
Combining Yoga Exercise with Rehabilitation Improves Balance and Depression in Patients with Chronic Stroke: A Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethic Statement
2.2. Inclusion and Exclusion Criteria
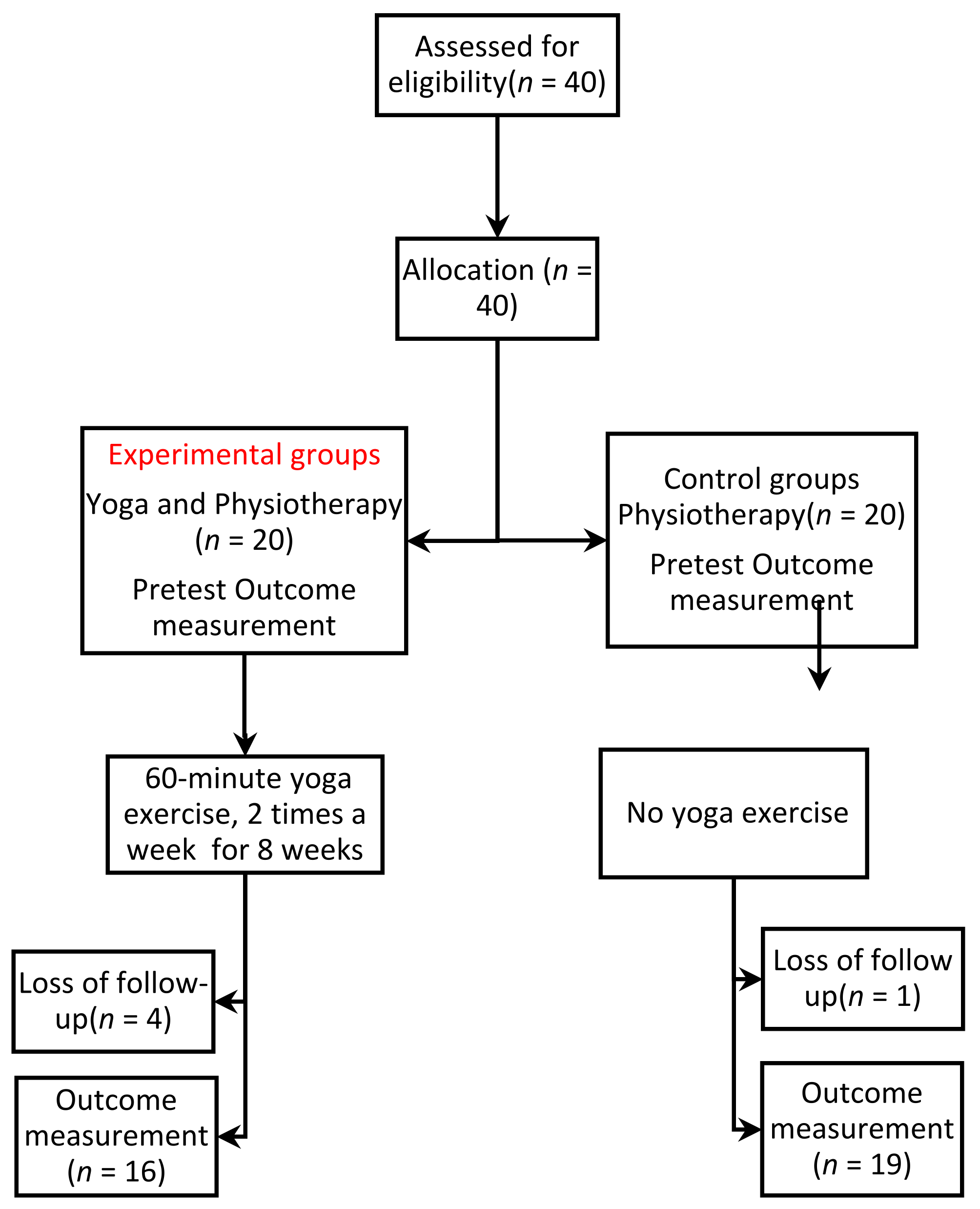
2.3. Protocol
2.4. Assessment of Outcome
2.5. Statistical Analysis
3. Results
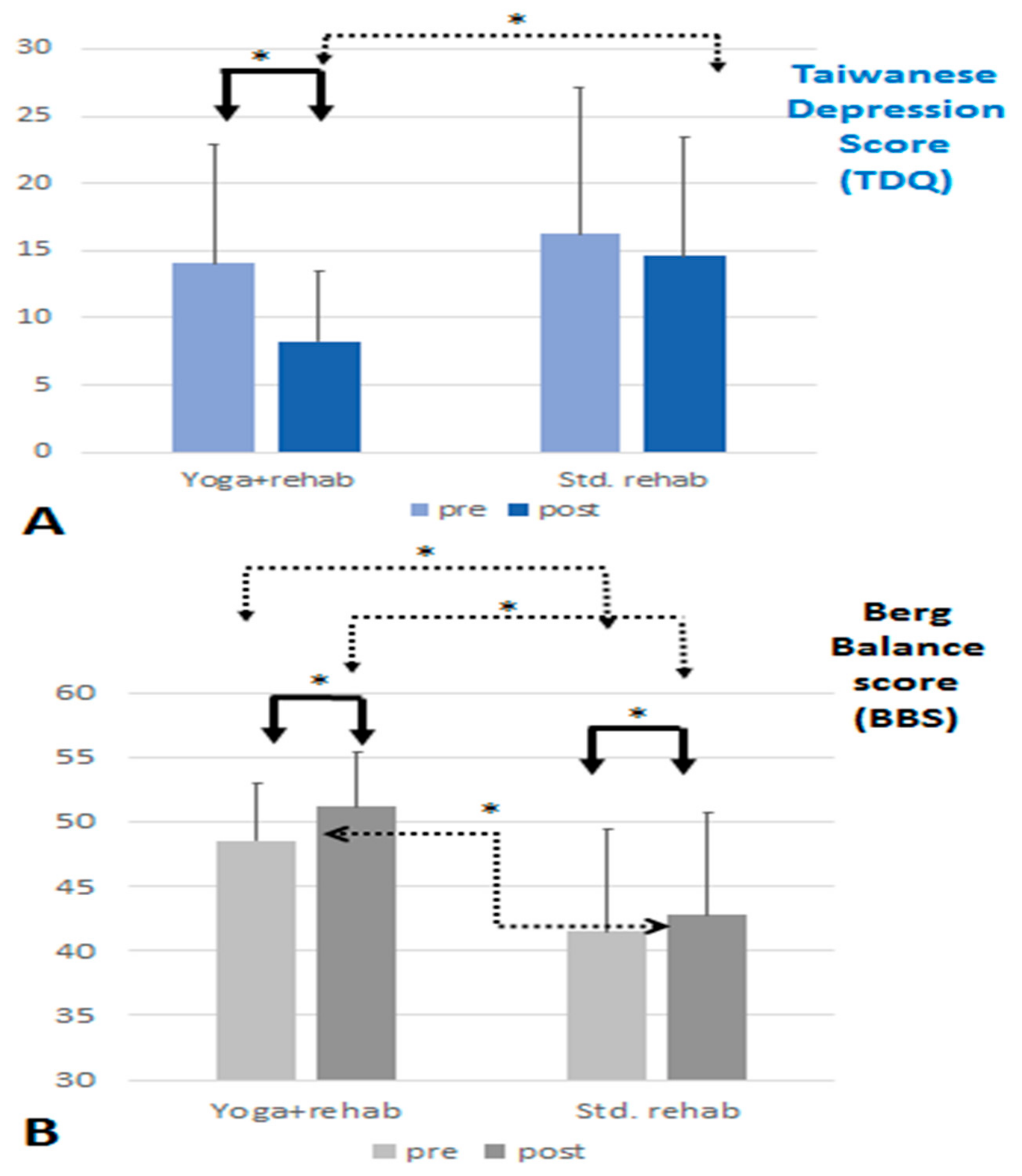
3.1. Primary Analysis of the Effect for Adding Yoga
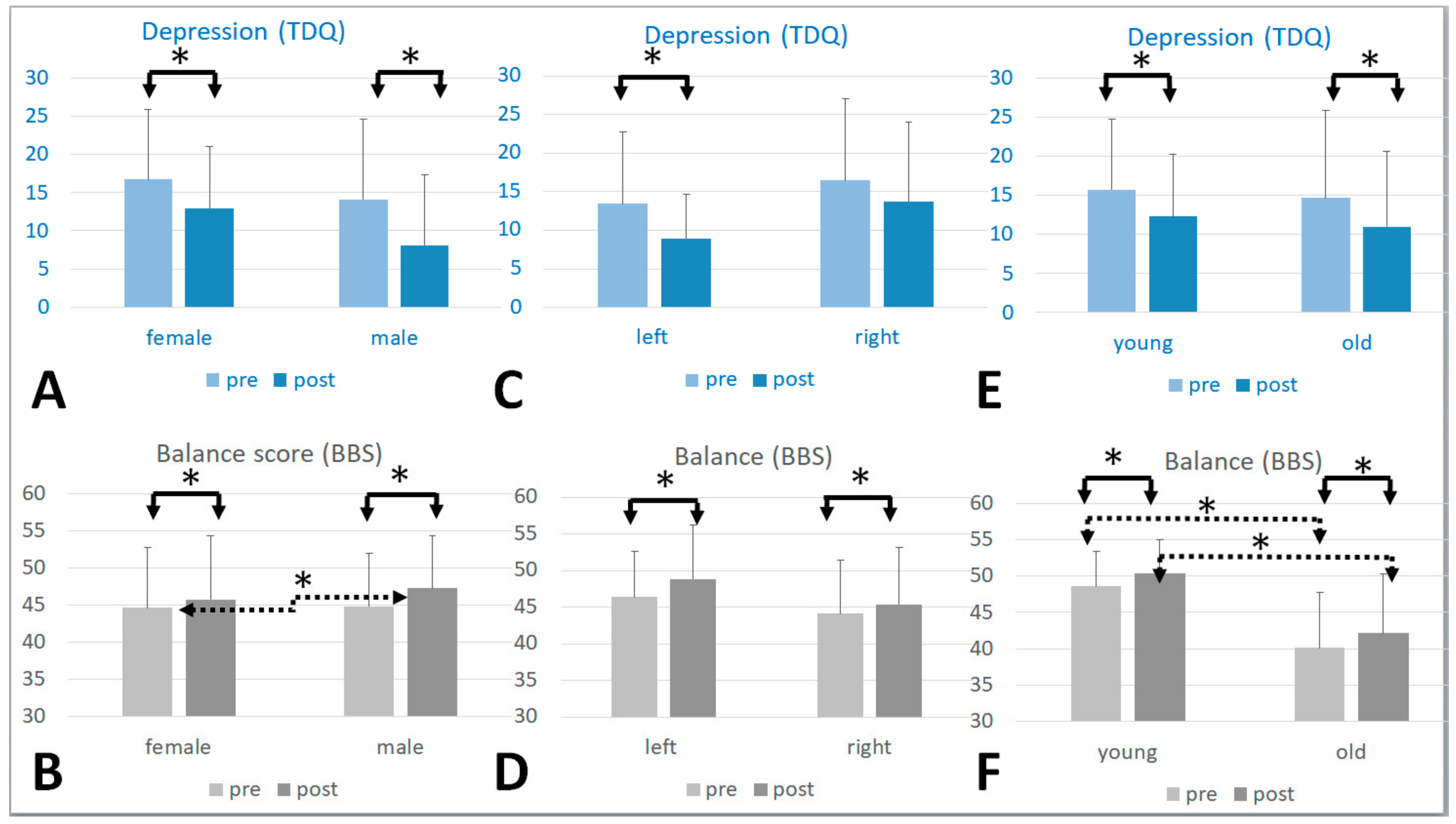
3.2. Subgroup Analysis
3.2.1. Gender
3.2.2. Brain Lesion Side
3.2.3. Age
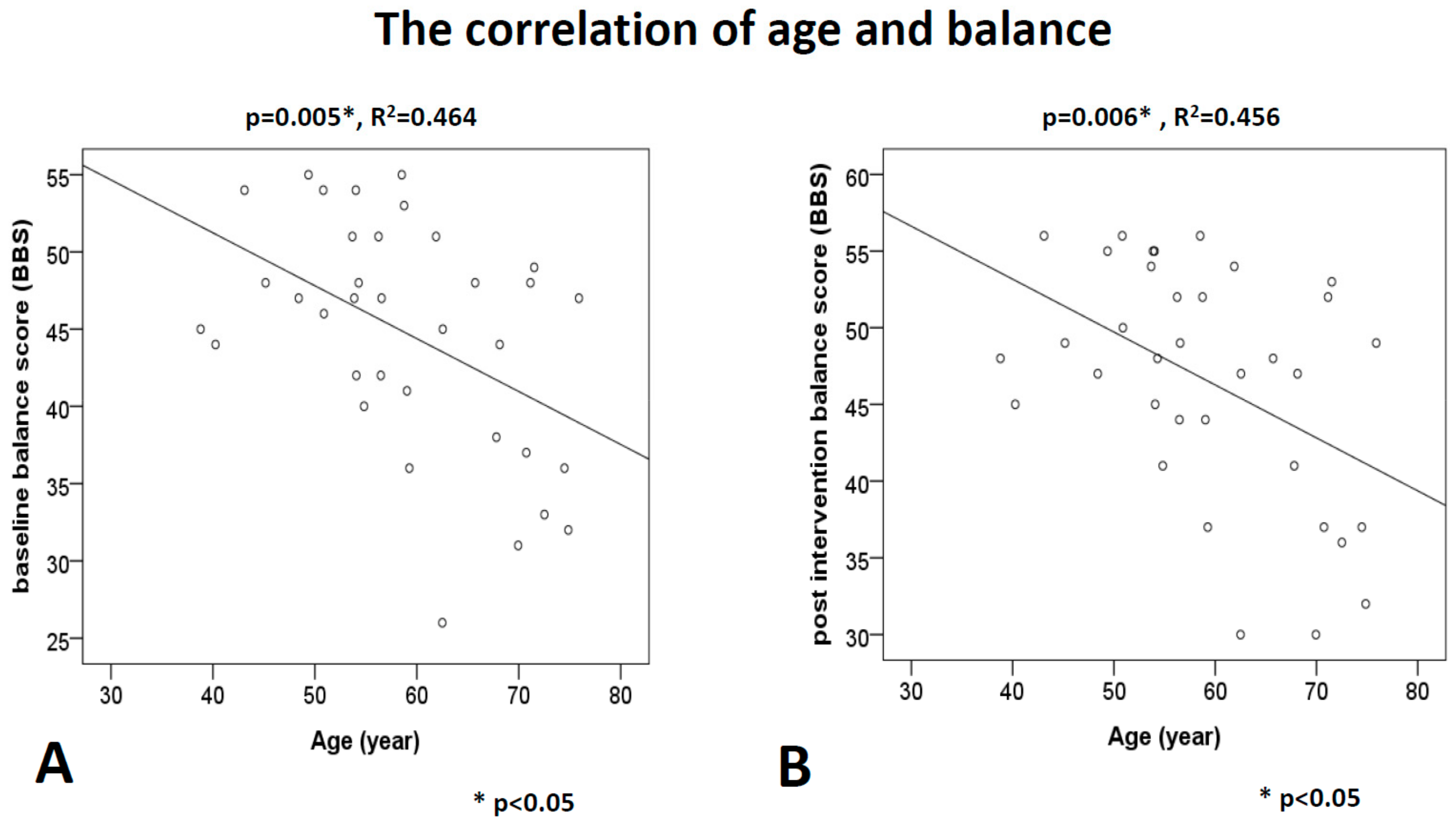
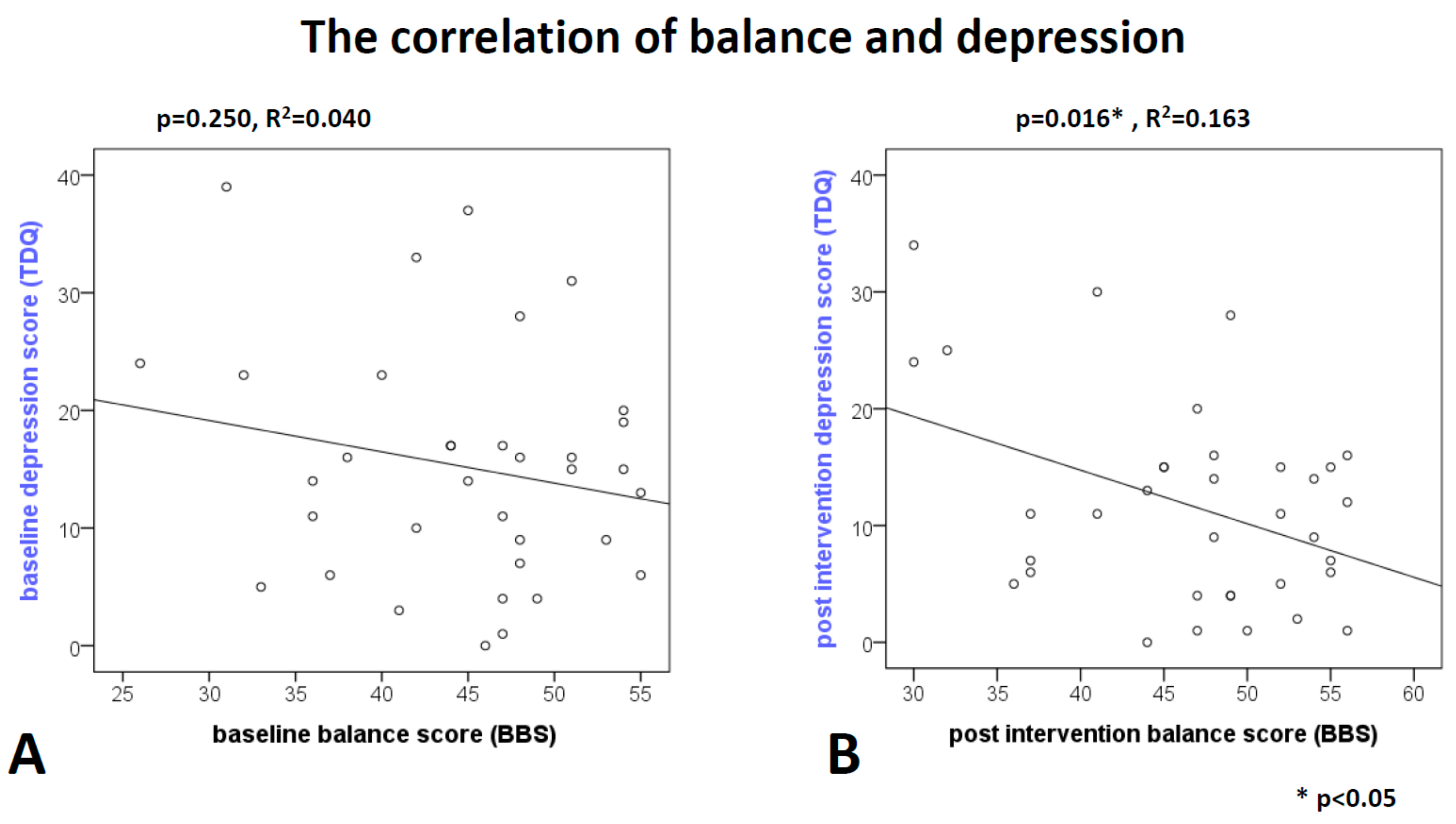
3.3. Factors Correlated with Balance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics—2017. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Pahlman, U.; Gutierrez-Perez, C.; Savborg, M.; Knopp, E.; Tarkowski, E. Cognitive function and improvement of balance after stroke in elderly people: The Gothenburg cognitive stroke study in the elderly. Disabil. Rehabil. 2011, 33, 1952–1962. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.G.; Jorge, R.E. Post-Stroke Depression: A Review. Am. J. Psychiatry 2016, 173, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.; Tallis, R.C. Balance disability after stroke. Phys. Ther. 2006, 86, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Hackett, M.L.; Pickles, K. Part I: Frequency of depression after stroke: An updated systematic review and meta-analysis of observational studies. Int. J. Stroke 2014, 9, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, L.P.; Kao, H.J. Depressive symptoms following ischemic stroke: A study of 207 patients. Acta Neurol. Taiwan. 2005, 14, 187–190. [Google Scholar]
