
Influences of Breathing Exercises and Breathing Exercise Combined with Aerobic Exercise on Changes in Basic Spirometry Parameters in Patients with Bronchial Asthma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention and Instruments
2.2.1. Experimental Protocol 1
2.2.2. Experimental Protocol 2
2.2.3. Control Protocol
2.3. Selection Criteria
2.4. Data Collections
2.5. Data Analysis
3. Results
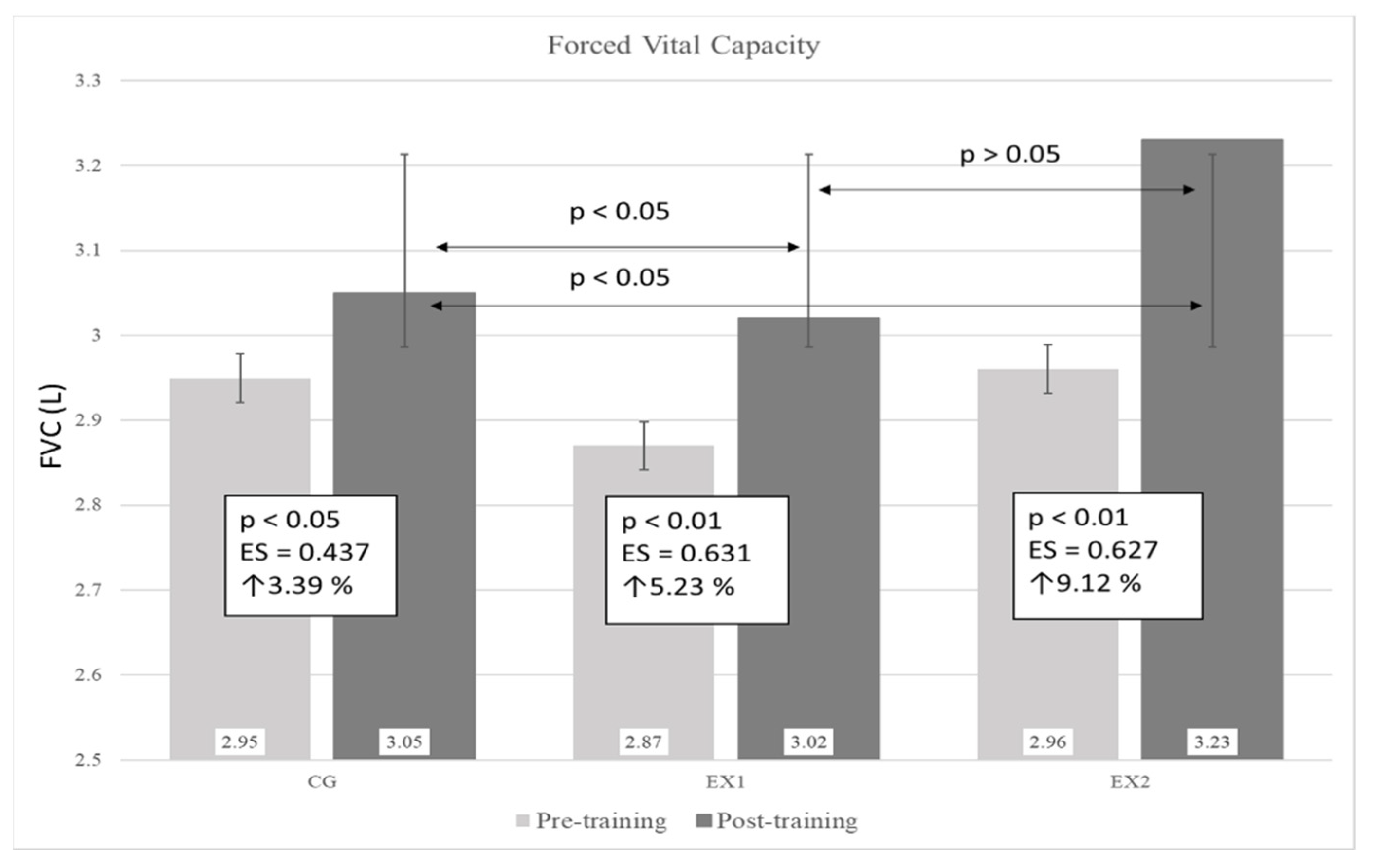
3.1. Forced Vital Capacity
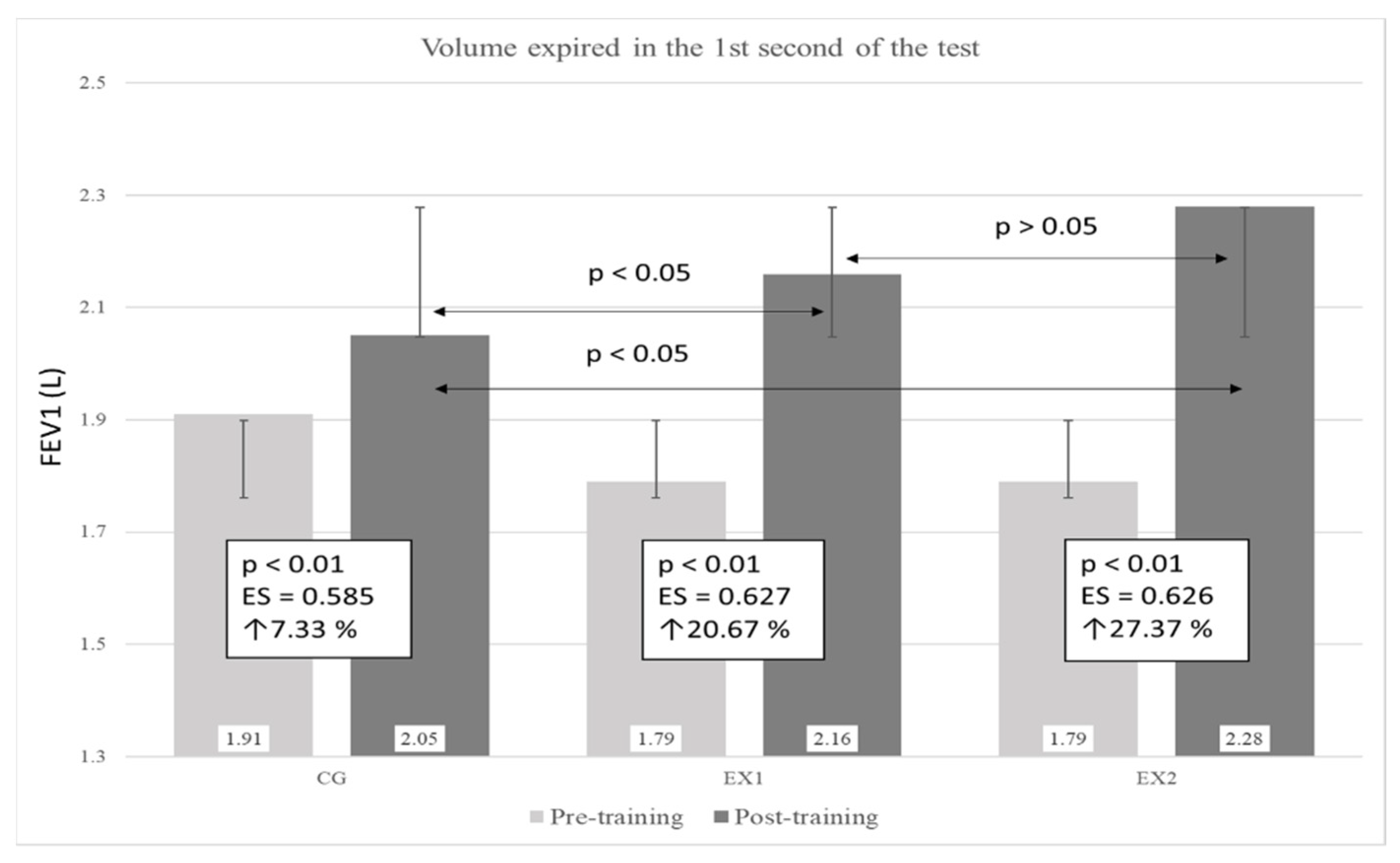
3.2. Volume Expired in the 1st Second of the Test
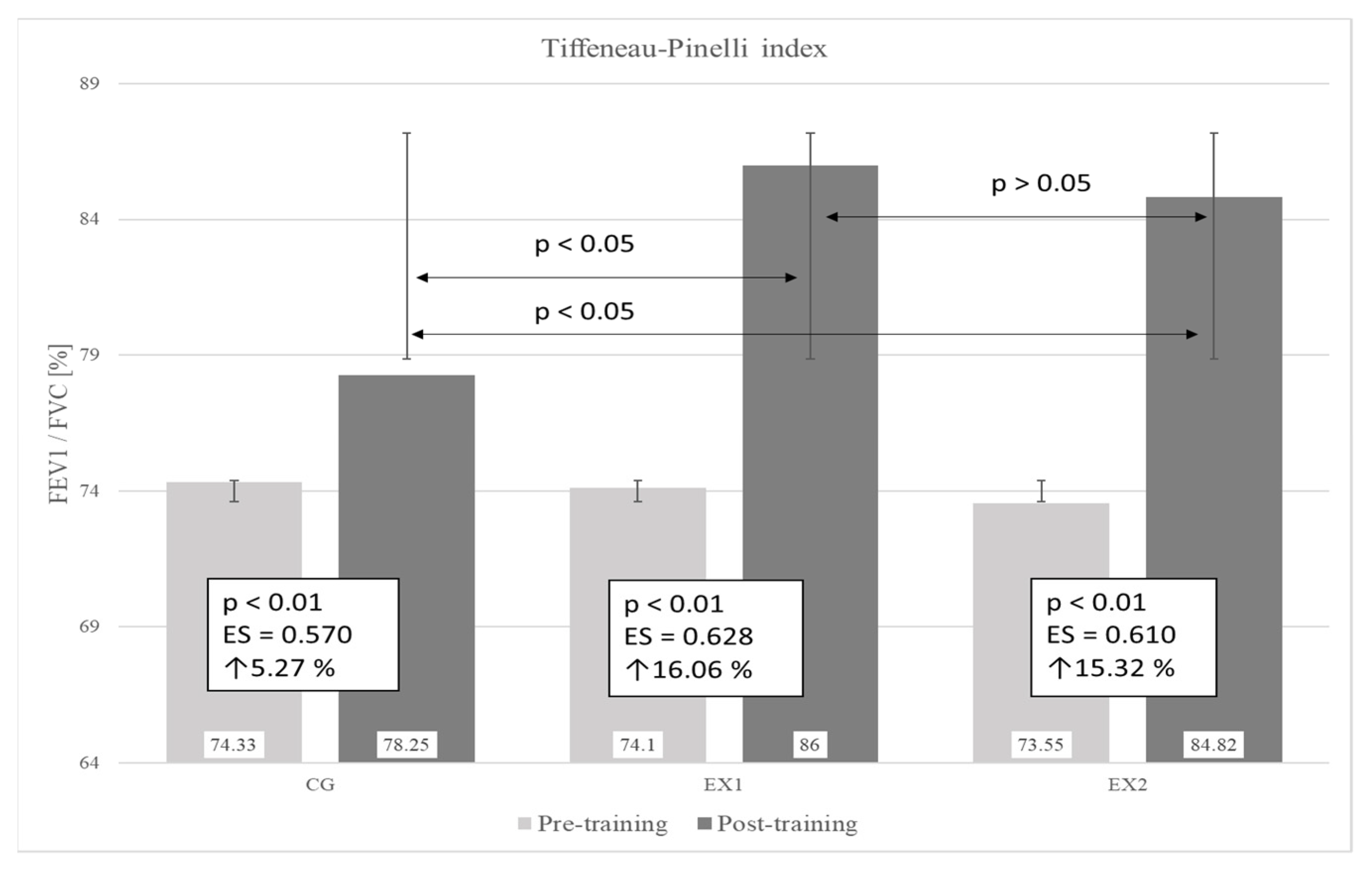
3.3. Tiffeneau–Pinelli Index
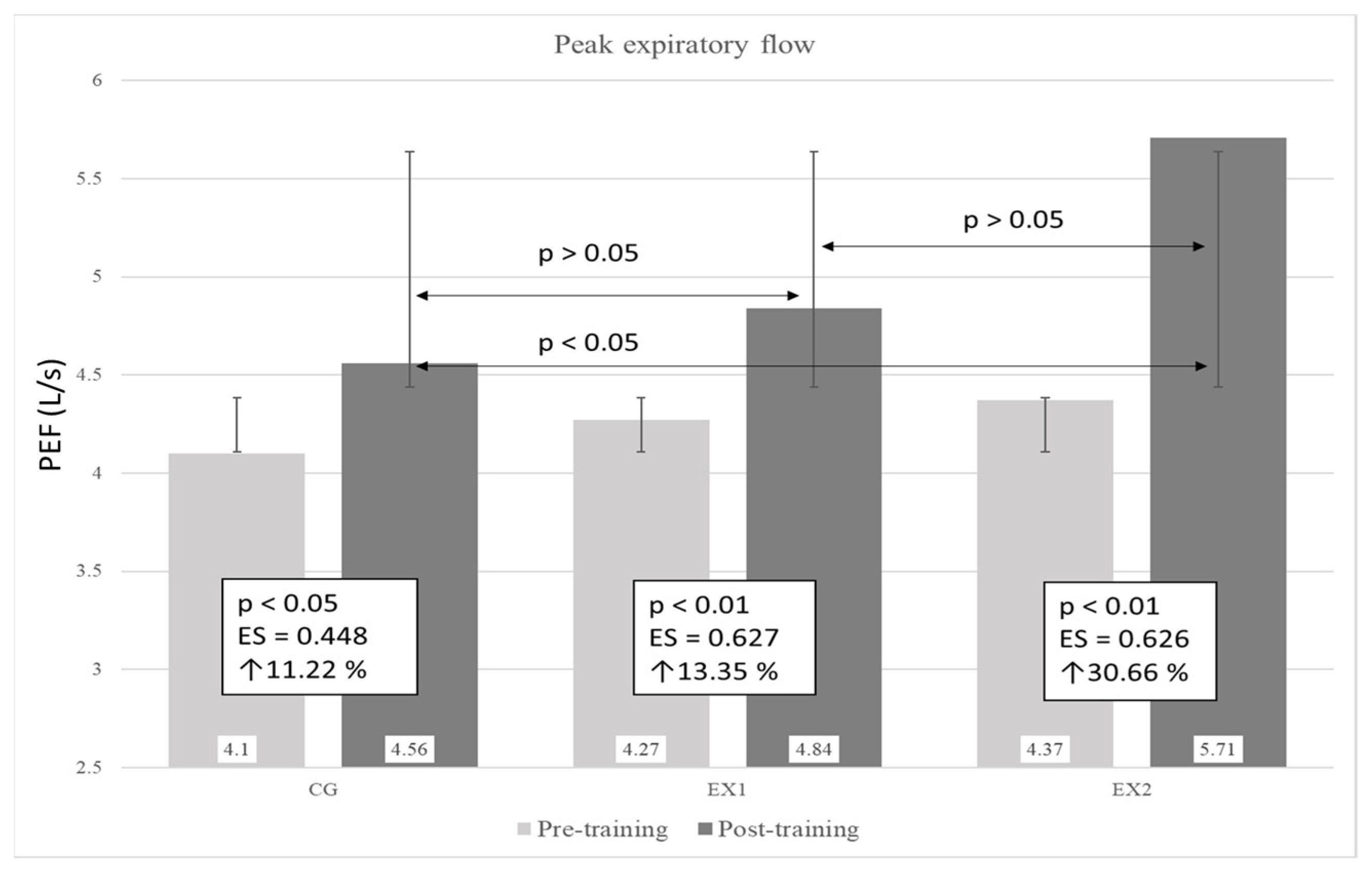
3.4. Peak Expiratory Flow
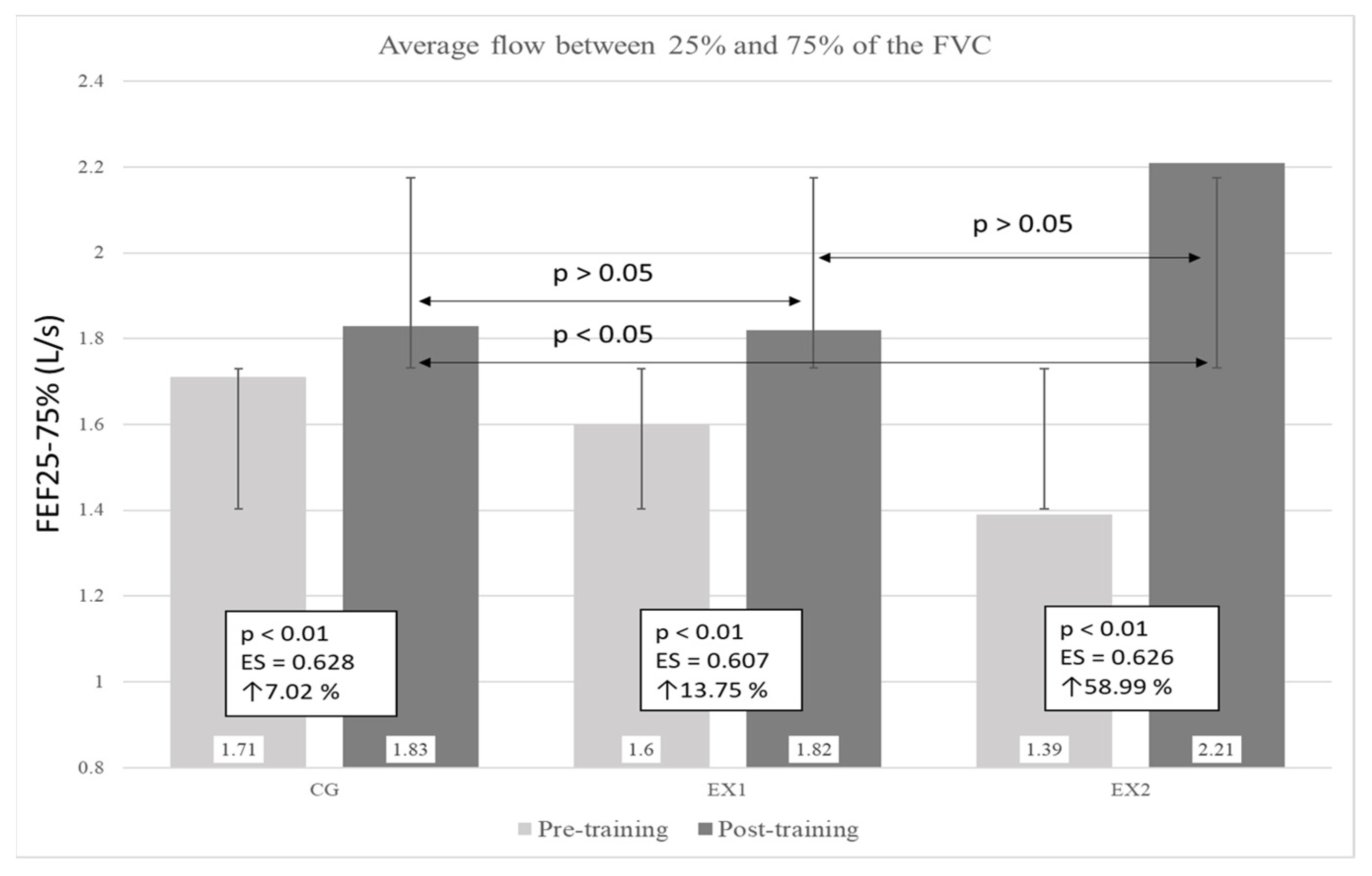
3.5. Average Flow between 25% and 75% of the FVC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- To, T.; Stanojevic, S.; Moores, G.; Gershon, A.S.; Bateman, E.D.; Cruz, A.A.; Boulet, L.P. Global asthma prevalence in adults: Findings from the cross-sectional world health survey. BMC Public Health 2012, 12, 204. [Google Scholar] [CrossRef] [Green Version]
- O’Byrne, P.M.; Naya, I.P.; Kallen, A.; Postma, D.S.; Barnes, P.J. Increasing doses of inhaled corticosteroids compared to adding long-acting inhaled beta2-agonists in achieving asthma control. Chest 2008, 134, 1192–1199. [Google Scholar] [CrossRef]
- Lalloo, U.G.; Malolepszy, J.; Kozma, D.; Krofta, K.; Ankerst, J.; Johansen, B.; Thomson, N.C. Budesonide and formoterol in a single inhaler improves asthma control compared with increasing the dose of corticosteroid in adults with mild-to-moderate asthma. Chest 2003, 123, 1480–1487. [Google Scholar] [CrossRef]
- Foresi, A.; Morelli, M.C.; Catena, E. Low-dose budesonide with the addition of an increased dose during exacerbations is effective in long-term asthma control. On behalf of the Italian Study Group. Chest 2000, 117, 440–446. [Google Scholar] [CrossRef]
