
Whole-Body Cryostimulation in Fibromyalgia: A Scoping Review
by
 , , and
, , and
Jacopo Maria Fontana
1,* ,
,
Michele Gobbi
1, 
Paolo Piterà
1,2,
Emanuele Maria Giusti
3 and
Paolo Capodaglio
1,4
1
Orthopedic Rehabilitation Unit and Research Lab in Biomechanics, Rehabilitation and Ergonomics, Ospedale San Giuseppe, Istituto Auxologico Italiano, IRCCS, Via Cadorna 90, 28824 Verbania, Italy
2
International Center for the Assessment of Nutritional Status (ICANS), Department of Food, Environmental and Nutritional Sciences (DeFENS), University of Milan, 20133 Milan, Italy
3
Department of Psychology, Catholic University of Milan, 20123 Milan, Italy
4
Department of Surgical Sciences, Physical and Rehabilitation Medicine, University of Turin, 10121 Turin, Italy
*
Author to whom correspondence should be addressed.
Appl. Sci. 2022, 12(9), 4794; https://0-doi-org.brum.beds.ac.uk/10.3390/app12094794
Submission received: 17 March 2022
/
Revised: 5 May 2022
/
Accepted: 7 May 2022
/
Published: 9 May 2022
(This article belongs to the Special Issue Role of Physiotherapy and Physical Agent Modalities for Musculoskeletal Disorders: Present and Future)
Abstract
:Currently, all available therapies for the control and management of fibromyalgia (FM) are mostly focused on relieving patients’ symptoms and improving their quality of life. The purpose of this review is to provide an up-to-date overview of the evidence supporting the beneficial effects of whole-body cryostimulation (WBC) in patients with FM and evidence-based guidance on the possible adjuvant use of WBC in the treatment of FM. We searched the most recent literature by retrieving 10 eligible studies, 4 of which were abstracts only, from a total of 263 records. Thermal stress caused by cryostimulation induces an analgesic effect, improving pain, redox balance, and inflammatory symptoms in an exercise-mimicking fashion. In addition, it reduces the feeling of fatigue, improves mood, and reduces mental health deterioration with positive consequences on depressive states and improved sleep quality. Although the studies included in this review are not of sufficient quality and quantity to draw definitive conclusions about the effectiveness of WBC in FM, initial evidence indicates WBC as a promising add-on option in the multidisciplinary treatment of FM, due to its rapid action and high patients’ compliance. The application of WBC protocols has the potential to expand therapeutic options for the treatment of FM and related disorders; however, larger, high-quality primary studies are still needed.
1. Introduction
Fibromyalgia (FM) is a medical condition characterized by the combination of complex, sometimes indistinct, symptoms. FM manifestations include chronic widespread musculoskeletal pain and associated fatigue, morning stiffness, sleep disturbances [1,2], depression, anxiety, and cognitive symptoms [3,4], in line with the biopsychosocial model of pain [5], and evidence related to other chronic pain conditions [6,7,8]. In addition, FM is associated with psychological factors, such as neuroticism [9], alexithymia [10], catastrophizing [11], and low health-related quality of life [4], limiting people’s daily activities as well as their social, professional, and recreational activities [12,13]. FM is the third most common musculoskeletal condition and is estimated to affect 0.2 to 6.6% of the adult general western population [14,15]. Due to its persistent and debilitating condition, FM imposes enormous economic burdens on society, as patients with FM have relatively high levels of comorbidities and high levels of health care utilization and cost [16].
Despite predisposing factors (genetic, stressful or traumatic events, viral infections, and obesity), the etiopathogenesis of FM is still not fully unraveled, making its diagnostic and classification criteria confusing. One of the most widely held hypotheses regarding the pathogenesis of FM is central sensitization to pain and deficits in endogenous pain-inhibiting mechanisms. Several studies in patients with FM have shown a lower threshold and tolerance for pain [17,18], hyperalgesia and allodynia [19], a slower cognitive processing speed [20], a cortical or subcortical increase in pain processing compared with healthy subjects [21], and evidence of the presence of polyneuropathy in both small and large fibers [22]. All these symptoms suggest a neurogenic common origin characterized by an imbalance in the levels of neurotransmitters and consequently of the peripheral pro- and anti-inflammatory mediators [23]. Due to lack of agreement regarding its diagnosis, classification and etiopathogenesis, no consistently effective treatments are yet available. In many cases, FM has been seen as a “disease of misconnection” at different levels characterized by lack of specific biomarkers [2,24].
In most cases, the therapeutic approach is characterized by multidisciplinary interventions that include patient’s education, physiotherapy (including physical agents and exercise), pharmacological treatment, and psychotherapy [2]. Therapies for the management of FM are mainly focused on easing patients’ symptoms and improving quality of life [25]. Although some studies have been conducted examining pharmacological and non-pharmacological interventions, treating patients with FM using a multimodal approach appears to be the most effective option even if more trials are needed [26]. Conventional pharmacological therapies usually rely on cyclic or chronic use of antidepressants, muscle relaxants, anti-inflammatories, and antioxidants [27]. Non-pharmacological measures consist of: (i) physiotherapy, including a variety of physical agents and land- or water-based physical exercise, such as aquatic or aerobic-based exercise, strength training (anaerobic exercise), and flexibility training; and (ii) psychotherapy, including cognitive-behavioral interventions, biofeedback, and psychological support [28,29]. With the growing recognition that there are different categories of FM with different clinical features, personalized prescription should be an important target to be achieved among the empirical and constantly evolving approaches that are proposed.