- Simpson, L.A.; Miller, W.C.; Eng, J.J. Effect of stroke on fall rate, location and predictors: A prospective comparison of older adults with and without stroke. PLoS ONE 2011, 6, e19431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, S.N. How to increase serotonin in the human brain without drugs. J. Psychiatry Neurosci. 2007, 32, 394–399. [Google Scholar]
- Carek, P.J.; Laibstain, S.E.; Carek, S.M. Exercise for the treatment of depression and anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [Google Scholar] [CrossRef]
- Troeung, L.; Egan, S.J.; Gasson, N. A waitlist-controlled trial of group cognitive behavioural therapy for depression and anxiety in Parkinson’s disease. BMC Psychiatry 2014, 14, 19. [Google Scholar] [CrossRef] [Green Version]
- Aidar, F.J.; Jacó de Oliveira, R.; Gama de Matos, D.; Chilibeck, P.D.; de Souza, R.F.; Carneiro, A.L.; Machado Reis, V. A randomized trial of the effects of an aquatic exercise program on depression, anxiety levels, and functional capacity of people who suffered an ischemic stroke. J. Sports Med. Phys. Fitness 2018, 58, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Franklin, R.A.; Butler, M.P.; Bentley, J.A. The physical postures of yoga practices may protect against depressive symptoms, even as life stressors increase: A moderation analysis. Psychol. Health Med. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ebnezar, J.; Nagarathna, R.; Yogitha, B.; Nagendra, H.R. Effects of an integrated approach of hatha yoga therapy on functional disability, pain, and flexibility in osteoarthritis of the knee joint: A randomized controlled study. J. Altern. Complementary Med. 2012, 18, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Bastille, J.V.; Gill-Body, K.M. A yoga-based exercise program for people with chronic poststroke hemiparesis. Phys. Ther. 2004, 84, 33–48. [Google Scholar] [CrossRef]
- Schmid, A.A.; Van Puymbroeck, M.; Altenburger, P.A.; Schalk, N.L.; Dierks, T.A.; Miller, K.K.; Damush, T.M.; Bravata, D.M.; Williams, L.S. Poststroke balance improves with yoga: A pilot study. Stroke 2012, 43, 2402–2407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Immink, M.A.; Hillier, S.; Petkov, J. Randomized controlled trial of yoga for chronic poststroke hemiparesis: Motor function, mental health, and quality of life outcomes. Top. Stroke Rehabil. 2014, 21, 256–271. [Google Scholar] [CrossRef]
- Hartley, L.; Dyakova, M.; Holmes, J.; Clarke, A.; Lee, M.S.; Ernst, E.; Rees, K. Yoga for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2014, Cd010072. [Google Scholar] [CrossRef] [Green Version]
- Anne, E.; Cox, S.U.-F.; Amy, N.; D’Hondt-Taylor, M. The role of state mindfulness during yoga in predicting self-objectification and reasons for exercise. Psychol. Sport Exerc. 2016, 22, 321–327. [Google Scholar] [CrossRef]
