
Biology of Drug-Induced Gingival Hyperplasia: In Vitro Study of the Effect of Nifedipine on Human Fibroblasts

 , ,
, ,
Abstract
:1. Introduction
Objectives
2. Materials and Methods
2.1. Primary Human Fibroblast Cells’ Culture
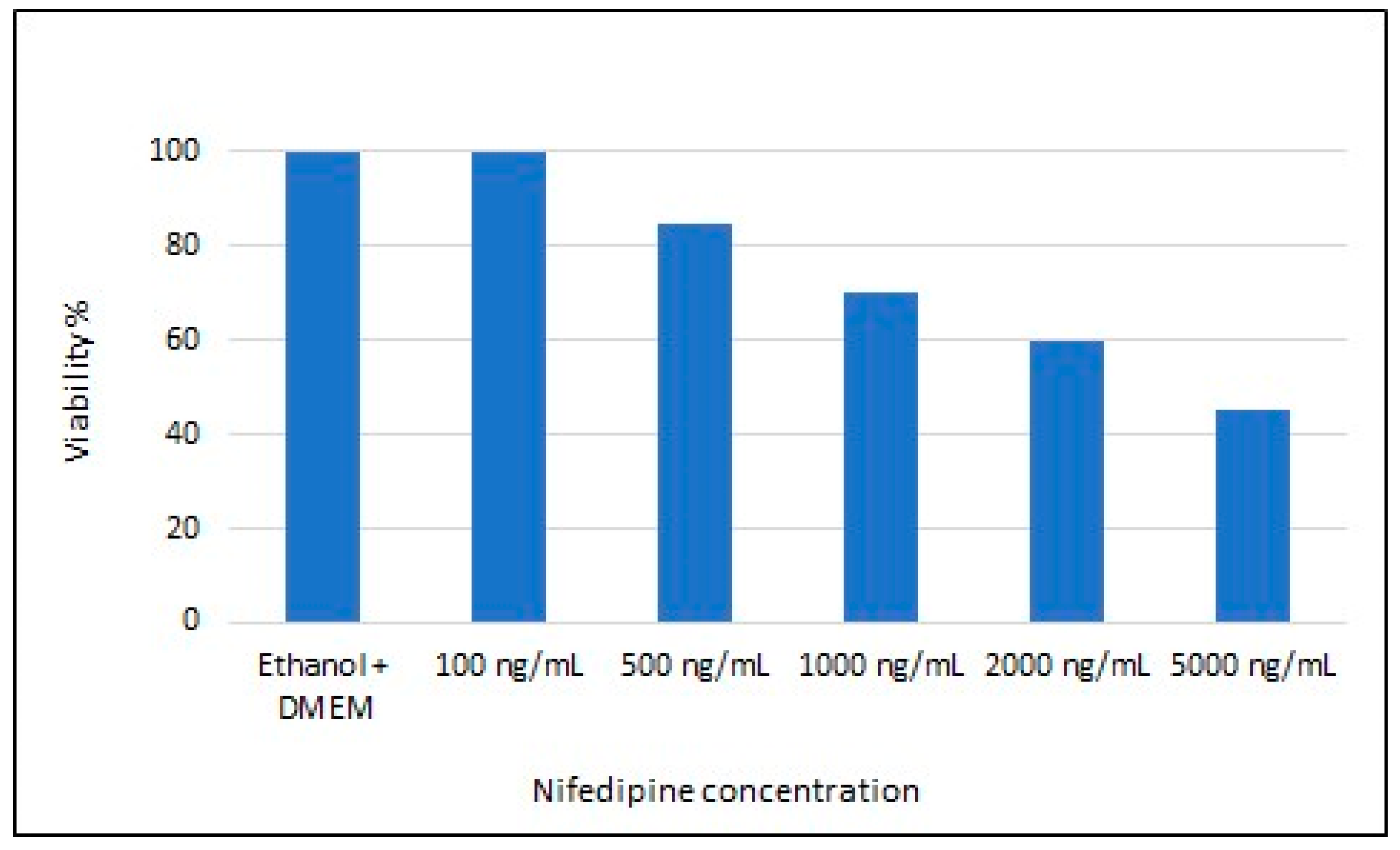
2.2. Cell Viability Test
2.3. Cell Treatment
2.4. RNA Isolation, Reverse Transcription, and Quantitative Real-Time Polymerase Chain Reaction
2.5. Statistical Analysis
2.6. Detection of E-Cadherin Levels by Enzyme-Linked Immunosorbent Assay
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Psaty, B.M.; Smith, N.L.; Siscovick, D.S.; Koepsell, T.D.; Weiss, N.S.; Heckbert, S.R.; Lemaitre, R.N.; Wagner, E.H.; Furberg, C.D. Health Outcomes Associated With Antihypertensive Therapies Used as First-Line AgentsA Systematic Review and Meta-analysis. JAMA 1997, 277, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [PubMed]
- Striessnig, J.; Ortner, N.; Pinggera, A. Pharmacology of L-type Calcium Channels: Novel Drugs for Old Targets? Curr. Mol. Pharmacol. 2015, 8, 110–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godfraind, T. Discovery and Development of Calcium Channel Blockers. Front. Pharmacol. 2017, 8, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Geijn, H.P.; Lenglet, J.E.; Bolte, A.C. Nifedipine trials: Effectiveness and safety aspects. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 79–83. [Google Scholar] [CrossRef]
- Khan, K.M.; Patel, J.; Schaefer, T.J. Nifedipine. StatPearls Publishing, Treasure Iland (FL). Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK537052/ (accessed on 14 December 2020).
- Ross, S.D.; Akhras, K.S.; Zhang, S.; Rozinsky, M.; Nalysnyk, L. Discontinuation of antihypertensive drugs due to adverse events: A systematic review and meta-analysis. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2001, 21, 940–953. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.; Brunet, L.; Roset, P.; Berini, L.; Farré, M.; Mendieta, C. Prevalence and Risk of Gingival Enlargement in Patients Treated With Nifedipine. J. Periodontol. 2001, 72, 605–611. [Google Scholar] [CrossRef] [Green Version]
