1. Introduction
Impaction and ectopic eruption of permanent teeth are frequently encountered in orthodontic practice. The prevalence of maxillary canine impaction is reported to be 0.8% to 2.9% [
1], which is the second most common after third molar impaction [
2,
3]. In Asians, including Japanese people, about 70% of canine eruption disturbances occur on the labial side [
4], and this condition is also common among patients consulting orthodontists.
Various etiologies have been reported for maxillary canine impaction, including an abnormal position of the tooth germ, lack of space, lack of guidance, and genetic factors [
1,
5]. Furthermore, compared with other teeth, the maxillary canines are formed in a deeper layer and thus have a longer eruption path, making them more prone to eruption disturbance [
6]. Becker et al. [
7] reported that the maxillary lateral incisors and first premolars erupt prior to the canines, and as long as the canines are in their normal eruption position and there is sufficient space, they can erupt unimpeded. However, if the adjacent first premolar erupts with mesial buccal rotation, its root can intrude into the eruption path of the canine. Such an abnormal alignment of the first premolar may result in impaction of the permanent maxillary canine. These findings suggest that maxillary canine impaction is strongly influenced by environmental factors. Celikoglu et al. [
8] also stated that because the canines erupt last, a lack of arch space due to premature loss of the deciduous teeth or other causes may result in canine impaction.
Kumar et al. suggested that the most important point for preventing maxillary canine impaction is to detect tooth malposition as early as possible and predict possible subsequent eruption disturbances [
9]. The mean age at which maxillary canines erupt is reported to be 10.10 ± 1.01 years [
6], and Ericson et al. [
10] reported that 10–13 years is the optimal age to check for abnormal eruption of the maxillary canines. Becker [
11] stated that patients 9–10 years of age who do not show a labial bulge should be suspected of having an impacted canine, which should be confirmed radiographically. Furthermore, given that 80–85% of canine eruption disturbances are unilateral [
12,
13], it is extremely important to perform a close radiographic examination in patients with a marked left–right difference in canine eruption status [
1]. However, in some patients, such examinations are delayed, treatment is delayed, and an impacted maxillary canine may be left in place until the permanent dentition stage. Depending on the severity, impacted teeth and abnormally erupted teeth can cause root resorption and displacement of adjacent teeth, eruption disturbance, and deterioration of the occlusal relationship. It is therefore important to accurately determine their position and applicable treatment methods, and to implement the appropriate treatment [
14]. Manne et al. [
15] argued that extracting a labially impacted maxillary canine to improve malocclusion should be contraindicated because although it may temporarily improve aesthetics, it may also reduce the patient’s functional occlusal force and lead to compromised outcomes in orthodontic treatment. In addition, they state that the most desirable approach is to align the maxillary canines through surgical fenestration and orthodontic treatment.
This report presents a case of a patient with eruption disturbance of the maxillary left canine in which the maxillary left second molar was extracted and the maxillary left first molar was distally moved with a Hyrax-type expander (Veltri Monolateral Screw®; Leone, Firenze, Italy) designed to enable the distal movement of a unilateral first molar in order to create eruption space for the maxillary left canine, resulting in smooth distal molar movement and alignment of the left maxillary canine in the dental arch. Furthermore, the maxillary third molar was also aligned to achieve a good occlusal relationship without reducing the number of teeth. Written consent was obtained from the patient’s guardians to publish this case report, including the patient’s photographs.
2. Diagnosis and Etiology
The patient was a boy aged 14 years and 4 months at the time of the initial presentation. He had a chief complaint of non-eruption of the maxillary left canine.
The facial features were symmetrical in the frontal view, with the maxillary midline coinciding with the facial midline and the mandibular midline deviated 1.5 mm to the right when smiling. The lateral view showed a straight profile. The occlusal relationship of the first molars was Angle Class I on the right side and Angle Class II on the left side, with overjet of +2.0 mm and overbite of +3.0 mm. The maxillary left canine was displaced to the labial side of the maxillary left lateral incisor, with its apex slightly and ectopically erupted. It was unclear whether the maxillary left deciduous tooth was lost prematurely during the deciduous-to-permanent dentition phase, as neither the patient nor his guardians could remember. Due to the mesial positioning of the maxillary left first molar, there was a lack of eruption space for the maxillary left canine, with an arch length discrepancy of −7.5 mm. The mandibular anterior teeth were slightly crowded, with an arch length discrepancy of −3.0 mm. The maxillary right lateral incisor and mandibular right lateral incisor were in crossbite (
Figure 1 and
Figure 2).
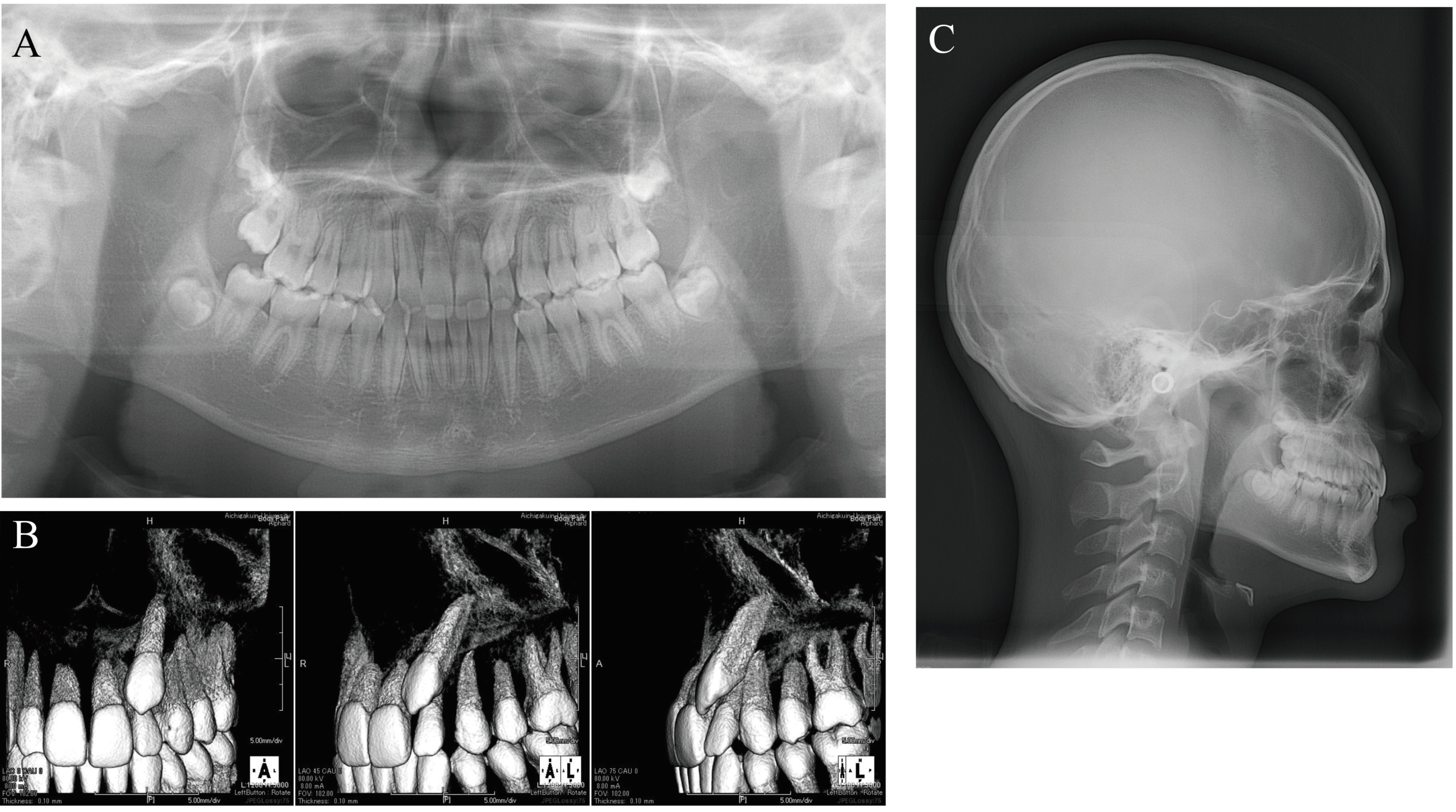
Panoramic X-ray and cone-beam computed tomography (CBCT) images showed that the maxillary left canine had erupted ectopically due to eruption disturbance. The maxillary left canine was mesially inclined with its crown near the labial root surface of the lateral incisor. The cusp of the canine was positioned more mesially than the lateral incisor axis. There was no evidence of canine contact with the lateral incisor or root resorption of the adjacent permanent teeth. There was no abnormality in the number of teeth. Tooth germs of the maxillary and mandibular right and left third molars were observed; the tooth germ of the maxillary left third molar was almost as large as the ipsilateral first and second molars.