- Tsai, H.-G.; Chang, T.-C.; Chen, H.-Y.; Chen, Y.-C.; Liu, C.-Y. The Application of YOGA Activity in Psychiatric Occupational Therapy. J. Taiwan Occup. Therapy Res. Pract. 2008, 4, 69–77. [Google Scholar] [CrossRef]
- Maraka, S.; Jiang, Q.; Jafari-Khouzani, K.; Li, L.; Malik, S.; Hamidian, H.; Zhang, T.; Lu, M.; Soltanian-Zadeh, H.; Chopp, M.; et al. Degree of corticospinal tract damage correlates with motor function after stroke. Ann. Clin. Transl. Neurol. 2014, 1, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Vive-Larsen, J.; Stoier, M.; Olsen, T.S. Outcome and time course of recovery in stroke. Part II: Time course of recovery. The Copenhagen Stroke Study. Arch. Phys. Med. Rehabil. 1995, 76, 406–412. [Google Scholar] [CrossRef]
- Der-Sheng, H.; Chia-Wei, L.; Lu, L.; Ming-Yen, H.; Chueh-Hung, W.; Huey-Wen, L.; Ke-Vin, C.; Shin-Liang, P.; Tyng-Guey, W.; Chein-Wei, C. Taiwan Guideline for Stroke Rehabilitation. Taiwan J. Phys. Med. Rehabil. 2016, 44, 1–9. [Google Scholar] [CrossRef]
- Lee, Y.; Yang, M.J.; Lai, T.J.; Chiu, N.M.; Chau, T.T. Development of the Taiwanese Depression Questionnaire. Change Gung Med. J. 2000, 23, 688–694. [Google Scholar]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I. The Balance Scale: Reliability assessment with elderly residents and patients with an acute stroke. Scand. J. Rehabil. Med. 1995, 27, 27–36. [Google Scholar] [PubMed]
- Huang, Y.C.; Hsu, S.T.; Hung, C.F.; Wang, L.J.; Chong, M.Y. Mental health of caregivers of individuals with disabilities: Relation to Suicidal Ideation. Compr. Psychiatry 2018, 81, 22–27. [Google Scholar] [CrossRef]
