
Smart Phone-Based Motion Capture and Analysis: Importance of Operating Envelope Definition and Application to Clinical Use

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Video Capture
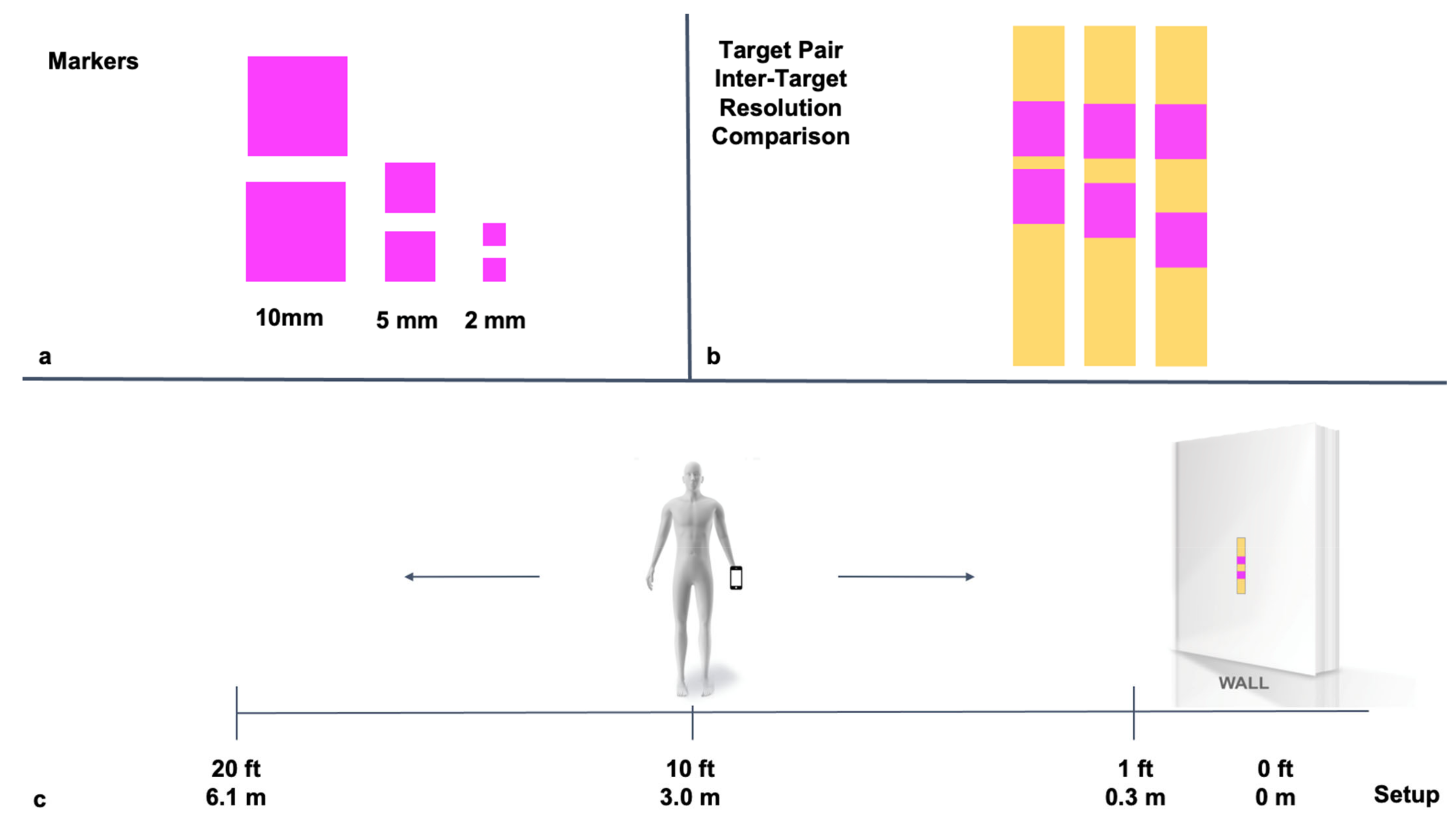
2.3. Protocol 1: Determination of Distance Limit of Target Detection
2.4. Protocol 2: Determination of Distance Limit of Target Pair Detection and Inter-Target Discrimination
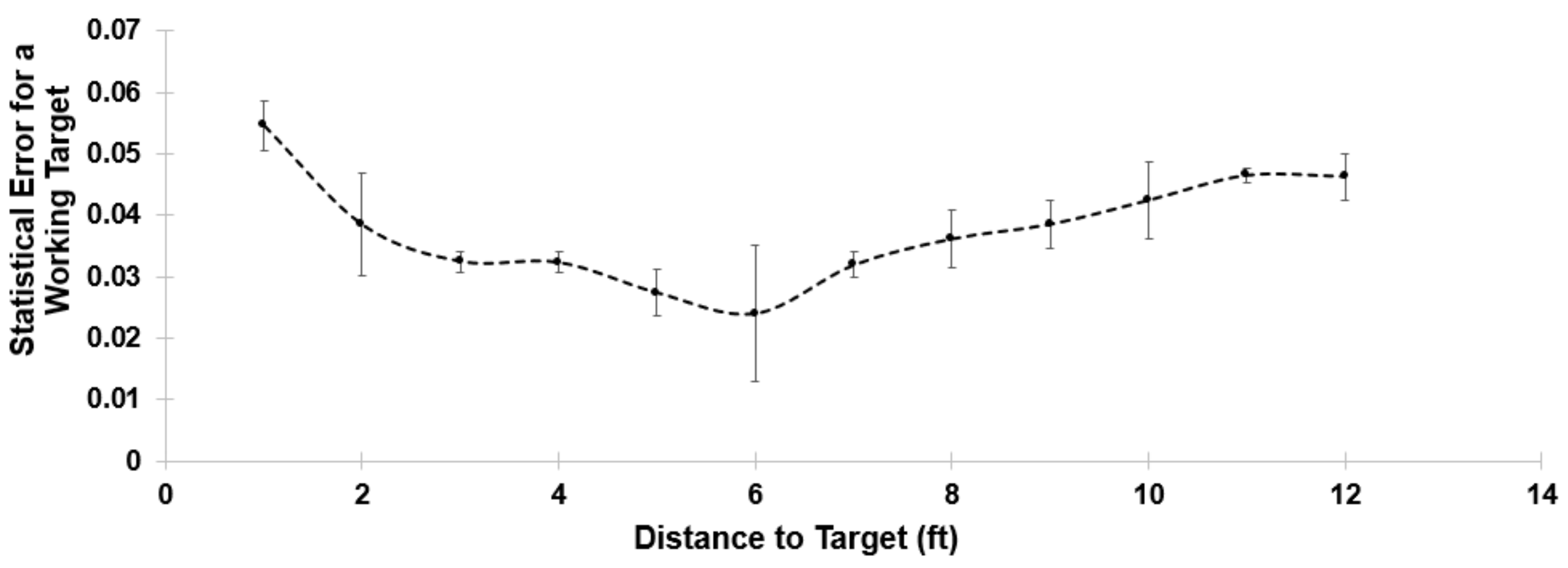
2.5. Protocol 3: Determination of Distance Limit of Moving Target Detection and Resolution (Working Distance)
2.6. Protocol 4: Determination of Effect of Illumination Intensity on Distance Limit of Target Detection and Resolution
2.7. Protocol 5: Application of Smart Phone-Based Motion Detection to Clinical Diagnostic Testing Maneuvers
2.8. Data Processing and Analysis
2.9. Statistical Analysis
2.10. Distance Limit of Target Detection and Target Resolution
2.11. Inter-Target Resolution
2.12. Motion
2.13. Illumination
2.14. Clinical Utility Assessment
3. Results
3.1. Target Resolution
3.2. Inter-Target Discrimination and Resolution
3.3. Distance Limit of Moving Target Detection and Resolution (Working Distance)
3.4. Illumination Intensity on Distance Limit of Target Detection and Resolution
3.5. Application of Smart Phone-Based Motion Detection to Clinical Diagnostic Testing Maneuvers
3.5.1. Finger Abduction/Adduction
3.5.2. Lateral Bend
4. Discussion
4.1. Importance of Defining an Operating Range
4.2. Markers and Marker Size
4.3. Synergies of Camera, Marker Color, and Lighting
4.4. Frequency and Rate of Movement and Capture
4.5. Limitations
4.6. Next Steps
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Patel, K.V.; Coppin, A.K.; Manini, T.M.; Lauretani, F.; Bandinelli, S.; Ferrucci, L.; Guralnik, J.M. Midlife Physical Activity and Mobility in Older Age. The InCHIANTI Study. Am. J. Prev. Med. 2006, 31, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A Review of the Effects of Physical Activity and Exercise on Cognitive and Brain Functions in Older Adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, D.L.; Hammond, C.C.; Reifsteck, E.J.; Jehu, C.M.; Williams, R.A.; Adams, M.M.; Lange, E.H.; Becofsky, K.; Rodriguez, E.; Shang, Y.-T. Physical Activity and Quality of Life. J. Prev. Med. Public Health 2013, 46 (Suppl. S1), S28–S34. [Google Scholar] [CrossRef] [PubMed]
