
Impact of Rehabilitation on Fatigue in Post-COVID-19 Patients: A Systematic Review and Meta-Analysis
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
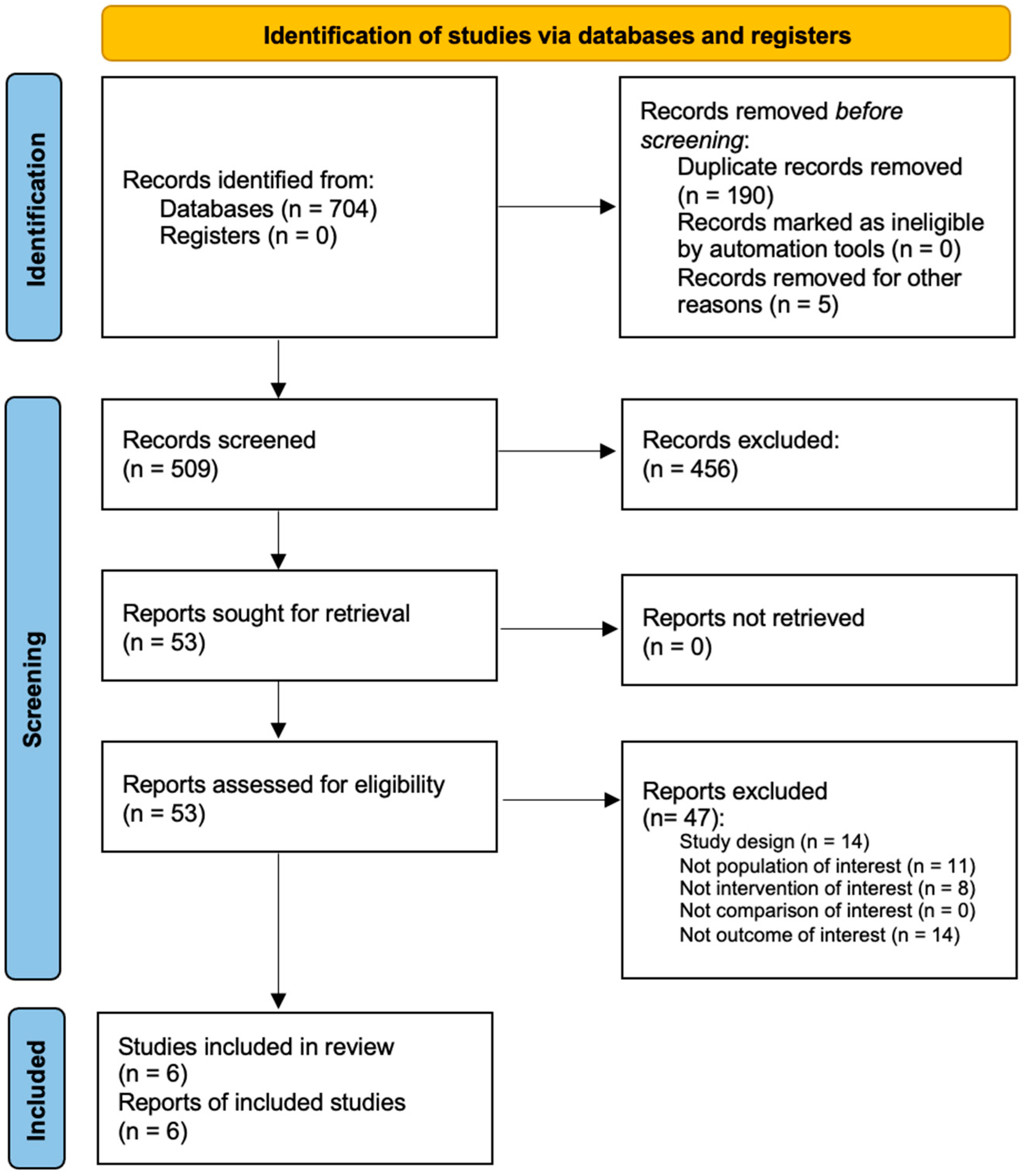
2.1. Search Strategy
2.2. Selection Criteria
- -
- (P) Participants: patients affected by PCS;
- -
- (I) Intervention: rehabilitative interventions;
- -
- (C) Comparator: not applicable;
- -
- (O) Outcome measure: fatigue evaluation through an evaluation tool that quantified the perceived exertion (i.e., fatigue severity scale (FSS); Borg Scale (BS); Borg Category Ratio 10 (CR10); Checklist Individual Strength (CIS) fatigue scale; FACIT (Functional Assessment of Chronic Illness Therapy) fatigue scale).