Whole-body cryostimulation (WBC) is a highly effective physical treatment mainly used in sports medicine to relieve pain, inflammatory symptoms, fatigue, and overuse symptoms due to its widely recognized anti-inflammatory and anti-oxidant effects [30]. Presently, it has been used as an add-on therapy in rheumatic (arthritis [30], fibromyalgia [31,32,33,34,35,36,37,38,39,40], and ankylosing spondylitis [41]), neurological (multiple sclerosis [42]) psychiatric (depression) [43], metabolic (obesity) [44], and diabetes [45]. WBC consists of exposure of a part or the whole body to very cold and dry air for generally 2 to 3-min. At present, there are two types of cryostimulation. Partial-body cryostimulation (PBC), where the body, excluding the head, is exposed to a cryogenic fluid injected and vaporized around the body inside a cryosauna, and the whole-body cryostimulation (WBC), performed inside a cryochamber, where the whole body is exposed to cold produced by cryogenic fluids or refrigerants [46]. Given the limited amount of published literature, we adopted studies performed with both a cryochamber and a cryosauna, all reported as “Whole-body Cryostimulation”, despite knowing the different physiological reactions after PBC and WBC due to their large differences in internal temperatures measured with PBC having a higher gradient. The thermal stress elicited by cryostimulation generates vasoconstriction and stimulate the thermal receptors of the dermis by lowering skin temperature, and slowing down nerve conduction in pain fibers, which may be a way that cryotherapy induces an analgesic effect, relieving pain and inflammatory symptoms [47,48]. Moreover, it causes changes in the endocrine, circulatory, neuromuscular, and immunological system [49]. It provides homeostatic autonomic responses of thermogenesis and vasoconstriction by stimulating cold receptors and the thermoregulatory center in the hypothalamus from which efferent signals cause activation of the sympathetic system resulting in vasoconstriction followed by release of noradrenaline. Along with endorphins, norepinephrine modulates pain and slow conduction velocity of sensory nerve fibers such as C fibers, disabling the sensory receptors as well as their connections to proprioceptors [50]. An increase in parasympathetic cardiac control also occurs. Indeed, after cryostimulation, as a compensatory mechanism, downregulation of blood pressure [50], even overnight [51], may result in reduced feelings of fatigue, improved mood, and reduced mental health deterioration with possible positive consequences on depressive states, and improved sleep quality [43]. Recent literature has shown that WBC is immunostimulating and yields an anti-inflammatory response, with a decrease of the pro-inflammatory cytokines and increases of anti-inflammatory mediators [52,53,54,55,56,57]. It also appears to improve the effect on redox balance in a session/treatment number-, age-, and fitness-dependent manner [58], probably through the decrease in the total oxidant production which, consequently, induces antioxidant activity [56,58,59,60,61,62,63]. Thus, due to its widely recognized anti-inflammatory, antioxidant, analgesic, and exercise-mimicking effects [64], WBC is proposed as a promising add-on option in the multidisciplinary treatment of FM, considering also that diffuse inflammation is one of the sub mechanisms of depression [65], and that co-morbid depression is very common among FM patients, with a lifetime prevalence of 62–86% [66]. In addition, all the articles we have cited in this scoping review reported no major side effects even after a great number of WBC sessions demonstrating the possibility of developing protocols that include a large number of treatments. This scoping review aims to update the reader as to the current evidence supporting the therapeutic effects of WBC in patients with FM and directions on the possible adjuvant use of WBC in the treatment of FM.
2. Materials and Methods
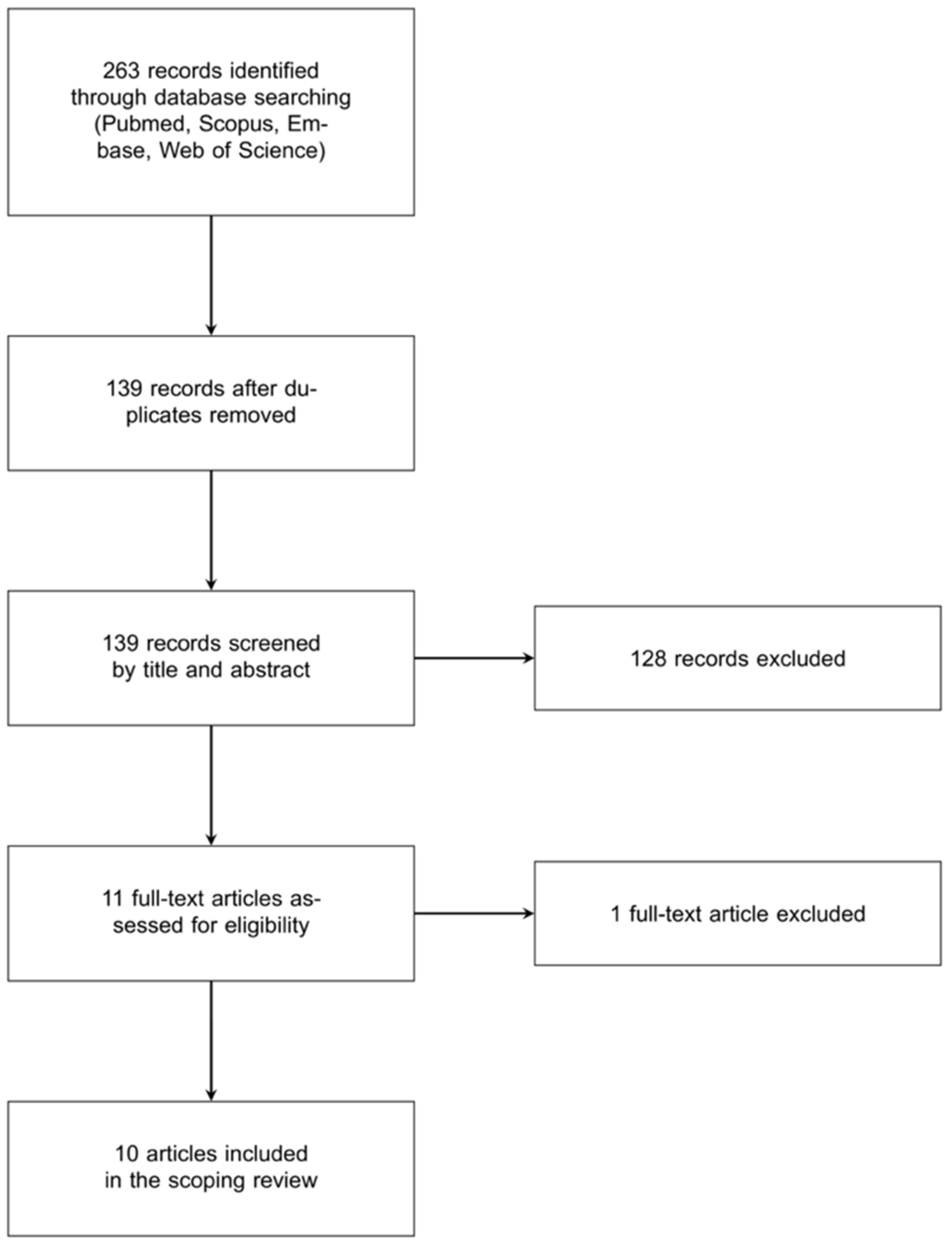