- Lasmar, L.; Camargos, P.; Champs, N.S.; Fonseca, M.T.; Fontes, M.J.; Ibiapina, C.; Alvim, C.; Moura, J.A. Adherence rate to inhaled corticosteroids and their impact on asthma control. Allergy 2009, 64, 784–789. [Google Scholar] [CrossRef]
- Legorreta, A.P.; Christian-Herman, J.; O’Connor, R.D.; Hasan, M.M.; Evans, R.; Leung, K.M. Compliance with national asthma management guidelines and specialty care: A health maintenance organization experience. Arch. Intern. Med. 1998, 158, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Gaga, M.; Papageorgiou, N.; Zervas, E.; Gioulekas, D.; Konstantopoulos, S. Control of asthma under specialist care: Is it achieved? Chest 2005, 128, 78–84. [Google Scholar] [CrossRef]
- Chapman, K.R.; Boulet, L.P.; Rea, R.M.; Franssen, E. Suboptimal asthma control: Prevalence, detection and consequences in general practice. Eur. Respir. J. 2008, 31, 320–325. [Google Scholar] [CrossRef]
- Williams, S.A.; Wagner, S.; Kannan, H.; Bolge, S.C. The association between asthma control and health care utilization, work productivity loss and health-related quality of life. J. Occup. Environ. Med. 2009, 51, 780–785. [Google Scholar] [CrossRef] [Green Version]
- Karam, M.; Kaur, B.P.; Baptist, A.P. A modified breathing exercise program for asthma is easy to perform and effective. J. Asthma 2017, 54, 217–222. [Google Scholar] [CrossRef]
- Carr, M.; Jones, J. Physiological effects of exercise on stroke survivors. Top. Stroke Rehabil. 2003, 9, 57–64. [Google Scholar] [CrossRef]