Lateral cephalometric radiography showed no discordance in the anteroposterior position of the maxilla and mandible, with SNA of 90.5°, SNB of 88.5°, and ANB of 2.0°. Vertically, the patient had a low Frankfort-mandibular plane angle (FMA) of 14.0°. U-1 to NA was 2.0 mm/14.0°, indicating that the axis of the maxillary central incisor was normal, but that it was lingually positioned. L-1 to NB was 2.0 mm/14.5° and the FMIA was 80.5°, indicating that the mandibular central incisor was inclined and positioned lingually. The resulting interincisal angle was 150.0°, a large value exceeding 2SD (
Figure 3).
The mesiodistal positions and axial inclination angles of the maxillary first molars were also measured (
Figure 4). Mesiodistal measurements were as follows: A′-ptm′ 51.0 mm, A′-Ms 32.5 mm for the right and 28.0 mm for the left, and ptm′-Ms 18.5 mm for the right and 23.0 mm for the left (the left one was approximately 4.5 mm more mesial than the right one). As described by Byloff et al. [
16] and Mayara et al. [
17], the line connecting the midpoint of the occlusal surface of the maxillary first molars and the midpoint of the mesial and distal root apexes was defined as the maxillary first molar axis (Mp), and the angle between the palatal plane and the maxillary first molar axis was defined as the maxillary first molar axial inclination angle (α). The inclination angle was 83.0° on the right and 88.0° on the left, indicating that the more mesially located left maxillary first molar was more mesially inclined (
Table 1).
Based on the above analysis results, the patient was diagnosed as a low-angle case with crowding and eruption disturbance of the maxillary left canine tooth.
3. Treatment Objectives
The treatment objective for this patient was to apply traction and align the ectopically erupted left maxillary canine while maintaining a good lateral profile. The specific plan was to extract the maxillary left second molar and distally move the mesially positioned maxillary left first molar to the Angle Class I position using a Hyrax-type expander with an expansion screw (Veltri Monolateral Screw
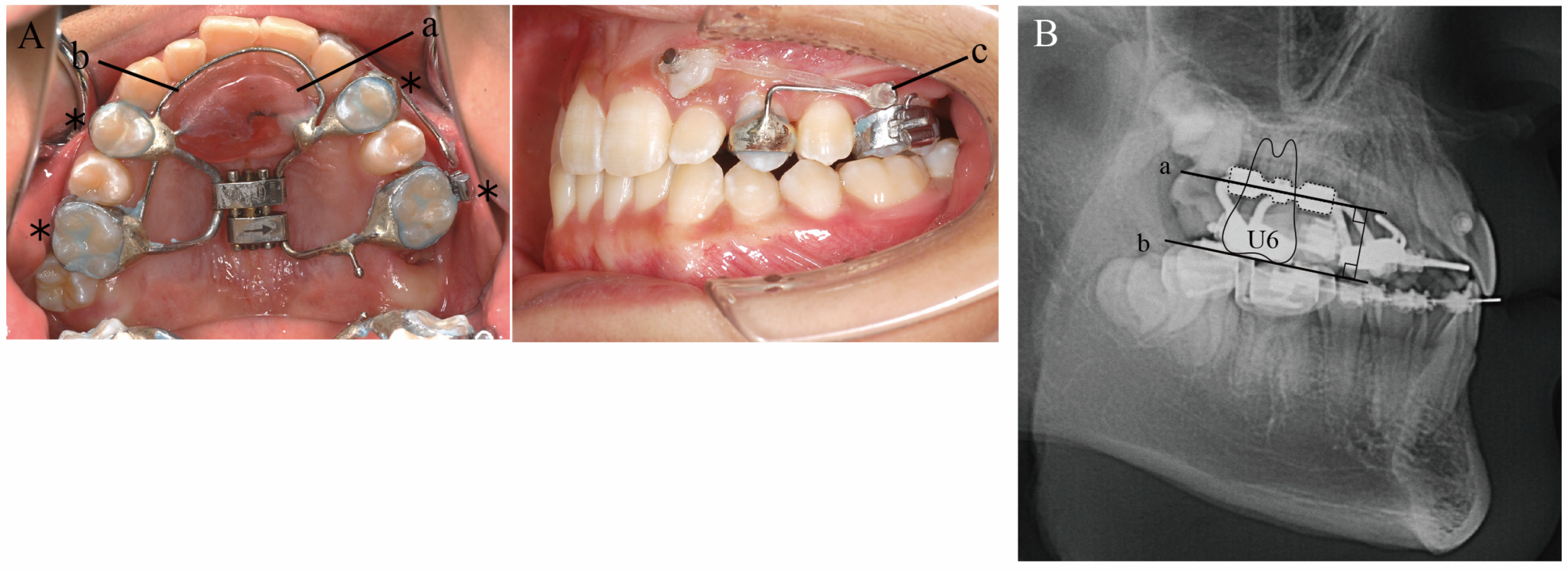
®, 8 mm A0629-08; Leone, Firenze, Italy), which is designed for distal/mesial and expansive/contractive movement of a single tooth, to create eruption space for the maxillary left canine. In the present case, the appliance was designed with bands attached to the maxillary left and right first premolars and left and right first molars, and the palatal screw was turned using the left and right first premolars and the right first molar as anchorage sources, so that only the left maxillary first molar could be moved distally. An expansion screw was placed parallel to the occlusal plane of the maxillary first molars to allow distal bodily movement of the left first molar. In addition, Nance’s holding arch was added to the palatal region and a lingual arch was placed along the maxillary anterior teeth to reinforce anchorage. Moreover, a 0.9 mm cobalt–chromium alloy wire was bent distally into a hook shape and brazed to the buccal side of the band on the left first premolar. The ectopically erupted canine was pulled in the distal–buccal direction by an elastic chain from the hook. This was followed by treatment of the maxillary and mandibular premolars with a multi-bracket system without extraction. In addition, because the tooth germ of the maxillary left third molar was found to be large enough, a plan was also made to align the maxillary left third molar into the maxillary arch (
Figure 5).