All the procedures of this scoping review followed an unpublished review protocol which was drafted prior to the electronic search. This search was conducted using the electronic databases Pubmed, Scopus, Embase and Web of Science using strings that combined keywords referring to WBC with keywords referring to FM. Figure 1 illustrates the flowchart of the literature search, while the complete strings and number of records retrieved in each database are given in the Supplementary Materials (Table S1). No restrictions were applied regarding the publication date, and only articles written in English, Italian, French, and Spanish languages were considered. The reference lists of the existing reviews focusing on cryotherapy were scanned to find further relevant records. The studies were included if: (1) they were published in an original article or as conference proceedings, (2) they evaluated the effects of WBC, defined as short exposures to air temperatures below −100 °C, and (3) their study sample was composed by patients with an age between 25 and 70 and with a medical diagnosis of FM. The lists of the records retrieved by performing the electronic search were uploaded to the online software Rayyan [67] to perform the title and abstract screening. Three independent reviewers performed this screening and conflicts were resolved by consensus. Then, the full texts of the screened articles were assessed and the ones that met the inclusion criteria and did not meet the exclusion criteria were included in the review. This assessment phase was performed by two reviewers and conflicts were solved by consensus. A pre-specified spreadsheet was used to extract data from the included articles. The following data were extracted: study design; country where the study was performed; experimental population and experimental subgroups (including drop-outs); age (means and standard deviations or median and interquartile ranges); female percentage of the sample; WBC protocol (and other therapy protocols, if used, such as mud bath and hot air) including number of WBC sessions, duration of each WBC sessions, and WBC temperature; sampling (measurements, surveys) time; primary and secondary outcome(s); outcome assessment instrument(s); and synthesis of the results. A Downs and Black modified checklist [68,69] was used to evaluate the methodological quality of evidence under the categories of reporting, external validity, internal validity-bias, internal validity-confidence (selection bias), and power. The Downs and Black quality assessment tool was modified by removing questions about interventions performed because some studies included in this review used observational study designs. This quality evaluation instrument consisted of four sections that assessed the quality of reported outcomes (items 1, 2, 3, 6, 7, 9, and 10), external validity (items 11 and 12), internal validity (16, 17, 18, 20, and 26), and power (item 27). The highest score for the item was 25, with a higher total score indicating higher quality of evidence for the specific study. Quality and level of evidence were assessed by two authors (JMF) and (MG), and is summarized in Table 1 It was not used to evaluate studies in abstract-only format due to their obvious low score as a result of the inability to address most of the checklist questions. The Downs and Black modified checklists assess the following domains in both randomized and non-randomized studies: quality of the reporting, external validity, presence of bias, presence of confounding, and power of the applied statistical analysis. The extracted data were tabulated to provide a description of each study and the results were described narratively.
3. Results
The database search retrieved 263 records in total, and 10 of the returned articles, which includes original articles and conference abstracts between 2000 and 2018, with a total of 597 participants (446 with primary fibromyalgia, 21 with rheumatoid arthritis, 20 with chronic low back pain, 13 with ankylosing spondylitis, 11 with osteoarthritis, 4 with secondary fibromyalgia, and 2 with other autoimmune diseases), met eligibility criteria and were included in this review.
Table S1 illustrates the search strings employed during the electronic search and the number of records retrieved, Table 1 summarizes the quality and level of evidence of the selected articles, Table 2 presents their characteristics and Table 3 summarizes their outcomes and results. Two articles used a non-controlled study design [31,36], three articles used a non-randomized controlled study design [33,37,38], five articles used a randomized controlled study design [32,34,35,39], and one of them used a crossover design [40]. Five studies were conducted in Germany [31,32,36,37,38], two in Italy [33,34], and one each in India [39], Spain [40], and Belgium [35].