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Main Findings of the Included Studies
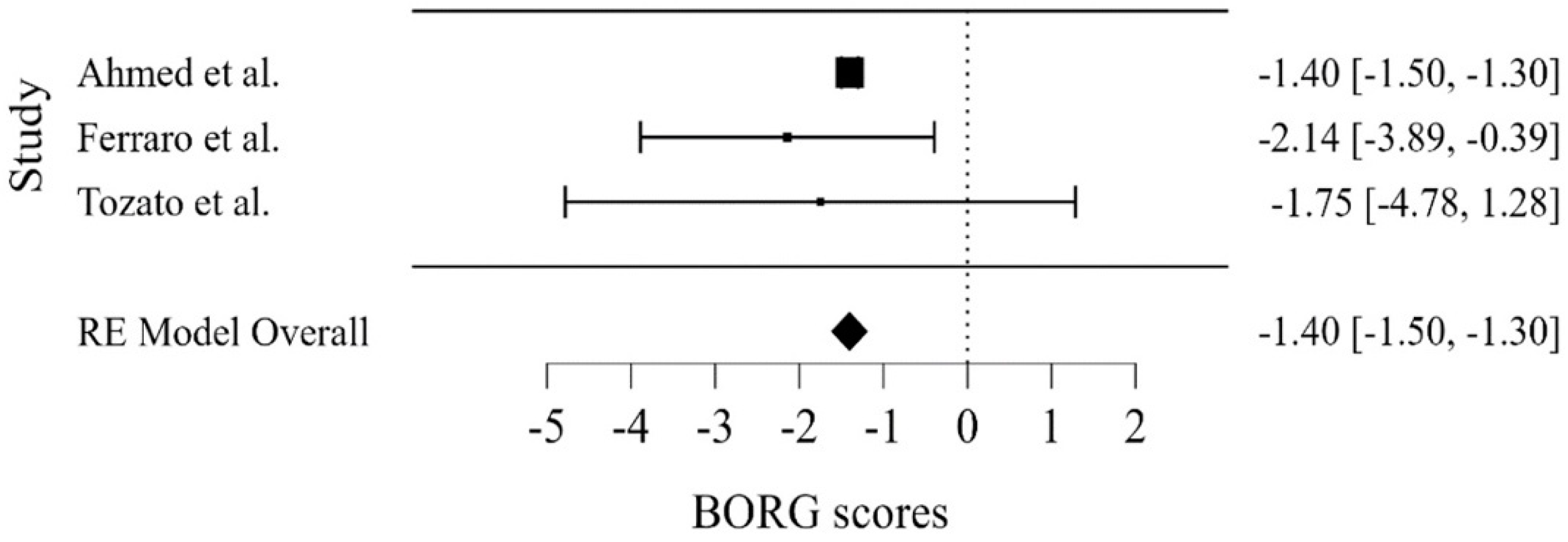
3.3. Meta-Analysis
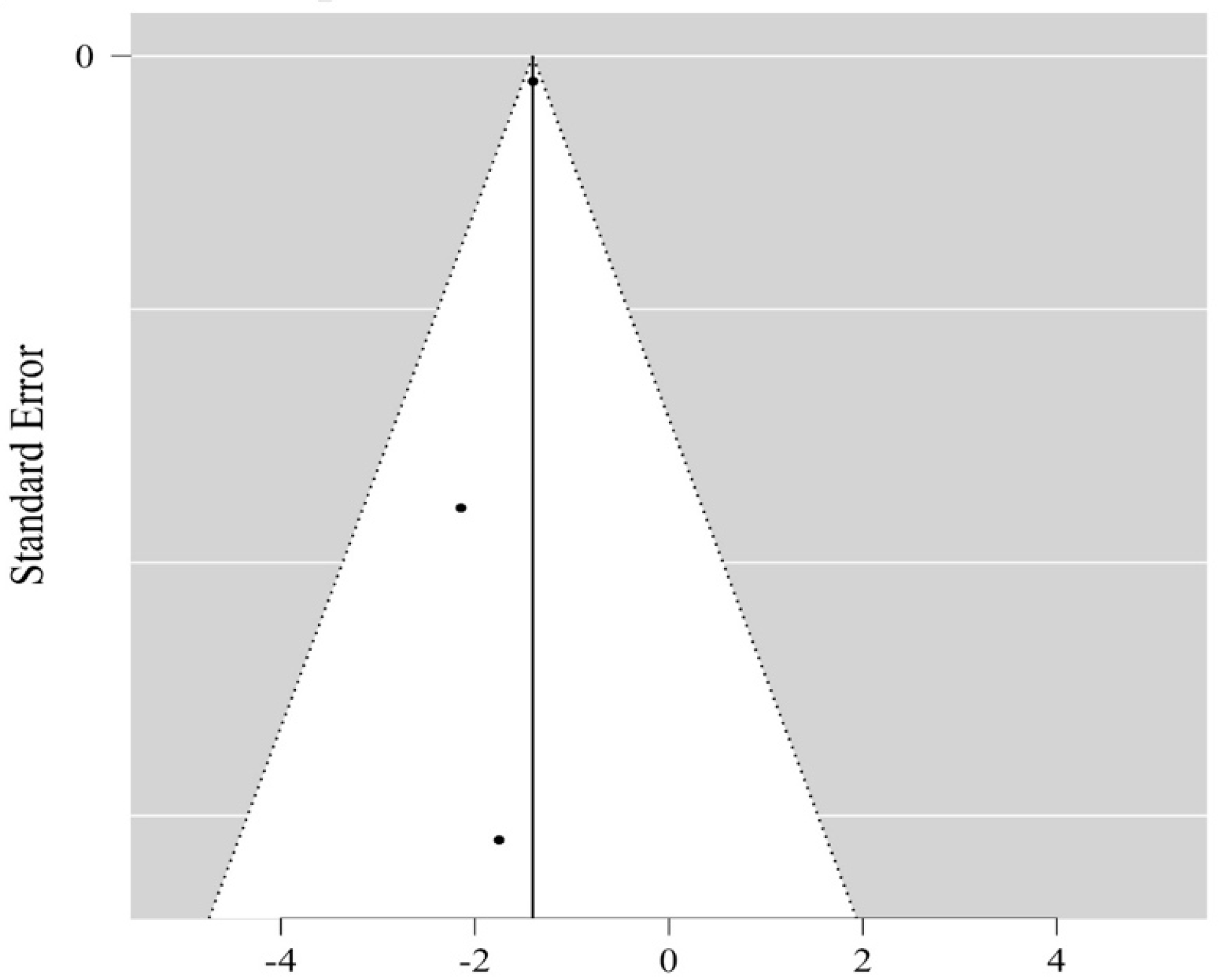
3.4. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiekens, C.; Boldrini, P.; Andreoli, A.; Avesani, R.; Gamna, F.; Grandi, M.; Lombardi, F.; Lusuardi, M.; Molteni, F.; Perboni, A.; et al. Rehabilitation and respiratory management in the acute and early post-acute phase. “Instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur. J. Phys. Rehabil. Med. 2020, 56, 323–326. [Google Scholar] [CrossRef]
- Azuma, K.; Yanagi, U.; Kagi, N.; Kim, H.; Ogata, M.; Hayashi, M. Environmental factors involved in SARS-CoV-2 transmission: Effect and role of indoor environmental quality in the strategy for COVID-19 infection control. Environ. Health Prev. Med. 2020, 25, 66. [Google Scholar] [CrossRef]
- Sanli, D.E.T.; Altundag, A.; Kandemirli, S.G.; Yildirim, D.; Sanli, A.N.; Saatci, O.; Kirisoglu, C.E.; Dikensoy, O.; Murrja, E.; Yesil, A.; et al. Relationship between disease severity and serum IL-6 levels in COVID-19 anosmia. Am. J. Otolaryngol. 2021, 42, 102796. [Google Scholar] [CrossRef]
- Corner, E.; Wood, H.; Englebretsen, C.; Thomas, A.; Grant, R.; Nikoletou, D.; Soni, N. The Chelsea Critical Care Physical Assessment Tool (CPAx): Validation of an innovative new tool to measure physical morbidity in the general adult critical care population; an observational proof-of-concept pilot study. Physiotherapy 2013, 99, 33–41. [Google Scholar] [CrossRef]
- de Sire, A.; Giray, E.; Taskiran, O.O. Chelsea physical assessment tool for evaluating functioning in post-intensive care unit COVID-19 patients. J. Med. Virol. 2021, 93, 2620–2622. [Google Scholar] [CrossRef]
- Boldrini, P.; Bernetti, A.; Fiore, P.; SIMFER Executive Committee; SIMFER Committee for International Affairs. Impact of COVID-19 outbreak on rehabilitation services and Physical and Rehabilitation Medicine physicians’ activities in Italy. An official document of the Italian PRM Society (SIMFER). Eur. J. Phys. Rehabil. Med. 2020, 56, 316–318. [Google Scholar] [CrossRef]
- Brugliera, L.; Spina, A.; Castellazzi, P.; Cimino, P.; Tettamanti, A.; Houdayer, E.; Arcuri, P.; Alemanno, F.; Mortini, P.; Iannaccone, S. Rehabilitation of COVID-19 patients. J. Rehabil. Med. 2020, 52, jrm00046. [Google Scholar] [CrossRef]