- Moodie, L.; Reeve, J.; Elkins, M. Inspiratory muscle training increases inspiratory muscle strength in patients weaning from mechanical ventilation: A systematic review. J. Physiother. 2011, 57, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Weiner, P.; Magadle, R.; Beckerman, M.; Weiner, M.; Berar-Yanay, N. Comparison of specific expiratory, inspiratory, and combined muscle training programs in COPD. Chest 2003, 124, 1357–1364. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Wisniewski, A.; Britton, J.; Tattersfield, A. Effect of yoga breathing exercises (pranayama) on airway reactivity in subjects with asthma. Lancet 1990, 335, 1381–1383. [Google Scholar] [CrossRef]
- Villareal, G.M.C.; Villazor, B.P.U.; Villegas, A.M.; Visaya, P.S.N.; Vista, M.E.; Tan, C.B.; Florendo, C.E.G. Effect of Buteyko Method on Asthma Control and Quality of Life of Filipino Adults with Bronchial Asthma. J. Macro Trends Health Med. 2014, 2, 44–60. [Google Scholar]
- Thomas, M.; Bruton, A. Breathing exercises for asthma. Breathe 2014, 10, 312–322. [Google Scholar] [CrossRef] [Green Version]
- Evaristo, K.B.; Mendes, F.A.R.; Saccomani, M.G.; Cukier, A.; Carvalho-Pinto, R.M.; Rodrigues, M.R.; Santaella, D.F.; Saraiva-Romanholo, B.M.; Martins, M.A.; Carvalho, C.R.F. Effects of Aerobic Training Versus Breathing Exercises on Asthma Control: A Randomized Trial. J. Allergy Clin. Immunol. Pract. 2020, 8, 2989–2996.e2984. [Google Scholar] [CrossRef]
- Dogra, S.; Baker, J.; Ardern, C.I. The role of physical activity and body mass index in the health care use of adults with asthma. Ann. Allergy Asthma Immunol. 2009, 102, 462–468. [Google Scholar] [CrossRef]
- Emtner, M.; Herala, M.; Stalenheim, G. High-intensity physical training in adults with asthma. A 10-week rehabilitation program. Chest 1996, 109, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, A.; Cabral, A.L.; Neder, J.A.; Martins, M.A.; Carvalho, C.R. Exercise training on disease control and quality of life in asthmatic children. Med. Sci. Sports Exerc. 