The treatment plan was as follows:
Extraction of the maxillary left second molar.
Distal movement of the maxillary left first molar.
Traction and aligning of the ectopically erupted maxillary left canine.
Aligning the midlines of the maxillary and mandibular arches.
Establishment of one-to-two tooth occlusion.
Improvement of crowding of the mandibular anterior teeth and crossbite.
4. Treatment Alternatives
For the treatment of the ectopically erupted maxillary canine, the first possible option was to extract the maxillary canine to improve the space shortage. The advantages of this method are that it would allow for early improvement of the space shortage and eliminate the need for traction on the canine. However, the maxillary canines have longer roots and may remain and function for a longer period of time compared with other tooth types [
18], so this option was considered disadvantageous both esthetically and functionally.
The second possible option was extraction of the maxillary left first premolar. This method would be effective for gaining traction space for the maxillary left canine but would be disadvantageous in that the removal of the maxillary left first premolar may cause deviation of the maxillary midline, which was aligned with the facial midline. Furthermore, it may also cause lingual inclination of the maxillary anterior teeth, whose axis was normal at the initial examination. Another disadvantage is that this option would result in an occlusal relationship with one fewer tooth than the normal dentition.
For the third option, we focused on the presence of the maxillary left third molar and examined the feasibility of extracting the second molar and distally moving the first molar to create space for the eruption of the left canine. In this method, after distal movement of the first molar, the second premolar and first premolar would be moved distally in sequence, and the canine would be aligned after the traction space has been secured, which may require a longer treatment period than other treatment methods. On the other hand, the advantage of this method is that the third molar could be aligned into the maxillary arch to obtain occlusal alignment without reducing the number of teeth.
After being informed of the expected results and the advantages and disadvantages of each treatment option, the patient and his guardians chose the third option.
For this method, we also considered the use of a unilateral first molar distal movement appliance with a screw implanted into the bone as an anchorage source, which is a common practice nowadays. However, because there were concerns about the stability of the implanted screw due to the young age of the patient (14 years), and because the patient refused to have the screw implanted, we decided to proceed with treatment using an appliance that was less surgically invasive. Although fixed maxillary molar distal movement appliances such as the pendulum and Greenfield molar distalizer appliances are commonly used, these appliances have been reported to cause distal inclination of the maxillary first molar while it is being moved distally [
19,
20]. Therefore, in the present case, we devised a maxillary molar distal movement appliance that would allow for distal bodily movement of the maxillary molar without distal inclination and used it for treatment.
5. Treatment Progress
After extraction of the maxillary left second molar, a Hyrax-type expander was applied to the maxillary arch for distal movement of the maxillary left first molar. The patient was instructed to turn the screw a quarter-turn every 3 days. In parallel with the distal movement of the left first molar, traction of the left canine in the distal-buccal direction was initiated (
Figure 6A). After about 3 months, when the patient had turned the screw a total of 32 times and an 8 mm expansion had been achieved, the occlusal relationship of the left molar was Angle Class I, indicating that the left first molar could be moved distally to the target position. The expansion screw was then fixed with resin to prevent relapse. A sectional archwire was placed on the left second premolar and first molar to initiate distal movement of the left second premolar (
Figure 6B). Distal movement of the left second premolar was completed in 3 months. The left second premolar and first molar were sequentially ligated to prevent relapse of the second premolar. Then, the band on the left first premolar was removed, and a sectional wire was placed from the left first premolar to the first molar to initiate distal movement of the left first premolar (
Figure 6C). After about 10 months, when the distal movement of the left first premolar was completed, the Hyrax-type expander was removed and an archwire was engaged in the left canine bracket to initiate leveling. In addition, to prevent the distally moved first molar from moving mesially, a lip bumper was applied to the first molars for reinforced anchorage during leveling (
Figure 6D). After about 8 months, leveling of the canines was completed and detailing was initiated (
Figure 6E). Three years and one month after the start of active treatment, detailing was completed and active treatment was terminated. Fixed retainers were placed between the maxillary and mandibular canines and on the mandibular left first and second molars, along with wraparound retainers, until the eruption of the maxillary left third molar. The maxillary wraparound retainer was designed to provide space for the eruption of the left third molar. The mandibular wraparound retainer was designed with a rest at the mandibular left second molar to prevent extrusion of the mandibular left second molar until the maxillary left third molar occluded with the opposing tooth (
Figure 6F). Three years and six months after active treatment was terminated, the maxillary left third molar had fully erupted and occluded with the mandibular left second molar. We also encouraged the patient to have the mandibular left third molars extracted, because of no occlusal contact due to a reduced number of teeth in upper left segment. In addition, the maxillary and mandibular right third molars are impacted and scheduled for extraction.
