
Comparison of 360° Turn Cycles among Individuals after Stroke and Healthy Older Adults


1
Crean College of Health and Behavioral Sciences, Chapman University, Orange, CA 92866, USA
2
Fowler School of Engineering, Chapman University, Orange, CA 92866, USA
3
Department of Physical Therapy, California State University Long Beach, Long Beach, CA 90840, USA
4
Department of Mathematics, Schmid College of Science and Technology, Orange, CA 92866, USA
5
Department of Industrial and Systems Engineering, Kate Gleason College of Engineering, Rochester, NY 14623, USA
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(7), 3202; https://0-doi-org.brum.beds.ac.uk/10.3390/app11073202
Submission received: 2 March 2021
/
Revised: 25 March 2021
/
Accepted: 30 March 2021
/
Published: 2 April 2021
(This article belongs to the Special Issue Assistive Technology: Biomechanics in Rehabilitation Engineering)
Abstract
:Stroke survivors are at high risk of falling during turning. The kinematics of performing a 360° turn have not been fully analyzed among individuals after stroke. Quantitative differences in the parameters of turning between healthy older adults and those after stroke could provide detailed information on turning ability among these groups. The purpose of the current study was to characterize differences between healthy older adults and adults after stroke in 360° turn kinematics. Fourteen individuals with chronic stroke (mean age: 69 ± 8.4 years) and 14 healthy older adults (mean age: 74 ± 8.7 years) performed three trials of 360° turning. Kinematics data were collected using 26 reflective markers at several body landmarks. This new method for quantifying turning revealed that stroke significantly affected the number of turn cycles, number of single support (SS) critical phases, and critical time. In some cases, falls among individuals with stroke may be related to the combination of impaired movement patterns and the complexity of tasks such as turning. Understanding turning kinematics can inform clinical interventions targeting improvements in turning ability and consequently, fall risk reduction in individuals after stroke.
1. Introduction
Turning is an essential functional skill for performing activities of daily living and maintaining mobility among persons after stroke [1] and older adults [2,3]. Falling during turning is eight times more likely to result in hip fracture than falling while walking [4], which is due to landing on the hip while turning [5]. Stroke is associated with difficulty in turning [6], and this limited turning capacity increases the risk of falls. Although an association between risk of fall and turning is well known, minimal research exists about the execution of turning behavior comparing stroke and healthy controls. New insights into turning behavior or strategies will effectuate appropriate interventions for those after stroke. Previous studies have reported stroke survivors to take more steps and time while turning different angles (45°, 90°, and 180°) than did age-matched healthy individuals [6]. Specifically, turning among stroke survivors is compromised by either declined sensorimotor function [7] or slower self-paced movement speed [8]; however, comparative studies on kinematic analysis while turning among stroke survivors and healthy controls are lacking. Bonnyaud et al. investigated turning in the Timed Up and Go (TUG) task with respect to spatiotemporal and kinematic parameters associated with stroke [9,10], and few other studies reported turning phases using inertial sensors for 180° turning [11,12]. Bonnyaud et al. reported that movement speed, cadence, and step length were reduced on both the paretic and non-paretic side among individuals after stroke during TUG. They also showed that single support phase, peak hip extension, knee flexion, and ankle dorsiflexion were significantly reduced on the paretic side among individuals after stroke compared to healthy counterparts during TUG [9,10]. In contrast to TUG, our study defines turn cycle (TC) during 360° turning, similar to the concept of gait cycle during walking. This new turn cycle definition helps develop a methodology to assess turning ability and key turning characteristics using kinematic data in stroke survivors.
Previous studies have focused on staggering (loss of balance), the number of steps taken to turn, time to turn, and type of turn (pivoting versus step turn) [3,12,13,14]. We understand the importance of these turning parameters, but standardization of turning movement may provide a simple and easy strategy to compare turning among individuals. A 360° turn is critical to study since turning in TUG [15], and figure-of-eight [16] are affected by acceleration and deceleration occurring before and after the turn. The 360° turn times have been studied in community-dwelling older adults [17] and people with Parkinson’s disease (PD) [18]. Some common activities of daily living such as toileting, showering, and other work activities in the kitchen may involve 360° turning. We investigated the 360° turn, which is critical since it is a quick, easy to perform test and suited for quick clinical assessments for stroke survivors. Contrastingly, other tests like TUG and figure-of-eight, where the body is required to reduce its momentum, rotate, and accelerate in a new direction are burdensome to stroke patients. This study aims to characterize patients’ 360° turning ability utilizing kinematic data and assess new parameters of turning disability, which can identify the effectiveness of targeted rehabilitation of turning and possibly identify the severity of disease post-stroke.
2. Materials and Methods
2.1. Participants
We recruited fourteen subjects with stroke and fourteen controls in the Gait Rehabilitation Research Laboratory at Chapman University. The anthropometric data of participants is provided in Table 1a. The Chapman University Institutional Review Board approved the study, and all participants signed the written informed consent. Participants were included if (i) they were able to walk for at least 10 m without any human assistance, (ii) they had no cognitive impairment as measured by Mini-Mental State Examination (MMSE > 24) [19], and (iii) no comorbidity limiting the performance of sit-to-stand was present. Two licensed physical therapists conducted the Fugl-Meyer assessment of participants. The sample size was determined through power analysis using G-Power [20] that indicated power of 80% and an effect size of 0.92 to detect a significant difference in turning time in stroke patients [8,21]. Seven stroke participants had the affected side as the right side and the remaining 7 had the left side as the affected side. All participants were able to ambulate and had stroke at least 6-months prior to participation.
2.2. Instrumentation
Twenty-six reflective markers were placed on several body landmarks utilizing Human Body Model 2 (HBM2) [22,23]. Ten infrared camera systems were used to capture motion through Nexus 1.2 (Vicon, CO, USA). The sampling rate of the camera was set to 100 Hz. The participant performed turning while standing on two force plates (GRAIL, Motek Medical, DIH Netherlands, Groningen, The Netherlands).
