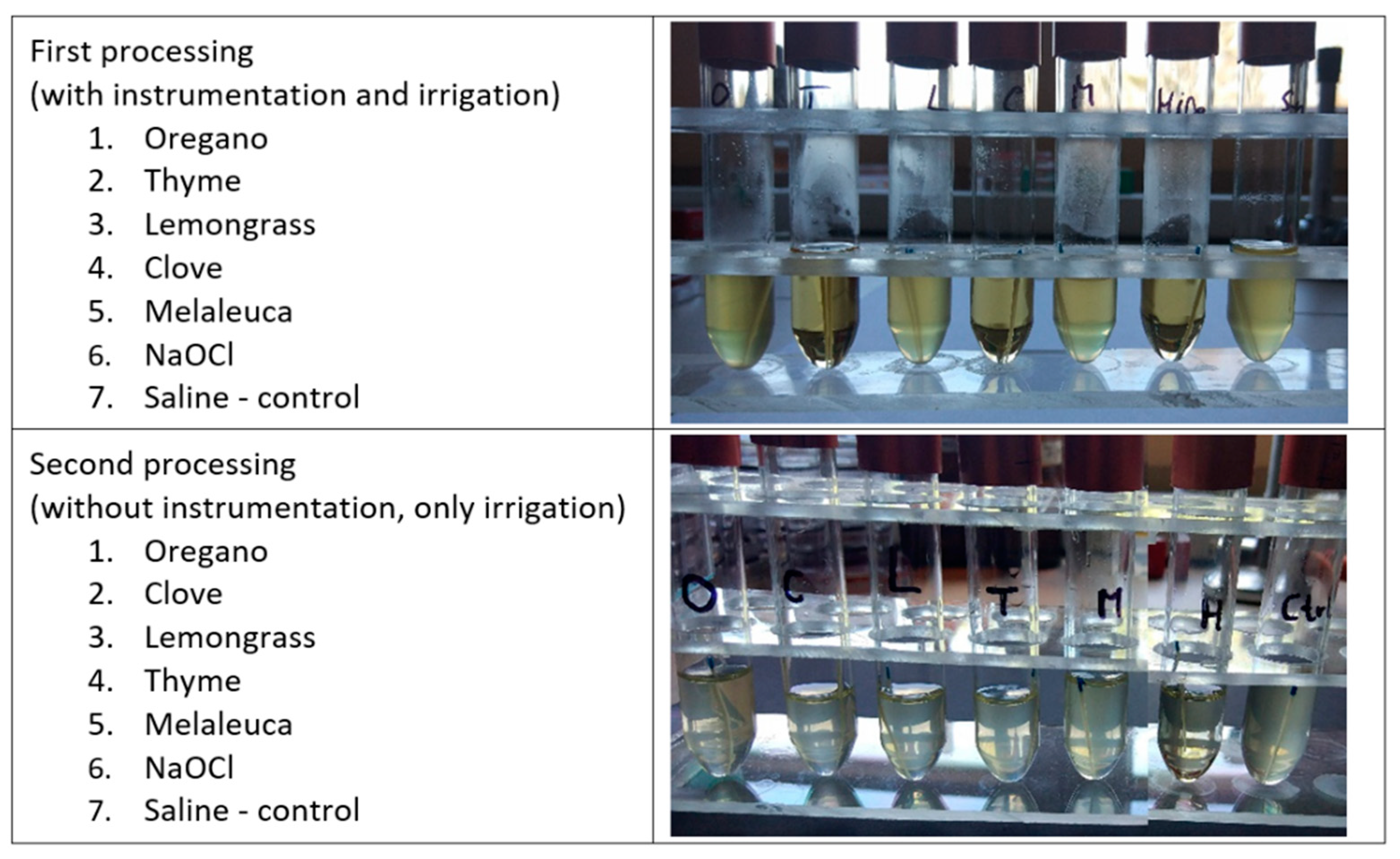
2.5. First Processing and Bacteriological Analysis of Infected Teeth
2.6. Second Processing and Bacteriological Analysis of Infected Teeth
3. Results
3.1. In Vitro Antibacterial Effects of AqEO
3.2. Processing and Bacteriological Analysis of Infected Teeth
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Narayanan, L.L.; Vaishnavi, C. Endodontic Microbiology. J. Conserv. Dent. 2010, 13, 233–239. [Google Scholar] [CrossRef]
- Siqueira, J. Microbiology of Apical Periodontitis. In Essential Endodontology: Prevention and Treatment of Aprical Periodnotitis; Orstavik, D., Ed.; Wiley Blackwell: Hoboken, NJ, USA, 2008; pp. 135–139. [Google Scholar]
- Kakehashi, S.; Stanley, H.R.; Fitzgerald, R.J. The Effects of Surgical Exposures of Dental Pulps in Germ-Free and Conventional Laboratory Rats. Oral Surg. Oral Med. Oral Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef]
- Bammann, L.; Estrela, C. Microbiological Aspects in Endodontics: Endodontic Science. Sci. Open 2009, 1, 258–281. [Google Scholar]
- Siqueira, J.F.; Rôças, I.N. Diversity of Endodontic Microbiota Revisited. J. Dent. Res. 2009, 88, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Singh, H. Microbiology of Endodontic Infections. J. Dent. Oral Health 2016, 2, 1–4. [Google Scholar]
- Alghamdi, F.; Shakir, M. The Influence of Enterococcus faecalis as a Dental Root Canal Pathogen on Endodontic Treatment: A Systematic Review. Cureus 2020, 12, e7257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuart, C.H.; Schwartz, S.A.; Beeson, T.J.; Owatz, C.B. Enterococcus faecalis: Its Role in Root Canal Treatment Failure and Current Concepts in Retreatment. J. Endod. 2006, 32, 93–98. [Google Scholar] [CrossRef]
- Borzini, L.; Condò, R.; De Dominicis, P.; Casaglia, A.; Cerroni, L. Root Canal Irrigation: Chemical Agents and Plant Extracts Against Enterococcus faecalis. Open Dent. J. 2016, 10, 692–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicham, B.; Seridi, R. Antimicrobial Efficacy of the Essential Oil of Origanum vulgare from Algeria. J. Pharm. Pharmacol. Res. 2017, 1, 19–27. [Google Scholar]
- Leyva-López, N.; Gutiérrez-Grijalva, E.P.; Vazquez-Olivo, G.; Heredia, J.B. Essential Oils of Oregano: Biological Activity beyond Their Antimicrobial Properties. Molecules 2017, 22, 989. [Google Scholar] [CrossRef] [Green Version]
- Veenstra, J.P.; Johnson, J.J. Oregano (Origanum vulgare) Extract for Food Preservation and Improvement in Gastrointestinal Health. Int. J. Nutr. 2019, 3, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Anžlovar, S.; Baričevič, D.; Ambrožič Avguštin, J.; Dolenc Koce, J. Essential Oil of Common Thyme as a Natural Antimicrobial Food Additive. Food Technol. Biotechnol. 2014, 52, 263–268. [Google Scholar]