2007, 39, 1474–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, C.J. The role of physical training in asthma. Chest 1992, 101, 293S–298S. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, L.M.; Clark, C.J. Benefits and problems of a physical training programme for asthmatic patients. Thorax 1990, 45, 345–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neder, J.A.; Nery, L.E.; Silva, A.C.; Cabral, A.L.; Fernandes, A.L. Short-term effects of aerobic training in the clinical management of moderate to severe asthma in children. Thorax 1999, 54, 202–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira, R.P.; Claudino, R.C.; Duarte, A.C.; Santos, A.B.; Perini, A.; Faria Neto, H.C.; Mauad, T.; Martins, M.A.; Dolhnikoff, M.; Carvalho, C.R. Aerobic exercise decreases chronic allergic lung inflammation and airway remodeling in mice. Am. J. Respir. Crit. Care Med. 2007, 176, 871–877. [Google Scholar] [CrossRef]
- Pastva, A.; Estell, K.; Schoeb, T.R.; Atkinson, T.P.; Schwiebert, L.M. Aerobic exercise attenuates airway inflammatory responses in a mouse model of atopic asthma. J. Immunol. 2004, 172, 4520–4526. [Google Scholar] [CrossRef] [Green Version]
- Shaw, I.; Shaw, B.S.; Brown, G.A. Role of diaphragmatic breathing and aerobic exercise in improving pulmonary function and maximal oxygen consumption in asthmatics. Sci. Sports 2010, 25, 139–145. [Google Scholar] [CrossRef]
- Zarneshan, A. The Efficacy of Aerobic and Breathing Exercise Training on Asthma Control and Physical—Psychological Health Promotion in Women with Asthma. Iran. J. Health Educ. Health Promot. 2018, 6, 179–188. [Google Scholar] [CrossRef]
- Clark, C.J. Asthma and exercise: A suitable case for rehabilitation? Thorax 1992, 47, 765–767. [Google Scholar] [CrossRef] [Green Version]