2.3. Experimental Tasks
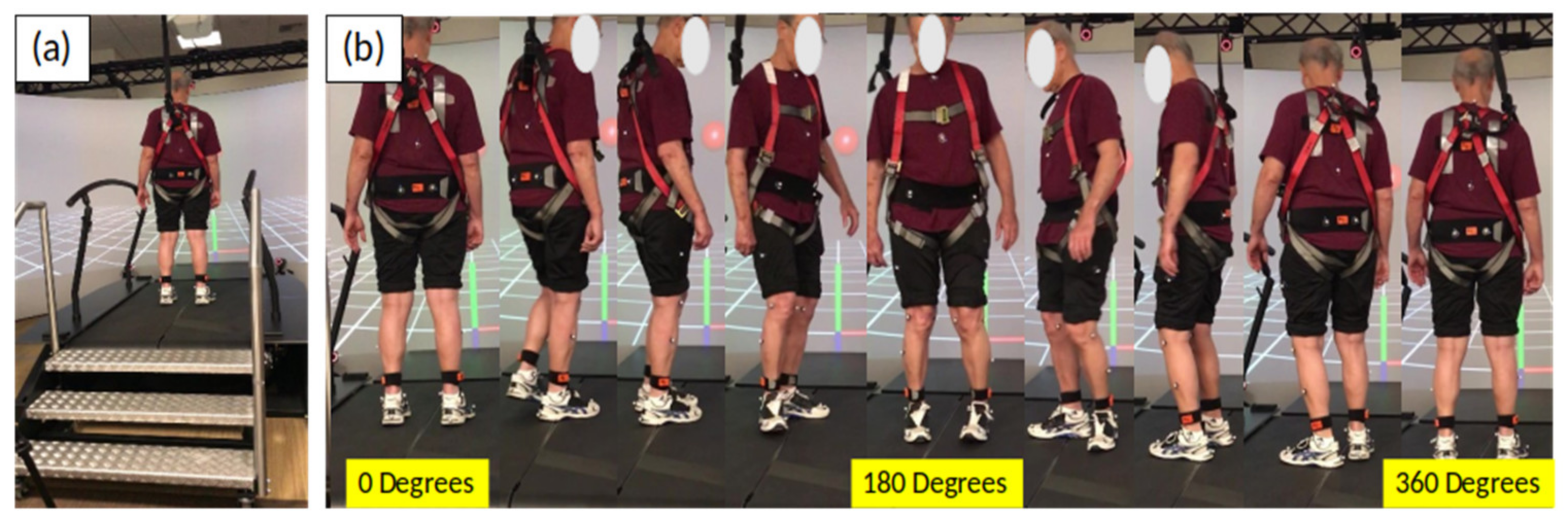
Participants stood straight with an assigned initial position facing a shoulder-level target and were asked to turn 360° at their comfortable pace (Figure 1a). The participants were asked not to look at the ground while turning. The participants were asked to face the target at the end position of the 360° turn (Figure 1b). They were asked to reposition their feet, similar to their initial position, using a footprint mark. The two footprints were on two force plates (GRAIL, DIH Hocoma Motekforce Link B.V., Amsterdam, The Netherlands) placed side-by-side of size, with area of turning within 1 m × 2 m. Two licensed physical therapists were present by the side (approximately 800 cm on each side) while participants performed the turning task. The force plates were situated at some height (approximately 80 cm) from the ground level as shown in Figure 1a. Two trials where participants initiated turns on both the right and left side were collected and the average of turning parameters was used for further analysis.
2.4. Data Processing
Data were processed using MATLAB (MathWorks, Natick, MA, USA). The marker trajectory gaps were filled using the spline function. Marker trajectorial data from heel and toe were filtered using a zero-lag 4th order low pass Butterworth filter. Two trials each when initiating from the affected limb and opposite limb (right and left side) were averaged for analysis of turning parameters. Events such as foot contact and foot off were identified and verified visually using the digital video recordings and force plates. Important turning variables shown in the results (Table 2 and Figure 2) were identified as per the cyclic patterns observed during turning.
2.5. Turning Data Analysis
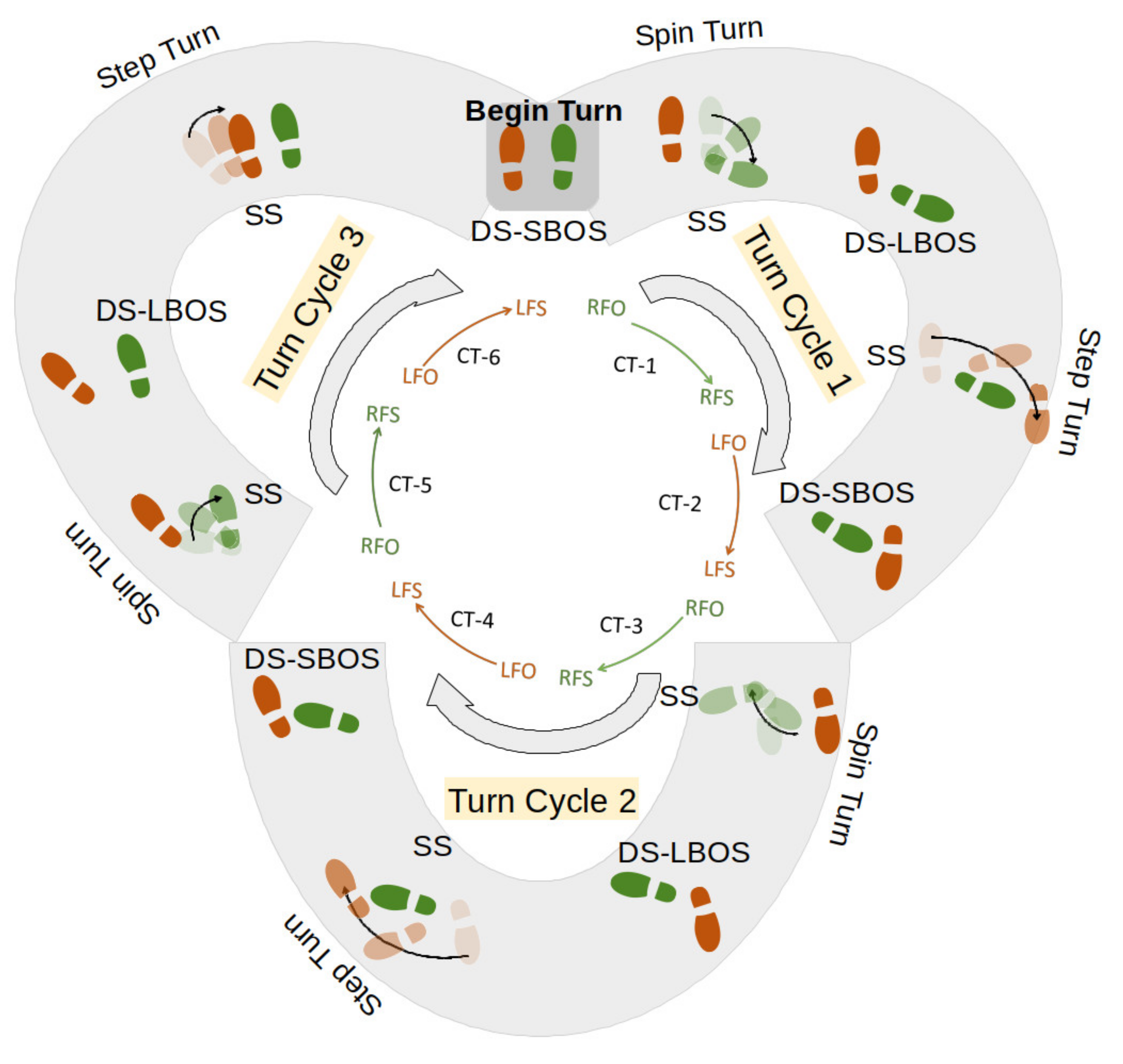
Turning as a cyclic behavior: A 360° turn is composed of several units of turn cycles depending on the balance ability of the subject, usually with a minimum of three turn cycles in healthy adults. Each turn cycle has two turns: (1) spin turn and (2) step turn. Each turn has a single support (SS critical phase) (one foot on ground) and double support (DS) (both feet on ground). The time interval of SS critical phase is defined as critical time (with high instability) when the participant is on a single limb support (either ipsilateral or contralateral foot). Double support can be placed into two categories: (i) double support with feet apart (large base of support DS-LBOS), which occurs in the spin turn, and (ii) double support with feet together (small base of support DS-SBOS), which occurs in the step turn. Turning variables are defined in Table 1b.
