
Performance of Artificial Intelligence Models Designed for Diagnosis, Treatment Planning and Predicting Prognosis of Orthognathic Surgery (OGS)—A Scoping Review

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Eligibility Criteria
2.4. Data Extraction
3. Results
3.1. Qualitative Synthesis of the Included Studies
3.2. Study Characteristics
3.3. Outcome Measures
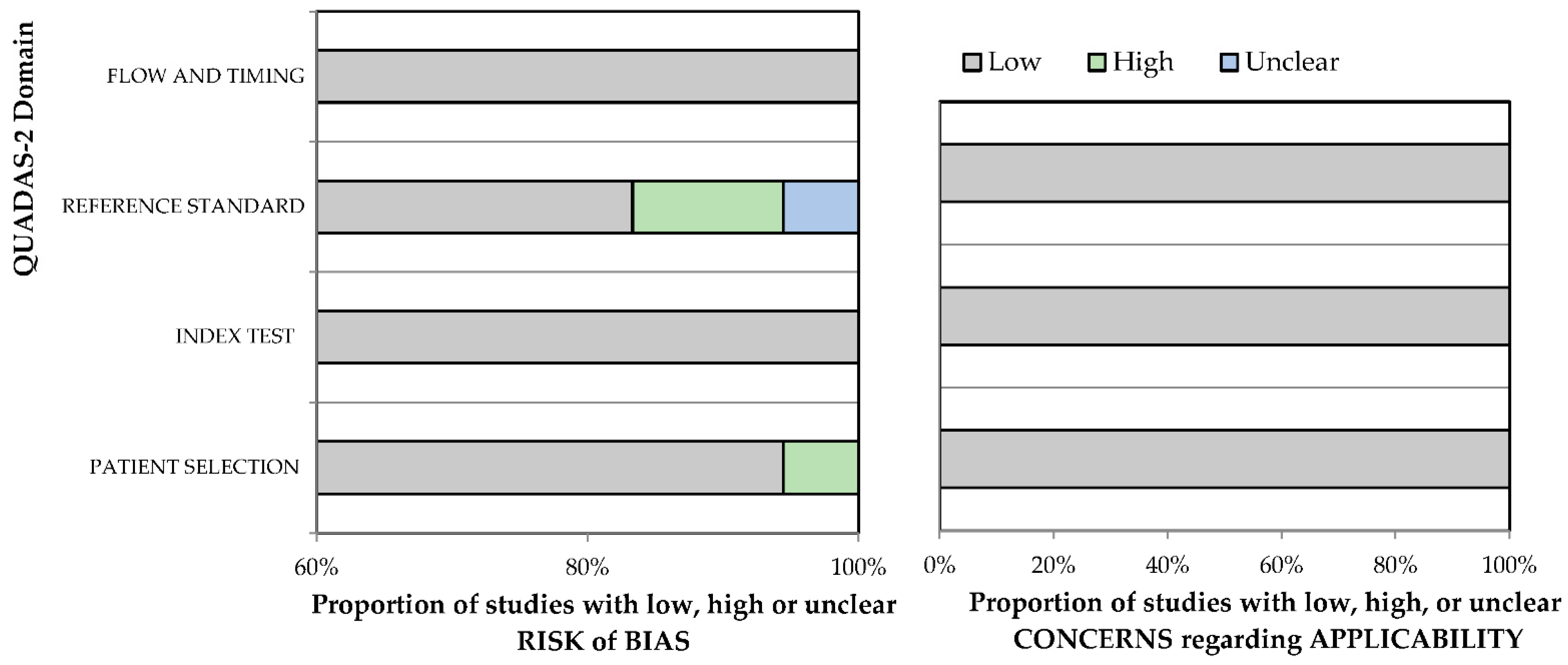
3.4. Risk of Bias Assessment and Applicability Concerns
3.5. Assessment of Strength of Evidence
4. Discussion
4.1. Application of AI in Diagnosis and Determining the Need of OGS
4.2. Application of AI in Predicting Facial Symmetry following OGS
4.3. Application of AI for Planning OGS
4.4. Application of AI for Predicting Blood Loss Prior to OGS
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larsson, P.; Bondemark, L.; Häggman-Henrikson, B. The Impact of Oro-Facial Appearance on Oral Health-Related Quality of Life: A Systematic Review. J. Oral Rehabil. 2021, 48, 271–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naini, F.B.; Donaldson, A.N.A.; McDonald, F.; Cobourne, M.T. Assessing the Influence of Asymmeftry Affecting the Mandible and Chin Point on Perceived Attractiveness in the Orthognathic Patient, Clinician, and Layperson. J. Oral Maxillofac. Surg. 2012, 70, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.H.; Mitroff, S.R.; Clark, K.; Proffit, W.R.; Lee, J.Y.; Nguyen, T.T. Face Symmetry Assessment Abilities: Clinical Implications for Diagnosing Asymmetry. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 663–671. [Google Scholar] [CrossRef] [Green Version]
- Olivetti, E.C.; Nicotera, S.; Marcolin, F.; Vezzetti, E.; Sotong, J.P.A.; Zavattero, E.; Ramieri, G. 3D Soft-Tissue Prediction Methodologies for Orthognathic Surgery—A Literature Review. Appl. Sci. 2019, 9, 4550. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F.; Yuan, P.; Chen, K.-C.; Li, J.; Zhang, X.; Tang, Z.; Alfi, D.M. Algorithm for Planning a Double-Jaw Orthognathic Surgery Using a Computer-Aided Surgical Simulation (CASS) Protocol. Part 1: Planning Sequence. Int. J. Oral Maxillofac. Surg. 2015, 44, 1431–1440. [Google Scholar] [CrossRef] [Green Version]
- Ho, C.-T.; Lin, H.-H.; Liou, E.J.W.; Lo, L.-J. Three-Dimensional Surgical Simulation Improves the Planning for Correction of Facial Prognathism and Asymmetry: A Qualitative and Quantitative Study. Sci. Rep. 2017, 7, 40423. [Google Scholar] [CrossRef]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F. New Clinical Protocol to Evaluate Craniomaxillofacial Deformity and Plan Surgical Correction. J. Oral Maxillofac. Surg. 2009, 67, 2093–2106. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.-Y.; Lin, H.-H.; Lo, L.-J.; Ho, C.-T. Postoperative Outcomes of Two- and Three-Dimensional Planning in Orthognathic Surgery: A Comparative Study. J. Plast. Reconstr. Aesthet. Surg. 2017, 70, 1101–1111. [Google Scholar] [CrossRef]
- Lin, H.-H.; Lonic, D.; Lo, L.-J. 3D Printing in Orthognathic Surgery—A Literature Review. J. Formos. Med. Assoc. 2018, 117, 547–558. [Google Scholar] [CrossRef]
- Alkhayer, A.; Piffkó, J.; Lippold, C.; Segatto, E. Accuracy of Virtual Planning in Orthognathic Surgery: A Systematic Review. Head Face Med. 2020, 16, 34. [Google Scholar] [CrossRef]