- Nagy-Bota, M.-C.; Man, A.; Della Mare, A.; Zsuzsanna, P.; Halmaciu, I.; Szanto, A.; Brinzaniuc, K. Antibacterial Activity of Five Essential Oils on Representative Bacterial Pathogens. Clujul Med. 2018, 91, 59–64. [Google Scholar]
- Satyal, P.; Murray, B.L.; McFeeters, R.L.; Setzer, W.N. Essential Oil Characterization of Thymus vulgaris from Various Geographical Locations. Foods 2016, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Boukhatem, M.N.; Ferhat, M.A.; Kameli, A.; Saidi, F.; Kebir, H.T. Lemon Grass (Cymbopogon citratus) Essential Oil as a Potent Anti-Inflammatory and Antifungal Drugs. Libyan J. Med. 2014, 9. [Google Scholar] [CrossRef]
- Adukwu, E.C.; Bowles, M.; Edwards-Jones, V.; Bone, H. Antimicrobial Activity, Cytotoxicity and Chemical Analysis of Lemongrass Essential Oil (Cymbopogon flexuosus) and Pure Citral. Appl. Microbiol. Biotechnol. 2016, 100, 9619–9627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnke, P.H.; Becker, S.T.; Podschun, R.; Sivananthan, S.; Springer, I.N.; Russo, P.A.J.; Wiltfang, J.; Fickenscher, H.; Sherry, E. The Battle against Multi-Resistant Strains: Renaissance of Antimicrobial Essential Oils as a Promising Force to Fight Hospital-Acquired Infections. J. Cranio Maxillofac. Surg. 2009, 37, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Adukwu, E.C.; Allen, S.C.H.; Phillips, C.A. The Anti-Biofilm Activity of Lemongrass (Cymbopogon flexuosus) and Grapefruit (Citrus paradisi) Essential Oils against Five Strains of Staphylococcus aureus. J. Appl. Microbiol. 2012, 113, 1217–1227. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Guo, Y.; Guo, L.; Jiang, H.; Ji, Q. In Vitro Evaluation of Antioxidant and Antimicrobial Activities of Melaleuca alternifolia Essential Oil. BioMed Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Siddique, S.; Perveen, Z.; Nawaz, S.; Shahzad, K.; Ali, Z. Chemical Composition and Antimicrobial Activities of Essential Oils of Six Species from Family Myrtaceae. J. Essent. Oil Bear. Plants 2015, 18, 950–956. [Google Scholar] [CrossRef]
- Felipe, L.D.O.; da Silva, W.F., Jr.; de Araújo, K.C.; Fabrino, D.L. Lactoferrin, Chitosan and Melaleuca alternifolia—Natural Products That Show Promise in Candidiasis Treatment. Braz. J. Microbiol. 2018, 49, 212–219. [Google Scholar] [CrossRef]
- Sharifi-Rad, J.; Salehi, B.; Varoni, E.M.; Sharopov, F.; Yousaf, Z.; Ayatollahi, S.A.; Kobarfard, F.; Sharifi-Rad, M.; Afdjei, M.H.; Sharifi-Rad, M.; et al. Plants of the Melaleuca Genus as Antimicrobial Agents: From Farm to Pharmacy. Phytother. Res. 2017, 31, 1475–1494. [Google Scholar] [CrossRef]