- Taskiran, O.O.; Turan, Z.; Tekin, S.; Senturk, E.; Topaloglu, M.; Yurdakul, F.; Ergonul, O.; Cakar, N. Physical rehabilitation in Intensive Care Unit in acute respiratory distress syndrome patients with COVID-19. Eur. J. Phys. Rehabil. Med. 2021, 57, 434–442. [Google Scholar] [CrossRef]
- Demeco, A.; Marotta, N.; Barletta, M.; Pino, I.; Marinaro, C.; Petraroli, A.; Moggio, L.; Ammendolia, A. Rehabilitation of patients post-COVID-19 infection: A literature review. J. Int. Med. Res. 2020, 48, 0300060520948382. [Google Scholar] [CrossRef]
- Agostini, F.; Mangone, M.; Ruiu, P.; Paolucci, T.; Santilli, V.; Bernetti, A. Rehabilitation setting during and after COVID-19: An overview on recommendations. J. Rehabil. Med. 2021, 53, jrm00141. [Google Scholar] [CrossRef]
- Andrenelli, E.; Negrini, F.; de Sire, A.; Arienti, C.; Patrini, M.; Negrini, S.; Ceravolo, M.G.; International Multiprofessional Steering Committee of Cochrane Rehabilitation REH-COVER action. Systematic rapid living review on rehabilitation needs due to COVID-19: Update to May 31st, 2020. Eur. J. Phys. Rehabil. Med. 2020, 56, 508–514. [Google Scholar] [CrossRef]
- de Sire, A.; Andrenelli, E.; Negrini, F.; Lazzarini, S.G.; Ceravolo, M.G. Rehabilitation and COVID-19: The Cochrane Rehabilitation 2020 rapid living systematic review. Update as of 31 August 2020. Eur. J. Phys. Rehabil. Med. 2020, 56, 839–845. [Google Scholar] [CrossRef]
- de Sire, A.; Andrenelli, E.; Negrini, F.; Patrini, M.; Lazzarini, S.G.; Ceravolo, M.G.; International Multiprofessional Steering Committee of Cochrane Rehabilitation REH-COVER Action. Rehabilitation and COVID-19: A rapid living systematic review by Cochrane Rehabilitation Field updated as of December 31st, 2020 and synthesis of the scientific literature of 2020. Eur. J. Phys. Rehabil. Med. 2021, 57, 161–188. [Google Scholar] [CrossRef]
- Aytür, Y.K.; Köseoğlu, B.F.; Taşkıran, Ö.Ö.; Ordu-Gökkaya, N.K.; Delialioğlu, S.Ü.; Tur, B.S.; Sarıkaya, S.; Şirzai, H.; Tiftik, T.T.; Alemdaroğlu, E.; et al. Pulmonary rehabilitation principles in SARS-CoV-2 infection (COVID-19): A guideline for the acute and subacute rehabilitation. Turk. J. Phys. Med. Rehabil. 2020, 66, 104–120. [Google Scholar] [CrossRef]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]