- Medeiros, F.A.; Jammal, A.A.; Thompson, A.C. From Machine to Machine: An OCT-Trained Deep Learning Algorithm for Objective Quantification of Glaucomatous Damage in Fundus Photographs. Ophthalmology 2019, 126, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Yao, Z.; Huang, Y.; Yu, Y.; Wang, Y.; Liu, Y.; Mao, R.; Li, F.; Xiao, Y.; Wang, Y.; et al. Deep Learning Radiomics Can Predict Axillary Lymph Node Status in Early-Stage Breast Cancer. Nat. Commun. 2020, 11, 1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-Level Classification of Skin Cancer with Deep Neural Networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Xiao, C.; Huang, Y.; Hassan, H.; Huang, B. Deep Learning Applications in Computed Tomography Images for Pulmonary Nodule Detection and Diagnosis: A Review. Diagnostics 2022, 12, 298. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.; Yong, T.-H.; Kang, S.-R.; Kim, J.-E.; Huh, K.-H.; Heo, M.-S.; Lee, S.-S.; Choi, S.-C.; Yi, W.-J. Automatic Diagnosis for Cysts and Tumors of Both Jaws on Panoramic Radiographs Using a Deep Convolution Neural Network. Dentomaxillofac. Radiol. 2020, 49, 20200185. [Google Scholar] [CrossRef]
- Hung, K.; Montalvao, C.; Tanaka, R.; Kawai, T.; Bornstein, M.M. The Use and Performance of Artificial Intelligence Applications in Dental and Maxillofacial Radiology: A Systematic Review. Dentomaxillofac. Radiol. 2020, 49, 20190107. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Sayres, R.; Taly, A.; Rahimy, E.; Blumer, K.; Coz, D.; Hammel, N.; Krause, J.; Narayanaswamy, A.; Rastegar, Z.; Wu, D.; et al. Using a Deep Learning Algorithm and Integrated Gradients Explanation to Assist Grading for Diabetic Retinopathy. Ophthalmology 2019, 126, 552–564. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Kim, D.-H.; Jeong, S.-N.; Choi, S.-H. Detection and Diagnosis of Dental Caries Using a Deep Learning-Based Convolutional Neural Network Algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef]
- Chang, H.-J.; Lee, S.-J.; Yong, T.-H.; Shin, N.-Y.; Jang, B.-G.; Kim, J.-E.; Huh, K.-H.; Lee, S.-S.; Heo, M.-S.; Choi, S.-C.; et al. Deep Learning Hybrid Method to Automatically Diagnose Periodontal Bone Loss and Stage Periodontitis. Sci. Rep. 2020, 10, 7531. [Google Scholar] [CrossRef]
- Yang, H.; Jo, E.; Kim, H.J.; Cha, I.-H.; Jung, Y.-S.; Nam, W.; Kim, J.-Y.; Kim, J.-K.; Kim, Y.H.; Oh, T.G.; et al. Deep Learning for Automated Detection of Cyst and Tumors of the Jaw in Panoramic Radiographs. J. Clin. Med. 2020, 9, 1839. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Kim, D.-H.; Jeong, S.-N.; Choi, S.-H. Diagnosis and Prediction of Periodontally Compromised Teeth Using a Deep Learning-Based Convolutional Neural Network Algorithm. J. Periodontal Implant Sci. 2018, 48, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, T.A.; Alabousi, M.; Skidmore, B.; Korevaar, D.A.; Bossuyt, P.M.M.; Moher, D.; Thombs, B.; McInnes, M.D.F. Recommendations for Reporting of Systematic Reviews and Meta-Analyses of Diagnostic Test Accuracy: A Systematic Review. Syst. Rev. 2017, 6, 194. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-H.; Ko, E.W.-C.; Liu, L. Improving the Video Imaging Prediction of Postsurgical Facial Profiles with an Artificial Neural Network. J. Dent. Sci. 2009, 4, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.-H.; Lo, L.-J.; Chiang, W.-C.; Chen, C.-F. An Automatic Assessment of Facial Symmetry before and after Orthognathic Surgery Based on Three-Dimensional Contour Features using Deep Learning System. Available online: http://www.iraj.in/journal/journal_file/journal_pdf/6-462-153034747838-41.pdf (accessed on 1 February 2022).
- Patcas, R.; Bernini, D.A.J.; Volokitin, A.; Agustsson, E.; Rothe, R.; Timofte, R. Applying Artificial Intelligence to Assess the Impact of Orthognathic Treatment on Facial Attractiveness and Estimated Age. Int. J. Oral Maxillofac. Surg. 2019, 48, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.H.; Yun, J.P.; Yeom, H.-G.; Lim, H.J.; Lee, J.; Kim, B.C. Deep Learning Based Discrimination of Soft Tissue Profiles Requiring Orthognathic Surgery by Facial Photographs. Sci. Rep. 2020, 10, 16235. [Google Scholar] [CrossRef]