- Pillay, S. How Simply Moving Benefits Your Mental Health. Available online: https://www.health.harvard.edu/blog/how-simply-moving-benefits-your-mental-health-201603289350 (accessed on 5 August 2021).
- Esmail, A.; Vrinceanu, T.; Lussier, M.; Predovan, D.; Berryman, N.; Houle, J.; Karelis, A.; Grenier, S.; Minh Vu, T.T.; Villalpando, J.M.; et al. Effects of Dance/Movement Training vs. Aerobic Exercise Training on Cognition, Physical Fitness and Quality of Life in Older Adults: A Randomized Controlled Trial. J. Bodyw. Mov. Ther. 2020, 24, 212–220. [Google Scholar] [CrossRef]
- Bouchard, C.; Shephard, R.J. Physical Activity, Fitness, and Health: The Model and Key Concepts. In Physical Activity, Fitness, and Health: International Proceedings and Consensus Statement; Bouchard, C., Shephard, R.J., Stephens, T., Eds.; Human Kinetic Publishers: Champaign, IL, USA, 1994; pp. 77–88. [Google Scholar]
- Dubbert, P.M.; Stetson, B.A. Exercise and Physical Activity. In Handbook of Health and Rehabilitation Psychology; Goreczny, A.J., Ed.; Spinger: Boston, MA, USA, 1995. [Google Scholar] [CrossRef]
- Powell, K.E.; Paluch, A.E.; Blair, S.N. Physical Activity for Health: What Kind? How Much? How Intense? On Top of What? Annu. Rev. Public Health 2011, 32, 349–365. [Google Scholar] [CrossRef] [Green Version]
- Kelley, G.A.; Kelley, K.S. Meditative Movement Therapies and Health-Related Quality-of-Life in Adults: A Systematic Review of Meta-Analyses. PLoS ONE 2015, 10, e0129181. [Google Scholar] [CrossRef] [Green Version]
- Piercy, K.L.; Troiano, R.P. Physical Activity Guidelines for Americans From the US Department of Health and Human Services. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e005263. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-Extremity Function in Persons over the Age of 70 Years as a Predictor of Subsequent Disability. N. Engl. J. Med. 1995, 332, 556–562. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower Extremity Function and Subsequent Disability: Consistency across Studies, Predictive Models, and Value of Gait Speed Alone Compared with the Short Physical Performance Battery. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef] [Green Version]