- Bai, A.V.; Rabasco, J.; Ceccatelli, V.; Floridia, S.; Sbardella, S.; Petrignani, C.; Agostini, F.; Paoloni, M. Suggestions for changes in professional procedures and adaptation to COVID-19: New models of care in the rehabilitation setting. Ann. Ig. Med. Prev. E Comunita 2021, 33, 299–304. [Google Scholar]
- Inoue, S.; Hatakeyama, J.; Kondo, Y.; Hifumi, T.; Sakuramoto, H.; Kawasaki, T.; Taito, S.; Nakamura, K.; Unoki, T.; Kawai, Y.; et al. Post-intensive care syndrome: Its pathophysiology, prevention, and future directions. Acute Med. Surg. 2019, 6, 233–246. [Google Scholar] [CrossRef]
- Simpson, R.; Robinson, L. Rehabilitation After Critical Illness in People with COVID-19 Infection. Am. J. Phys. Med. Rehabil. 2020, 99, 470–474. [Google Scholar] [CrossRef]
- Mandal, S.; Barnett, J.; E Brill, S.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; E Hillman, T.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2020, 76, 396–398. [Google Scholar] [CrossRef]
- Venkatesan, P. NICE guideline on long COVID. Lancet Respir. Med. 2021, 9, 129. [Google Scholar] [CrossRef]
- Perrin, R.; Riste, L.; Hann, M.; Walther, A.; Mukherjee, A.; Heald, A. Into the looking glass: Post-viral syndrome post COVID-19. Med. Hypotheses 2020, 144, 110055. [Google Scholar] [CrossRef]
- Fugazzaro, S.; Contri, A.; Esseroukh, O.; Kaleci, S.; Croci, S.; Massari, M.; Facciolongo, N.C.; Besutti, G.; Iori, M.; Salvarani, C.; et al. Rehabilitation Interventions for Post-Acute COVID-19 Syndrome: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5185. [Google Scholar] [CrossRef]
- Humphreys, H.; Kilby, L.; Kudiersky, N.; Copeland, R. Long COVID and the role of physical activity: A qualitative study. BMJ Open 2021, 11, e047632. [Google Scholar] [CrossRef]
- Wong, T.L.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)—A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Alhumayn, A.; Alsaif, I.; Enabi, J.; Bin Nafisah, S. A systematic review of the systematic review of post COVID-19 syndrome. J. Med. Law Public Health 2022, 2, 64–69. [Google Scholar] [CrossRef]
- Willi, S.; Lüthold, R.; Hunt, A.; Hänggi, N.V.; Sejdiu, D.; Scaff, C.; Bender, N.; Staub, K.; Schlagenhauf, P. COVID-19 sequelae in adults aged less than 50 years: A systematic review. Travel Med. Infect. Dis. 2021, 40, 101995. [Google Scholar] [CrossRef]