- Su, S.F.; Chang, M.Y.; He, C.P. Social Support, Unstable Angina, and Stroke as Predictors of Depression in Patients With Coronary Heart Disease. J. Cardiovasc. Nurs. 2018, 33, 179–186. [Google Scholar] [CrossRef]
- Lee, Y.; Wu, Y.-S.; Chien, C.-Y.; Fang, F.-M.; Hung, C.-F. Use of the Hospital Anxiety and Depression Scale and the Taiwanese Depression Questionnaire for screening depression in head and neck cancer patients in Taiwan. Neuropsychiatr. Dis. Treat. 2016, 12, 2649–2657. [Google Scholar] [CrossRef] [Green Version]
- Langley, F.A.; Mackintosh, S.F.H. Functional balance assessment of older community dwelling adults: A systematic review of the literature. Int. J. All. Health Sci. Pract. 2007, 5, 1–11. [Google Scholar] [CrossRef]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health 1992, 83 (Suppl. S2), S7–S11. [Google Scholar]
- Maeda, N.; Kato, J.; Shimada, T. Predicting the probability for fall incidence in stroke patients using the Berg Balance Scale. J. Int. Med. Res. 2009, 37, 697–704. [Google Scholar] [CrossRef]
- Froom, P.; Melamed, S.; Kristal-Boneh, E.; Benbassat, J.; Ribak, J. Healthy volunteer effect in industrial workers. J. Clin. Epidemiol. 1999, 52, 731–735. [Google Scholar] [CrossRef]
- Hansen, M.; Kjaer, M. Sex Hormones and Tendon. Adv. Exp. Med. Biol. 2016, 920, 139–149. [Google Scholar] [CrossRef]
- Bucht, H.; Donath, L. Sauna Yoga Superiorly Improves Flexibility, Strength, and Balance: A Two-Armed Randomized Controlled Trial in Healthy Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 3721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overmoyer, G.V.; Reiser, R.F., 2nd. Relationships between lower-extremity flexibility, asymmetries, and the Y balance test. J. Strength Cond. Res. 2015, 29, 1240–1247. [Google Scholar] [CrossRef]