- Pöhlmann, S.T.L.; Harkness, E.F.; Taylor, C.J.; Astley, S.M. Evaluation of Kinect 3D Sensor for Healthcare Imaging. J. Med. Biol. Eng. 2016, 36, 857–870. [Google Scholar] [CrossRef]
- Van der Kruk, E.; Reijne, M.M. Accuracy of Human Motion Capture Systems for Sport Applications; State-of-the-Art Review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef] [PubMed]
- Parks, M.T.; Want, Z.; Siu, K.-C. Current Low-Cost Video-Based Motion Analysis Options for Clinical Rehabilitation: A Systematic Review. Phys. Ther. 2019, 99, 1405–1425. [Google Scholar] [CrossRef] [PubMed]
- Parks, M.; Chien, J.H.; Siu, K.C. Development of a Mobile Motion Capture (MO 2 CA) System for Future Military Application. In Military Medicine; Oxford University Press: Oxford, UK, 2019; Volume 184, pp. 65–71. [Google Scholar] [CrossRef] [Green Version]
- Barris, S.; Button, C. A Review of Vision-Based Motion Analysis in Sport. Sports Med. 2008, 38, 1025–1043. [Google Scholar] [CrossRef] [PubMed]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods Towards Developing a Markerless System. In Sports Medicine—Open; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef] [Green Version]
- Matthew, R.P.; Seko, S.; Bajcsy, R.; Lotz, J. Kinematic and Kinetic Validation of an Improved Depth Camera Motion Assessment System Using Rigid Bodies. IEEE J. Biomed. Health Inform. 2019, 23, 1784–1793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfister, A.; West, A.M.; Bronner, S.; Noah, J.A. Comparative Abilities of Microsoft Kinect and Vicon 3D Motion Capture for Gait Analysis. J. Med. Eng. Technol. 2014, 38, 274–280. [Google Scholar] [CrossRef]
- Maykut, J.N.; Taylor-Haas, J.A.; Paterno, M.V.; DiCesare, C.A.; Ford, K.R. Concurrent Validity and Reliability of 2D Kinematic Analysis of Frontal Plane Motion During Running. Int. J. Sports Phys. Ther. 2015, 10, 136–146. [Google Scholar]
- Bell, K.; Onyeukwu, C.; McClincy, M.; Allen, M.; Bechard, L.; Mukherjee, A.; Hartman, R.; Smith, C.; Lynch, A.; Irrgang, J. Verification of a Portable Motion Tracking System for Remote Management of Physical Rehabilitation of the Knee. Sensors 2019, 19, 1021. [Google Scholar] [CrossRef] [Green Version]