Scoring the quality of the articles using the Downs and Black modified quality checklist was carried out independently by three researchers (MG, JMF, and PP), who discussed their scoring disagreements and reached a consensus. The maximum score that articles could receive from this assessment tool was 14 out of 15 points. The average score was 11.6 points. No articles reached the maximum score of 15. The quality assessment of each of the included articles is presented in Table 2. As mentioned above, evaluation of the quality of conference abstracts [31,32,34,39] was not included due to the different type of format that would have influenced the evaluation. Pain intensity, condition, state, or level was evaluated in eight studies [32,33,34,35,36,37,38,40]. Four studies assessed physical and mental health [33,35,39,40] while only one assessed global health status [33]. Three studies assessed fatigue [33,34,39], and well-being [36], number of tender points [38], sleep disturbances [39], and quality of life [35] were each assessed by only one study. Severity of FM [39] and disease activity [40] were evaluated in one study each. Two studies quantified the changes in gene expression: one using transcriptomics [60] and analyzing transcripts fold change, the other study quantifying the change of gene expression in specifically selected genes (CCL4, TGFBR3, CD69, and MAP2k3) [31]. Finally, only one study investigated the markers of inflammation IL-1, IL-6, IL-10, and TNF-α [37]. Each study considered recruiting of patients diagnosed with FM. One study also included patients with rheumatoid arthritis, chronic low back pain, ankylosing spondylitis, osteoarthritis, secondary fibromyalgia, and other autoimmune diseases [36]. All articles compared the effects of WBC on FM, at baseline and after more than one exposure. Eight articles used only one experimental group (FM patients) [31,32,33,34,35,38,39,40], while, as mentioned above, one paper included other diseases besides FM [36]. Of note, healthy controls exposed to WBC were used only in one occasion [37]. One article also compared the effect of WBC to the effect of warm therapy (consisting of a warm mud bath followed by hot air) [38]. Two articles performed a follow-up of one [35] and three [37] months respectively. All studies included more than 50% female subjects.
In six studies using WBC, the participants spent a 10-sec-to-1-min adaptation period at −60 °C in a vestibule connected directly to the main chamber [31,32,33,34,38,40]. Afterward, cryostimulation was applied at −110 °C in four studies, −140 °C in two studies, and −105 °C, −130 °C, and −196 °C in one study each. One study did not state the temperature [39]. The cryostimulation treatments lasted between two and three minutes in every study. The number of exposures varied between 3 and 48 sessions. A cryosauna was used in two cases [37,40], and a cryochamber in the eight other studies. Among the adverse effects during and after cryotherapy included: heartbeat feeling in whole body, palpitations, sleep difficulties, bowel sounds and bloating, muscle stiffness, tremor, headache [40] or migraine, burns (comparable to a light sunburn), increase in pain, shortness of breath, feeling of anxiety due to the narrowness of the chamber, circulatory problems, dizziness, and anxiety [36] and anxiety symptoms, partly with panic attacks [38].
4. Discussion
This literature review includes original articles and conference abstracts between 2000 and 2018 describing the effects of WBC in patients with FM and aims to provide a comprehensive and up-to-date summary of the most recent findings supporting its adjuvant therapeutic use. Given the paucity of good quality published studies on this topic, a systematic review could not be conducted. This exploratory review primarily describes and discusses the effects of WBC on pain (intensity, level, changes and impact, and painful tender points); impact of disease (ability to perform large muscle tasks, difficulty with work, pain, fatigue, morning tiredness, stiffness, and depression); severity of FM (prevalent clinical manifestations, emotional, physical, and coping [active and passive] aspects); self-rated physical mental and global health; emotional (anxiety and depression) and physical factors (pain, fatigue, sleep quality, and functional ability); well-being index; health-related quality of life; hematological inflammatory parameters; gene expression of protein involved in inflammatory, pain processing pathways and small nucleolar RNAs.
4.1. Clinical Effects of WBC in FM
Pain perception involves interconnected physiological and psychological mechanisms that include anatomical, physiological, cognitive, and affective components of pain [70]. There are two neural pathways that regulate pain signals: ascending pathways that transmit sensory signals through peripheral nerves, including nociceptive signals, to the spine and brain for processing; and descending pathways that send modulatory (excitatory and/or inhibitory) signals from the brain to the periphery, regulating ascending nociceptive signals that reach the brain [71]. These physical and noxious chemical signals are detected by nociceptors, specialized receptors in peripheral nerves activated by physical stimuli (i.e., changes in temperature, pressure, and impact). Many neurotransmitters and neurochemicals are involved in the transmission of pain signals such as norepinephrine and serotonin [72].
In FM, these two neural pathways operate abnormally causing an increased activity in the pain matrix which results in central amplification of pain signals, a phenomenon named central sensitization [73]. Several studies of FM-related pain and hyperalgesia have demonstrated the involvement of spinal mechanisms and an enhanced response to somatic and cutaneous stimuli throughout the brain’s pain matrix, allodynia and hyperalgesia. In most cases, patients become hypersensitive to pain. The constant hypervigilance to pain can also be associated with psychological problems [74].
Most of the studies included in this review (7 out of 10) hypothesized that WBC should alleviate pain and/or inflammatory processes in FM patients, with the aim of improving health-related quality of life. These studies tested the therapeutic efficacy of WBC and its practicability for clinical routine in FM, also comparing it to other therapies (warm therapy or steam therapy) or treatments (antioxidants and analgesic agents).