6. Treatment Results
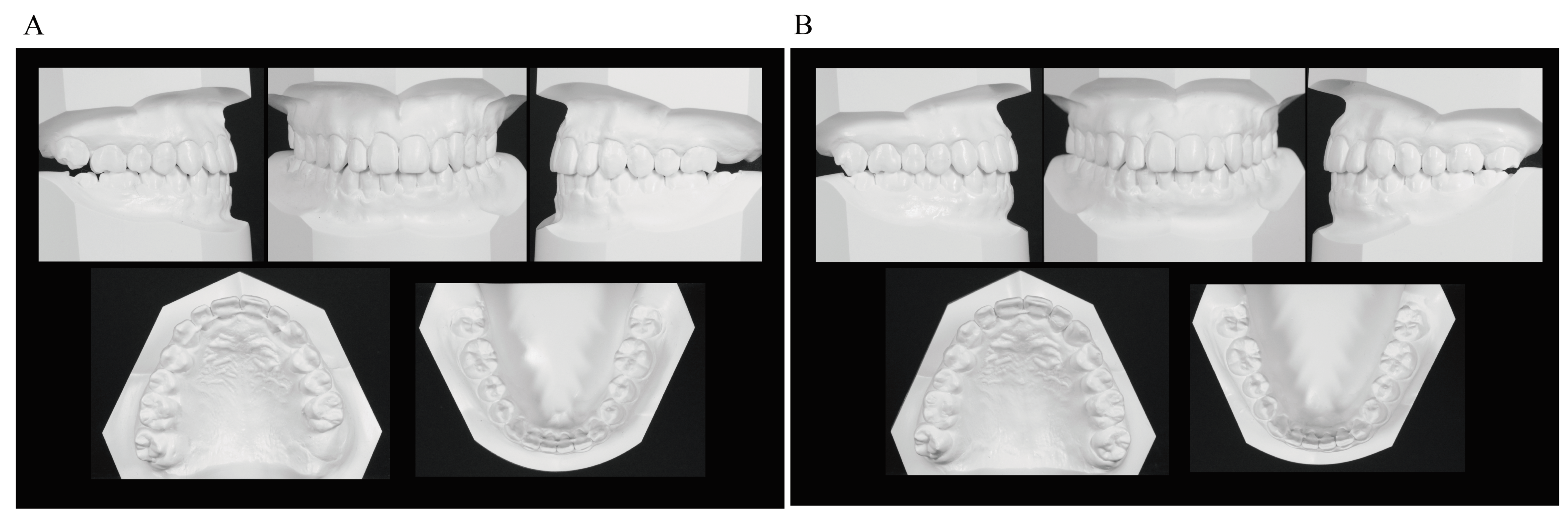
In the frontal view, the midline deviation seen at the initial presentation was corrected, with the maxillary and mandibular midlines aligned with the facial midline. In the lateral view, a good E-line was maintained. The occlusal relationship of the first molars was Angle Class I on both sides, demonstrating close occlusion. The maxillary left canine that had shown eruption disturbance was aligned in the dental arch. The maxillary left third molar naturally erupted and occluded with the mandibular left second molar. The maxillary and maxillary anterior teeth were in an appropriate covering relationship (
Figure 7 and
Figure 8).
Panoramic radiographs showed good root parallelism, no root resorption in the tractioned maxillary left canine or other teeth, and no abnormalities in the periodontal tissue. The maxillary left third molar, which had been impacted when active treatment was terminated, fully erupted 3 years and 6 months after active treatment was terminated. The maxillary right third molar and mandibular right and left third molars are impacted and scheduled for extraction (
Figure 9).
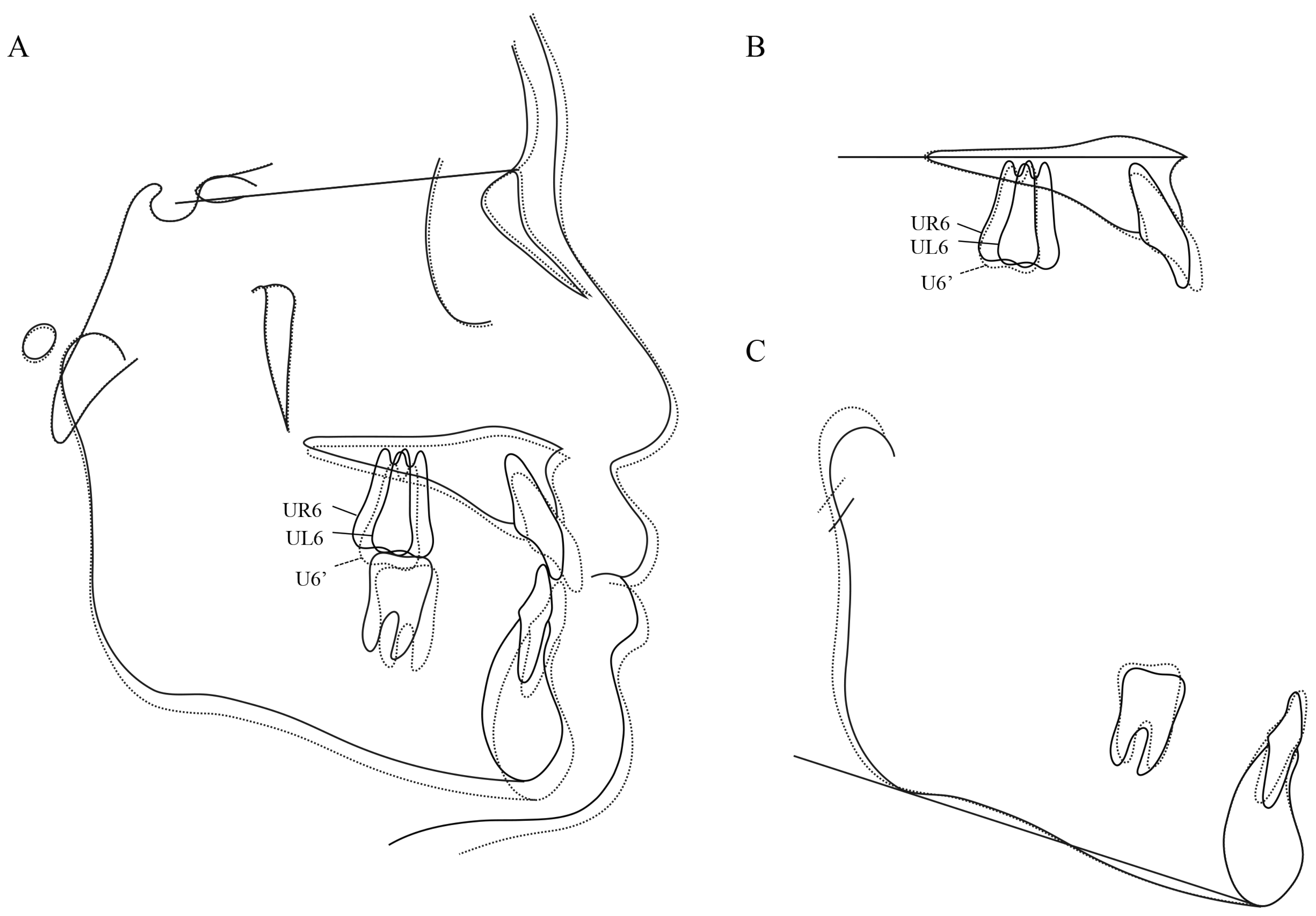
Lateral cephalometric radiography showed the following changes in the anteroposterior position of the maxillary first molars before and after the use of the Hyrax-type expander: A′-Ms from 32.5 mm to 33.0 mm for the right and from 28.0 mm to 33.0 mm for the left, and ptm′-Ms from 18.5 mm to 19.0 mm for the right and from 23.0 mm to 19.0 mm for the right. Thus, the right first molar showed no change in position while the left first molar was moved distally by about 4.5 mm to almost the same position as the right one. The axial inclination angle of the right maxillary first molar was unchanged from 83.0° while that of the left first molar decreased from 88.0° to 83.0°, indicating that the mesially inclined left first molar was caused to slightly incline distally (
Figure 10 and
Table 1).