- Sauget, P.; Monteil, R.A.; Morand, P.; Loubiere, R.; Lapalus, P.; Haudebourg, C. Gingival hyperplasia secondary to the use of calcium antagonists: Analysis. J. Boil. Buccale 1992, 20, 25–32. [Google Scholar]
- Lucas, R.M.; Howell, L.P.; Wall, B.A. Nifedipine-Induced Gingival Hyperplasia: A Histochemical and Ultrastructural Study. J. Periodontol. 1985, 56, 211–215. [Google Scholar] [CrossRef]
- Brunet, L.; Miranda, J.; Roset, P.; Berini, L.; Farré, M.; Mendieta, C. Prevalence and risk of gingival enlargement in patients treated with anticonvulsant drugs. Eur. J. Clin. Investig. 2001, 31, 781–788. [Google Scholar] [CrossRef]
- Dongari-Bagtzoglou, A. Informational Paper: Drug-Associated Gingival Enlargement. J. Periodontol. 2004, 75, 1424–1431. [Google Scholar] [CrossRef]
- Ramírez-Rámiz, A.; Brunet-Llobet, L.; Lahor-Soler, E.; Miranda-Rius, J. On the Cellular and Molecular Mechanisms of Drug-Induced Gingival Overgrowth. Open Dent. J. 2017, 11, 420–435. [Google Scholar] [CrossRef] [Green Version]
- Miranda, J.; Brunet, L.; Roset, P.; Farre, M.; Mendieta, C. Reliability of two measurement indices for gingival enlargement. J. Periodontal Res. 2012, 47, 776–782. [Google Scholar] [CrossRef]
- Bharti, V.; Bansal, C. Drug-induced gingival overgrowth: The nemesis of gingiva unravelled. J. Indian Soc. Periodontol. 2013, 17, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Eslami, M.; Baghaii, F.; Jalayer Nadery, N. An Investigation on gingival hyperplasia induced by nifedipine. J. Dent. 2004, 1, 33–37. [Google Scholar]
- Sunil, P.M.; Nalluswami, J.S.; Sanghar, S.J.; Joseph, I. Nifedipine-induced gingival enlargement: Correlation with dose and oral hygiene. J. Pharm. Bioallied Sci. 2012, 4, S191–S193. [Google Scholar] [CrossRef] [PubMed]