All studies reported an analgesic effect of WBC with significant reduction in pain level, but had different settings. Bettoni et al. carried out two studies on the efficacy and safety of WBC in FM patients. The first report showed the superiority of WBC compared to antioxidants and analgesic agents, in terms of pain and fatigue reduction [34]. In the second study, patients performed aerobic exercise (cycle ergometer or treadmill) for 30 min immediately after WBC [33]. Physical activity, which is also used to treat FM, may have masked these results by opposing its induced vasodilation to WBC-induced vasoconstriction. In the cross-over trial of Rivera et al., the individuals’ VAS and FIQ scores did not return to baseline after the first treatment with WBC due to too short wash-out periods, so that only results of the first sequence could be reported [40]. Vitenet et al. reported that WBC significantly improved health-reported quality of life, evaluated through the changes in the Medical Outcome Study Short Form-36 (10 sessions over 8 days) [35]. However, the sample size was limited, as only 11 patients underwent WBC and the control group protocol was not described in detail. This was the same for the study of Metzger et al. that described a decreased pain intensity and a short-term pain relief of about 1.5 h after cold application. No control group receiving a regular rehabilitation program could be compared to a group additionally treated with WBC [36]. Therefore, the reduction in pain could probably be due not only to the analgesic effect of the WBC, but also to the effect of the applications carried out in parallel. However, they described some adjustment time before reaching maximum pain relief, in their case after about two weeks (half of the treatment). Interestingly, most patients rated the effect of WBC as not very effective in the context of the overall treatment, perhaps also due to the session conditions (temperature −105 °C and 2–3 patients in the chamber). Klemm et al. included patients with standard treatment before and during the study, excluding physical activity as a possible confounder of the reduced level of pain found after WBC treatment, but no control group not undergoing WBC was present [37].
Only Rivera et al. [40] and Klemm et al. [37] investigated the effects of WBC on FIQ, and only Vitenet et al. [35] and Klemm et al. [37] included a follow-up, after 1 and 3 months, respectively, showing that the effects of WBC on pain and disease activity after discontinued treatment were no longer reduced. In addition, Klemm et al. demonstrated that serial WBC (between 6 and 10 sessions in a maximum of 3 weeks) elicited effects for more than 1 month after the end of WBC treatment, then decreasing gradually to null effect after 3 months [37].
Two studies compared the effects of WBC with other classic thermotherapy methods. Kurzeja et al. investigated the effect of thermotherapy with WBC (−110 °C) alone compared with mud bath (+40 °C) and hot air (+42 °C) combined in the daily shift. Pain intensity was reduced in all groups with no significant differences between groups [38]. However, the pain scores in the WBC group were lower and the patients described a 2-h pain relief after cold exposure.
The abstract of Sundaram mentions that WBC provides better results in association with physiotherapy than with steam therapy. Improvement in pain, general health, fatigue, and sleep are attributed by the author to the systemic response and serotonin levels stimulated by WBC [39]. However, no information about the temperature was mentioned, the sample was not homogeneous in terms of age and gender, and there were no actual data to corroborate the findings and conclusions.
4.2. Molecular Effects of WBC in FM
The pathogenesis of FM not only includes pain sensitivity, pain inhibition, or pain amplification, but also an imbalance of pro- and anti-inflammatory cytokines, genetic predisposition, and environmental triggers such as mechanical/physical trauma or injury and psychosocial stressors that ultimately leads to pain and impaired pain processing.
There is growing evidence of neuroinflammation in FM. Several pro-inflammatory cytokines, including TNF-α, IL-1β, IL-6, and tumor necrosis factor α (TNF-α), have been found to be elevated in animal models of neuropathic pain and in the cerebrospinal fluid (CSF), peripheral tissues, and blood of patients with chronic neuropathic pain conditions [75]. In addition, pharmacologically lowering or blocking of these pro-inflammatory cytokines has been demonstrated to prevent, reduce, or reverse pain (allodynia and hyperalgesia) in both animal models and clinical studies [76].
Thus, the imbalance of pro- and anti-inflammatory cytokines is assumed to play a role in the induction and maintenance of pain and the occurrence of many of the clinical features of FM (such as swelling, dysesthesia, skin manifestations, fluid retention, and increased levels of fibronectin, which is a tissue marker of endothelial activation) as a result of a neuroinflammatory condition that gives rise to descending pathways that influence predominant symptoms, such as pain, fatigue, and cognitive impairment. In addition, environmental triggers, stress, and emotions are the upstream driving mechanism of neurogenic inflammation in FM [77].
Therefore, the likelihood that FM may have an imbalance in cytokine production and secretion has been confirmed. Ucelyer et al. showed that FM patients have higher serum levels of IL-1ra, IL-6, and IL-8, and higher plasma levels of IL-8, compared to controls [78], while two studies of Lubkowska et al. showed how WBC affects the inflammatory status by inducing an imbalance towards the anti-inflammatory side [55,56]. Consecutive sessions of cryotherapy increased levels of IL-6, which can act both as a pro-inflammatory and anti-inflammatory cytokine, and IL-10, an anti-inflammatory cytokine, and lowered the IL-1α levels. Furthermore, WBC appears to improve the oxidative status already after a limited number of sessions, in a dose-dependent way [58,59].
Klemm et al. integrated the clinical effects with the molecular effects of WBC [37]. In parallel with changes in disease activity and pain reduction, patients with FM showed a significantly different response to WBC compared with healthy controls in terms of changes in IL1, -6, -10, and TNF-α over time to WBCs. FM patients had higher levels of IL-1, -6, -10, and TNF-α at baseline compared to healthy subjects. IL-1, IL-6, and IL-10 levels decreased significantly after three and six sessions and stabilized up to three months after discontinued WBC treatment. Interestingly, IL-6 levels returned to baseline after three months only in healthy controls and showed significantly decreased IL-6 levels at each reading point compared to baseline. WBC had no effect on TNF-α levels, neither in FM patients nor in healthy controls.
Therefore, even if the levels of IL-1, IL-6, and IL-10 in FM patients were higher than healthy controls after 6 WBC sessions and 3 months after the last WBC session, their significant alteration confirms the overall beneficial effects of WBC.