The direction of turning starts with the initiation foot (or leading/ipsilateral foot) undergoing a spin turn through foot off (FO) followed by ipsilateral foot strike (FS) leading to DS-LBOS. The time taken from the first FO to FS is defined as critical time-1 (CT-1). Similarly, the events are followed sequentially for the contralateral foot (trailing limb) from a position of DS-LBOS to SS critical phase and then back to DS-SBOS. Thus, all odd-numbered critical times (such as CT-1, CT-3, CT-5) are from ipsilateral (or leading) foot SS movement via spin turns and all even-numbered critical times (such as CT-2, CT-4, CT-6) are from the contralateral (trailing) foot SS movement via step turns. Figure 2 shows all these events in a sequence, with the right foot being the initiation foot (leading or ipsilateral foot) and the left foot being the contralateral foot (or trailing limb). Thus, a turn cycle (TC) starts with a spin turn of (a) FO of leading limb (SS) and (b) FS of leading limb (DS-LBOS), followed by a step turn of (c) FO of trailing limb (SS) and (d) FS of the trailing foot (DS-SBOS). Thus, each turn cycle consists of two FOs and two FSs for each leading and trailing limb.
2.6. Statistical Analysis
A multivariate analysis of variance (MANOVA) was first performed on temporal variables to help protect against inflating the Type 1 error rate in the follow-up univariate ANOVAs. Initially, Pearson correlations were performed on all the dependent variables (Table 2) to test the MANOVA assumption. Variables were found to be moderately correlated. Before conducting a series of follow-up ANOVAs, the homogeneity of variance assumption was tested for all variables. Participant groups were evaluated for group differences for age, and Body Mass Index (BMI) using T-test. Cohen’s d was used to describe the standardized mean difference of an effect for the turning variables.