When active treatment was terminated, SNA was increased by 0.5° compared with before active treatment was terminated due to anterior maxillary growth. Although point B was retracted, the SNB was unchanged at 88.5° due to anterior mandibular growth, which resulted in a 0.5° increase in ANB. Vertically, FMA was increased by 0.5°, indicating a slight clockwise rotation of the mandible. U-1 to NA increased to 4.0 mm/22.5°, indicating labial tipping movement of the maxillary central incisor, while the L-1 to NB increased to 4.0 mm/20.5°and the FMIA decreased from 80.5° to 73.5°, indicating labial tipping of the mandibular central incisor. This resulted in the improvement of the interincisal angle to 135.5° (
Figure 11 and
Table 1).
At completion of eruption of the maxillary left third molar, there was a slight skeletal change (ANB: 0.5° decrease; FMA: 0.5° decrease) from the termination of active treatment, but there was no change in the position of the maxillary and mandibular anterior teeth and the maxillary first molar (
Figure 12 and
Table 1).
7. Discussion
7.1. Treatment Planning Focusing on the Presence of the Third Molars
Because the maxillary canines play an important role both esthetically and functionally, it is recommended that the maximum effort be made to guide them into the dental arch even when they are erupting in abnormal positions or impacted [
18]. In the present case, the crown of the maxillary left canine had erupted near the labial root surface of the left lateral incisor, while panoramic radiographs and CBCT images showed that its root apex was located between the lateral incisor and first premolar. We therefore assumed that if the left maxillary canine could be distally inclined and tractioned, it could be aligned between the maxillary left lateral incisor and first premolar. A plan was thus made to traction the ectopically erupted maxillary left canine to align it in the dental arch. However, because of the lack of room for eruption due to the mesial positioning of the maxillary left molar, it was necessary to create space for the eruption of the maxillary left canine. The well-known methods of creating eruption space include expansion of the dental arch and extraction of anterior teeth and premolars. In the present case, however, the maxillary space shortage was 7.5 mm, which was considered difficult to obtain only by expanding the dental arch. Tooth extraction was thus considered necessary to gain eruption space.
According to previous reports, in patients with a maxillary third molar of proper size, shape, and position, extracting the maxillary second molar to allow for the eruption of the maxillary third molar is effective for improving Angle Class II malocclusion [
21,
22,
23]. Donihue et al. noted that the advantage of extracting a maxillary second molar is that it increases the efficiency of distal movement of the maxillary first molar and allows the first molars to achieve a Class I occlusal relationship [
24]. It has also been reported that extraction of the maxillary second molar results in eruption of the maxillary third molar with a likelihood of 96.2% to 99% [
25,
26]. To allow the maxillary third molar to erupt in the appropriate position, it is recommended that the second molar be extracted when the third molar reaches the root–crown junction of the second molar or when calcification of the third molar crown is almost complete [
27]. In the present case, panoramic and lateral cephalometric radiographs showed that the crown of the maxillary left third molar was upright and almost as large as that of the ipsilateral first and second molars, and calcification of the crown was almost complete. The patient also had a straight facial profile, a labially impacted maxillary canine, and Angle Class II malocclusion with a slightly under-spaced mandibular arch. These features made maxillary left second molar extraction a viable treatment option. During treatment, extraction of the maxillary left second molar allowed for efficient distal movement of the maxillary left first molar, and subsequent successful alignment of the maxillary left canine.
These results suggest that gaining eruption space for the maxillary canine by extracting the second molar and distally moving the first molar, taking into consideration the presence of the maxillary third molar and the position and size of its tooth germ, is an effective treatment method.
7.2. Development of a Maxillary Molar Distal Movement Appliance
To date, many researchers have developed new intraoral appliances for distal molar movement [
28]. The pendulum appliance is a fixed appliance for distal movement of maxillary molars that was first reported by Hilgers in 1992 [
29]; it has been shown to be capable of distal movement of maxillary molars in a relatively short period. However, with this appliance, the orthodontic force acts on the crown of the molar, which is away from the center of resistance of the tooth, making distal crown tipping likely to occur during distal movement. Acácio et al. [
19] used a pendulum appliance to distally move the maxillary first molars and reported an average 18.5° distal tipping. They also noted that this appliance can also cause mesial movement of premolars and subsequent loss of anchorage, and that care must be taken to control them. Loss of anchorage during use of a pendulum appliance has also been indicated by increased incidence of labial dislocation and tipping of the maxillary incisors [
29,
30].
In the present case, a Hyrax-type expander with a Veltri Monolateral Screw
® attached to the palate in the sagittal direction was used for distal movement of only the maxillary left first molar. For this purpose, an expansion screw, bands, and wires for connecting the abutment bands were firmly attached to the appliance to reinforce anchorage. The appliance was also designed so that the force vector of the expansion screw passed near the center of resistance of the maxillary first molar and parallel to the occlusal plane of the maxillary first molar, allowing for distal bodily movement of the maxillary first molar. Brunetto et al. [
31] and Pereira et al. [
32] investigated the frequency of activation of the expansion screw of a maxillary expander and reported that buccal bodily movement was more likely to occur when the screw was rotated twice a week for slow expansion compared with when it was expanded twice a day. In the present case, we planned to expand the screw once every 3 days, hoping to achieve distal bodily movement of the first molar while preventing its tipping. This resulted in distal movement of the left first molar by about 4.5 mm, with limited distal tipping of +5°. The maxillary central incisor axis could have been limited to a slight labial tilt by utilizing the expansion screw for additional anchorage to the mucosa and multiple teeth.
These findings suggest that the appliance used in the present case for distal movement of a unilateral molar consisting of a Hyrax-type expander with a Veltri Monolateral Screw®, with consideration of anchorage and the frequency of activation, is effective for distal bodily movement of a unilateral molar.
8. Conclusions
In cases of malocclusion with eruption disturbance of a canine, the results here indicate that gaining eruption space for the maxillary canine by extracting the second molar and distally moving the first molar, taking into consideration the presence of the maxillary third molar and the position and size of its tooth germ, is an effective treatment method. The results also suggest that the current unilateral molar distal movement appliance consisting of a Hyrax-type expander (Veltri Monolateral Screw®), with consideration of anchorage and the frequency of activation, is effective for distal bodily movement of a unilateral molar. This treatment method is also considered to be an effective alternative in patients for whom orthodontic treatment using anchor screws, which are commonly used nowadays, is not an option for reasons such as patient refusal, young age, insufficient bone thickness, and prior screw dropout.