- Pizarro-Pennarolli, C.; Sánchez-Rojas, C.; Torres-Castro, R.; Vera-Uribe, R.; Sanchez-Ramirez, D.C.; Vasconcello-Castillo, L.; Solís-Navarro, L.; Rivera-Lillo, G. Assessment of activities of daily living in patients post COVID-19: A systematic review. PeerJ 2021, 9, e11026. [Google Scholar] [CrossRef]
- Alizadehsani, R.; Sani, Z.A.; Behjati, M.; Roshanzamir, Z.; Hussain, S.; Abedini, N.; Hasanzadeh, F.; Khosravi, A.; Shoeibi, A.; Roshanzamir, M.; et al. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. J. Med. Virol. 2021, 93, 2307–2320. [Google Scholar] [CrossRef]
- Liang, L.; Yang, B.; Jiang, N.; Fu, W.; He, X.; Zhou, Y.; Ma, W.-L.; Wang, X. Three-Month follow-up Study of Survivors of Coronavirus Disease 2019 after Discharge. J. Korean Med. Sci. 2020, 35, e418. [Google Scholar] [CrossRef]
- van den Borst, B.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.H.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive health assessment three months after recovery from acute COVID-19. Clin. Infect Dis. 2020, 73, e1089–e1098. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K. Management of shoulder pain in patients with stroke. Postgrad. Med. J. 2001, 77, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Daher, A.; Balfanz, P.; Cornelissen, C.; Müller, A.; Bergs, I.; Marx, N.; Müller-Wieland, D.; Hartmann, B.; Dreher, M.; Müller, T. Follow up of patients with severe coronavirus disease 2019 (COVID-19): Pulmonary and extrapulmonary disease sequelae. Respir. Med. 2020, 174, 106197. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Telles, A.; López-Romero, S.; Figueroa-Hurtado, E.; Pou-Aguilar, Y.N.; Wong, A.W.; Milne, K.M.; Ryerson, C.J.; Guenette, J.A. Pulmonary function and functional capacity in COVID-19 survivors with persistent dyspnoea. Respir. Physiol. Neurobiol. 2021, 288, 103644. [Google Scholar] [CrossRef]
- Frota, A.X.; Vieira, M.C.; Soares, C.C.S.; da Silva, P.S.; da Silva, G.M.S.; Mendes, F.D.S.N.S.; Mazzoli-Rocha, F.; Veloso, H.H.; da Costa, A.D.; Lamas, C.D.C.; et al. Functional capacity and rehabilitation strategies in COVID-19 patients: Current knowledge and challenges. Rev. Soc. Bras. Med. Trop. 2021, 54, e07892020. [Google Scholar] [CrossRef]
- Mayer, K.P.; Steele, A.K.; Soper, M.K.; Branton, J.D.; Lusby, M.L.; Kalema, A.G.; E Dupont-Versteegden, E.; Montgomery-Yates, A. Physical Therapy Management of an Individual with Post-COVID Syndrome: A Case Report. Phys. Ther. 2021, 101, pzab098. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 30 June 2022).