- Ashaie, S.A.; Hurwitz, R.; Cherney, L.R. Depression and Subthreshold Depression in Stroke-Related Aphasia. Arch. Phys. Med. Rehabil. 2019, 100, 1294–1299. [Google Scholar] [CrossRef]
- Lynton, H.; Kligler, B.; Shiflett, S. Yoga in stroke rehabilitation: A systematic review and results of a pilot study. Top. Stroke Rehabil. 2007, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolahunase, M.R.; Sagar, R.; Faiq, M.; Dada, R. Yoga- and meditation-based lifestyle intervention increases neuroplasticity and reduces severity of major depressive disorder: A randomized controlled trial. Restor. Neurol. Neurosci. 2018, 36, 423–442. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 35) | With Yoga (n = 16) | Without Yoga (n = 19) | p | |
|---|---|---|---|---|
| Study completion rate, −/+ | 35/40 | 16/20 | 19/20 | 0.151 |
| Categorical variables, Chi-square test | ||||
| Sex, female:male | 15:20 | 6:10 | 9:10 | 0.734 |
| Stroke side, left:right † | 17:17 | 11:5 | 6:12 | 0.084 |
| Age < 60:age ≥ 60, years | 19:16 | 11:5 | 8:11 | 0.176 |
| Continuous variables, t-test | ||||
| Age | 59.0± 10.10 | 56.8 ± 9.11 | 60.9 ± 10.743 | 0.241 |
| T onset (days) | 691.9± 20.17 | 560.6 ± 538.57 | 802.4 ± 1153.00 | 0.447 |
| Taiwanese Depression Questionnaire (TDQ) score | ||||
| Baseline TDQ | 15.23± 9.91 | 14.06 ± 8.85 | 16.21 ± 10.86 | 0.531 |