- Trackman, P.; Kantarci, A. Molecular and clinical aspects of drug-induced gingival overgrowth. J. Dent. Res. 2015, 94, 540–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanno, C.M.; De Oliveira, J.A.; Ervolino, E.; Soubhia, A.M.P. Effects of cyclosporin, nifedipine and phenytoin on gingival myofibroblast transdifferentiation in monkeys. J. Appl. Oral Sci. 2018, 27, e20180135. [Google Scholar] [CrossRef] [Green Version]
- Dannewitz, B.; Edrich, C.; Tomakidi, P.; Kohl, A.; Gabbert, O.; Steinberg, T.; Staehle, H.-J. Elevated levels of gene expression for collagen and decorin in human gingival overgrowth. J. Clin. Periodontol. 2006, 33, 510–516. [Google Scholar] [CrossRef]
- Kanno, C.M.; Oliveira, J.A.; Garcia, J.F.; Castro, A.L.; Crivelini, M.M. Effects of Cyclosporin, Phenytoin, and Nifedipine on the Synthesis and Degradation of Gingival Collagen in Tufted Capuchin Monkeys (Cebus apella): Histochemical and MMP-1 and -2 and Collagen I Gene Expression Analyses. J. Periodontol. 2008, 79, 114–122. [Google Scholar] [CrossRef]
- Lauritano, D.; Palmieri, A.; Lucchese, A.; Di Stasio, D.; Moreo, G.; Carinci, F. Role of Cyclosporine in Gingival Hyperplasia: An In Vitro Study on Gingival Fibroblasts. Int. J. Mol. Sci. 2020, 21, 595. [Google Scholar] [CrossRef] [Green Version]
- Lauritano, D.; Lucchese, A.; Di Stasio, D.; Della Vella, F.; Cura, F.; Palmieri, A.; Carinci, F. Molecular Aspects of Drug-Induced Gingival Overgrowth: An In Vitro Study on Amlodipine and Gingival Fibroblasts. Int. J. Mol. Sci. 2019, 20, 2047. [Google Scholar] [CrossRef] [Green Version]
- Lauritano, D.; Moreo, G.; Limongelli, L.; Tregambi, E.; Palmieri, A.; Carinci, F. Drug-Induced Gingival Overgrowth: A Pilot Study on the Effect of Diphenylhydantoin and Gabapentin on Human Gingival Fibroblasts. Int. J. Environ. Res. Public Heal. 2020, 17, 8229. [Google Scholar] [CrossRef]
- Pre-treatment with berberine enhances effect of 5-fluorouracil and cisplatin in HEP2 laryngeal cancer cell line. J. Biol. Regul. Homeost. Agents. 2018, 32 (2 Suppl. 1), 167–177.