Author Contributions
Conceptualization, K.M.; methodology, M.T. (Masako Tabuchi) and K.M.; validation, M.T. (Mifumi Takahashi) and M.T. (Masako Tabuchi); formal analysis, M.T. (Mifumi Takahashi); investigation, M.T. (Mifumi Takahashi), T.S. and R.H.; data curation, M.T. (Mifumi Takahashi) and R.H.; writing—original draft preparation, M.T. (Mifumi Takahashi); writing—review and editing, M.T. (Masako Tabuchi) and K.M.; visualization, R.H.; supervision, S.G.; project administration, S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent was obtained from the patient’s guardians to publish this paper.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kurol, J.; Ericson, S.; Andreasen, J.O. The impacted maxillary canine. In Textbook and Color Atlas of Tooth Impactions; Andreasen, J.O., Petersen, J.K., Laskin, D.M., Eds.; Munksgaard: Copenhagen, Denmark, 1997; pp. 125–165. [Google Scholar]
- Ngan, P.; Hornbrook, R.; Weaver, B. Early timely management of ectopically erupting maxillary canines. Semin Orthod. 2005, 11, 152–163. [Google Scholar] [CrossRef] [Green Version]
- Nomura, Y.; Ozaki, M.; Baba, A.; Ishikawa, H.; Motokawa, W. Investigation of impacted teeth using cone-beam computed tomography. Jpn. Soc. Pediatr. Oral. Maxillofac. Surg. 2009, 19, 122–128. [Google Scholar]
- Noda, T. Treatment guidance for eruption disturbance. Niigata Dent. J. 2000, 30, 1–13. [Google Scholar]
- Jacoby, H. The etiology of maxillary canine impactions. Am. J. Orthod. 1983, 84, 125–132. [Google Scholar] [CrossRef]
- Bishara, S.E. Impacted maxillary canines: A review. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 159–171. [Google Scholar] [CrossRef]
- Becker, A.; Chaushu, S. Etiology of maxillary canine impaction: A review. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 557–567. [Google Scholar] [CrossRef]
- Celikoglu, M.; Kamak, H.; Oktay, H. Investigation of transmigrated and impacted maxillary and mandibular canine teeth in an orthodontic patient population. J. Oral. Maxillofac. Surg. 2010, 68, 1001–1006. [Google Scholar] [CrossRef]
- Kumar, S.; Mehrotra, P.; Bhagchandani, J.; Singh, A.; Garg, A.; Kumar, S.; Sharma, A.; Yaday, H. Localization of impacted canines. J. Clin. Diagn. Res. 2015, 9, ZE11–ZE14. [Google Scholar] [CrossRef]
- Ericson, S.; Kurol, J. Radiographic examination of ectopically erupting maxillary canines. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 483–492. [Google Scholar] [CrossRef]
- Becker, A. Orthodontic Treatment of Impacted Teeth, 2nd ed.; Informa Healthcare: Abingdon, UK, 2007; pp. 1–228. [Google Scholar]
- Taguchi, Y.; Kobayashi, H.; Noda, T. The palatally displaced canine in Japanese children. Pediatr. Dent. J. 2000, 10, 155–158. [Google Scholar]
- Taguchi, Y.; Kurol, J.; Kobayashi, H.; Noda, T. Eruption disturbances of maxillary permanent canines in Japanese children. Pediatr. Dent. J. 2001, 11, 11–18. [Google Scholar]
- Noda, T.; Takagi, M.; Hayashi-Sakai, S.; Taguchi, Y. Eruption disturbances in Japanese children and adolescents. Ped. Dent. J. 2006, 16, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Manne, R.; Gandikota, C.; Juvvadi, S.R.; Rama, H.R.M.; Anche, S. Impacted canines: Etiology, diagnosis, and orthodontic management. J. Pharm. Bioallied. Sci. 2012, 4 (Suppl. 2), S234–S238. [Google Scholar]
- Byloff, F.K.; Darendeliler, M.A. Distal molar movement using the pendulum appliance. Part 1: Clinical and radiological evaluation. Angle Orthod. 1997, 67, 249–260. [Google Scholar]
- Patel, M.P.; Janson, G.; Henriques, J.F.C.; de Almeida, R.R.; de Freitas, M.R.; Pinzan, A.; de Freitas, K.M.S. Comparative distalization effects of Jones jig and pendulum appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 336–342. [Google Scholar] [CrossRef]
- Arriola-Guillén, L.E.; Ruíz-Mora, G.A.; Rodríguez-Cárdenas, Y.A.; Aliaga-Del Castillo, A.; Boessio-Vizzotto, M.; Dias-Da Silveira, H.L. Influence of impacted maxillary canine orthodontic traction complexity on root resorption of incisors: A retrospective longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 28–39. [Google Scholar] [CrossRef]
- Fuziy, A.; de Almeida, R.R.; Janson, G.; Angelieri, F.; Pinzan, A. Sagittal, vertical, and transverse changes consequent to maxillary molar distalization with the pendulum appliance. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 502–510. [Google Scholar] [CrossRef]
- Alfaifi, M.; Park, J.H.; Tai, K.; Ku, J.H.; Vaid, N.R.; Kook, Y.A.; Shoaib, A.M.; Bayome, M. Comparison of treatment effects with modified C-palatal plates vs. greenfield molar distalizer appliances in adolescents. J. Clin. Pediatr. Dent. 2020, 44, 202–208. [Google Scholar] [CrossRef]
- de Freitas, M.R.; de Lima, D.V.; de Freitas, K.M.S.; Janson, G.; Henriques, J.F.C. Strategic maxillary second-molar extraction in Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 878–886. [Google Scholar] [CrossRef]
- Basdra, E.K.; Stellzig, A.; Komposch, G. Extraction of maxillary second molars in the treatment of Class II malocclusion. Angle Orthod 1996, 66, 287–292. [Google Scholar]
- Aras, A. Class II correction with the modified sagittal appliance and maxillary second molar extraction. Angle Orthod. 2000, 70, 332–338. [Google Scholar]
- Waters, D.; Harris, E.F. Cephalometric comparison of maxillary second molar extraction and nonextraction treatments in patients with Class II malocclusions. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 608–613. [Google Scholar] [CrossRef]
- Orton-Gibbs, S.; Crow, V.; Orton, H.S. Eruption of third permanent molars after the extraction of second permanent molars. Part 1: Assessment of third molar position and size. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 226–238. [Google Scholar] [CrossRef]
- De-la-Rosa-Gay, C.; Valmaseda-Castellon, E.; Gay-Escoda, C. Spontaneous third-molar eruption after second-molar extraction in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Magness, W.B. Extraction of second molars. J. Clin. Orthod. 1986, 20, 519–522. [Google Scholar] [PubMed]
- Keles, A.; Sayinsu, K. A new approach in maxillary molar distalization: Intraoral bodily molar distalizer. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 39–48. [Google Scholar] [CrossRef]
- Hilgers, J.J. The pendulum appliance for class II non-compliance therapy. J. Clin. Orthod. 1992, 26, 706–714. [Google Scholar]
- Bussick, T.A.J.; McNamara, J.A., Jr. Dentoalveolar and skeletal changes associated with the pendulum appliance. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 333–343. [Google Scholar] [CrossRef]
- Brunetto, M.; Pereira Andriani, J.S.; Ribeiro, G.L.U.; Locks, A.; Correa, M.; Correa, L.R. Three-dimensional assessment of buccal alveolar bone after rapid and slow maxillary expansion: A clinical trial study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 633–644. [Google Scholar] [CrossRef]
- Pereira, J.S.; Jacob, H.B.; Locks, A.; Brunetto, M.; Ribeiro, G.L.U. Evaluation of the rapid and slow maxillary expansion using cone-beam computed tomography: A randomized clinical trial. Dent. Press J. Orthod. 2017, 22, 61–68. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Initial facial and intraoral photographs (age, 14 years 4 months).