| Post intervention TDQ | 11.71 ± 8.66 | 8.25 ± 5.19 | 14.63 ± 9.99 | 0.028 * |
| The change of TDQ | −3.51 ± 5.84 | −5.81 ± 6.13 | −1.57 ± 4.94 | 0.806 |
| Paired t (p) | 0.001 * | 0.002 * | 0.181 | |
| Berg Balance Scale (BBS) score | ||||
| Baseline BBS | 44.71 ± 7.64 | 48.56 ± 4.42 | 41.47 ± 8.01 | <0.001 * |
| Post intervention BBS | 46.60 ± 7.46 | 51.13 ± 4.25 | 42.79 ± 7.85 | <0.001 * |
| The change of BBS | 1.87 ± 1.79 | 2.56 ± 1.96 | 1.31 ± 1.45 | 0.029 * |
| Paired t-test (p) | <0.001 * | <0.001 * | 0.001 * | |
| Subgroup Variable | Women n = 15 | Men n = 20 | p | Left n = 17 | Right n = 17 | p | Age < 60 n = 19 | Age ≥ 60 n = 16 | p |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 60.88 ± 12.42 | 57.64 ± 7.99 | 0.386 | 55.79 ± 7.81 | 62.06 ± 11.57 | 0.733 | 51.48 ± 5.91 | 68.00 ± 5.56 | <0.001 |
| T onset (days) | 426.67 ± 376.12 | 376.12 ± 1146.20 | 0.103 | 1002.76 ± 1212.40 | 404.65 ± 358.96 | 0.60 | 734.00 ± 951.33 | 641.81 ± 910.08 | 0.773 |
| Taiwanese Depression Questionnaire (TDQ) score | |||||||||
| D0 | 16.73 ± 9.18 | 14.10 ± 10.51 | 0.445 | 13.47 ± 9.28 | 16.47 ± 10.61 | 0.387 | 15.74 ± 8.93 | 14.63 ± 11.23 | 0.746 |
| D1 | 12.93± 8.10 | 8.10 ± 9.16 | 0.479 | 8.94 ± 5.68 | 13.76 ± 10.26 | 0.102 | 12.32 ± 7.97 | 11.00 ± 9.64 | 0.661 |
| Delta D | −3.80 ± 5.62 | −3.30 ± 6.13 | 0.806 | −4.52 ± 5.95 | −2.70 ± 5.87 | 0.376 | −3.42 ± 6.41 | −3.62 ± 5.28 | 0.920 |
| Paired t (p) | 0.020 * | 0.027 * | 0.006 * | 0.076 | 0.032 * | 0.015 * | |||
| Berg Balance Scale (BBS) score (BBS) score | |||||||||
