
Heart Failure Patients’ Adherence to Hybrid Comprehensive Telerehabilitation and Its Impact on Prognosis Based on Data from TELEREH-HF Randomized Clinical Trial


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cardiopulmonary Exercise Test
2.2. Assessment of Physical Capacity Improvement
2.3. Assessment of the Adherence to Hybrid Comprehensive Telerehabilitation
2.4. Statistical Analyses
3. Results
3.1. Functional Outcomes after 9 Weeks
3.1.1. NYHA Class
3.1.2. Functional Capacity
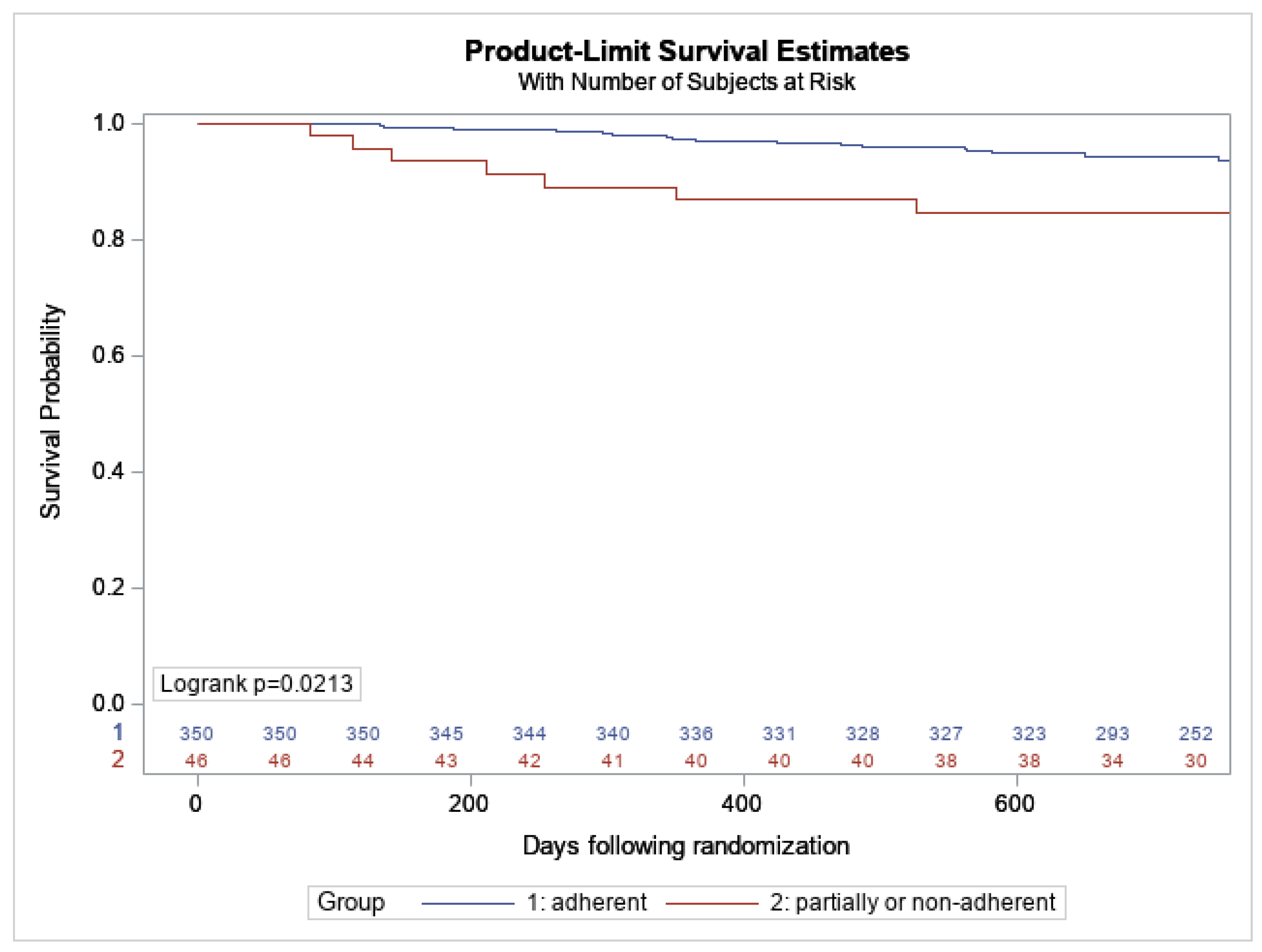
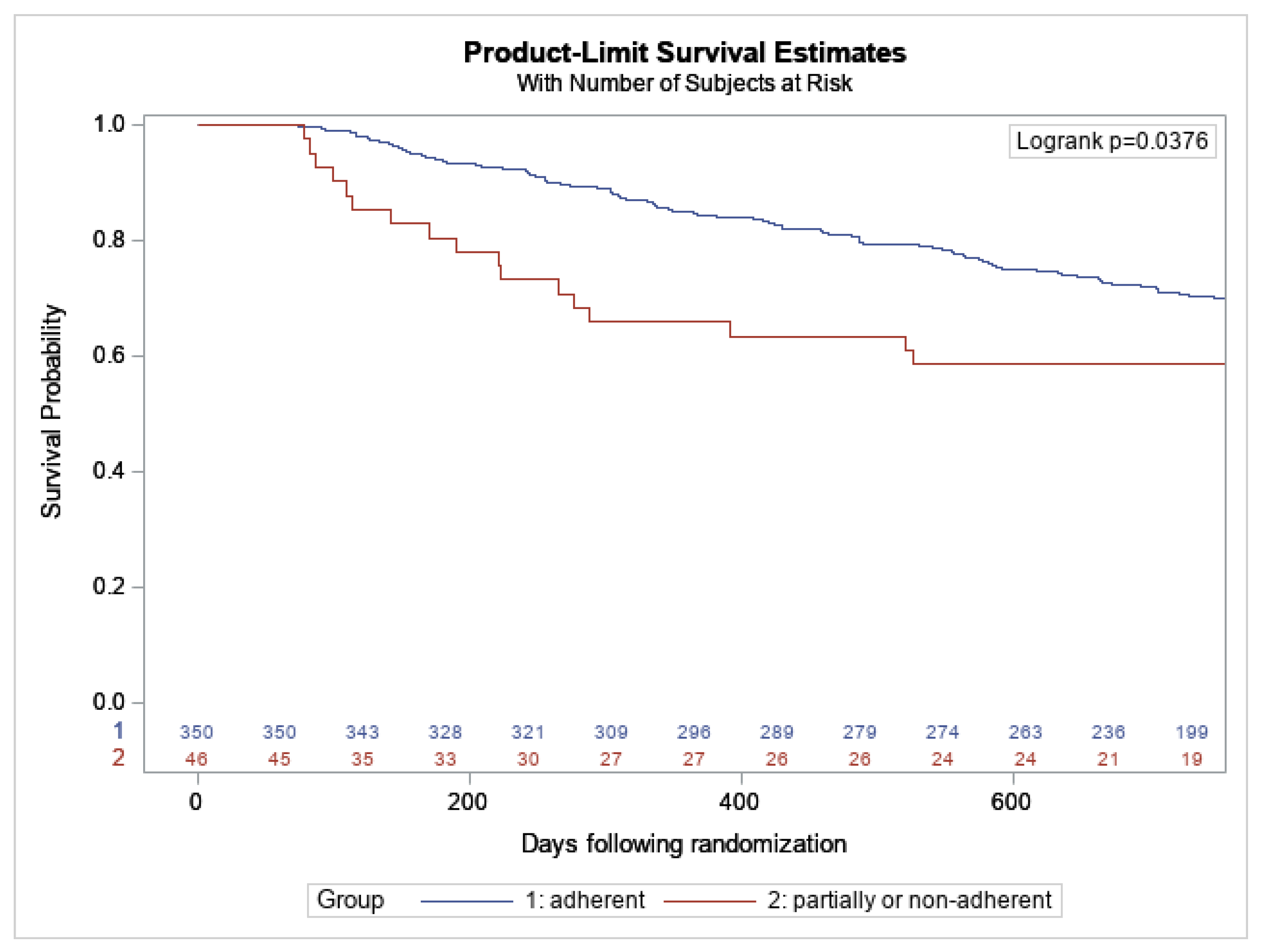
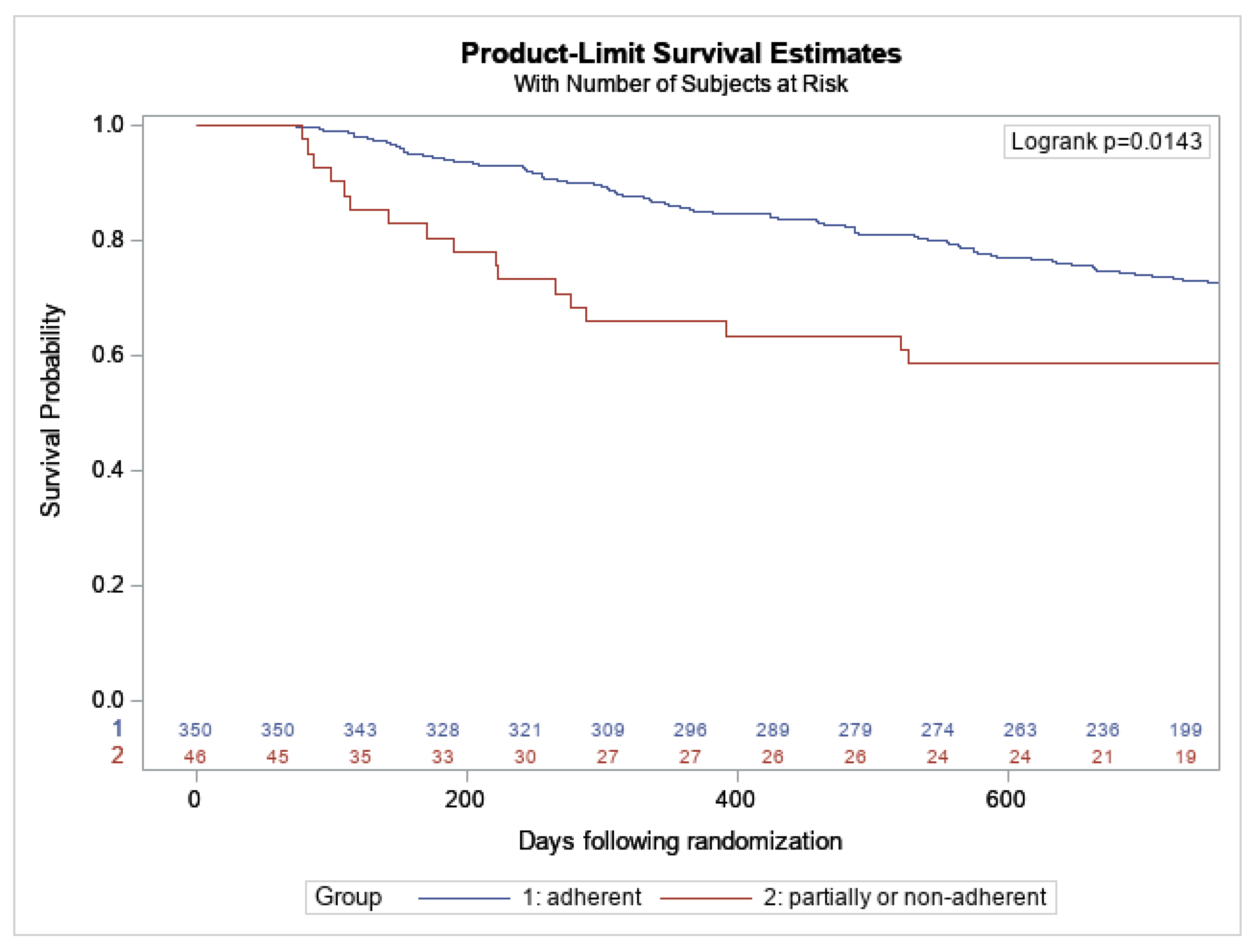
3.2. Impact of Patients’ Adherence to HCTR on Long-Term Prognosis during 14–26 Months after the Intervention Was Completed
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conraads, V.M.; Deaton, C.; Piotrowicz, E.; Santaularia, N.; Tierney, S.; Piepoli, M.F.; Pieske, B.; Schmid, J.P.; Dickstein, K.; Ponikowski, P.P.; et al. Adherence of heart failure patients to exercise: Barriers and possible solutions: A position statement of the Study Group on Exercise Training in Heart Failure of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2012, 14, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Deka, P.; Pozehl, B.; Williams, M.A.; Yates, B. Adherence to recommended exercise guidelines in patients with heart failure. Hear. Fail. Rev. 2016, 22, 41–53. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Seferovic, P.M.; Ponikowski, P.; Anker, S.D.; Bauersachs, J.; Chioncel, O.; Cleland, J.G.; De Boer, R.A.; Drexel, H.; Ben Gal, T.; Hill, L.; et al. Clinical practice update on heart failure 2019: Pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the Heart Failure Association of the European Society of Cardiology. Eur. J. Hear. Fail. 2019, 21, 1169–1186. [Google Scholar] [CrossRef]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation. A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation the American Heart Association, and the American College of Cardiology. J. Am. Coll. Cardiol. 2019, 74, 133–153. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Fonarow, G.C.; Goldberg, L.R.; Guglin, M.; Josephson, R.A.; Forman, D.E.; Lin, G.; Lindenfeld, J.; O’Connor, C.; Panjrath, G.; et al. Cardiac Rehabilitation for Patients With Heart Failure. JACC Expert Panel Perspective From the ACC Heart Failure and Transplant Section and Leadership Council, Reviewed by the Prevention Section Cardiac Rehabilitation Work Group. J. Am. Coll. Cardiol. 2021, 77, 1454–1469. [Google Scholar] [CrossRef] [PubMed]