- Tanikawa, C.; Yamashiro, T. Development of Novel Artificial Intelligence Systems to Predict Facial Morphology after Orthognathic Surgery and Orthodontic Treatment in Japanese Patients. Sci. Rep. 2021, 11, 15853. [Google Scholar] [CrossRef]
- Lin, H.-H.; Chiang, W.-C.; Yang, C.-T.; Cheng, C.-T.; Zhang, T.; Lo, L.-J. On Construction of Transfer Learning for Facial Symmetry Assessment before and after Orthognathic Surgery. Comput. Methods Programs Biomed. 2021, 200, 105928. [Google Scholar] [CrossRef]
- Lo, L.-J.; Yang, C.-T.; Ho, C.-T.; Liao, C.-H.; Lin, H.-H. Automatic Assessment of 3-Dimensional Facial Soft Tissue Symmetry before and after Orthognathic Surgery Using a Machine Learning Model: A Preliminary Experience. Ann. Plast. Surg. 2021, 86, S224–S228. [Google Scholar] [CrossRef]
- Ter Horst, R.; van Weert, H.; Loonen, T.; Bergé, S.; Vinayahalingam, S.; Baan, F.; Maal, T.; de Jong, G.; Xi, T. Three-Dimensional Virtual Planning in Mandibular Advancement Surgery: Soft Tissue Prediction Based on Deep Learning. J. Craniomaxillofac. Surg. 2021, 49, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-I.; Jung, S.-K.; Baek, S.-H.; Lim, W.H.; Ahn, S.-J.; Yang, I.-H.; Kim, T.-W. Artificial Intelligent Model with Neural Network Machine Learning for the Diagnosis of Orthognathic Surgery. J. Craniofac. Surg. 2019, 30, 1986–1989. [Google Scholar] [CrossRef] [PubMed]
- Knoops, P.G.M.; Papaioannou, A.; Borghi, A.; Breakey, R.W.F.; Wilson, A.T.; Jeelani, O.; Zafeiriou, S.; Steinbacher, D.; Padwa, B.L.; Dunaway, D.J.; et al. A Machine Learning Framework for Automated Diagnosis and Computer-Assisted Planning in Plastic and Reconstructive Surgery. Sci. Rep. 2019, 9, 13597. [Google Scholar] [CrossRef]
- Lin, G.; Kim, P.-J.; Baek, S.-H.; Kim, H.-G.; Kim, S.-W.; Chung, J.-H. Early Prediction of the Need for Orthognathic Surgery in Patients with Repaired Unilateral Cleft Lip and Palate Using Machine Learning and Longitudinal Lateral Cephalometric Analysis Data. J. Craniofac. Surg. 2021, 32, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.; Yeom, H.-G.; Lee, G.H.; Yun, J.P.; Jeong, S.H.; Lee, J.H.; Kim, H.K.; Kim, B.C. Deep Learning Based Prediction of Necessity for Orthognathic Surgery of Skeletal Malocclusion Using Cephalogram in Korean Individuals. BMC Oral Health 2021, 21, 130. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Park, J.-B.; Chang, M.-S.; Ryu, J.-J.; Lim, W.H.; Jung, S.-K. Influence of the Depth of the Convolutional Neural Networks on an Artificial Intelligence Model for Diagnosis of Orthognathic Surgery. J. Pers. Med. 2021, 11, 356. [Google Scholar] [CrossRef]
- Stehrer, R.; Hingsammer, L.; Staudigl, C.; Hunger, S.; Malek, M.; Jacob, M.; Meier, J. Machine Learning Based Prediction of Perioperative Blood Loss in Orthognathic Surgery. J. Craniomaxillofac. Surg. 2019, 47, 1676–1681. [Google Scholar] [CrossRef]
- Xiao, D.; Lian, C.; Deng, H.; Kuang, T.; Liu, Q.; Ma, L.; Kim, D.; Lang, Y.; Chen, X.; Gateno, J.; et al. Estimating Reference Bony Shape Models for Orthognathic Surgical Planning Using 3D Point-Cloud Deep Learning. IEEE J. Biomed. Health Inform. 2021, 25, 2958–2966. [Google Scholar] [CrossRef]
- Xiao, D.; Deng, H.; Lian, C.; Kuang, T.; Liu, Q.; Ma, L.; Lang, Y.; Chen, X.; Kim, D.; Gateno, J.; et al. Unsupervised Learning of Reference Bony Shapes for Orthognathic Surgical Planning with a Surface Deformation Network. Med. Phys. 2021, 48, 7735–7746. [Google Scholar] [CrossRef]
- Dot, G.; Schouman, T.; Dubois, G.; Rouch, P.; Gajny, L. Fully Automatic Segmentation of Craniomaxillofacial CT Scans for Computer-Assisted Orthognathic Surgery Planning Using the NnU-Net Framework. Eur. Radiol. 2022, 32, 3639–3648. [Google Scholar] [CrossRef]