- Silva, C.; Torres, L.; Rahal, A.; Terra Filho, J.; Vianna, E. Comparison of morning and afternoon exercise training for asthmatic children. Braz. J. Med. Biol. Res. 2006, 39, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Mendes, F.; Almeida, F.M.; Cukier, A.; Stelmach, R.; Jacob-Filho, W.; Martins, M.A.; Carvalho, C. Effects of aerobic training on airway inflammation in asthmatic patients. Med. Sci. Sports Exerc. 2011, 43, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, L.B.d.; Britto, M.C.A.; Lucena-Silva, N.; Gomes, R.G.; Figueroa, J.N. The efficacy of aerobic training in improving the inflammatory component of asthmatic children. Randomized trial. Respir. Med. 2014, 108, 1438–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varray, A.L.; Mercier, J.G.; Terral, C.M.; Prefaut, C.G. Individualized Aerobic and High Intensity Training for Asthmatic Children in an Exercise Readaptation Program. Is Training Always Helpful for Better Adaptation to Exercise? Chest 1991, 99, 579–586. [Google Scholar] [CrossRef] [PubMed]
- van Veldhoven, N.H.; Vermeer, A.; Bogaard, J.; Hessels, M.G.; Wijnroks, L.; Colland, V.; van Essen-Zandvliet, E.E. Children with asthma and physical exercise: Effects of an exercise programme. Clin. Rehabil. 2001, 15, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Onur, E.; Kabaroğlu, C.; Günay, Ö.; Var, A.; Yilmaz, Ö.; Dündar, P.; Tikiz, C.; Güvenç, Y.; Yüksel, H. The beneficial effects of physical exercise on antioxidant status in asthmatic children. Allergol. Immunopathol. 2011, 39, 90–95. [Google Scholar] [CrossRef]
- Farid, R.; Ghasemi, R.; Jabari, A.F.; Baradaran, R.M.; Talaei, K.M.; Ghafari, J.; Ebrahimi, A.A.; Khaledan, A. Effect of aerobic exercise training on pulmonary function and tolerance of activity in asthmatic patients. Iran. J. Allergy Asthma Immunol. 2005, 4, 133–138. [Google Scholar]