Each turn cycle includes one spin turn followed by a step turn. Spin turn has a single support (SS critical phase) (or corresponding critical time, CT) and double support with large base of support (DS-LBOS). The step turn has a single support (or corresponding CT) and double support with small base of support (DS-SBOS). Figure 2 shows six critical times in three turn cycles when the participant was turning and when supported by one foot. Turning events like right foot off (RFO), right foot strike (RFS), left foot off (LFO), and left foot strike (LFS) with critical times (CT1–CT6) are shown during 3 turn cycles. Two trials where participants initiated turns by both right and left side were collected (only right-side initiation is represented in Figure 2).
3. Results
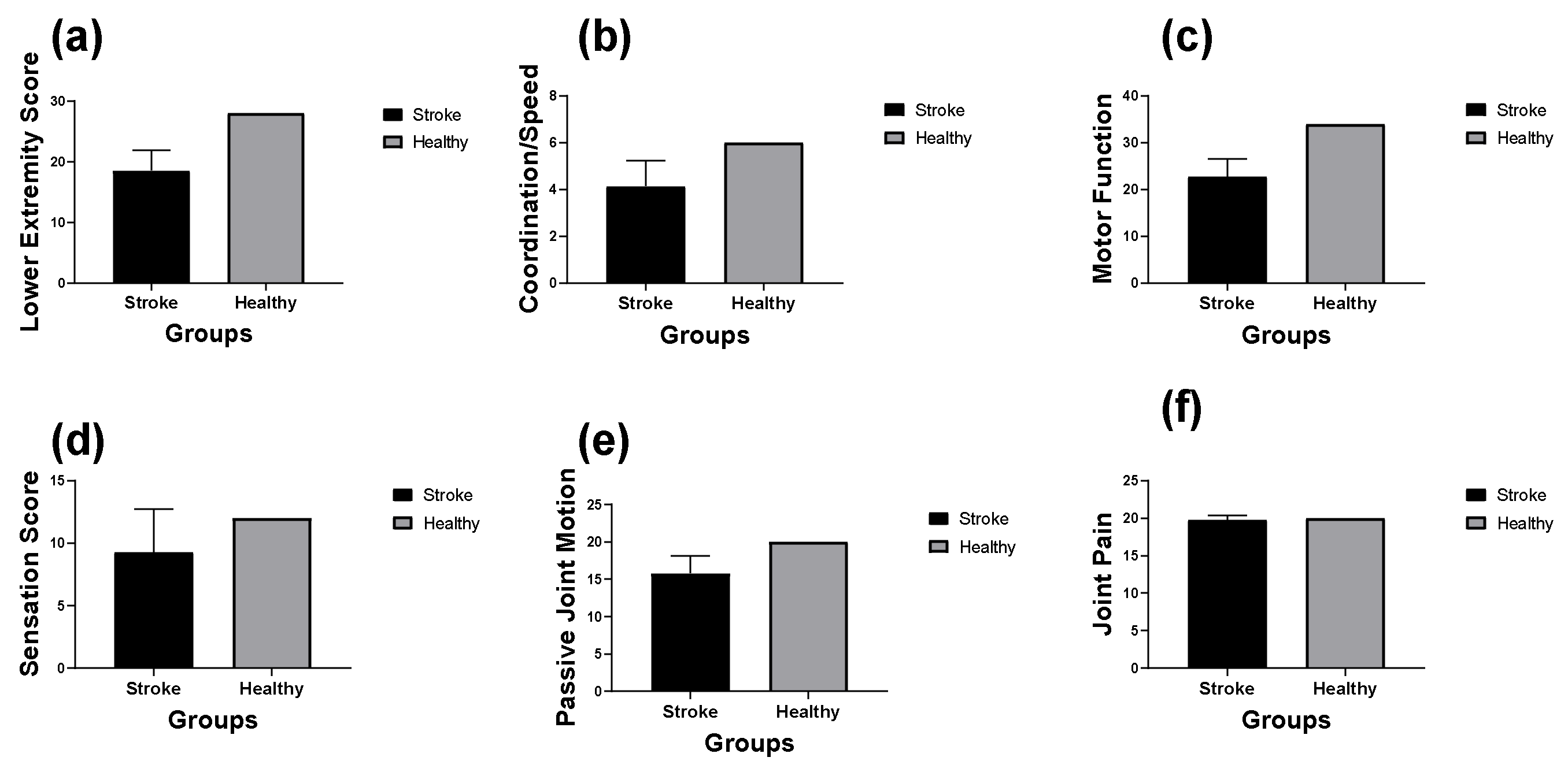
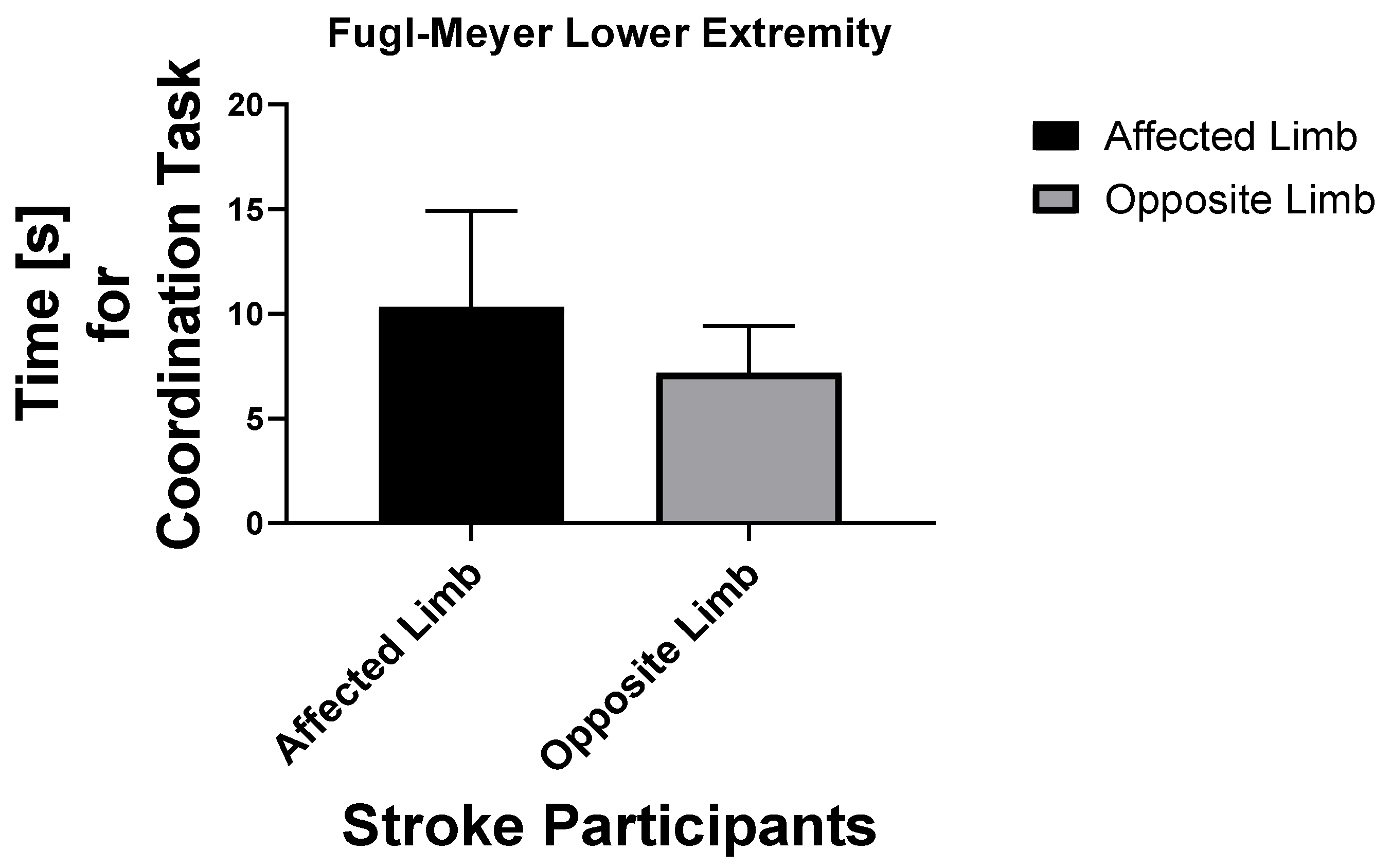
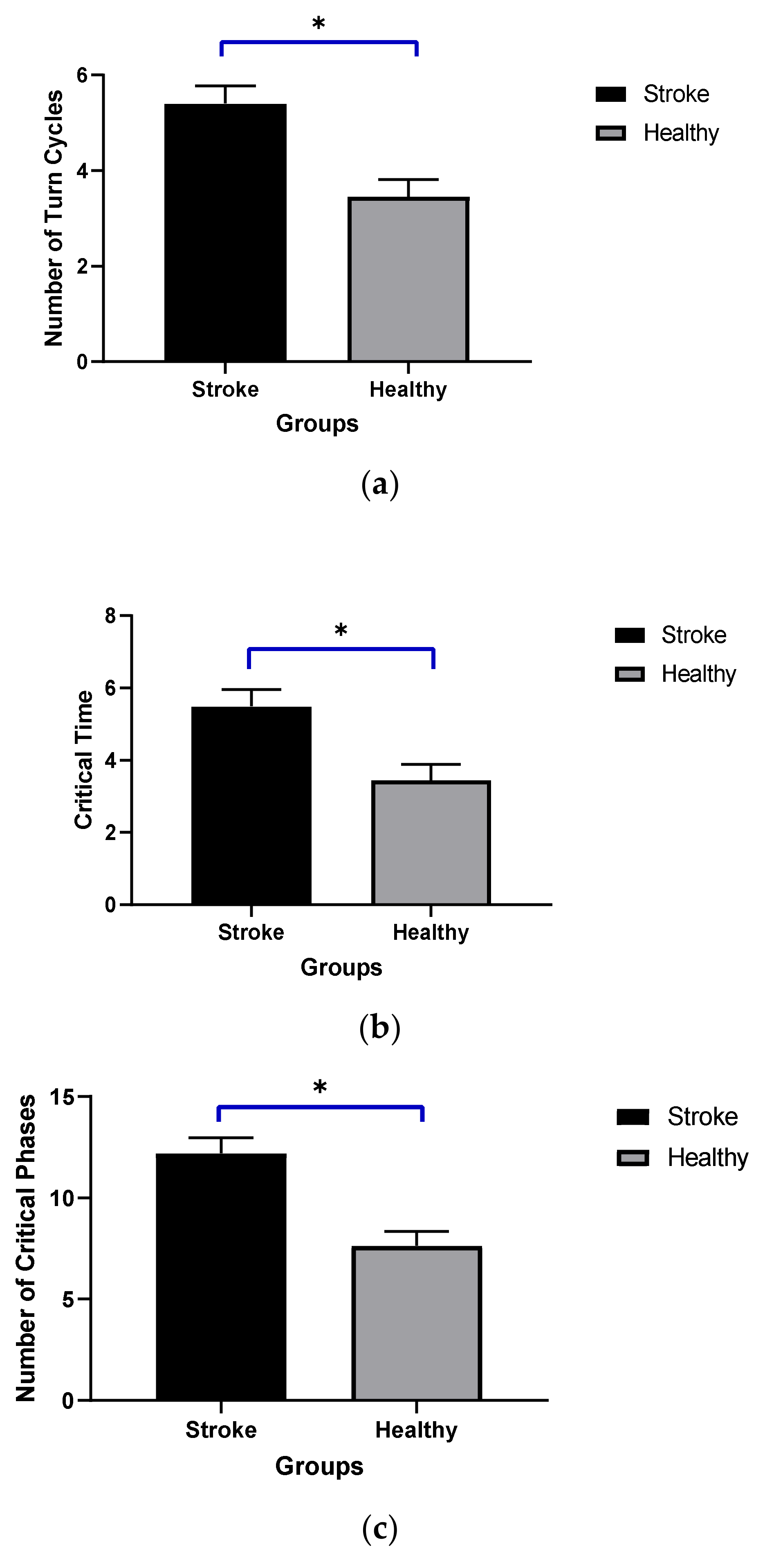
The demographic data showed that the age and BMI were significantly different (p < 0.05). Fugl-Meyer lower extremity assessments were done in both healthy participants and those after stroke, as shown in Figure 3. For individuals after stroke, the time for coordination of task was assessed for the participants’ affected and opposite side (or less affected) (Figure 4). Persons after stroke took significantly more turn cycles than healthy individuals with p = 0.0014 (5.4 ± 0.37 s versus 3.45 ± 0.36 s) (Figure 5a). Participants after stroke also had significantly more critical time than healthy older adults; p = 0.0054 (Figure 5b). They also had more critical phases than healthy counterparts; p = 0.0004 (Figure 5c).
4. Discussion
Turning is a vital motor skill required in the performance of daily living activities and human mobility. Previous investigators have reported that impaired turning may increase the risk of falls [24,25] and fall injuries in several populations such as PD [26] and stroke [27]. To our knowledge, this is one of the first studies to investigate turning using motion-capture data and characterizing turning into turn cycles similar to gait cycles. This characterization into turn cycles makes it easier to study complicated movements such as 360° turns. This study aimed to characterize the turning ability of patients utilizing kinematic data from infrared markers. This would allow clinicians to assess new parameters of turning disability, which can identify the effectiveness of rehabilitation and possibly identify which persons after stroke are at risk of falling.