- Lee, K.-S.; Ryu, J.-J.; Jang, H.S.; Lee, D.-Y.; Jung, S.-K. Deep Convolutional Neural Networks Based Analysis of Cephalometric Radiographs for Differential Diagnosis of Orthognathic Surgery Indications. Appl. Sci. 2020, 10, 2124. [Google Scholar] [CrossRef] [Green Version]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE Approach in Systematic Reviews and Guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Casalegno, F.; Newton, T.; Daher, R.; Abdelaziz, M.; Lodi-Rizzini, A.; Schürmann, F.; Krejci, I.; Markram, H. Caries Detection with Near-Infrared Transillumination Using Deep Learning. J. Dent. Res. 2019, 98, 1227–1233. [Google Scholar] [CrossRef] [Green Version]
- Devito, K.L.; de Souza Barbosa, F.; Felippe Filho, W.N. An Artificial Multilayer Perceptron Neural Network for Diagnosis of Proximal Dental Caries. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.; Voss, M.W.; Rosales, M.N.; Li, W.; Su, W.; Xu, J.; Bounsanga, J.; Ruiz-Negrón, B.; Lauren, E.; Licari, F.W. Application of Machine Learning for Diagnostic Prediction of Root Caries. Gerodontology 2019, 36, 395–404. [Google Scholar] [CrossRef]
- Murata, M.; Ariji, Y.; Ohashi, Y.; Kawai, T.; Fukuda, M.; Funakoshi, T.; Kise, Y.; Nozawa, M.; Katsumata, A.; Fujita, H.; et al. Deep-Learning Classification Using Convolutional Neural Network for Evaluation of Maxillary Sinusitis on Panoramic Radiography. Oral Radiol. 2019, 35, 301–307. [Google Scholar] [CrossRef]
- Kise, Y.; Ikeda, H.; Fujii, T.; Fukuda, M.; Ariji, Y.; Fujita, H.; Katsumata, A.; Ariji, E. Preliminary Study on the Application of Deep Learning System to Diagnosis of Sjögren’s Syndrome on CT Images. Dentomaxillofac. Radiol. 2019, 48, 20190019. [Google Scholar] [CrossRef] [PubMed]
- Ariji, Y.; Sugita, Y.; Nagao, T.; Nakayama, A.; Fukuda, M.; Kise, Y.; Nozawa, M.; Nishiyama, M.; Katumata, A.; Ariji, E. CT Evaluation of Extranodal Extension of Cervical Lymph Node Metastases in Patients with Oral Squamous Cell Carcinoma Using Deep Learning Classification. Oral Radiol. 2020, 36, 148–155. [Google Scholar] [CrossRef]
- Lee, K.-S.; Jung, S.-K.; Ryu, J.-J.; Shin, S.-W.; Choi, J. Evaluation of Transfer Learning with Deep Convolutional Neural Networks for Screening Osteoporosis in Dental Panoramic Radiographs. J. Clin. Med. 2020, 9, 392. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-S.; Adhikari, S.; Liu, L.; Jeong, H.-G.; Kim, H.; Yoon, S.-J. Osteoporosis Detection in Panoramic Radiographs Using a Deep Convolutional Neural Network-Based Computer-Assisted Diagnosis System: A Preliminary Study. Dentomaxillofac. Radiol. 2019, 48, 20170344. [Google Scholar] [CrossRef]
- Xie, X.; Wang, L.; Wang, A. Artificial Neural Network Modeling for Deciding If Extractions Are Necessary Prior to Orthodontic Treatment. Angle Orthod. 2010, 80, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thanathornwong, B. Bayesian-Based Decision Support System for Assessing the Needs for Orthodontic Treatment. Healthc. Inform. Res. 2018, 24, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Saghiri, M.A.; Asgar, K.; Boukani, K.K.; Lotfi, M.; Aghili, H.; Delvarani, A.; Karamifar, K.; Saghiri, A.M.; Mehrvarzfar, P.; Garcia-Godoy, F. A New Approach for Locating the Minor Apical Foramen Using an Artificial Neural Network: Artificial Neural Network in Dentistry. Int. Endod. J. 2012, 45, 257–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johari, M.; Esmaeili, F.; Andalib, A.; Garjani, S.; Saberkari, H. Detection of Vertical Root Fractures in Intact and Endodontically Treated Premolar Teeth by Designing a Probabilistic Neural Network: An Ex Vivo Study. Dentomaxillofac. Radiol. 2017, 46, 20160107. [Google Scholar] [CrossRef] [Green Version]