Figure 1.
Initial facial and intraoral photographs (age, 14 years 4 months).
Figure 2.
Initial dental casts (age, 14 years 4 months).
Figure 2.
Initial dental casts (age, 14 years 4 months).
Figure 3.
Initial radiographs. (A) Panoramic radiograph. (B) Cone-beam computed tomography. (C) Lateral cephalogram (age, 14 years 4 months).
Figure 3.
Initial radiographs. (A) Panoramic radiograph. (B) Cone-beam computed tomography. (C) Lateral cephalogram (age, 14 years 4 months).
Figure 4.
Measurement points and lines used for determining the mesiodistal position and axial inclination angles of the maxillary first molars. A′, intersection of the palatal plane and the perpendicular line from point A; ptm′, intersection of the palatal plane and the perpendicular line from ptm; Mo, midpoint of the occlusal surface of the maxillary first molars; Ms, intersection of the palatal plane and the perpendicular line from the midpoint of the occlusal surface of the maxillary first molars; Mp, line connecting the midpoint of the occlusal surface of the maxillary first molars and the midpoint of the mesial and distal root apexes; NF, palatal plane.
Figure 4.
Measurement points and lines used for determining the mesiodistal position and axial inclination angles of the maxillary first molars. A′, intersection of the palatal plane and the perpendicular line from point A; ptm′, intersection of the palatal plane and the perpendicular line from ptm; Mo, midpoint of the occlusal surface of the maxillary first molars; Ms, intersection of the palatal plane and the perpendicular line from the midpoint of the occlusal surface of the maxillary first molars; Mp, line connecting the midpoint of the occlusal surface of the maxillary first molars and the midpoint of the mesial and distal root apexes; NF, palatal plane.
Figure 5.
Orthodontic occlusal guidance appliance. (A) Intraoral photographs. Abutment bands (*); resin button (a); lingual arch (b); canine traction hook (c). (B) Lateral cephalogram. Expansion screw (dotted line); expansion screw placement plane (a); maxillary first molar (U6) occlusal surface (b).
Figure 5.
Orthodontic occlusal guidance appliance. (A) Intraoral photographs. Abutment bands (*); resin button (a); lingual arch (b); canine traction hook (c). (B) Lateral cephalogram. Expansion screw (dotted line); expansion screw placement plane (a); maxillary first molar (U6) occlusal surface (b).
Figure 6.
Treatment progress. (A) Orthodontic occlusal guidance appliance applied. Distal movement of the maxillary left first molar started. Traction of the maxillary left canine started. (B) Distal movement of the maxillary left first molar completed. A sectional archwire was placed on the maxillary left second premolar and first molar to start distal movement of the left second premolar. (C) Distal movement of the maxillary left second premolar completed. A sectional archwire was placed from the maxillary left first premolar to the first molar to start distal movement of the left first premolar. (D) Distal movement of the maxillary left first premolar completed. Leveling of the maxillary left canine started. A lip bumper was applied to the maxillary first molars reinforced anchorage. (E) Leveling completed. Detailing started. (F) Active treatment was terminated. Fixed retainers were placed between the maxillary and mandibular canines and on the mandibular left first and second molars. Maxillary and mandibular wraparound retainers were applied.
Figure 6.
Treatment progress. (A) Orthodontic occlusal guidance appliance applied. Distal movement of the maxillary left first molar started. Traction of the maxillary left canine started. (B) Distal movement of the maxillary left first molar completed. A sectional archwire was placed on the maxillary left second premolar and first molar to start distal movement of the left second premolar. (C) Distal movement of the maxillary left second premolar completed. A sectional archwire was placed from the maxillary left first premolar to the first molar to start distal movement of the left first premolar. (D) Distal movement of the maxillary left first premolar completed. Leveling of the maxillary left canine started. A lip bumper was applied to the maxillary first molars reinforced anchorage. (E) Leveling completed. Detailing started. (F) Active treatment was terminated. Fixed retainers were placed between the maxillary and mandibular canines and on the mandibular left first and second molars. Maxillary and mandibular wraparound retainers were applied.
![Applsci 12 07620 g006]()
Figure 7.
Facial and intraoral photographs. (A) At termination of active treatment (age, 17 years 9 months). (B) At completion of eruption of the maxillary left third molar (age, 21 years 3 months).
Figure 7.
Facial and intraoral photographs. (A) At termination of active treatment (age, 17 years 9 months). (B) At completion of eruption of the maxillary left third molar (age, 21 years 3 months).
Figure 8.
Dental casts. (A) At termination of active treatment (age, 17 years 9 months). (B) At completion of eruption of the maxillary left third molar (age, 21 years 3 months).
Figure 8.
Dental casts. (A) At termination of active treatment (age, 17 years 9 months). (B) At completion of eruption of the maxillary left third molar (age, 21 years 3 months).
Figure 9.
Panoramic radiographs and lateral cephalograms. (A) At termination of active treatment (age, 17 years 9 months). (B) At completion of eruption of the maxillary left third molar (age, 21 years 3 months).
Figure 9.
Panoramic radiographs and lateral cephalograms. (A) At termination of active treatment (age, 17 years 9 months). (B) At completion of eruption of the maxillary left third molar (age, 21 years 3 months).
Figure 10.