- Li, M.; Zhu, L.; Liu, B.; Du, L.; Jia, X.; Han, L.; Jin, Y. Tea Tree Oil Nanoemulsions for Inhalation Therapies of Bacterial and Fungal Pneumonia. Colloids Surf. B Biointerfaces 2016, 141, 408–416. [Google Scholar] [CrossRef]
- Chaieb, K.; Hajlaoui, H.; Zmantar, T.; Kahla-Nakbi, A.B.; Rouabhia, M.; Mahdouani, K.; Bakhrouf, A. The Chemical Composition and Biological Activity of Clove Essential Oil, Eugenia caryophyllata (Syzigium aromaticum L. Myrtaceae): A Short Review. Phytother. Res. 2007, 21, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.-G.; Liu, T.; Hu, Q.-P.; Cao, X.-M. Chemical Composition, Antibacterial Properties and Mechanism of Action of Essential Oil from Clove Buds against Staphylococcus aureus. Molecules 2016, 21, 1194. [Google Scholar] [CrossRef] [PubMed]
- Vajrabhaya, L.-O.; Sangalungkarn, V.; Srisatjaluk, R.; Korsuwannawong, S.; Phruksaniyom, C. Hypochlorite Solution for Root Canal Irrigation That Lacks a Chlorinated Odor. Eur. J. Dent. 2017, 11, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuruvilla, J.R.; Kamath, M.P. Antimicrobial Activity of 2.5% Sodium Hypochlorite and 0.2% Chlorhexidine Gluconate Separately and Combined, as Endodontic Irrigants. J. Endod. 1998, 24, 472–476. [Google Scholar] [CrossRef]
- Byström, A.; Sundqvist, G. Bacteriologic Evaluation of the Effect of 0.5 Percent Sodium Hypochlorite in Endodontic Therapy. Oral Surg. Oral Med. Oral Pathol. 1983, 55, 307–312. [Google Scholar] [CrossRef]
- Podar, R.; Kulkarni, G.P.; Dadu, S.S.; Singh, S.; Singh, S.H. In Vivo Antimicrobial Efficacy of 6% Morinda citrifolia, Azadirachta indica, and 3% Sodium Hypochlorite as Root Canal Irrigants. Eur. J. Dent. 2015, 9, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Gül, S.; Savsar, A.; Tayfa, Z. Cytotoxic and Genotoxic Effects of Sodium Hypochlorite on Human Peripheral Lymphocytes in Vitro. Cytotechnology 2009, 59, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Venkateshbabu, N.; Anand, S.; Abarajithan, M.; Sheriff, S.O.; Jacob, P.S.; Sonia, N. Natural Therapeutic Options in Endodontics—A Review. Open Dent. J. 2016, 10, 214–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jhajharia, K.; Parolia, A.; Shetty, K.V.; Mehta, L.K. Biofilm in Endodontics: A Review. J. Int. Soc. Prev. Community Dent. 2015, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estrela, C.; Estrela, C.R.; Barbin, E.L.; Spanó, J.C.E.; Marchesan, M.A.; Pécora, J.D. Mechanism of Action of Sodium Hypochlorite. Braz. Dent. J. 2002, 13, 113–117. [Google Scholar] [CrossRef]