- Krois, J.; Ekert, T.; Meinhold, L.; Golla, T.; Kharbot, B.; Wittemeier, A.; Dörfer, C.; Schwendicke, F. Deep Learning for the Radiographic Detection of Periodontal Bone Loss. Sci. Rep. 2019, 9, 8495. [Google Scholar] [CrossRef]
- Aubreville, M.; Knipfer, C.; Oetter, N.; Jaremenko, C.; Rodner, E.; Denzler, J.; Bohr, C.; Neumann, H.; Stelzle, F.; Maier, A. Automatic Classification of Cancerous Tissue in Laserendomicroscopy Images of the Oral Cavity Using Deep Learning. Sci. Rep. 2017, 7, 11979. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Ren, Y.; Gao, Y.; Tang, Z.; Chen, K.-C.; Li, J.; Shen, S.G.F.; Yan, J.; Lee, P.K.M.; Chow, B.; et al. Estimating Patient-Specific and Anatomically Correct Reference Model for Craniomaxillofacial Deformity via Sparse Representation: Estimating Patient-Specific and Anatomically Correct Reference Model. Med. Phys. 2015, 42, 5809–5816. [Google Scholar] [CrossRef] [Green Version]
- Piñeiro-Aguilar, A.; Somoza-Martín, M.; Gandara-Rey, J.M.; García-García, A. Blood Loss in Orthognathic Surgery: A Systematic Review. J. Oral Maxillofac. Surg. 2011, 69, 885–892. [Google Scholar] [CrossRef]
- Olsen, J.J.; Ingerslev, J.; Thorn, J.J.; Pinholt, E.M.; Gram, J.B.; Sidelmann, J.J. Can Preoperative Sex-Related Differences in Hemostatic Parameters Predict Bleeding in Orthognathic Surgery? J. Oral Maxillofac. Surg. 2016, 74, 1637–1642. [Google Scholar] [CrossRef]
- Thastum, M.; Andersen, K.; Rude, K.; Nørholt, S.E.; Blomlöf, J. Factors Influencing Intraoperative Blood Loss in Orthognathic Surgery. Int. J. Oral Maxillofac. Surg. 2016, 45, 1070–1073. [Google Scholar] [CrossRef]
- Salma, R.G.; Al-Shammari, F.M.; Al-Garni, B.A.; Al-Qarzaee, M.A. Operative Time, Blood Loss, Hemoglobin Drop, Blood Transfusion, and Hospital Stay in Orthognathic Surgery. Oral Maxillofac. Surg. 2017, 21, 259–266. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Research question | What are the AI applications designed for OGS, and its performance in diagnosis, planning and prediction of the prognosis of OGS |
| Population | Patients who underwent investigations for OGS (Maxillary Osteotomy, Mandibular Osteotomy, Bilateral Sagittal Split Osteotomy (BSSO), Genioplasty, Le Fort 1 Osteotomy) |
| Intervention | AI applications for diagnosis, treatment planning and prediction of the prognosis of OGS |
| Comparison | Specialist opinions, Reference standards |
| Outcome | Measurable or predictive outcomes such as Accuracy, Sensitivity, Specificity, ROC = Receiver Operating Characteristic curve, AUC = Area Under the Curve, ICC = Intraclass Correlation Coefficient, Statistical Significance, F1 Scores, vDSC: Volumetric Dice Similarity Coefficient, sDSC: Surface Dice Similarity Coefficient |
| Serial No. | Authors | Year of Publication | Study Design | Algorithm Architecture | Objective of the Study | No. of Patients/Images/Photographs for Testing | Study Factor | Modality | Comparison if any | Evaluation Accuracy /Average Accuracy/Statistical Significance | Results (+)Effective, (−)Non Effective (N) Neutral | Outcomes | Authors Suggestions/Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | C.H Lu et al. [25] | 2009 | Retrospective Cohort study | ANNs | To evaluate post-OGS image prediction using the AI model | 30 subjects | Landmarks | Lateral Cephalogram Facial images | Compared with actual profile post- surgery | Most of the prediction errors were <1 mm | (+)Effective | ANNs are able to predict the post-surgical facial profile | The model might be more reliable and accurate in predictions if more variables are considered |