As expected, we found individuals after stroke took significantly more time and required a greater number of steps compared to age-matched healthy older controls. Stroke-affected participants faced difficulty turning due to the effects of hemiparalysis and impairments in balance, muscle weakness, and coordination [1,6]. The slowness of turning in those after stroke can be linked to their level of impairment [2,28] or increased fall risk [24,29]. Healthy control participants have been reported to complete a 360° turn in under 4 s [3]. However, the method for how the turning speed was measured was not reported, and no normative data exist. In this study, we defined turn cycles, their phases, and how they are measured. Individuals after stroke took 1.88 ± 2.05 s to complete a turn cycle, whereas healthy older adults took 1.08 ± 0.28 s to complete the turn cycle. We found participants after stroke took significantly more turn cycles compared to healthy individuals (F (1, 19) = 13.8, with p = 0.0014 (5.4 ± 0.37 s versus 3.45 ± 0.36 s)) (Figure 5a).
As a turning strategy, individuals after stroke had longer critical times (rests) on the trailing foot, whereas healthy adults had longer critical times on the leading foot. We also found that the stroke group had longer double support times than the healthy adult group, approximately five times more when feet were apart and six times more when feet were together. We found that stroke participants spent on average 8.74 s (SD = 12) and healthy participants 1.27 s (SD = 0.44) on double support (both feet apart and feet together) when completing a 360° turn (Table 2). During double support phase, proprioceptive inputs from skin mechanoreceptors, spindle fibers, and joint receptors provide loading information to our central nervous system [30,31]. The increased double support phase during turning in stroke survivors may be due to neuromuscular dysfunction relating to reduced proprioceptive signals and increased time to attain more signals and stabilize during double support phase.