4.3. Gene Expression after WBC in FM
Drynda et al. investigated the changes in gene expression on peripheral blood cells of patients with FM going through a series of three exposures to WBC within three days [32]. One study correlated the reduced pain intensity with transcripts that were found significantly changed already after a single exposure to WBC. The majority of down-regulated transcripts belonged to a group of small nucleolar RNA (SNORD) while the up-regulated transcripts were a few specific genes, such as PBX1, SFRP2, MAP2K3, and SLC25A39. SNORD molecules belong to so-called non-coding RNAs. Emerging evidence has demonstrated that they are involved in various physiological and pathological cellular processes acting as internal signals that control various levels of gene expression. However, the sample size and homogeneity were rather limited, as only 10 patients were studied.
Another study from the same group investigated on a larger cohort of 22 patients the changes in the gene expression of selected genes (CCL4, TGFBR3, CD69, and MAP2K3) identified as significantly regulated in cells from peripheral blood of patients with FM going through a series of three exposures to WBC within three days [31]. The expression levels of CCL4 and CD69, two proteins produced upon activation of T-lymphocytes, reduced significantly after the third exposure compared to baseline. In contrast, the expression of MAP2K3, a protein activated by cytokines and environmental stress in vivo, was found to be up-regulated in 13 patients, while the expression levels in the other 9 patients remained almost unchanged. Interestingly, the changes of gene expression were evident already after the first cold exposure, but reached statistical significance after the third exposure. The down-regulation of TGFBR3, a membrane proteoglycan that often functions as a co-receptor with other TGF-β receptors observed in the pilot study, could not be confirmed in the larger cohort. Unfortunately, both studies are scientific abstracts only and do not provide further speculation or discussion of the results.
5. Conclusions
Our scoping review summarizes the current understanding of the role of WBC as an adjunctive treatment for FM. The article has several limitations. First, the molecular mechanisms and regulation of gene expression behind the reported beneficial effects of WBC have not been fully investigated, as only changes in a few inflammatory markers and genes have been observed. Second, the absence of standard protocols for the use of WBC in the treatment of FM (temperature, number of sessions, exposure time, and sample collection time) might be responsible for the inconsistency of the reported results. In this regard, many of the studies we evaluated had confounding factors such as physical activity and pharmacological treatment, which play a key role in the modulation of several pain components (such as anti-inflammatory and antioxidants). Third, the lack of adequately designed randomized controlled trials, a blinding system, or adequate control groups within the researched papers substantially reduced the quality of the articles. In general, the modest amount of published literature, the low quality of the studies and information provided, the absence of standard protocols, and the small irregular sample sizes make it difficult to compare results between studies. Randomized control trials are needed to confirm and strengthen the significance of WBC-induced clinical changes and identify its effects at the molecular level. Therefore, the results of our scoping review cannot definitively support WBC as an effective adjunctive treatment for FM. However, despite important limitations of the available studies, initial evidence indicates that WBC reduces FM symptoms. Particularly due to its rapid anti-inflammatory effect, WBC has the potential to improve rehabilitation programs in patients with FM, which seems attractive in terms of the cost-effectiveness of rehabilitation. Not secondarily, the high patient compliance and highly positive perception of treatment reported in most studies seem to make WBC a preferred component of the rehabilitation program, which appears crucial in the long-term management of FM.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/app12094794/s1, Table S1: Search strings employed during the electronic search and number of records retrieved.
Author Contributions
Conceptualization, P.C., J.M.F., M.G. and P.P.; Methodology, J.M.F., M.G., P.P. and E.M.G.; Validation, J.M.F., M.G., P.P. and E.M.G.; Formal Analysis, P.C. and J.M.F.; Investigation, J.M.F., M.G. and P.P.; Resources, P.C.; Data Curation, E.M.G.; Writing—Original Draft Preparation, J.M.F., M.G. and P.P.; Writing—Review & Editing, P.C., J.M.F., M.G., P.P. and E.M.G.; Visualization, J.M.F., M.G., P.P. and E.M.G.; Supervision, P.C.; Project Administration, P.C., J.M.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest. The authors alone are responsible for the content and writing of the article.
Abbreviations
AD: other Autoimmune Diseases; AS: ankylosing spondylitis; avg: average; CLBP: chronic low back pain; F: females; FIQ: Fibromyalgia Impact Questionnaire; FM: patients with fibromyalgia; 1º FM: Primary Fibromyalgia; 2º FM: Secondary fibromyalgia; FSS fatigue severity scale; GH Global Health; hrs: hours; ICAF: Combined Index of Severity of Fibromyalgia; M: males; MCID: minimum clinically important difference; MCS: mental composite score; MOS SF-36: Medical Outcome Study Short Form-36; n: sample size; n.r.: not reported; OA: Osteoarthritis; PCS: physical composite score; PSE: patient self-assessment; Ps: study participants; RA: Rheumatoid Arthritis; SI: pain intensity; SNORD: small nucleolar RNA; TNFα: tumor necrosis factor; TP: tender points; VAS: Visual Analog Scale; WBC: whole-body cryostimulation; WT: Warm Therapy.