- França-Pinto, A.; Mendes, F.A.; de Carvalho-Pinto, R.M.; Agondi, R.C.; Cukier, A.; Stelmach, R.; Saraiva-Romanholo, B.M.; Kalil, J.; Martins, M.A.; Giavina-Bianchi, P.; et al. Aerobic training decreases bronchial hyperresponsiveness and systemic inflammation in patients with moderate or severe asthma: A randomised controlled trial. Thorax 2015, 70, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Gao, S.; Lian, Y. Effects of continuous aerobic exercise on lung function and quality of life with asthma: A systematic review and meta-analysis. J. Thorac. Dis. 2020, 12, 4781–4795. [Google Scholar] [CrossRef]
- Cohen, J. The earth is round (p < 0.05). Am. Psychol. 1994, 49, 997–1003. [Google Scholar]
- Maher, J.M.; Markey, J.C.; Ebert-May, D. The other half of the story: Effect size analysis in quantitative research. CBE Life Sci Educ. 2013, 12, 345–351. [Google Scholar] [CrossRef]
- Santino, T.A.; Chaves, G.S.; Freitas, D.A.; Fregonezi, G.A.; Mendonça, K.M. Breathing exercises for adults with asthma. Cochrane Database Syst. Rev. 2020, 3, Cd001277. [Google Scholar] [CrossRef]
- Bolton, C.E.; Bevan-Smith, E.F.; Blakey, J.D.; Crowe, P.; Elkin, S.L.; Garrod, R.; Greening, N.J.; Heslop, K.; Hull, J.H.; Man, W.D.; et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 2013, 68 (Suppl. 2), ii1–ii30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, Z. How to diagnose exercise induced asthma? Asian J. Sports Med. 2011, 2, 63–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiler, J.M.; Anderson, S.D.; Randolph, C.; Bonini, S.; Craig, T.J.; Pearlman, D.S.; Rundell, K.W.; Silvers, W.S.; Storms, W.W.; Bernstein, D.I.; et al. Pathogenesis, prevalence, diagnosis, and management of exercise-induced bronchoconstriction: A practice parameter. Ann. Allergy Asthma Immunol. 2010, 105, S1–S47. [Google Scholar] [CrossRef] [PubMed]