- Farreras, D.C.R.; Puente, C.G.; Estrela, C. Sodium Hypochlorite Chemical Burn in an Endodontist’s Eye during Canal Treatment Using Operating Microscope. J. Endod. 2014, 40, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Al-Sebaei, M.O.; Halabi, O.A.; El-Hakim, I.E. Sodium Hypochlorite Accident Resulting in Life-Threatening Airway Obstruction during Root Canal Treatment: A Case Report. Clin. Cosmet. Investig. Dent. 2015, 7, 41–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almadi, E.M.; Almohaimede, A.A. Natural Products in Endodontics. Saudi Med. J. 2018, 39, 124–130. [Google Scholar] [CrossRef]
- de Sermeño, R.F.; da Silva, L.A.B.; Herrera, H.; Herrera, H.; Silva, R.A.B.; Leonardo, M.R. Tissue Damage after Sodium Hypochlorite Extrusion during Root Canal Treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e46–e49. [Google Scholar] [CrossRef]
- Benbelaïd, F.; Khadir, A.; Abdoune, M.A.; Bendahou, M.; Muselli, A.; Costa, J. Antimicrobial Activity of Some Essential Oils against Oral Multidrug-Resistant Enterococcus faecalis in Both Planktonic and Biofilm State. Asian Pac. J. Trop. Biomed. 2014, 4, 463–472. [Google Scholar] [CrossRef] [Green Version]
- Estrela, C.; Silva, J.A.; de Alencar, A.H.G.; Leles, C.R.; Decurcio, D.A. Efficacy of Sodium Hypochlorite and Chlorhexidine against Enterococcus faecalis: A Systematic Review. J. Appl. Oral Sci. 2008, 16, 364–368. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Palazzi, F.; Giardino, L.; Shalavi, S. Microbial Biofilms in Endodontic Infections: An Update Review. Biomed. J. 2013, 36, 59–70. [Google Scholar] [CrossRef]
- Zehnder, M.; Guggenheim, B. The Mysterious Appearance of Enterococci in Filled Root Canals. Int. Endod. J. 2009, 42, 277–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidana, R.; Sullivan, A.; Billström, H.; Ahlquist, M.; Lund, B. Enterococcus faecalis Infection in Root Canals-Host-Derived or Exogenous Source? Lett. Appl. Microbiol. 2011, 52, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Rôças, I.N.; Lima, K.C.; Siqueira, J.F. Reduction in Bacterial Counts in Infected Root Canals after Rotary or Hand Nickel-Titanium Instrumentation—A Clinical Study. Int. Endod. J. 2013, 46, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Amaral, R.R.; Oliveira, A.G.G.; Braga, T.; Reher, P.; de Macedo Farias, L.; Magalhães, P.P.; Ferreira, P.G.; de Souza Côrtes, M.I. Quantitative Assessment of the Efficacy of Two Different Single-File Systems in Reducing the Bacterial Load in Oval-Shaped Canals: A Clinical Study. J. Endod. 2020, 46, 1228–1234. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N.; Santos, S.R.L.D.; Lima, K.C.; Magalhães, F.A.C.; de Uzeda, M. Efficacy of Instrumentation Techniques and Irrigation Regimens in Reducing the Bacterial Population within Root Canals. J. Endod. 2002, 28, 181–184. [Google Scholar] [CrossRef]