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An Update on Clinical Characteristics, Aetiopathogenesis and Treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- van Middendorp, H.; Lumley, M.A.; Jacobs, J.W.G.; van Doornen, L.J.P.; Bijlsma, J.W.J.; Geenen, R. Emotions and Emotional Approach and Avoidance Strategies in Fibromyalgia. J. Psychosom. Res. 2008, 64, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Reyes Del Paso, G.A. Depression and Trait-Anxiety Mediate the Influence of Clinical Pain on Health-Related Quality of Life in Fibromyalgia. J. Affect. Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Wilson, H.; Swanson, K.S. The Biopsychosocial Model of Pain and Pain Management. In Behavioral and Psychopharmacologic Pain Management; Cambridge University Press: Cambridge, UK, 2010; pp. 16–43. ISBN 978-0-521-88434-1. [Google Scholar]
- Varallo, G.; Giusti, E.M.; Scarpina, F.; Cattivelli, R.; Capodaglio, P.; Castelnuovo, G. The Association of Kinesiophobia and Pain Catastrophizing with Pain-Related Disability and Pain Intensity in Obesity and Chronic Lower-Back Pain. Brain Sci. 2021, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Varallo, G.; Scarpina, F.; Giusti, E.M.; Cattivelli, R.; Guerrini Usubini, A.; Capodaglio, P.; Castelnuovo, G. Does Kinesiophobia Mediate the Relationship between Pain Intensity and Disability in Individuals with Chronic Low-Back Pain and Obesity? Brain Sci. 2021, 11, 684. [Google Scholar] [CrossRef] [PubMed]
- Picavet, H.S.J.; Vlaeyen, J.W.S.; Schouten, J.S.A.G. Pain Catastrophizing and Kinesiophobia: Predictors of Chronic Low Back Pain. Am. J. Epidemiol. 2002, 156, 1028–1034. [Google Scholar] [CrossRef]
- Montoro, C.I.; Reyes del Paso, G.A. Personality and Fibromyalgia: Relationships with Clinical, Emotional, and Functional Variables. Personal. Individ. Differ. 2015, 85, 236–244. [Google Scholar] [CrossRef]
- Montoro, C.I.; Reyes del Paso, G.A.; Duschek, S. Alexithymia in Fibromyalgia Syndrome. Personal. Individ. Differ. 2016, 102, 170–179. [Google Scholar] [CrossRef]
- Velasco, L.; López-Gómez, I.; Gutiérrez, L.; Écija, C.; Catalá, P.; Peñacoba, C. Exploring the Preference for Fatigue-Avoidance Goals as a Mediator Between Pain Catastrophizing, Functional Impairment, and Walking Behavior in Women with Fibromyalgia. Clin. J. Pain 2022, 38, 182–188. [Google Scholar] [CrossRef]
- Kramer, S.; Deuschle, L.; Kohls, N.; Offenbächer, M.; Winkelmann, A. The Importance of Daily Activity for Reducing Fibromyalgia Symptoms: A Retrospective “Real World” Data Comparison of Two Multimodal Treatment Programs. Arch. Rheumatol. 2020, 35, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Farin, E.; Ullrich, A.; Hauer, J. Participation and Social Functioning in Patients with Fibromyalgia: Development and Testing of a New Questionnaire. Health Qual. Life Outcomes 2013, 11, 135. [Google Scholar] [CrossRef] [Green Version]
- Creed, F. A Review of the Incidence and Risk Factors for Fibromyalgia and Chronic Widespread Pain in Population-Based Studies. Pain 2020, 161, 1169–1176. [Google Scholar] [CrossRef]
- Marques, A.P.; Santo, A.d.S.d.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of Fibromyalgia: Literature Review Update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Berger, A.; Dukes, E.; Martin, S.; Edelsberg, J.; Oster, G. Characteristics and Healthcare Costs of Patients with Fibromyalgia Syndrome. Int. J. Clin. Pract. 2007, 61, 1498–1508. [Google Scholar] [CrossRef] [Green Version]
- de la Coba, P.; Bruehl, S.; Moreno-Padilla, M.; Reyes del Paso, G.A. Responses to Slowly Repeated Evoked Pain Stimuli in Fibromyalgia Patients: Evidence of Enhanced Pain Sensitization. Pain Med. 2017, 18, 1778–1786. [Google Scholar] [CrossRef]
- de la Coba, P.; Bruehl, S.; Galvez-Sánchez, C.M.; Reyes Del Paso, G.A. Slowly Repeated Evoked Pain as a Marker of Central Sensitization in Fibromyalgia: Diagnostic Accuracy and Reliability in Comparison with Temporal Summation of Pain. Psychosom. Med. 2018, 80, 573–580. [Google Scholar] [CrossRef]
- Maugars, Y.; Berthelot, J.-M.; Le Goff, B.; Darrieutort-Laffite, C. Fibromyalgia and Associated Disorders: From Pain to Chronic Suffering, from Subjective Hypersensitivity to Hypersensitivity Syndrome. Front. Med. 2021, 8, 666914. [Google Scholar] [CrossRef] [PubMed]
- Montoro, C.I.; Duschek, S.; Muñoz Ladrón de Guevara, C.; Fernández-Serrano, M.J.; Reyes del Paso, G.A. Aberrant Cerebral Blood Flow Responses during Cognition: Implications for the Understanding of Cognitive Deficits in Fibromyalgia. Neuropsychology 2015, 29, 173–182. [Google Scholar] [CrossRef]
- Gracely, R.H.; Petzke, F.; Wolf, J.M.; Clauw, D.J. Functional Magnetic Resonance Imaging Evidence of Augmented Pain Processing in Fibromyalgia. Arthritis Rheum. 2002, 46, 1333–1343. [Google Scholar] [CrossRef]
- Martínez-Lavín, M. Fibromyalgia and Small Fiber Neuropathy: The Plot Thickens! Clin. Rheumatol. 2018, 37, 3167–3171. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J.; Arnold, L.M.; McCarberg, B.H. The Science of Fibromyalgia. Mayo Clin. Proc. 2011, 86, 907–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrot, S. Fibromyalgia: A Misconnection in a Multiconnected World? Perrot—European Journal of Pain; Wiley Online Library. 2019. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/ejp.1367 (accessed on 7 March 2022).