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.; Schmid, J.P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper fromthe Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Winnige, P.; Filakova, K.; Hnatiak, J.; Dosbaba, F.; Bocek, O.; Pepera, G.; Papathanasiou, J.; Batalik, L.; Grace, S.L. Validity and Reliability of the Cardiac Rehabilitation Barriers Scale in the Czech Republic (CRBS-CZE): Determination of Key Barriers in East-Central Europe. Int. J. Environ. Res. Public Health 2021, 18, 13113. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Piepoli, M.F.; Jaarsma, T.; Lambrinou, E.; Coats, A.J.; Schmid, J.-P.; Corrà, U.; Agostoni, P.; Dickstein, K.; Seferović, P.M.; et al. Telerehabilitation in heart failure patients: The evidence and the pitfalls. Int. J. Cardiol. 2016, 220, 408–413. [Google Scholar] [CrossRef] [Green Version]
- Varma, N.; Cygankiewicz, I.; Turakhia, M.; Heidbuchel, H.; Hu, Y.; Chen, L.Y.; Couderc, J.; Cronin, E.M.; Estep, J.D.; Grieten, L.; et al. 2021 ISHNE/ HRS/ EHRA/ APHRS collaborative statement on mHealth in Arrhythmia Management: Digital Medical Tools for Heart Rhythm Professionals. Ann. Noninvasive Electrocardiol. 2021, 26, e12795. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, R.; Krzesiński, P.; Balsam, P.; Piotrowicz, E.; Kempa, M.; Lewicka, E.; Główczyńska, R.; Grabowski, M.; Kołtowski, Ł.; Peller, M.; et al. Telemedicine solutions in cardiology: A joint expert opinion by the Information Technology and Telemedicine Committee of the Polish Cardiac Society, the Section of Noninvasive Electrocardiology and Telemedicine of the Polish Cardiac Society, and the Clinical Research Committee of the Polish Academy of Sciences (short version, 2021). Kardiol. Pol. 2021, 79, 227–241. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Baranowski, R.; Bilinska, M.; Stepnowska, M.; Piotrowska, M.; Wójcik, A.; Korewicki, J.; Chojnowska, L.; Małek, Ł.A.; Klopotowski, M.; et al. A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: Effectiveness, quality of life, and adherence. Eur. J. Hear. Fail. 2010, 12, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Zieliński, T.; Bodalski, R.; Rywik, T.; Dobraszkiewicz-Wasilewska, B.; Sobieszczańska-Małek, M.; Stepnowska, M.; Przybylski, A.; Browarek, A.; Szumowski, Ł.; et al. Home-based telemonitored Nordic walking training is well accepted, safe, effective and has high adherence among heart failure patients, including those with cardiovascular implantable electronic devices—A randomized controlled study. Eur. J. Prev. Cardiol. 2015, 22, 1368–1377. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Conraads, V.; Corrà, U.; Dickstein, K.; Francis, D.P.; Jaarsma, T.; Mcmurray, J.; Pieske, B.; Piotrowicz, E.; Schmid, J.-P.; et al. Exercise training in heart failure: From theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur. J. Hear. Fail. 2011, 13, 347–357. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Piotrowicz, R.; Opolski, G.; Pencina, M.; Banach, M.; Zaręba, W. Hybrid comprehensive telerehabilitation in heart failure patients (TELEREH-HF): A randomized, multicenter, prospective, open-label, parallel group controlled trial—Study design and description of the intervention. Am. Hear. J. 2019, 217, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Pencina, M.J.; Opolski, G.; Zaręba, W.; Banach, M.; Kowalik, I.; Orzechowski, P.; Szalewska, D.; Pluta, S.; Główczyńska, R.; et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients With Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 300–308. [Google Scholar] [CrossRef]
- Batalik, L.; Pepera, G.; Papathanasiou, J.; Rutkowski, S.; Líška, D.; Batalikova, K.; Hartman, M.; Felšőci, M.; Dosbaba, F. Is the Training Intensity in Phase Two Cardiovascular Rehabilitation Different in Telehealth versus Outpatient Rehabilitation? J. Clin. Med. 2021, 10, 4069. [Google Scholar] [CrossRef] [PubMed]
- Balady, G.J. Medical evaluation and exercise testing. In Guidelines for Cardiac Rehabilitation and Secondary Prevention Programs, 4th ed.; Williams, M.A., Ed.; Human Kinetics: Champaign, IL, USA, 2004; p. 79. [Google Scholar]