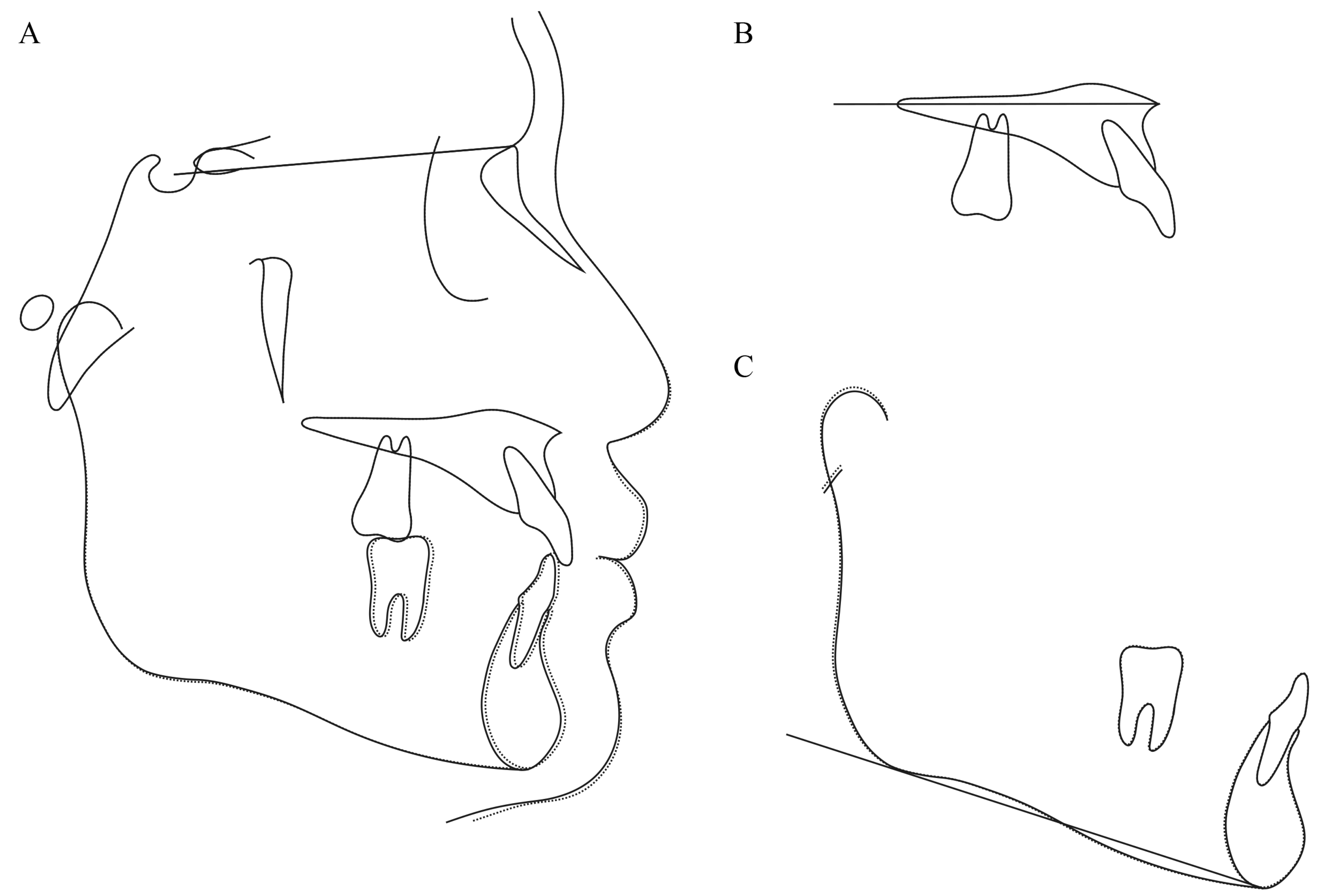
Superimposition at the start of active treatment and at removal of the Hyrax-type expander. At the start of active treatment (14 years 4 months) (solid line); at removal of the Hyrax-type expander (15 years 8 months) (dashed line). (A) On the SN plane at S. (B) On the palatal plane at ANS. (C) On the mandibular plane at Me. Maxillary left first molar at the start of active treatment (UL6); left first molar at removal of the Hyrax-type expander (UL6′); maxillary right first molar at the start of active treatment (UR6); maxillary right first molar of the Hyrax-type expander (UR6′).
Figure 10.
Superimposition at the start of active treatment and at removal of the Hyrax-type expander. At the start of active treatment (14 years 4 months) (solid line); at removal of the Hyrax-type expander (15 years 8 months) (dashed line). (A) On the SN plane at S. (B) On the palatal plane at ANS. (C) On the mandibular plane at Me. Maxillary left first molar at the start of active treatment (UL6); left first molar at removal of the Hyrax-type expander (UL6′); maxillary right first molar at the start of active treatment (UR6); maxillary right first molar of the Hyrax-type expander (UR6′).
Figure 11.
Superimposition at the start of active treatment and at termination of active treatment. (A) On the SN plane at S. (B) On the palatal plane at ANS. (C) On the mandibular plane at Me. At the start of active treatment (14 years 4 months) (solid line); at termination of active treatment (17 years 9 months) (dashed line). Maxillary right first molar at the start of active treatment (UR6); maxillary left first molar at the start of active treatment (UL6); maxillary first molar at termination of active treatment (midpoint of the left and right sides) (U6′).
Figure 11.
Superimposition at the start of active treatment and at termination of active treatment. (A) On the SN plane at S. (B) On the palatal plane at ANS. (C) On the mandibular plane at Me. At the start of active treatment (14 years 4 months) (solid line); at termination of active treatment (17 years 9 months) (dashed line). Maxillary right first molar at the start of active treatment (UR6); maxillary left first molar at the start of active treatment (UL6); maxillary first molar at termination of active treatment (midpoint of the left and right sides) (U6′).
Figure 12.
Superimposition at termination of active treatment and at completion of eruption of the maxillary left third molar. (A) On the SN plane at S. (B) On the palatal plane at ANS. (C) On the mandibular plane at Me. At termination of active treatment (17 years 9 months) (solid line); at completion of eruption of the maxillary left third molar (21 years 3 months) (dashed line).
Figure 12.
Superimposition at termination of active treatment and at completion of eruption of the maxillary left third molar. (A) On the SN plane at S. (B) On the palatal plane at ANS. (C) On the mandibular plane at Me. At termination of active treatment (17 years 9 months) (solid line); at completion of eruption of the maxillary left third molar (21 years 3 months) (dashed line).
Table 1.
Cephalometric measurements.
Table 1.
Cephalometric measurements.
| | At Start of Active Treatment (14 y 4 m) | At Removal of the Hyrax-Type Expander (15 y 8 m) | At Termination of Active Treatment (17 y 9 m) | At Completion of Eruption of the Maxillary Left Third Molar (21 y 3 m) |
|---|
| ∠SNA (°) | 90.5 | 91.5 | 91.0 | 91.0 |
| ∠SNB (°) | 88.5 | 90.0 | 88.5 | 89.0 |
| ∠ANB (°) | +2.0 | +1.5 | +2.5 | +2.0 |
| ∠FMA (°) | 14.0 | 14.0 | 14.5 | 14.0 |
| U1 to NA (mm/°) | 2.0/14.0 | 3.0/17.0 | 4.0/22.5 | 4.0/22.5 |
| L1 to NB (mm/°) | 2.0/14.5 | 3.0/17.0 | 4.0/20.5 | 4.0/20.5 |
| ∠FMIA (°) | 80.5 | 77.5 | 73.5 | 73.5 |
| Interincisal angle (°) | 150.0 | 136.5 | 135.0 | 135.0 |
| A′-ptm′ (mm) | 51.0 | 52.0 | 56.0 | 56.0 |
| A′-Ms (mm) (R/L) | 32.5/28.0 | 33.0/33.0 | 36.0 | 36.0 |
| ptm′-Ms (mm) (R/L) | 18.5/23.0 | 19.0/19.0 | 20.0 | 20.0 |
| Maxillary first molar axial inclination angle, α (°) (R/L) | 83.0/88.0 | 83.0/83.0 | 82.0 | 82.0 |
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}