- Whiting, P.; Rutjes, A.W.S.; Reitsma, J.B.; Bossuyt, P.M.M.; Kleijnen, J. The development of QUADAS: A tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med. Res. Methodol. 2003, 3, 25. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid.-Based Health 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Ferraro, F.; Calafiore, D.; Dambruoso, F.; Guidarini, S.; de Sire, A. COVID-19 related fatigue: Which role for rehabilitation in post-COVID-19 patients? A case series. J. Med. Virol. 2020, 93, 1896–1899. [Google Scholar] [CrossRef] [PubMed]
- Tozato, C.; Ferreira, B.F.C.; Dalavina, J.P.; Molinari, C.V.; Alves, V.L.D.S. Cardiopulmonary rehabilitation in post-COVID-19 patients: Case series. Rev. Bras. Ter. Intensiva. 2021, 33, 167–171. [Google Scholar]
- Wootton, S.L.; King, M.; Alison, J.A.; Mahadev, S.; Chan, A.S.L. COVID-19 rehabilitation delivered via a telehealth pulmonary rehabilitation model: A case series. Respirol. Case Rep. 2020, 8, e00669. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Bin Inam, A.; Belli, S.; Ahmad, J.; Khalil, W.; Jafar, M.M. Effectiveness of aerobic exercise training program on cardio-respiratory fitness and quality of life in patients recovered from COVID-19. Eur. J. Physiother. 2021, 1–6. [Google Scholar] [CrossRef]
- Daynes, E.; Gerlis, C.; Chaplin, E.; Gardiner, N.; Singh, S.J. Early experiences of rehabilitation for individuals post-COVID to improve fatigue, breathlessness exercise capacity and cognition–A cohort study. Chronic Respir. Dis. 2021, 18, 14799731211015691. [Google Scholar] [CrossRef]
- Bickton, F.M.; Chisati, E.; Rylance, J.; Morton, B. An Improvised Pulmonary Telerehabilitation Program for Postacute COVID-19 Patients Would Be Feasible and Acceptable in a Low-Resource Setting. Am. J. Phys. Med. Rehabil. 2021, 100, 209–212. [Google Scholar] [CrossRef]
- Negrini, S.; Kiekens, C.; Bernetti, A.; Capecci, M.; Ceravolo, M.G.; Lavezzi, S.; Zampolini, M.; Boldrini, P. Telemedicine from research to practice during the pandemic. “Instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur. J. Phys. Rehabil. Med. 2020, 56, 327–330. [Google Scholar] [CrossRef]
- VanElzakker, M.B.; Brumfield, S.A.; Mejia, P.S.L. Neuroinflammation and Cytokines in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): A Critical Review of Research Methods [published correction appears in Front Neurol. 2019 Apr 02;10:316] [published correction appears in Front Neurol. 2020 Sep 17;11:863]. Front. Neurol. 2019, 9, 1033. [Google Scholar] [CrossRef]
- Wostyn, P. COVID-19 and chronic fatigue syndrome: Is the worst yet to come? Med. Hypotheses 2021, 146, 110469. [Google Scholar] [CrossRef] [PubMed]
- van Erp, L.W.; Roosenboom, B.; Komdeur, P.; Dijkstra-Heida, W.; Wisse, J.; Horje, C.S.H.T.; Liem, C.S.; van Cingel, R.E.H.; Wahab, P.J.; Groenen, M.J.M. Improvement of Fatigue and Quality of Life in Patients with Quiescent Inflammatory Bowel Disease following a Personalized Exercise Program. Dig. Dis. Sci. 2021, 66, 597–604. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Harvey, N. The concept of “fatigue” in tackling COVID-19. BMJ 2020, 371, m4171. [Google Scholar] [CrossRef] [PubMed]
- Ream, E.; Richardson, A. Fatigue in patients with cancer and chronic obstructive airways disease: A phenomenological enquiry. Int. J. Nurs. Stud. 1997, 34, 44–53. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Marinaro, C.; Curci, C.; Invernizzi, M.; Ammendolia, A. Role of Physical Exercise and Nutraceuticals in Modulating Molecular Pathways of Osteoarthritis. Int. J. Mol. Sci. 2021, 22, 5722. [Google Scholar] [CrossRef]
- Atan, T.; Özyemişci Taşkıran, Ö.; Bora Tokçaer, A.; Kaymak Karataş, G.; Karakuş Çalışkan, A.; Karaoğlan, B. Effects of different percentages of body weight-supported treadmill training in Parkinson’s disease: A double-blind randomized controlled trial. Turk. J. Med. Sci. 2019, 49, 999–1007. [Google Scholar] [CrossRef]
- Nardone, O.M.; de Sire, R.; Petito, V.; Testa, A.; Villani, G.; Scaldaferri, F.; Castiglione, F. Inflammatory Bowel Diseases and Sarcopenia: The Role of Inflammation and Gut Microbiota in the Development of Muscle Failure. Front. Immunol. 2021, 12, 694217. [Google Scholar] [CrossRef]