We also found that stroke survivors had significantly longer critical time than the healthy adult group (F (1, 19) = 9.83, with p = 0.0054). The critical time is an indicator of high instability, which may lead to falling. Since during single support phase, one of the feet is in the air and the other on the ground, stroke survivors have to (i) modulate the pace of the swing foot (either affected limb or opposite limb), requiring an appropriate motor control strategy that results in stable landing of the foot and (ii) counter for reduced proprioceptive signals from the stance foot (either affected limb or opposite limb). Thus, this complex SS critical phase may require more time for those after stroke due to neuromuscular deficits compared to healthy controls.
We also found that the number of SS critical phases was significantly higher among stroke groups than healthy counterparts (F (1, 19) = 18.8, with p = 0.0004). This increase in the number of SS critical phases may increase the risk of falls among stroke survivors due to instability during SS critical phases. An asymmetric turn pattern was observed in our participants likely due to abnormal muscle tone and hemiparesis in participants after stroke. An abnormal turn could be associated with diminished power generation and increased critical time since the SS critical phase requires adequate foot trajectory and placement, thereby resulting in significantly higher critical times than healthy counterparts. We did not find any preference among stroke survivors to initiate turning with the affected or opposite limb in our subject population. We acknowledge several limitations associated with this study. The stroke population in this study is younger than healthy older adults with an average of 69 versus 74 years of age. The participants who had stroke had significantly greater BMI compared to healthy older adults. This may be attributed to stroke occurrence at young age (about 10% of stroke occurs in people aged less than 45 years) [32] and affecting mobility and body mass of the individuals [33]. We also acknowledge for selection bias in this study since all stroke participants were recruited from Stroke Boot Camp, which is a rehabilitation camp held at university.
Turning ability requires dynamic and reactive balance control, which is an important measure for fall risk assessment. It could also be a measure of the severity of stroke or objectively quantify rehabilitation progress post-stroke. In the future, this research can be translated to clinics as metrics of fall risk or functional mobility among those after stroke. For example, new quick assessments using smartphone sensors and mobile applications could be developed for turning diagnosis in clinical environments.
5. Conclusions
Turning ability requires a dynamic and reactive balance with appropriate motor control. In this study, new turning measures were developed to discriminate turning ability in two groups of participants (stroke versus healthy adults). Turning is a frequently performed maneuver by those after stroke [27,34] and healthy older participants [35]. Impairment in turning may increase fall risk [36] and elevate the risk of hip injuries [37]. Undoubtedly, those after chronic stroke are a subgroup of older adults who inherit functional and motor limitations due to their age and risk of falls.
We recommend that clinicians examine their patients for turning ability as a means of quantifying the functional impairment and fall risk associated after stroke. Examining individuals in clinical and senior center environments may provide valuable insights into turning difficulties and provide physical therapists with information about the aids needed for postural transitions in their environments (home, senior living centers, shopping markets, etc.). Given the functional demands of performing Activities of Daily Livings (ADLs), clinicians may have to rely on a battery of assessments to understand fall risk in stroke survivors, including an assessment of turning ability.
Author Contributions
Conceptualization, R.S.; methodology, R.S.; software, V.K., R.S.; validation, R.S., J.J., E.R., V.K., A.M.; formal analysis, R.S.; investigation, R.S.; resources, A.M.; data curation, R.S., A.M.; writing—original draft preparation, R.S., E.R., J.J., V.K., A.M.; writing—review and editing, V.K., A.M., R.S., J.J.; visualization, V.K.; supervision, A.M.; project administration, R.S., A.M.; funding acquisition, R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Crean College Internal College Funding and The APC was funded by Department of Physical Therapy, Chapman University.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Chapman University (Chapman University IRB# 17-13 and date of approval as 10-21-2017).
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All data included in this study are available upon request by contact with the corresponding author.
Acknowledgments
We are very thankful to Patricia Brown, Caryn Ito, Christopher Hoang, Norah Nyangau, Michael Shiraishi for their help in data collection and data processing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Manaf, H.; Justine, M.; Omar, M.; Isa, K.A.M.; Salleh, Z. Turning Ability in Stroke Survivors: A Review of Literature. ISRN Rehabil. 2012, 2012, 1–8. [Google Scholar] [CrossRef]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: The “get-up and go” test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar]
- Berg, K. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Cumming, R.G.; Klineberg, R.J. Fall frequency and characteristics and the risk of hip fractures. J. Am. Geriatr. Soc. 1994, 42, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, C.M.; Cummings, S.R. Type of fall and risk of hip and wrist fractures: The study of osteoporotic fractures. The Study of Osteoporotic Fractures Research Group. J. Am. Geriatr. Soc. 1993, 41, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.; Luttmann, K. Turning capacity in ambulatory individuals poststroke. Am. J. Phys. Med. Rehabil. 2009, 88, 873–883. [Google Scholar] [CrossRef]
- Lamontagne, A.; Fung, J. Gaze and Postural Reorientation in the Control of Locomotor Steering After Stroke. Neurorehabilit. Neural. Repair. 2008, 23, 256–266. [Google Scholar] [CrossRef]
- Leigh Hollands, K.; Hollands, M.A.; Zietz, D.; Wing, A.M.; Wright, C.; Vliet, P.V. Kinematics of Turning 180° During the Timed Up and Go in Stroke Survivors With and Without Falls History. Neurorehabilit. Neural. Repair. 2009, 24, 358–367. [Google Scholar] [CrossRef]
- Bonnyaud, C.; Pardon, D.; Vuillerme, N.; Bensmail, D.; Roche, N. Spatiotemporal and Kinematic Parameters Relating to Oriented Gait and Turn Performance in Patients with Chronic Stroke. PLoS ONE 2015, 10, e0129821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnyaud, C.; Pardon, D.; Vaugier, I.; Vuillerme, N.; Bensmail, D.; Roche, N. Timed Up and Go test: Comparison of kinematics between patients with chronic stroke and healthy subjects. Gait Posture 2016, 49, 258–263. [Google Scholar] [CrossRef]