- Ritz, T.; Rosenfield, D.; Steptoe, A. Physical activity, lung function, and shortness of breath in the daily life of individuals with asthma. Chest 2010, 138, 913–918. [Google Scholar] [CrossRef]
- Garcia-Aymerich, J.; Varraso, R.; Antó, J.M.; Camargo, C.A., Jr. Prospective study of physical activity and risk of asthma exacerbations in older women. Am. J. Respir. Crit. Care Med. 2009, 179, 999–1003. [Google Scholar] [CrossRef] [Green Version]
- Teramoto, M.; Moonie, S. Physical activity participation among adult Nevadans with self-reported asthma. J. Asthma 2011, 48, 517–522. [Google Scholar] [CrossRef]
- Feng, Z.; Wang, J.; Xie, Y.; Li, J. Effects of exercise-based pulmonary rehabilitation on adults with asthma: A systematic review and meta-analysis. Respir Res. 2021, 22, 33. [Google Scholar] [CrossRef]
- Erdoğan Yüce, G.; Taşcı, S. Effect of pranayama breathing technique on asthma control, pulmonary function, and quality of life: A single-blind, randomized, controlled trial. Complementary Ther. Clin. Pract. 2020, 38, 101081. [Google Scholar] [CrossRef]
- Multani, N.K. Comparison of Breathing Exercises and Aerobic Exercise in Asthmatic Children. J. Exerc. Sci. Physiother. 2010, 6, 112–119. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | CG | EX1 | EX2 |
|---|---|---|---|
| Participants [n] | 12 | 10 | 11 |
| Age | 34.80 ± 1.93 | 34.82 ± 1.33 | 34.58 ± 1.44 |
| Height (cm) | 166.08 ± 4.25 | 166.10 ± 4.89 | 167.27 ± 4.54 |
| Weight (kg) | 66.33 ± 4.33 | 69.50 ± 6.29 | 68.91 ± 4.97 |
| FVC (L) | 2.95 ± 0.21 | 2.87 ± 0.23 | 2.96 ± 0.25 |
| FEV1 (L) | 1.91 ± 0.23 | 1.79 ± 0.28 | 1.79 ± 0.20 |
| FEV1/FVC (%) | 74.33 ± 6.51 | 74.1 ± 7.56 | 73.55 ± 5.84 |