- Ok, E.; Adanir, N.; Hakki, S. Comparison of Cytotoxicity of Various Concentrations Origanum Extract Solution with 2% Chlorhexidine Gluconate and 5.25% Sodium Hypochlorite. Eur. J. Dent. 2015, 9, 6–10. [Google Scholar] [CrossRef]
- Ok, E.; Adanir, N.; Ozturk, T. Antibacterial and Smear Layer Removal Capability of Oregano Extract Solution. Eur. J. Dent. 2015, 9, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Man, A.; Santacroce, L.; Jacob, R.; Mare, A.; Man, L. Antimicrobial Activity of Six Essential Oils Against a Group of Human Pathogens: A Comparative Study. Pathogens 2019, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Selim, S. Antimicrobial Activity Of Essential Oils Against Vancomycin-Resistant Enterococci (Vre) And Escherichia coli O157:H7 In Feta Soft Cheese And Minced Beef Meat. Braz. J. Microbiol. 2011, 42, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakkas, H.; Economou, V.; Gousia, P.; Bozidis, P.; Sakkas, V.A.; Petsios, S.; Mpekoulis, G.; Ilia, A.; Papadopoulou, C. Antibacterial Efficacy of Commercially Available Essential Oils Tested Against Drug-Resistant Gram-Positive Pathogens. Appl. Sci. 2018, 8, 2201. [Google Scholar] [CrossRef] [Green Version]
- Borugă, O.; Jianu, C.; Mişcă, C.; Goleţ, I.; Gruia, A.; Horhat, F. Thymus Vulgaris Essential Oil: Chemical Composition and Antimicrobial Activity. J. Med. Life 2014, 7, 56–60. [Google Scholar] [PubMed]
- Mak, K.-K.; Kamal, M.B.; Ayuba, S.B.; Sakirolla, R.; Kang, Y.-B.; Mohandas, K.; Balijepalli, M.K.; Ahmad, S.H.; Pichika, M.R. A Comprehensive Review on Eugenol’s Antimicrobial Properties and Industry Applications: A Transformation from Ethnomedicine to Industry. Pharmacogn. Rev. 2019, 13. [Google Scholar] [CrossRef]
- Madhavan, S.; Muralidharan. Comparing the Antibacterial Efficacy of Intracanal Medicaments in Combination with Clove Oil against Enterococcus faecalis. Asian J. Pharm. Clin. Res. 2015, 8, 136–138. [Google Scholar]
- Prashar, A.; Locke, I.C.; Evans, C.S. Cytotoxicity of Clove (Syzygium aromaticum) Oil and Its Major Components to Human Skin Cells. Cell Prolif. 2006, 39, 241–248. [Google Scholar] [CrossRef]
- Shakya, V.K.; Luqman, S.; Tikku, A.P.; Chandra, A.; Singh, D.K. A Relative Assessment of Essential Oil of Chrysopogon zizanioides and Matricaria chamomilla along with Calcium Hydroxide and Chlorhexidine Gel against Enterococcus faecalis in Ex Vivo Root Canal Models. J. Conserv. Dent. 2019, 22, 34–39. [Google Scholar] [CrossRef]