- Barrois, R.P.-M.; Ricard, D.; Oudre, L.; Tlili, L.; Provost, C.; Vienne, A.; Vidal, P.P.; Buffat, S.; Yelnik, A.P. Observational Study of 180° Turning Strategies Using Inertial Measurement Units and Fall Risk in Poststroke Hemiparetic Patients. Front. Neurol. 2017, 8, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsitz, L.A.; Jonsson, P.V.; Kelley, M.M.; Koestner, J.S. Causes and correlates of recurrent falls in ambulatory frail elderly. J. Gerontol. 1991, 46, M114–M122. [Google Scholar] [CrossRef]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Hase, K.; Stein, R.B. Turning strategies during human walking. J. Neurophysiol. 1999, 81, 2914–2922. [Google Scholar] [CrossRef]
- Persson, C.U.; Danielsson, A.; Sunnerhagen, K.S.; Grimby-Ekman, A.; Hansson, P.-O. Timed Up & Go as a measure for longitudinal change in mobility after stroke-Postural Stroke Study in Gothenburg (POSTGOT). J. Neuroeng. Rehabil. 2014, 11, 83. [Google Scholar]
- Wong, S.S.; Yam, M.S.; Ng, S.S. The Figure-of-Eight Walk test: Reliability and associations with stroke-specific impairments. Disabil. Rehabil. 2013, 35, 1896–1902. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Williams, C.S.; Tinetti, M.E. Assessing Risk for the Onset of Functional Dependence Among Older Adults: The Role of Physical Performance. J. Am. Geriatr. Soc. 1995, 43, 603–609. [Google Scholar] [CrossRef]
- Schenkman, M.; Cutson, T.M.; Kuchibhatla, M.; Chandler, J.; Pieper, C. Reliability of Impairment and Physical Performance Measures for Persons With Parkinson’s Disease. Phys. Ther. 1997, 77, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A general power analysis program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Ng, S.S.; Hui-Chan, C.W. The timed up & go test: Its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1641–1647. [Google Scholar]
- Mousavi, S.H.; Kouwenhove, L.V.; Rajabi, R.; Zwerver, J.; Hijmans, J.M. The effect of changing mediolateral center of pressure on rearfoot eversion during treadmill running. Gait Posture 2021, 83, 201–209. [Google Scholar] [CrossRef]
- van den Bogert, A.J.; Geijtenbeek, T.; Even-Zohar, O.; Steenbrink, F.; Hardin, E.C. A real-time system for biomechanical analysis of human movement and muscle function. Med. Biol. Eng. Comput. 2013, 51, 1069–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leach, J.M.; Mellone, S.; Palumbo, P.; Bandinelli, S.; Chiari, L. Natural turn measures predict recurrent falls in community-dwelling older adults: A longitudinal cohort study. Sci. Rep. 2018, 8, 4316. [Google Scholar] [CrossRef] [Green Version]
- Haertner, L.; Elshehabi, M.; Zaunbrecher, L.; Pham, M.H.; Maetzler, C.; van Uem, J.M.; Hobert, M.A.; Hucker, S.; Nussbaum, S.; Berg, D.; et al. Effect of Fear of Falling on Turning Performance in Parkinson’s Disease in the Lab and at Home. Front. Aging Neurosci. 2018, 10, 78. [Google Scholar] [CrossRef] [PubMed]
- Mellone, S.; Mancini, M.; King, L.A.; Horak, F.B.; Chiari, L. The quality of turning in Parkinson’s disease: A compensatory strategy to prevent postural instability? J. Neuroeng. Rehabil. 2016, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Chan, N.W.; Tsang, W.W. The performance of stroke survivors in turning-while-walking while carrying out a concurrent cognitive task compared with controls. PLoS ONE 2017, 12, e0189800. [Google Scholar]
- Martinez-Martin, P.; Urra, D.G.; Quijano, T.; Gomez, J.B.; Utrero, E.G.; Pineiro, R.; Andres, M.T. A new clinical tool for gait evaluation in Parkinson’s disease. Clin. Neuropharmacol. 1997, 20, 183–194. [Google Scholar] [CrossRef]
- Mancini, M.; Schlueter, H.; El-Gohary, M.; Mattek, N.; Duncan, C.; Kaye, J.; Horak, F.B. Continuous Monitoring of Turning Mobility and Its Association to Falls and Cognitive Function: A Pilot Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1102–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, V.; Duysens, J. Significance of load receptor input during locomotion: A review. Gait Posture 2000, 11, 102–110. [Google Scholar] [CrossRef]
- Zhang, J.; Lockhart, T.E.; Soangra, R. Classifying lower extremity muscle fatigue during walking using machine learning and inertial sensors. Ann. Biomed. Eng. 2014, 42, 600–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, M.G. Risk Factors for Ischemic Stroke in Younger Adults. Stroke 2020, 51, 729–735. [Google Scholar] [CrossRef]
- Irfani Fitri, F.; Fithrie, A.; Rambe, S.R. Association between working memory impairment and activities of daily living in post-stroke patients. Med. Glas 2020, 17, 433–438. [Google Scholar] [PubMed]
- Son, H.; Park, C. Effect of turning direction on Timed Up and Go test results in stroke patients. Eur. J. Phys. Rehabil. Med. 2019, 55, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Rehman, R.Z.U.; Yu, X.; Xiong, S. Application of Wearable Inertial Sensors and A New Test Battery for Distinguishing Retrospective Fallers from Non-fallers among Community-dwelling Older People. Sci. Rep. 2018, 8, 16349. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.Y.; Yang, Y.R.; Wang, C.J.; Wu, Y.H.; Cheng, S.J.; Wang, H.C.; Wang, R.Y. Factors Influencing Turning and Its Relationship with Falls in Individuals with Parkinson’s Disease. PLoS ONE 2014, 9, e93572. [Google Scholar]
- Muangpaisan, W.; Suwanpatoomlerd, S.; Srinonprasert, V.; Sutipornpalangkul, W.; Wongprikron, A.; Assantchai, P. Causes and course of falls resulting in hip fracture among elderly Thai patients. J. Med. Assoc. Thai 2015, 98, 298–305. [Google Scholar] [PubMed]
Figure 1.
(a) Experimental setup where a representative participant is supported by an overhead harness and looking at a virtual target. (b) Participant turning 360°.
Figure 1.
(a) Experimental setup where a representative participant is supported by an overhead harness and looking at a virtual target. (b) Participant turning 360°.

Figure 2.
Three turn cycles (TCs) during a 360° turn.

Figure 3.
(a) A lower extremity score was attained by (i) reflex activity, (ii) volitional movement within synergies, (iii) volitional movement mixing synergies, (iv) volitional movement with little or no synergy, or (v) normal reflex activity. (b) Coordination/speed was attained by moving feet from heel to knee of other leg, 5 times, as fast as possible with eyes closed in supine position. (c) Motor function was a composite score evaluated from lower extremity score and coordination/speed score. (d) Sensation score was estimated from slight touch with eyes closed compared with unaffected side. (e) Passive joint motion was assessed at supine position. (f) Joint pain during passive motion was assessed.