- Piepoli, M.F.; Corrà, U.; Agostoni, P.G.; Belardinelli, R.; Cohen-Solal, A.; Hambrecht, R.; Vanhees, L. Task Force of the Italian Working Group on Cardiac Rehabilitation and Prevention (Gruppo Italiano di Cardiologia Riabilitativa e Prevenzione, GICR); Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology. Statement on cardiopulmonary exercise testing in chronic heart failure due to left ventricular dysfunction: Recommendations for performance and interpretation Part II: How to perform cardiopulmonary exercise testing in chronic heart failure. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 300–311. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Mierzyńska, A.; Banach, M.; Jaworska, I.; Pencina, M.; Kowalik, I.; Pluta, S.; Szalewska, D.; Opolski, G.; Zaręba, W.; et al. Quality of life in heart failure patients undergoing hybrid comprehensive telerehabilitation versus usual care—Results of the Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. Arch. Med Sci. 2020, 17, 1599–1612. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Adherence to Long-Term Therapies: Evidence for Action; Sabete, E., Ed.; World Health Organization: Geneva, Switzerland, 2003; Available online: http://www.who.int/chp/knowledge/publications/ adherence_introduction.pdf (accessed on 4 August 2017).
- Smart, N.; Haluska, B.; Jeffriess, L.; Marwick, T.H. Predictors of sustained response to exercise training in patients with chronić heart failure: A telemonitoring study. Am. Heart J. 2005, 150, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Hwang, R.; Bruning, J.; Morris, N.R.; Mandrusiak, A.; Russell, T. Home-based telerehabilitation is not inferior to a centre-based program in patients with chronic heart failure: A randomised trial. J. Physiother. 2017, 63, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frederix, I.; Hansen, D.; Coninx, K.; Vandervoort, P.; Vandijck, D.; Hens, N.; Van Craenenbroeck, E.; Van Driessche, N.; Dendale, P. Effect of comprehensive cardiac telerehabilitation on one-year cardiovascular rehospitalization rate, medical costs and quality of life: A cost-effectiveness analysis. Eur. J. Prev. Cardiol. 2016, 23, 674–682. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Whellan, D.J.; Lee, K.L.; Keteyian, S.J.; Cooper, L.S.; Ellis, S.J.; Leifer, E.S.; Kraus, W.E.; Kitzman, D.W.; Blumenthal, J.A.; et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009, 301, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.B.; Mentz, R.J.; Sun, J.L.; Schulte, P.J.; Fleg, J.L.; Cooper, L.S.; Piña, I.L.; Leifer, E.S.; Kraus, W.E.; Whellan, D.J.; et al. Psychosocial Factors, Exercise Adherence, and Outcomes in Heart Failure Patients Insights From Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION). Circ. Heart Fail. 2015, 8, 1044–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whellan, D.J. Long-Term Exercise Training and Adherence It Is Not Just Exercise. J. Am. Coll. Cardiol. 2012, 60, 1529–1530. [Google Scholar] [CrossRef]
- Niewada, M.; Tabor, B.; Piotrowicz, E.; Piotrowicz, R.; Opolski, G.; Banach, M.; Jakubczyk, M. Cost-effectiveness of telerehabilitation in patients with heart failure in Poland: An analysis based on the results of Telerehabilitation in the Heart Failure Patients (TELEREH-HF) randomized clinical trial. Kardiol Pol. 2021, 79, 510–516. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Hybrid Comprehensive Telerehabilitation Group (n = 396) | Adherent Patients Group (n = 350) | Partially Adherent and Non-Adherent Patients Group (n = 46) | p | |
|---|---|---|---|---|
| Males, n (%) | 354 (89.4) | 313 (89.4%) | 41 (89.1%) | 1.00 |
| Age (years), mean ± SD | 62.2 ± 10.7 | 62.3 ± 10.4 | 61.2 ± 13.1 | 0.594 |
| Left ventricular ejection fraction (%), mean ± SD | 30.8 ± 6.9 | 31.0 ± 6.8 | 29.7 ± 7.1 | 0.222 |
| Atrial fibrillation or atrial flutter, n (%) | 75 (18.9) | 61 (17.4) | 14 (30.4) | 0.034 |
| Body mass index (kg/m2), mean ± SD | 28.9 ± 5.1 | 28.7 ± 5.0 | 29.9 ± 5.9 | 0.136 |
| Etiology of heart failure, n (%) | ||||
| Ischemic | 258 (65.1) | 234 (66.7) | 24 (52.2) | 0.049 |
| Non-ischemic | 138 (34.9) | 116 (33.1) | 22 (47.8) | |
| Past medical history, n (%) | ||||
| Myocardial infarction | 231 (58.3) | 208 (59.4) | 23 (50.0) | 0.223 |
| Angioplasty | 187 (47.2) | 171 (48.9) | 16 (37.8) | 0.072 |
| Coronary artery bypass grafting | 59 (14.9) | 52 (14.9) | 7 (15.2) | 0.949 |
| Valve surgery | 32 (8.1) | 28 (8.0) | 4 (8.7) | 0.777 |
| Hypertension | 234 (59.1) | 209 (59.7) | 25 (54.3) | 0.486 |
| Stroke | 22 (5.6) | 19 (5.4) | 3 (6.5) | 0.731 |
| Diabetes | 133 (33.6) | 121 (34.6) | 12 (26.1) | 0.252 |
| Chronic kidney disease | 73 (18.4) | 61 (17.4) | 12 (26.1) | 0.154 |