- McLean, S.G.; Walker, K.; Ford, K.R.; Myer, G.D.; Hewett, T.E.; Van Den Bogert, A.J. Evaluation of a Two Dimensional Analysis Method as a Screening and Evaluation Tool for Anterior Cruciate Ligament Injury. Br. J. Sports Med. 2005, 39, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Arai, K.; Asmara, R.A. 3D Skeleton Model Derived from Kinect Depth Sensor Camera and Its Application to Walking Style Quality Evaluations. Int. J. Adv. Res. Artif. Intell. 2013, 2, 24–28. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Zhang, P.; Chait, J. Accurate Realtime Full-Body Motion Capture Using a Single Depth Camera. ACM Trans. Graph. 2012, 31, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.A.; Mentiplay, B.F.; Hough, E.; Pua, Y.H. Three-Dimensional Cameras and Skeleton Pose Tracking for Physcial Function Assessment: A Review of Uses, Validity, Current Developments and Kinect Alternatives. Gait Posture 2019, 68, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Ceseracciu, E.; Sawacha, Z.; Cobelli, C. Comparison of Markerless and Marker-Based Motion Capture Technologies through Simultaneous Data Collection during Gait: Proof of Concept. PLoS ONE 2014, 9, e87640. [Google Scholar] [CrossRef] [PubMed]
- Drazan, J.F.; Phillips, W.T.; Seethapathi, N.; Hullfish, T.J.; Baxter, J.R. Moving Outside the Lab: Markerless Motion Capture Accurately Quantifies Sagittal Plane Kinematics during the Vertical Jump. J. Biomech. 2021, 125, 110547. [Google Scholar] [CrossRef] [PubMed]
- Kanko, R.M.; Laende, E.K.; Davis, E.M.; Selbie, W.S.; Deluzio, K.J. Concurrent Assessment of Gait Kinematics Using Marker-Based and Markerless Motion Capture. J. Biomech. 2021, 127, 110665. [Google Scholar] [CrossRef]
- Needham, R.; Stebbins, J.; Chockalingam, N. Three-Dimensional Kinematics of the Lumbar Spine during Gait Using Marker-Based Systems: A Systematic Review. J. Med. Eng. Technol. 2016, 40, 172–185. [Google Scholar] [CrossRef] [Green Version]
- Ammann, K.R.; Ahamed, T.; Sweedo, A.L.; Ghaffari, R.; Weiner, Y.E.; Slepian, R.C.; Jo, H.; Slepian, M.J. Human Motion Component and Envelope Characterization via Wireless Wearable Sensors. BMC Biomed. Eng. 2020, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Findlow, A.; Goulermas, J.Y.; Nester, C.; Howard, D.; Kenney, L.P.J. Predicting Lower Limb Joint Kinematics Using Wearable Motion Sensors. Gait Posture 2008, 28, 120–126. [Google Scholar] [CrossRef]