- Kim, Y.; Lai, B.; Mehta, T.; Thirumalai, M.; Padalabalanarayanan, S.; Rimmer, J.H.; Motl, R.W. Exercise Training Guidelines for Multiple Sclerosis, Stroke, and Parkinson Disease: Rapid Review and Synthesis. Am. J. Phys. Med. Rehabil. 2019, 98, 613–621. [Google Scholar] [CrossRef]
- Tew, G.A.; Leighton, D.; Carpenter, R.; Anderson, S.; Langmead, L.; Ramage, J.; Faulkner, J.; Coleman, E.; Fairhurst, C.; Seed, M.; et al. High-intensity interval training and moderate-intensity continuous training in adults with Crohn’s disease: A pilot randomised controlled trial. BMC Gastroenterol. 2019, 19, 19. [Google Scholar] [CrossRef]
- Kujala, U.M. Evidence on the effects of exercise therapy in the treatment of chronic disease. Br. J. Sports Med. 2009, 43, 550–555. [Google Scholar] [CrossRef]
- Schiavi, M.; Fugazzaro, S.; Bertolini, A.; Denti, M.; Mainini, C.; Accogli, M.A.; Bedogni, G.; Ghizzoni, D.; Esseroukh, O.; Gualdi, C.; et al. “Like before, but not exactly”: The Qualy-REACT qualitative inquiry into the lived experience of long COVID. BMC Public Health 2022, 22, 599. [Google Scholar] [CrossRef] [PubMed]
- Marotta, N.; Demeco, A.; Moggio, L.; Ammendolia, A. Why is telerehabilitation necessary? A pre-post COVID-19 comparative study of ICF activity and participation. J. Enabling Technol. 2021, 15, 117–121. [Google Scholar] [CrossRef]
- Sanchez-Ramirez, D.; Normand, K.; Zhaoyun, Y.; Torres-Castro, R. Long-Term Impact of COVID-19: A Systematic Review of the Literature and Meta-Analysis. Biomedicines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C. Concern coronavirus may trigger post-viral fatigue syndromes. New Sci. (1971) 2020, 246, 10–11. [Google Scholar] [CrossRef]
- Paneroni, M.; Simonelli, C.; Saleri, M.; Bertacchini, L.; Venturelli, M.; Troosters, T.; Ambrosino, N.; Vitacca, M. Muscle Strength and Physical Performance in Patients without Previous Disabilities Recovering from COVID-19 Pneumonia. Am. J. Phys. Med. Rehabil. 2021, 100, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, M.; Nel, J.; Blumberg, L.; A Madhi, S.; Dryden, M.; Stevens, W.; Venter, F.W.D. Long-COVID: An evolving problem with an extensive impact. S. Afr. Med. J. 2020, 111, 10–12. [Google Scholar] [CrossRef]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PubMed (“coronavirus” OR “COVID-19” OR “post-COVID” or “long COVID”) AND (“rehabilitation” OR “exercise” OR “physical therapy” OR “telemedicine” OR “telerehabilitation”) AND (“fatigue” OR “Borg” OR “fatigue severity scale” OR “FSS” OR “FACIT” OR “CIS”) |
| Scopus TITLE-ABS-KEY (((“coronavirus” OR “COVID-19” OR “post-COVID” or “long COVID”) AND (“rehabilitation” OR “exercise” OR “physical therapy” OR “telemedicine” OR “telerehabilitation”) AND (“fatigue” OR “Borg” OR “fatigue severity scale” OR “FSS” OR “FACIT” OR “CIS”))) |
| Web of Science ((“coronavirus” OR “COVID-19” OR “post-COVID” or “long COVID”) AND (“rehabilitation” OR “exercise” OR “physical therapy” OR “telemedicine” OR “telerehabilitation”) AND (“fatigue” OR “Borg” OR “fatigue severity scale” OR “FSS” OR “FACIT” OR “CIS”)) |
| Articles excluded after title and abstract screening phase (n = 456) * | |
| Study design | 139 (31%) |
| Not population of interest | 173 (38%) |
| Not intervention of interest | 132 (29%) |
| Not comparison of interest | 0 (0%) |
| Not outcome of interest | 12 (3%) |
| Articles excluded after full-text screening phase (n = 47) | |
| Study design | 14 (30%) |
| Not population of interest | 11 (24%) |
| Not intervention of interest | 8 (17%) |
| Not comparison of interest | 0 (0%) |
| Not outcome of interest | 14 (30%) |
| Article | Nationality | Study Design | Study Group | Intervention | Outcome | Main Findings |
|---|---|---|---|---|---|---|
| Ferraro et al. [44] Journal of Medical Virology 2020 | Italy | Case series | n tot = 7 male/female = 5/2 mean age = 43.8 years LOS in ICU = 4.7 days LOS in COVID-19 Unit = 16.57 days LOS in Rehabilitation Unit = nr | Increased-intensity physical exercises 1/2 sessions per day of 30 min each for 6 days/week | Borg CR10 | At baseline, 86% of patients presented COVID-19-related fatigue, but after rehabilitation treatment, 71% did not show any fatigue. |
| Tozato et al. [45] Revista Brasileira de Terapia Intensiva, 2020 | Brazil | Case series | n tot = 4 male/female = 2/2 mean age = 56 years LOS in ICU = 15 days LOS in COVID-19 Unit = 19.75 days LOS in Rehabilitation Unit = 90 days | Aerobic exercise 3 times/week, 30 min, resistance exercise 3 times/week, 3 series of 10 repetitions each | Borg CR10 | At the end of the treatment, CR10-associated dyspnea variables were reduced for all cases. |