| 2 | H. H Lin et al. [26] | 2018 | Case Control study | CNNs | To assess the degree of facial asymmetry in patients who had undergone OGS | 100 subjects | Landmarks | 3D facial images | Specialist | 78.85% accuracy on held-out test patterns facial symmetry degree assessment within 1 degree was 98.63% Assessment of pre-surgery and post-surgery: the predications were statistically significant p < 0.05 | (+)Effective | This model is an efficient decision making tool | This automated model can be useful in clinics for assessing the pre and post-operative facial symmetry |
| 3 | R. Patcas et al. [27] | 2019 | Case Control study | CNNs | AI model for assessing the impact of OGS on facial attractiveness and estimating the age | 146 subjects (2164 photographs) | Landmarks | Facial photographs | Compared with actual profile post- surgery | 66.4% patients appearance improved post-surgery which was in comparison with the actual improvement post-surgery 74.7% | (+)Effective | This model is efficient in scoring face attractiveness and apparent age | This model outperformed past approaches and can be considered for clinical application. |
| 4 | H-Il Choi et al. [33] | 2019 | Case Control study | ANNs | Decision making on surgery/non surgery, type of surgery and assessing the need for extractions | 316 subjects (204 for training 112 for testing) | Landmarks | Lateral Cephalogram | 1 Orthodontic specialist | ICC were ranging between 0.97–0.99. Accuracy of 96% for surgery/non-surgery decision making 91% for diagnosing type of surgery and decision making in extractions | (+)Effective | ANN model demonstrated excellent reliability | This model could be applied in the diagnosis of OGS |
| 5 | P. G. M. Knoops et al. [34] | 2019 | Retrospective Cohort study | CNNs | Automated model for diagnosing and clinical decision making of OGS | Trained with 4261 3D Facial images Tested with 151 subjects (273 3D Facial images) | Landmarks | Data sets 3D face scans | Not mentioned | 95.5% sensitivity, 95.2% specificity, mean accuracy of 1.1 ± 0.3 mm | (+)Effective | Efficient in diagnosing, risk stratification, treatment simulation. | The model is efficient in clinical decision making |
| 6 | R.Stehrer et al. [38] | 2019 | Case Control study | CNNs | To predict perioperative blood loss prior to OGS | 950 subjects 80% for training 20% for testing | Correlation between actual and predicted perioperative blood loss | Data sets | Data on actual blood loss | Statistical significance (p < 0.001). | (+)Effective | Efficient in predicting perioperative blood loss | This model is helpful in predicting blood loss prior to OGS |
| 7 | S.H.Jeong et al. [28] | 2020 | Interventional Cohort study | CNNs | To determine the ability of the CNN model in predicting soft tissue profiles requiring OGS | 822 subjects 411 requiring OGS 411 not requiring OGS | Landmarks | Facial photographs | 2 orthodontist, 3 maxillofacial surgeons, 1 maxillofacial radiologist. | Accuracy = 0.893, Precision =0.912, recall = 0.867, and F1 score = 0.889 | (+)Effective | Efficient in predicting soft tissue profiles requiring orthognathic surgery | This model can judge soft tissue profiles requiring OGS using facial photographs |
| 8 | K.S. Lee et al. [42] | 2020 | Cohort study | DCNNs | To evaluate the DCNN-based model designed for differential diagnosis of OGS | 220 cases for training and 73 for validation | Landmarks | Lateral Cephalogram | Four different models Modified-Alexnet, MobileNet, and Resnet50 were used | Modified-Alexnet, MobileNet, and Resnet50 demonstrated AUC 0.969, 0.908 0.923. Accuracy 0.919, 0.838, 0.838. Sensitivity 0.852, 0.761, 0.750. Specificity 0.973, 0.931, 0.944 ‘respectively’ | (+)Effective | Modified-Alexnet demonstrated the highest level of performance | These models can be successfully applied for differential diagnosis of OGS |