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2-ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Umeizudike, K.A.; Olawuyi, A.B.; Umeizudike, T.I.; Olusegun-Joseph, A.D.; Bello, B.T. Effect of Calcium Channel Blockers on Gingival Tissues in Hypertensive Patients in Lagos, Nigeria: A Pilot Study. Contemp. Clin. Dent. 2017, 8, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Barclay, S.; Thomason, J.M.; Idle, J.R.; Seymour, R.A. The incidence and severity of nifedipine-induced gingival overgrowth. J. Clin. Periodontol. 1992, 19, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Livada, R.; Shiloah, J. Calcium channel blocker-induced gingival enlargement. J. Hum. Hypertens. 2014, 28, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.S.; Arany, P.R. Mechanism of drug-induced gingival overgrowth revisited: A unifying hypothesis. Oral Dis. 2015, 21, e51–e61. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Khalil, R.A. Matrix metalloproteinases, vascular remodeling, and vascular disease. Adv. Pharmacol. 2018, 81, 241–330. [Google Scholar] [CrossRef] [PubMed]
- Lauritano, D.; Moreo, G.; Limongelli, L.; Palmieri, A.; Carinci, F. Drug-Induced Gingival Overgrowth: The Effect of Cyclosporin A and Mycophenolate Mophetil on Human Gingival Fibroblasts. Biomedicines 2020, 8, 221. [Google Scholar] [CrossRef]
- Kataoka, M.; Shimizu, Y.; Kunikiyo, K.; Asahara, Y.; Yamashita, K.; Ninomiya, M.; Morisaki, I.; Oshaki, Y.; Kido, J.-I.; Nagata, T. Cyclosporin A decreases the degradation of type I collagen in rat gingival overgrowth. J. Cell Physiol. 2000, 182, 351–358. [Google Scholar] [CrossRef]
- Kato, T.; Okahashi, N.; Kawai, S.; Kato, T.; Inaba, H.; Morisaki, I.; Amano, A. Impaired Degradation of Matrix Collagen in Human Gingival Fibroblasts by the Antiepileptic Drug Phenytoin. J. Periodontol. 2005, 76, 941–950. [Google Scholar] [CrossRef]
- Kato, T.; Okahashi, N.; Ohno, T.; Inaba, H.; Kawai, S.; Amano, A. Effect of phenytoin on collagen accumulation by human gingival fibroblasts exposed to TNF-alphain vitro. Oral Dis. 2006, 12, 156–162. [Google Scholar] [CrossRef]
- Kataoka, M.; Shimizu, Y.; Kunikiyo, K.; Asahara, Y.; Azuma, H.; Sawa, T.; Kido, J.-I.; Nagata, T. Nifedipine Induces Gingival Overgrowth in Rats Through a Reduction in Collagen Phagocytosis by Gingival Fibroblasts. J. Periodontol. 2001, 72, 1078–1083. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Jackson-Boeters, L.; Darling, M.R.; Rieder, M.J.; Hamilton, D. Nifedipine Induces Periostin Expression in Gingival Fibroblasts through TGF-beta. J. Dent. Res. 2013, 92, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Caja, L.; Dituri, F.; Mancarella, S.; Caballero-Diaz, D.; Moustakas, A.; Giannelli, G.; Fabregat, I. TGF-β and the Tissue Microenvironment: Relevance in Fibrosis and Cancer. Int. J. Mol. Sci. 2018, 19, 1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, D.W. Functional role of periostin in development and wound repair: Implications for connective tissue disease. J. Cell Commun. Signal. 2008, 2, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyfuss, J.L.; Veiga, S.S.; Coulson-Thomas, V.J.; Santos, I.A.; Toma, L.; Coletta, R.D.; Nader, H.B. Differences in the expression of glycosaminoglycans in human fibroblasts derived from gingival overgrowths is related to TGF-beta up-regulation. Growth Factors 2009, 28, 24–33. [Google Scholar] [CrossRef]
- Ganesh, P.R. Immunoexpression of interleukin-6 in drug-induced gingival overgrowth patients. Contemp. Clin. Dent. 2016, 7, 140–145. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Protein Summary for NCBI Protein P12830, Cadherin-1. 2021. Available online: https://pubchem.ncbi.nlm.nih.gov/protein/P12830 (accessed on 6 January 2021).