| Depression BDI-II > 13 | 84/389 (21.6) | 71 (20.7) | 13 (28.3) | 0.242 |
| SF-36 overall (score) mean ± SD | 90.1 ± 12.4 | 90.3 ± 12.4 | 87.7 ± 11.3 | 0.178 |
| Functional status, n (%) | ||||
| NYHA I | 52 (13.1) | 45 (12.9) | 7 (15.2) | 0.318 |
| NYHA II | 277 (69.9) | 249 (71.1) | 28 (60.9) | |
| NYHA III | 67 (16.9) | 56 (16.0) | 11 (23.9) | |
| Parameters | ||||
| NT-proBNP Medians [Q1–Q3] | 867.5 [362.0–1997.0] | 859.5 [356–1935] | 1139.5 [373.0–3030] | 0.185 |
| Peak oxygen consumption pVO2 (mL/kg/min) mean SD | 17.0 ± 5.6 | 17.2 ± 5.6 | 15.5 ± 5.5 | 0.066 |
| Treatment, n (%) | ||||
| Beta-blocker | 380 (96.0) | 335 (95.7) | 45 (97.8) | 0.706 |
| ACEI/ARB | 369 (93.2) | 329 (94.0) | 40 (87.0) | 0.110 |
| Digoxin | 51 (12.9) | 44 (12.6) | 7 (15.2) | 0.614 |
| Loop diuretics | 292 (73.7) | 257 (73.4) | 35 (76.1) | 0.700 |
| Spironolactone/eplerenone | 328 (82.8) | 290 (82.9) | 38 (82.6) | 0.966 |
| Aspirin/clopidogrel | 222 (56.1) | 205 (58.6) | 17 (37.0) | 0.005 |
| Anticoagulants | 117 (29.5) | 104 (29.7) | 13 (28.3) | 0.839 |
| NOAC | 65 (16.4) | 52 (14.9) | 13 (28.3) | 0.021 |
| Statins | 321 (81.1) | 292 (83.4) | 29 (63.0) | <0.001 |
| CIEDs | 314 (79.3) | 275 (78.6) | 39 (84.8) | 0.328 |
| ICD | 193 (61.5) | 170 (61.8) | 23 (59.0) | 0.689 |
| Adherent Patient Group | Partially Adherent and Non-Adherent Patients Group | |||
|---|---|---|---|---|
| NYHA Class | Baseline | 9th Week | Baseline | 9th Week |
| I | 45 (12.9%) | 92 (26.3%) | 7 (15.2%) | 7 (15.2%) |
| II | 249 (71.1%) | 215 (61.4%) | 28 (60.9%) | 26 (56.5%) |
| III | 56 (16.0%) | 43 (12.3%) | 11 (23.9%) | 13 (28.3%) |
| Outcome | Adherent Patients Group N = 350 | Partially Adherent and Non-Adherent Patients Group N = 46 | Hazard Ratio 95% Wald CL Partially Adherent or Non-Adherent vs. Adherent | p-Value | Hazard Ratio * 95% Wald CL Partially Adherent or Non-Adherent vs. Adherent | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| N (%) | Event Rate at 26 Months | N (%) | Event Rate at 26 Months | |||||
| All-cause mortality | 38 (10.9) | 10.5 | 8 (17.4%) | 17.4 | 1.79 (0.83–3.85) | 0.135 | 1.56 (0.71–3.43) | 0.267 |
| Cardiovascular mortality | 23 (6.6%) | 6.3 | 7 (15.6%) | 15.2 | 2.62 (1.12–6.13) | 0.021 | 2.07 (0.85–5.03) | 0.108 |