- Yang, C.-C.; Hsu, Y.-L. A Review of Accelerometry-Based Wearable Motion Detectors for Physical Activity Monitoring. Sensors 2010, 10, 7772–7788. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J. Using Accelerometers to Measure Physical Activity in Large-Scale Epidemiological Studies: Issues and Challenges. Br. J. Sports Med. 2014, 48, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Zhong, R.; Rau, P.L.P.; Yan, X. Application of Smart Bracelet to Monitor Frailty-Related Gait Parameters of Older Chinese Adults: A Preliminary Study. Geriatr. Gerontol. Int. 2018, 18, 1366–1371. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glowinski, S.; Obst, M.; Majdanik, S.; Potocka-Banaś, B. Dynamic Model of a Humanoid Exoskeleton of a Lower Limb with Hydraulic Actuators. Sensors 2021, 21, 3432. [Google Scholar] [CrossRef] [PubMed]
- Glicksman, J.T.; Reger, C.; Parasher, A.K.; Kennedy, D.W. Accuracy of Computer-Assisted Navigation: Significant Augmentation by Facial Recognition Software. Int. Forum Allergy Rhinol. 2017, 7, 884–888. [Google Scholar] [CrossRef]
- Köhler, J.; Pagani, A.; Stricker, D. Detection and Identification Techniques for Markers Used in Computer Vision. In Open Access Series in Informatics; Dagstuhl Publishing: Saarbrucken, Germany, 2011; Volume 19, pp. 36–44. [Google Scholar] [CrossRef]
- Ojha, S.; Sakhare, S. Image Processing Techniques for Object Tracking in Video Surveillance—A Survey. In Proceedings of the 2015 International Conference on Pervasive Computing (ICPC), Pune, India, 8–10 January 2015; IEEE: Pune, India, 2015. [Google Scholar] [CrossRef]
- Zhang, X.; Fronz, S.; Navab, N. Visual Marker Detection and Decoding in AR Systems: A Comparative Study. In Proceedings of the International Symposium on Mixed and Augmented Reality, Darmstadt, Germany, 1 October 2002; IEEE: Darmstadt, Germany, 2002. [Google Scholar] [CrossRef]
- iOS Device Compatibility Reference. Available online: https://developer.apple.com/library/archive/documentation/DeviceInformation/Reference/iOSDeviceCompatibility/Cameras/Cameras.html (accessed on 20 March 2021).