Figure 3.
(a) A lower extremity score was attained by (i) reflex activity, (ii) volitional movement within synergies, (iii) volitional movement mixing synergies, (iv) volitional movement with little or no synergy, or (v) normal reflex activity. (b) Coordination/speed was attained by moving feet from heel to knee of other leg, 5 times, as fast as possible with eyes closed in supine position. (c) Motor function was a composite score evaluated from lower extremity score and coordination/speed score. (d) Sensation score was estimated from slight touch with eyes closed compared with unaffected side. (e) Passive joint motion was assessed at supine position. (f) Joint pain during passive motion was assessed.

Figure 4.
Time taken by affected and opposite foot for coordination task among stroke survivors during Fugl-Meyer assessment.
Figure 4.
Time taken by affected and opposite foot for coordination task among stroke survivors during Fugl-Meyer assessment.

Figure 5.
(a) Average number of turn cycles in stroke and healthy groups. (b) Critical time in seconds in stroke and healthy adults. (c) Number of critical phases during 360° turn in stroke and healthy adults. Where * represents significant different among groups.
Figure 5.
(a) Average number of turn cycles in stroke and healthy groups. (b) Critical time in seconds in stroke and healthy adults. (c) Number of critical phases during 360° turn in stroke and healthy adults. Where * represents significant different among groups.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
(a) Anthropometric data of stroke participants and healthy older adults. (b) Turning variable and its definitions.
Table 1.
(a) Anthropometric data of stroke participants and healthy older adults. (b) Turning variable and its definitions.
| (a) | |||||
| Age (years) (Mean ± SD) | Height (cm) (Mean ± SD) | Weight (kg) (Mean ± SD) | Body Mass Index (BMI) (kg/m2) | Gender | |
| Control (n = 14) | 74 ± 8.7 | 162 ± 10 | 68 ± 13 | 26.18 ± 3.03 | 8 females and 6 males |
| Stroke (n = 14) | 69 ± 8.4 | 179 ± 8.27 | 84.9 ± 22.3 | 30.87 ± 5.64 | 6 females and 8 males |
| (b) | |||||
| Turning Variable | Definition | ||||
| Double support (DS-LBOS) | Both feet on the ground with feet apart (large base of support) | ||||
| Double support (DS-SBOS) | Both feet on the ground with feet together (small base of support) | ||||
| Single support (SS) | One foot on the ground | ||||
| Critical time (CT) | Time interval between foot off (FO) and foot strike (FS) or during single support (SS critical phase) | ||||
| Turn cycle (TC) | FO of one foot (ipsilateral or contralateral foot) to the next FO of the same foot | ||||
| Leading limb | Foot that initiates the swing first toward the direction of turn | ||||
| Trailing limb | Foot following the leading limb while turning | ||||
Table 2.
Comparisons of kinematic turning variables (means ± SD) between stroke and older adults.
| Healthy Individuals | Stroke | Cohen’s d | |
|---|---|---|---|
| Mean leading limb critical times (CTs) [seconds] | 0.47 ± 0.17 | 0.44 ± 0.12 | 0.20 |
| Standard deviation of leading limb critical times [seconds] | 0.13 ± 0.06 | 0.11 ± 0.10 | 0.24 |
| Mean trailing limb critical times [seconds] | 0.44 ± 0.12 | 0.47 ± 0.18 | 0.19 |
| Standard deviation of trailing limb critical times [seconds] | 0.08 ± 0.06 | 0.11 ± 0.08 | 0.42 |
| Number of critical time/single support (SS) [n] | 7.64 ± 1.36 | 12.20 ± 3.19 | 1.85 |
| Total critical time duration [seconds] | 3.45 ± 1.18 | 5.49 ± 1.77 | 1.35 |
| Mean critical time duration [seconds] | 0.91 ± 0.28 | 0.91 ± 0.22 | 0.0 |
| Standard deviation of critical time duration [seconds] | 0.21 ± 0.09 | 0.21 ± 0.12 | 0.0 |
| Mean double support feet apart (DS-LBOS) [seconds] | 16.94 ± 7.49 | 98.38 ± 209.3 | 0.54 |
| Standard deviation of double support feet apart [seconds] | 8.17 ± 3.75 | 10.97 ± 8.05 | 0.44 |
| Mean double support feet together (DS-SBOS) [seconds] | 20.64 ± 6.98 | 118.5 ± 196.0 | 0.70 |
| Standard deviation of double support feet together [seconds] | 10.48 ± 4.61 | 19.21 ± 30.64 | 0.39 |
| Total double support duration [seconds] | 1.27 ± 0.44 | 8.74 ± 12.00 | 0.87 |
| Mean double support duration [seconds] | 0.19 ± 0.04 | 1.08 ± 2.02 | 0.62 |
| Standard deviation of double support duration [seconds] | 0.11 ± 0.03 | 0.24 ± 0.21 | 0.86 |
| Number of turn cycles | 3.45 ± 0.69 | 5.40 ± 1.58 | 1.59 |
| Mean time taken in a turn cycle [seconds] | 1.08 ± 0.28 | 1.88 ± 2.05 | 0.54 |
| Standard deviation of time in a turn cycle [seconds] | 0.13 ± 0.08 | 0.14 ± 0.07 | 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Soangra, R.; Krishnan, V.; John, J.; Rashedi, E.; McKenzie, A. Comparison of 360° Turn Cycles among Individuals after Stroke and Healthy Older Adults. Appl. Sci. 2021, 11, 3202. https://0-doi-org.brum.beds.ac.uk/10.3390/app11073202
AMA Style
Soangra R, Krishnan V, John J, Rashedi E, McKenzie A. Comparison of 360° Turn Cycles among Individuals after Stroke and Healthy Older Adults. Applied Sciences. 2021; 11(7):3202. https://0-doi-org.brum.beds.ac.uk/10.3390/app11073202
Chicago/Turabian StyleSoangra, Rahul, Vennila Krishnan, Joby John, Ehsan Rashedi, and Alison McKenzie. 2021. "Comparison of 360° Turn Cycles among Individuals after Stroke and Healthy Older Adults" Applied Sciences 11, no. 7: 3202. https://0-doi-org.brum.beds.ac.uk/10.3390/app11073202
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.