| Wootton et al. [46] Respirology Case Reports, 2020. | Australia | Case series | n tot = 3 male/female = 3/0 mean age = 70.6 years LOS in ICU = 1.33 days LOS in COVID-19 Unit = 12 days LOS in Rehabilitation Unit = 42 days | Individual telerehabilitation program, including education and progressive exercise sessions (15–30 min each) featuring breathing, aerobic, and strength training | 5 STS, 1 min STS, FSS, mMRC | Fatigue score on the FSS worsened at the six-week time-point in two cases. Patients demonstrated improvements from commencement of rehabilitation to the six-week time-point on the 5 STS and 1 min STS. |
| Bickton et al. [49] American Journal of Medicine & Rehabilitation, 2021 | Malawi | Case report | n tot = 1 male/female = 1/0 mean age = 46 years LOS in ICU = 0 days LOS in COVID-19 Unit = 10 days LOS in Rehabilitation Unit = 21 days | Individual telerehabilitation program, using a treatable traits approach, with weekly contact by a physiotherapist with multidisciplinary team (MDT) input | mMRC, CIS-Fatigue | At the end of the treatment, the CIS fatigue scale score was 11, indicating normal fatigue. |
| Article | Nationality | Study Design | Study Group | Intervention | Outcome | Main Findings |
|---|---|---|---|---|---|---|
| Ahmed et al. [47] European Journal of Physiotherapy, 2021 | Pakistan | Prospective interventional study | n tot = 20 male/female = 13/7 mean age = 39.6 years LOS in ICU = 3–5 days LOS in COVID-19 Unit = 5–8 days LOS in Rehabilitation Unit = nr | 5 weeks (3 session/week) of aerobic training (20–60 min/session) and breathing exercise training (10 min/session) | 6 MWT, Modified Borg dyspnea scale evaluated before and after treatment. | At the end of the treatment, there was a statistically significant improvement in performance at the 6 MWT (635.3 ± 11.6 vs. 560.3 ± 11.3; p < 0.001) and at the Borg Dyspnea Scale (3.1 ± 0.1 vs. 4.5 ± 0.2; p < 0.001) |
| Daynes et al. [48] Chronic Respiratory Disease, 2021 | United Kingdom | Observational study | n tot = 30 male/female = 16/14 mean age = 58 years LOS in ICU = nr LOS in COVID-19 Unit = 10 days LOS in Rehabilitation Unit = nr | 6 weeks (2 session/week) of aerobic exercise, strength training of upper and lower limbs and educational discussions | ISWT, ESWT, FACIT evaluated before and after treatment. | At the end of the treatment there was significant improvements in clinical outcomes of walking capacity as ISWT (413 [229] vs. 300 [198] m; p < 0.01) and ESWT (837 [406] vs. 292 [260]; p < 0.01). Moreover, there was a statistically significant increase in FACIT values (34 [13] vs. 29 [14]; p < 0.01) |
| Author and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|
| Ferraro et al. [44] | N/A | N/A | Y | N | Y | Y | Y | Y | Y |
| Tozato et al. [45] | N/A | N/A | Y | N | Y | Y | N | Y | Y |
| Wootton et al. [46] | N/A | N/A | Y | N | Y | Y | Y | Y | Y |
| Ahmed et al. [47] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Daynes et al. [48] | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Bickton et al. [49] | N/A | N/A | Y | N | Y | Y | N | Y | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Sire, A.; Moggio, L.; Marotta, N.; Agostini, F.; Tasselli, A.; Drago Ferrante, V.; Curci, C.; Calafiore, D.; Ferraro, F.; Bernetti, A.; et al. Impact of Rehabilitation on Fatigue in Post-COVID-19 Patients: A Systematic Review and Meta-Analysis. Appl. Sci. 2022, 12, 8593. https://0-doi-org.brum.beds.ac.uk/10.3390/app12178593
de Sire A, Moggio L, Marotta N, Agostini F, Tasselli A, Drago Ferrante V, Curci C, Calafiore D, Ferraro F, Bernetti A, et al. Impact of Rehabilitation on Fatigue in Post-COVID-19 Patients: A Systematic Review and Meta-Analysis. Applied Sciences. 2022; 12(17):8593. https://0-doi-org.brum.beds.ac.uk/10.3390/app12178593
Chicago/Turabian Stylede Sire, Alessandro, Lucrezia Moggio, Nicola Marotta, Francesco Agostini, Anna Tasselli, Vera Drago Ferrante, Claudio Curci, Dario Calafiore, Francesco Ferraro, Andrea Bernetti, and et al. 2022. "Impact of Rehabilitation on Fatigue in Post-COVID-19 Patients: A Systematic Review and Meta-Analysis" Applied Sciences 12, no. 17: 8593. https://0-doi-org.brum.beds.ac.uk/10.3390/app12178593