| B0 | 44.60 ± 8.16 | 44.80 ± 7.08 | 0.939 | 46.41 ± 6.21 | 44.12 ± 7.34 | 0.333 | 48.58 ± 4.77 | 40.13 ± 7.55 | 0.001 * |
| B1 | 45.73 ± 8.53 | 47.25 ± 7.05 | 0.569 | 48.82 ± 6.24 | 45.35 ± 7.80 | 0.162 | 50.37 ± 4.65 | 42.13 ± 8.18 | 0.002 * |
| Delta B | 1.13 ± 1.45 | 2.45 ± 1.84 | 0.029 * | 2.41 ± 1.90 | 1.23 ± 1.48 | 0.053 | 1.78 ± 1.96 | 2.00 ± 1.63 | 0.735 |
| Paired t (p) | 0.009 * | <0.001 * | <0.001 * | 0.003 * | 0.001 * | <0.001 * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-T.; Lin, C.-H.; Hsieh, C.C.; Yang, J.-C.; Tsou, H.-H.; Lin, C.-C.; Li, S.-Y.; Chan, H.-L.; Liu, W.-S. Combining Yoga Exercise with Rehabilitation Improves Balance and Depression in Patients with Chronic Stroke: A Controlled Trial. Appl. Sci. 2022, 12, 922. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020922
Lai Y-T, Lin C-H, Hsieh CC, Yang J-C, Tsou H-H, Lin C-C, Li S-Y, Chan H-L, Liu W-S. Combining Yoga Exercise with Rehabilitation Improves Balance and Depression in Patients with Chronic Stroke: A Controlled Trial. Applied Sciences. 2022; 12(2):922. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020922
Chicago/Turabian StyleLai, Yen-Ting, Chien-Hung Lin, City C. Hsieh, Jung-Cheng Yang, Han-Hsing Tsou, Chih-Ching Lin, Szu-Yuan Li, Hsiang-Lin Chan, and Wen-Sheng Liu. 2022. "Combining Yoga Exercise with Rehabilitation Improves Balance and Depression in Patients with Chronic Stroke: A Controlled Trial" Applied Sciences 12, no. 2: 922. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020922