- Mansurov, N. Camera Resolution Explained. Available online: https://photographylife.com/camera-resolution-explained (accessed on 20 March 2021).
- Tominaga, S.; Nishi, S.; Ohtera, R. Measurement and Estimation of Spectral Sensitivity Functions for Mobile Phone Cameras. Sensors 2021, 21, 4985. [Google Scholar] [CrossRef]
- Lubek, T. Video Depth of Field with iPhone: A Simple Beginners Guide. Available online: https://www.diyvideostudio.com/depth-of-field-with-iphone/ (accessed on 20 March 2021).
- How to Evaluate Camera Sensitivity. Available online: https://www.flir.com/discover/iis/machine-vision/how-to-evaluate-camera-sensitivity/ (accessed on 20 March 2021).
- Song, M.H.; Godøy, R.I. How Fast Is Your Body Motion? Determining a Sufficient Frame Rate for an Optical Motion Tracking System Using Passive Markers. PLoS ONE 2016, 11, e0150993. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Distance of Separation (mm) | 2 mm Targets | 5 mm Targets | 10 mm Targets | p-Value |
|---|---|---|---|---|
| 2 | 2.5 ft | 2.67 ft | 4 ft | 0.003 |
| 5 | 4.67 ft | 5.33 ft | 9 ft | <0.001 |
| 10 | 5.17 ft | 7.67 ft | 11 ft | <0.001 |
| p-value | 0.001 | <0.001 | <0.001 |
| Body Element | Flexibility | Specific Medical Use |
|---|---|---|
| Whole Body | Toe Touch Sit and Reach Schober Test Side Bending Test Trunk Rotation Test | Adams Forward Bend Test (Scoliosis) Lateral Bend Test |
| Large Body Region/Limb | Cervical Flexion/Extension Shoulder-Neck Mobility Back Scratch Test Straight Leg Raise Modified Thomas Test Calf Muscle Flexibility Test | Hawkins-Kennedy Test (Shoulder) Anterior Drawer Test (Knee-ACL) Apley’s Test (Knee-Meniscus) Lachman’s Test (Knee-ACL) McMurray’s Test (Knee-Meniscus) Craig’s Test (Hip) Thomas Test (Hip Flexion) Trendelenburg Test (Hip Abduction) Ober’s Test (IT Band) |
| Regional Element/Digits | Wrist Extension/Flexion Ankle Extension/Flexion Finger Extension/Flexion Toe Extension/Flexion | Finger Abduction/Adduction Temporomandibular Joint Movement Metacarpophalangeal Joint Flexion/Extension Interphalangeal Joint Flexion/Extension Claw Test Finger Lift Thumb Movement |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vincent, A.C.; Furman, H.; Slepian, R.C.; Ammann, K.R.; Di Maria, C.; Chien, J.H.; Siu, K.-C.; Slepian, M.J. Smart Phone-Based Motion Capture and Analysis: Importance of Operating Envelope Definition and Application to Clinical Use. Appl. Sci. 2022, 12, 6173. https://0-doi-org.brum.beds.ac.uk/10.3390/app12126173
Vincent AC, Furman H, Slepian RC, Ammann KR, Di Maria C, Chien JH, Siu K-C, Slepian MJ. Smart Phone-Based Motion Capture and Analysis: Importance of Operating Envelope Definition and Application to Clinical Use. Applied Sciences. 2022; 12(12):6173. https://0-doi-org.brum.beds.ac.uk/10.3390/app12126173
Chicago/Turabian StyleVincent, Ashley Chey, Haley Furman, Rebecca C. Slepian, Kaitlyn R. Ammann, Carson Di Maria, Jung Hung Chien, Ka-Chun Siu, and Marvin J. Slepian. 2022. "Smart Phone-Based Motion Capture and Analysis: Importance of Operating Envelope Definition and Application to Clinical Use" Applied Sciences 12, no. 12: 6173. https://0-doi-org.brum.beds.ac.uk/10.3390/app12126173