| 9 | C.Tanikawa et al. [29] | 2020 | Case Control study | ANNs | AI model for predicting the facial morphology after OGS and orthodontic treatment | 137 subjects (72 OGS and 65 orthodontic treatment) | Landmarks | Lateral cephalogram and 3-D facial images | 2 AI models (System S) for OGS and (System E) for orthodontic treatment | Success rates, when system error of <1 mm, were 54% and 98%and for system error of <2 mm success rates were 100% for both | (+)Effective | Success rate for the models was 100% when system error was set of <2 mm | These models are clinically acceptable for predicting facial morphology |
| 10 | D. Xiao et al. [39] | 2021 | Case Control study | CNNs | AI model for OGS planning | CT scans of 47 normal subjects for training, 24 CT scans for testing | Landmarks | CT Scans Clinical data sets | Landmark-based sparse representation | AI model was significantly more accurate (p < 0.05) than LSR | (+)Effective | The model demonstrated significant performance improvements | This AI -based model generates accurate shape models that meet clinical standards |
| 11 | D. Xiao et al. [40] | 2021 | Cohort study | CNNs | AI model DefNet for estimating patient-specific reference models for planning OGS. | CT scans of 47 subjects | Landmarks | CT Scans Clinical data sets | Sparse representation method | Vertex distance (VD), edge-length distance (ED), were significantly smaller than the SR method (p < 0.05). | (+)Effective | The model demonstrated comparable performance for the synthetic data and better performance for the real data. | This projected model outperforms an existing sparse representation method |
| 12 | G. Lin et al. [35] | 2021 | Cohort study | CNNs | AI model for determining the need for OGS in Unilateral Cleft Lip and Palate patients | 56 subjects | Landmarks | Lateral Cephalogram | Boruta method | Accuracy of 87.4%. F1-score of 0.714, Sensitivity 97.83%, Specificity 90.00% | (+)Effective | The XGBoost algorithm demonstracted high accuracy in prediction | This model can be applied for predicting the need for OGS in correcting the sagittal discrepancies |
| 13 | H.H.Lin et al. [30] | 2021 | Case Control study | CNNs | AI model for assessing facial symmetry before and after OGS | 71 subjects | Landmarks | CBCT images | 4 orthodontists and 4 plastic surgeons and also with previously reported models VGG16, VGG19, ResNet50, and Xception | Accuracy of 90%. | (+)Effective | Xception model and the constant data amplification approach achieved the highest accuracy | This model successfully demonstrated prediction of facial asymmetry before and after surgery |
| 14 | L.J. Lo et al. [31] | 2021 | Retrospective Cohort study | CNNs | AI model for assessing facial soft tissue symmetry before and after OGS | 158 subjects | Landmarks | 3-D facial photographs | Pre and post- operative | Mean score significant improvements from2.74 to 3.52 | (+)Effective | The model demonstrated results that can aid clinicians in assessing facial symmetry | This model can be integrated as a 3D surgical simulation model for effective treatment planning |
| 15 | R.Horst et al. [32] | 2021 | Case Control study | CNNs | AI model to predict the virtual soft tissue profile after mandibular advancement surgery | 133 subjects (119 for training, 14 for testing) | Landmarks | 3D photographs and CBCT images | Mass Tensor Model (MTM) | Mean absolute Error was 1.0 ± 0.6 mm and was lower that of MTM, which was statistically significant (p = 0.02), | (+)Effective | This model demonstrated higher accuracy compared to MTM. | This model can successfully predict 3D soft tissue profiles following mandibular advancement surgery. |