- Kantarci, A.; Nseir, Z.; Kim, Y.-S.; Sume, S.S.; Trackman, P. Loss of Basement Membrane Integrity in Human Gingival Overgrowth. J. Dent. Res. 2011, 90, 887–893. [Google Scholar] [CrossRef] [Green Version]
- Sume, S.S.; Kantarci, A.; Lee, A.; Hasturk, H.; Trackman, P.C. Epithelial to Mesenchymal Transition in Gingival Overgrowth. Am. J. Pathol. 2010, 177, 208–218. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gene | Fold Change | SD | Gene Function |
|---|---|---|---|
| CD44 | 0.64 | 0.08 | Cell-Cell Adhesion |
| CDH1 | 5.62 | 2.06 | Cell-Cell Adhesion |
| COL1A2 | 0.77 | 0.12 | Collagens and Extracellular Matrix Structural constituent |
| COL2A1 | 0.57 | 0.15 | Collagens and Extracellular Matrix Structural constituent |
| COL3A1 | 0.66 | 0.05 | Collagens and Extracellular Matrix Structural constituent |
| COL4A1 | 0.85 | 0.14 | Collagens and Extracellular Matrix Structural constituent |
| COL5A1 | 0.66 | 0.08 | Collagens and Extracellular Matrix Structural constituent |
| COL6A1 | 0.90 | 0.17 | Collagens and Extracellular Matrix Structural constituent |
| COL7A1 | 0.55 | 0.19 | Collagens and Extracellular Matrix Structural constituent |
| COL8A1 | 0.92 | 0.09 | Collagens and Extracellular Matrix Structural constituent |
| COL9A1 | 1.10 | 0.02 | Collagens and Extracellular Matrix Structural constituent |
| COL10A1 | 1.54 | 0.06 | Collagens and Extracellular Matrix Structural constituent |
| COL11A1 | 0.96 | 0.11 | Collagens and Extracellular Matrix Structural constituent |
| CCTNA1 | 0.69 | 0.02 | Cell Adhesion Molecule |
| CTNB | 0.67 | 0.07 | Cell Adhesion Molecule |
| CTNND2 | 0.96 | 0.30 | Cell Adhesion Molecule |
| FN1 | 0.54 | 0.09 | Cell Adhesion Molecule |
| HAS1 | 0.68 | 0.09 | Transmembrane Receptor |
| ILF3 | 0.62 | 0.07 | Transmembrane Receptor |