| PEF (L/s) | 4.1 ± 1.03 | 4.27 ± 0.48 | 4.37 ± 0.9 |
| FEF25–75% (L/s) | 1.71 ± 0.59 | 1.6 ± 0.45 | 1.39 ± 0.35 |
| Breathing Exercises | Breathing Cycles [n] | Series [n] | Method |
|---|---|---|---|
| Balloon inflation | 10 | 2 | Resistance |
| Diaphragmatic breathing while standing | 6 | 2 | Diaphragm |
| Diaphragmatic breathing while sitting | 5 | 2 | Diaphragm |
| Diaphragmatic breathing in bed with legs bent | 4 | 3 | Diaphragm |
| Torso rotation with active breathing in the sideways | 10 | 2 | Yoga |
| Squat with spine rotation and active breathing | 10 | 2 | Yoga |
| Walking with alternating rhythm of breathing | 12 | 2 | Buteyko |
| Running with alternating rhythm of breathing | 12 | 4 | Buteyko |
| Breath holding | 6 | 4 | Buteyko |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grznár, Ľ.; Sucháň, D.; Labudová, J.; Odráška, L.; Matúš, I. Influences of Breathing Exercises and Breathing Exercise Combined with Aerobic Exercise on Changes in Basic Spirometry Parameters in Patients with Bronchial Asthma. Appl. Sci. 2022, 12, 7352. https://0-doi-org.brum.beds.ac.uk/10.3390/app12147352
Grznár Ľ, Sucháň D, Labudová J, Odráška L, Matúš I. Influences of Breathing Exercises and Breathing Exercise Combined with Aerobic Exercise on Changes in Basic Spirometry Parameters in Patients with Bronchial Asthma. Applied Sciences. 2022; 12(14):7352. https://0-doi-org.brum.beds.ac.uk/10.3390/app12147352
Chicago/Turabian StyleGrznár, Ľuboš, Dávid Sucháň, Jana Labudová, Lukáš Odráška, and Ivan Matúš. 2022. "Influences of Breathing Exercises and Breathing Exercise Combined with Aerobic Exercise on Changes in Basic Spirometry Parameters in Patients with Bronchial Asthma" Applied Sciences 12, no. 14: 7352. https://0-doi-org.brum.beds.ac.uk/10.3390/app12147352