- Inchingolo, F.; Dipalma, G.; Cirulli, N.; Cantore, S.; Saini, R.S.; Altini, V.; Santacroce, L.; Ballini, A.; Saini, R. Microbiological Results of Improvement in Periodontal Condition by Administration of Oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1323–1328. [Google Scholar]
- Bohora, A.A.; Kokate, S.R.; Khedkar, S.; Vankudre, A. Antimicrobial Activity of Probiotics against Endodontic Pathogens: A Preliminary Study. Indian J. Med. Microbiol. 2019, 37, 5–11. [Google Scholar] [CrossRef]
- Ran, S.; Liu, B.; Jiang, W.; Sun, Z.; Liang, J. Transcriptome Analysis of Enterococcus faecalis in Response to Alkaline Stress. Front. Microbiol. 2015, 6, 795. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Im, J.; Na, H.; Ryu, S.; Yun, C.-H.; Han, S.H. The Novel Enterococcus Phage VB_EfaS_HEf13 Has Broad Lytic Activity against Clinical Isolates of Enterococcus faecalis. Front. Microbiol. 2019, 10, 2877. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N. Clinical Implications and Microbiology of Bacterial Persistence after Treatment Procedures. J. Endod. 2008, 34, 1291–1301.e3. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CFU/mL (Control) | CFU/mL (AqEO) | % of Inhibition | |
|---|---|---|---|
| Clove | 6.9 × 104 | 0 | 100.0% |
| Thyme | 1.2 × 105 | 102 | 99.9% |
| Oregano | 5.4 × 104 | 0 | 100.0% |
| Lemongrass | 7.5 × 104 | 1.9 × 104 | 75.1% |
| Melaleuca | 1.4 × 105 | 9.5 × 104 | 31.5% |
| NaOCl | 1.5 × 105 | 0 | 100.0% |
| Control | 1.2 × 105 | 7.3 × 104 | 37.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy-Bota, M.C.; Man, A.; Santacroce, L.; Brinzaniuc, K.; Pap, Z.; Pacurar, M.; Pribac, M.; Ciurea, C.N.; Pintea-Simon, I.A.; Kovacs, M. Essential Oils as Alternatives for Root-Canal Treatment and Infection Control against Enterococcus faecalis—A Preliminary Study. Appl. Sci. 2021, 11, 1422. https://0-doi-org.brum.beds.ac.uk/10.3390/app11041422
Nagy-Bota MC, Man A, Santacroce L, Brinzaniuc K, Pap Z, Pacurar M, Pribac M, Ciurea CN, Pintea-Simon IA, Kovacs M. Essential Oils as Alternatives for Root-Canal Treatment and Infection Control against Enterococcus faecalis—A Preliminary Study. Applied Sciences. 2021; 11(4):1422. https://0-doi-org.brum.beds.ac.uk/10.3390/app11041422
Chicago/Turabian StyleNagy-Bota, Monica Cristina, Adrian Man, Luigi Santacroce, Klara Brinzaniuc, Zsuzsanna Pap, Mariana Pacurar, Mirela Pribac, Cristina Nicoleta Ciurea, Ionela Anca Pintea-Simon, and Monika Kovacs. 2021. "Essential Oils as Alternatives for Root-Canal Treatment and Infection Control against Enterococcus faecalis—A Preliminary Study" Applied Sciences 11, no. 4: 1422. https://0-doi-org.brum.beds.ac.uk/10.3390/app11041422