| ITGA1 | 0.95 | 0.10 | Transmembrane Receptor |
| ITGA2 | 1.19 | 0.18 | Transmembrane Receptor |
| ITGA3 | 0.88 | 0.15 | Transmembrane Receptor |
| ITGA4 | 0.61 | 0.10 | Transmembrane Receptor |
| ITGA5 | 0.70 | 0.03 | Transmembrane Receptor |
| ITGA6 | 0.41 | 0.04 | Transmembrane Receptor |
| ITGA7 | 1.48 | 0.31 | Transmembrane Receptor |
| ITGA8 | 0.59 | 0.06 | Transmembrane Receptor |
| ITGB1 | 0.87 | 0.09 | Transmembrane Receptor |
| ITGB2 | 0.73 | 0.07 | Transmembrane Receptor |
| ITGB4 | 0.23 | 0.03 | Transmembrane Receptor |
| ITGB5 | 0.75 | 0.06 | Transmembrane Receptor |
| LAMA1 | 0.45 | 0.04 | Basement Membrane Constituent |
| LAMA2 | 1.06 | 0.19 | Basement Membrane Constituent |
| LAMA3 | 0.64 | 0.08 | Basement Membrane Constituent |
| LAMB1 | 0.39 | 0.02 | Basement Membrane Constituent |
| LAMB2 | 0.75 | 0.10 | Basement Membrane Constituent |
| LAMB3 | 0.88 | 0.11 | Basement Membrane Constituent |
| MMP2 | 0.73 | 0.10 | Extracellular Matrix Protease |
| MMP3 | 0.90 | 0.08 | Extracellular Matrix Protease |
| MMP7 | 1.03 | 0.42 | Extracellular Matrix Protease |
| MMP8 | 3.98 | 1.47 | Extracellular Matrix Protease |
| MMP9 | 1.04 | 0.35 | Extracellular Matrix Protease |
| MMP10 | 1.24 | 0.05 | Extracellular Matrix Protease |
| MMP11 | 0.14 | 0.05 | Extracellular Matrix Protease |
| MMP12 | 1.20 | 0.13 | Extracellular Matrix Protease |
| MMP13 | 1.14 | 0.19 | Extracellular Matrix Protease |
| MMP14 | 0.96 | 0.07 | Extracellular Matrix Protease |
| MMP15 | 1.90 | 0.08 | Extracellular Matrix Protease |
| MMP16 | 0.38 | 0.04 | Extracellular Matrix Protease |
| MMP24 | 9.68 | 1.05 | Extracellular Matrix Protease |
| MMP26 | 0.31 | 0.01 | Extracellular Matrix Protease |
| TGFB1 | 0.88 | 0.14 | Transforming growth factor β Signaling |
| TGFB2 | 1.20 | 0.12 | Transforming growth factor β Signaling |