| 16 | W.S.Shin et al. [36] | 2021 | Cohort study | CNNs | AI model to predict the need for OGS using cephalogram. | 413 subjects | Landmarks | Cephalogram | 2 orthodontists, 3 maxillofacial surgeons, 1 maxillofacial radiologist. | Accuracy of 0.954, sensitivity of 0.844, and specificity of 0.993 | (+)Effective | This model demonstrated higher accuracy in predicting the need for OGS | This model will assist specialists as well as general dentists in decision making |
| 17 | Y.H Kim et al. [37] | 2021 | Case Control study | CNNs | AI model to diagnose cases requiring orthodontic surgery using 4 models ResNet-18, 34, 50, and 101 | 960 subjects (810 for training, 150 for testing) | Landmarks | Cephalogram | ResNet-18, 34, 50, and 101 | Success rate ResNet-18 = 93.80%, ResNet-34 = 93.60%, ResNet-50 = 91.13%, and ResNet -101was 91.33% AUC for ResNet-18 = 0.979, ResNet-34 = 0.974, ResNet-50 = 0.945, and ResNet -101 = 0.944 | (+)Effective | ResNet-18 and 34 demonstrated high prediction performance accuracy in comparison with the ResNet-50 or 101 models | These models demonstrated good accuracies in predicting the need for 0GS |
| 18 | G. Dot et. al. [41] | 2022 | Cohort study | CNNs | To evaluate the performance of deep learning model for multi-task segmentation of cranio-maxillofacial structures for OGS | CT scans of 453 subjects (300 for training, 153 for testing) | Landmarks | CT Scans | Ground truth segmentations generated by 2 operators | Mean total vDSC and sDSC were 92.24 ± 6.19 and 98.03 ± 2.48 ‘respectively’ | (+)Effective | The AI model demonstrated adequate reliability | This model can be be trained easily using more data sets for better performance |
| Outcome | Inconsistency | Indirectness | Imprecision | Risk of Bias | Strength of Evidence |
|---|---|---|---|---|---|
| Application of AI diagnosis and determining the need of OGS [33,34,35,36,37] | Not Present | Not Present | Not Present | Not Present | ⨁⨁⨁⨁ |
| Application of AI in differential diagnosis of OGS [42]. | Not Present | Not Present | Not Present | Not Present | ⨁⨁⨁⨁ |
| Application of AI for predicting the post-operative facial profiles and facial symmetry [25,26,27,28,29,30,31,32]. | Not Present | Not Present | Not Present | Not Present | ⨁⨁⨁⨁ |
| Application of AI for planning OGS [39,40]. | Not Present | Not Present | Not Present | Present | ⨁⨁⨁◯ |
| Application of segmentation of maxillofacial structures for OGS [41]. | Not Present | Not Present | Not Present | Not Present | ⨁⨁⨁⨁ |
| Application of AI for predicting blood loss prior to OGS [38]. | Not Present | Not Present | Not Present | Present | ⨁⨁⨁◯ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanagar, S.B.; Alfouzan, K.; Awawdeh, M.; Alkadi, L.; Albalawi, F.; Alghilan, M.A. Performance of Artificial Intelligence Models Designed for Diagnosis, Treatment Planning and Predicting Prognosis of Orthognathic Surgery (OGS)—A Scoping Review. Appl. Sci. 2022, 12, 5581. https://0-doi-org.brum.beds.ac.uk/10.3390/app12115581
Khanagar SB, Alfouzan K, Awawdeh M, Alkadi L, Albalawi F, Alghilan MA. Performance of Artificial Intelligence Models Designed for Diagnosis, Treatment Planning and Predicting Prognosis of Orthognathic Surgery (OGS)—A Scoping Review. Applied Sciences. 2022; 12(11):5581. https://0-doi-org.brum.beds.ac.uk/10.3390/app12115581
Chicago/Turabian StyleKhanagar, Sanjeev B., Khalid Alfouzan, Mohammed Awawdeh, Lubna Alkadi, Farraj Albalawi, and Maryam A. Alghilan. 2022. "Performance of Artificial Intelligence Models Designed for Diagnosis, Treatment Planning and Predicting Prognosis of Orthognathic Surgery (OGS)—A Scoping Review" Applied Sciences 12, no. 11: 5581. https://0-doi-org.brum.beds.ac.uk/10.3390/app12115581