| All-cause hospitalization | 201 (57.4) | 58.3 | 19 (41.3%) | 47.9 | 0.99 (0.62–1.58) | 0.963 | 0.94 (0.58–1.51) | 0.784 |
| Cardiovascular hospitalization | 126 (36.0) | 38.0 | 11 (23.9%) | 28.1 | 0.84 (0.45–1.55) | 0.570 | 0.81 (0.43–1.51) | 0.508 |
| Heart failure hospitalization | 86 (24.6) | 25.7 | 13 (28.3%) | 33.8 | 1.60 (0.89–2.86) | 0.116 | 1.65 (0.91–3.01) | 0.108 |
| All-cause mortality or all-cause hospitalization | 208 (59.4) | 59.7 | 23 (50.0%) | 55.3 | 1.16 (0.75–1.78) | 0.506 | 1.09 (0.71–1.69) | 0.694 |
| All-cause mortality or cardiovascular hospitalization | 151 (43.1) | 43.9 | 17 (37.0%) | 40.9 | 1.08 (0.65–1.78) | 0.761 | 1.03 (0.62–1.72) | 0.904 |
| All-cause mortality or heart failure hospitalization | 105 (30.0) | 30.6 | 17 (37.0%) | 41.2 | 1.71 (1.02–2.86) | 0.038 | 1.79 (1.06–3.04) | 0.030 |
| Cardiovascular mortality or heart failure hospitalization | 95 (27.1) | 28.1 | 17 (37.0%) | 41.2 | 1.89 (1.13–3.16) | 0.014 | 1.99 (1.17–3.39) | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piotrowicz, E.; Pencina, M.; Opolski, G.; Zaręba, W.; Banach, M.; Kowalik, I.; Orzechowski, P.; Główczyńska, R.; Szalewska, D.; Pluta, S.; et al. Heart Failure Patients’ Adherence to Hybrid Comprehensive Telerehabilitation and Its Impact on Prognosis Based on Data from TELEREH-HF Randomized Clinical Trial. Appl. Sci. 2022, 12, 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/app12052595
Piotrowicz E, Pencina M, Opolski G, Zaręba W, Banach M, Kowalik I, Orzechowski P, Główczyńska R, Szalewska D, Pluta S, et al. Heart Failure Patients’ Adherence to Hybrid Comprehensive Telerehabilitation and Its Impact on Prognosis Based on Data from TELEREH-HF Randomized Clinical Trial. Applied Sciences. 2022; 12(5):2595. https://0-doi-org.brum.beds.ac.uk/10.3390/app12052595
Chicago/Turabian StylePiotrowicz, Ewa, Michael Pencina, Grzegorz Opolski, Wojciech Zaręba, Maciej Banach, Ilona Kowalik, Piotr Orzechowski, Renata Główczyńska, Dominika Szalewska, Sławomir Pluta, and et al. 2022. "Heart Failure Patients’ Adherence to Hybrid Comprehensive Telerehabilitation and Its Impact on Prognosis Based on Data from TELEREH-HF Randomized Clinical Trial" Applied Sciences 12, no. 5: 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/app12052595