| TGFB3 | 0.62 | 0.02 | Transforming growth factor β Signaling |
| TIMP1 | 0.76 | 0.11 | Extracellular Matrix Protease Inhibitor |
| VCAN | 0.75 | 0.03 | Cell Adhesion Molecule |
| RPL13 | 1.00 | 0.00 | Housekeeping gene |
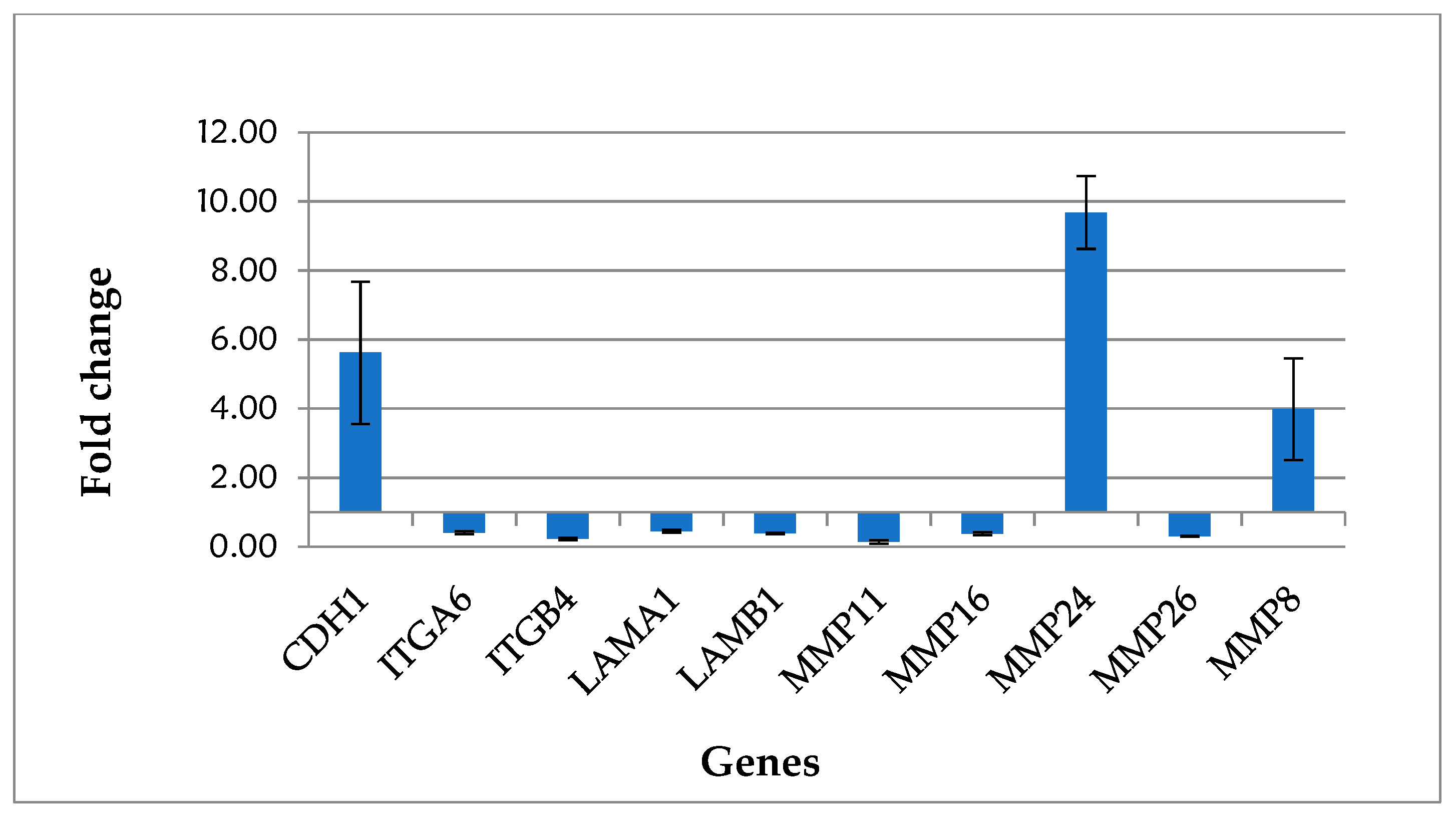
| Gene | Fold Change | SD | Gene Function |
|---|---|---|---|
| CDH1 | 5.62 | 2.06 | Cell-Cell Adhesion |
| ITGA6 | 0.41 | 0.04 | Transmembrane Receptor |
| ITGB4 | 0.23 | 0.03 | Transmembrane Receptor |
| LAMA1 | 0.45 | 0.04 | Basement Membrane Constituent |
| LAMB1 | 0.39 | 0.02 | Basement Membrane Constituent |
| MMP8 | 3.98 | 1.47 | Extracellular Matrix Protease |
| MMP11 | 0.14 | 0.05 | Extracellular Matrix Protease |
| MMP16 | 0.38 | 0.04 | Extracellular Matrix Protease |
| MMP24 | 9.68 | 1.05 | Extracellular Matrix Protease |
| MMP26 | 0.31 | 0.01 | Extracellular Matrix Protease |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauritano, D.; Moreo, G.; Vella, F.D.; Palmieri, A.; Carinci, F.; Petruzzi, M. Biology of Drug-Induced Gingival Hyperplasia: In Vitro Study of the Effect of Nifedipine on Human Fibroblasts. Appl. Sci. 2021, 11, 3287. https://0-doi-org.brum.beds.ac.uk/10.3390/app11073287
Lauritano D, Moreo G, Vella FD, Palmieri A, Carinci F, Petruzzi M. Biology of Drug-Induced Gingival Hyperplasia: In Vitro Study of the Effect of Nifedipine on Human Fibroblasts. Applied Sciences. 2021; 11(7):3287. https://0-doi-org.brum.beds.ac.uk/10.3390/app11073287
Chicago/Turabian StyleLauritano, Dorina, Giulia Moreo, Fedora Della Vella, Annalisa Palmieri, Francesco Carinci, and Massimo Petruzzi. 2021. "Biology of Drug-Induced Gingival Hyperplasia: In Vitro Study of the Effect of Nifedipine on Human Fibroblasts" Applied Sciences 11, no. 7: 3287. https://0-doi-org.brum.beds.ac.uk/10.3390/app11073287