- Briones-Vozmediano, E.; Vives-Cases, C.; Ronda-Pérez, E.; Gil-González, D. Patients’ and Professionals’ Views on Managing Fibromyalgia. Pain Res. Manag. 2013, 18, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR Revised Recommendations for the Management of Fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Welsch, P.; Klose, P.; Derry, S.; Straube, S.; Wiffen, P.J.; Moore, R.A. Pharmacological Therapies for Fibromyalgia in Adults—An Overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2018, 2018, CD013151. [Google Scholar] [CrossRef]
- Rolls, C.; Prior, Y. 285 Non-Pharmacological Interventions for People with Fibromyalgia: A Systematic Review. Rheumatology 2018, 57, key075.509. [Google Scholar] [CrossRef] [Green Version]
- Hassett, A.L.; Williams, D.A. Non-Pharmacological Treatment of Chronic Widespread Musculoskeletal Pain. Best Pract. Res. Clin. Rheumatol. 2011, 25, 299–309. [Google Scholar] [CrossRef]
- Sadura-Sieklucka, T.; Sołtysiuk, B.; Karlicka, A.; Sokołowska, B.; Kontny, E.; Księżopolska-Orłowska, K. Effects of Whole Body Cryotherapy in Patients with Rheumatoid Arthritis Considering Immune Parameters. Reumatologia/Rheumatology 2019, 57, 320–325. [Google Scholar] [CrossRef]
- Drynda, S.; Mika, O.; Kekow, J. THU0313 Impact of Whole-Body Cryotherapy on Gene Expression of Peripheral Blood Cells in Patients with Fibromyalgia. Ann. Rheum. Dis. 2015, 74, 309. [Google Scholar] [CrossRef]
- Drynda, S.; Mika, O.; Koczan, D.; Kekow, J. AB0661 Impact of Whole-Body Cryotherapy on Transcriptome of Peripheral Blood Cells in Patients with Fibromyalgia. Ann. Rheum. Dis. 2013, 72, A990–A991. [Google Scholar] [CrossRef]
- Bettoni, L.; Bonomi, F.G.; Zani, V.; Manisco, L.; Indelicato, A.; Lanteri, P.; Banfi, G.; Lombardi, G. Effects of 15 Consecutive Cryotherapy Sessions on the Clinical Output of Fibromyalgic Patients. Clin. Rheumatol. 2013, 32, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Bettoni, L.; Bonomi, F.G.; Zani, V.; Indelicato, A.; Banfi, G. THU0347|Efficacy and Safety of Whole Body Cryotherapy in Fibromyalgic Patients|Annals of the Rheumatic Diseases. Available online: https://0-ard-bmj-com.brum.beds.ac.uk/content/71/Suppl_3/273.1 (accessed on 7 March 2022).
- Vitenet, M.; Tubez, F.; Marreiro, A.; Polidori, G.; Taiar, R.; Legrand, F.; Boyer, F.C. Effect of Whole Body Cryotherapy Interventions on Health-Related Quality of Life in Fibromyalgia Patients: A Randomized Controlled Trial. Complement. Ther. Med. 2018, 36, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Metzger, D.; Zwingmann, C.; Protz, W.; Jäckel, W.H. Whole-body cryotherapy in rehabilitation of patients with rheumatoid diseases—Pilot study. Rehabilitation 2000, 39, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Klemm, P.; Becker, J.; Aykara, I.; Asendorf, T.; Dischereit, G.; Neumann, E.; Müller-Ladner, U.; Lange, U. Serial Whole-Body Cryotherapy in Fibromyalgia Is Effective and Alters Cytokine Profiles. Adv. Rheumatol. 2021, 61, 3. [Google Scholar] [CrossRef]
- Kurzeja, R.; Gutenbrunner, C.; Krohn-Grimberghe, B. Primäre Fibromyalgie: Vergleich der Kältekammertherapie mit zwei klassischen Wärmetherapieverfahren. Aktuelle Rheumatol. 2003, 28, 158–163. [Google Scholar] [CrossRef]
- Sundaram, V.M. To Compare the Effectiveness of Whole Body Cryotherapy against Steam Therapy in Patients with Chronic Fibromyalgia. Physiotherapy 2015, 101, e988–e989. [Google Scholar] [CrossRef] [Green Version]
- Rivera, J.; Tercero, M.J.; Salas, J.S.; Gimeno, J.H.; Alejo, J.S. The Effect of Cryotherapy on Fibromyalgia: A Randomised Clinical Trial Carried out in a Cryosauna Cabin. Rheumatol. Int. 2018, 38, 2243–2250. [Google Scholar] [CrossRef] [Green Version]
- Romanowski, M.W.; Straburzyńska-Lupa, A. Is the Whole-Body Cryotherapy a Beneficial Supplement to Exercise Therapy for Patients with Ankylosing Spondylitis? J. Back Musculoskelet. Rehabil. 2020, 33, 185–192. [Google Scholar] [CrossRef]
- Miller, E.; Kostka, J.; Włodarczyk, T.; Dugué, B. Whole-Body Cryostimulation (Cryotherapy) Provides Benefits for Fatigue and Functional Status in Multiple Sclerosis Patients. A Case-Control Study. Acta Neurol. Scand. 2016, 134, 420–426. [Google Scholar] [CrossRef]
- Rymaszewska, J.; Lion, K.M.; Pawlik-Sobecka, L.; Pawłowski, T.; Szcześniak, D.; Trypka, E.; Rymaszewska, J.E.; Zabłocka, A.; Stanczykiewicz, B. Efficacy of the Whole-Body Cryotherapy as Add-on Therapy to Pharmacological Treatment of Depression—A Randomized Controlled Trial. Front. Psychiatry 2020, 11, 522. [Google Scholar] [CrossRef]
- Fontana, J.M.; Bozgeyik, S.; Gobbi, M.; Piterà, P.; Giusti, E.M.; Dugué, B.; Lombardi, G.; Capodaglio, P. Whole-Body Cryostimulation in Obesity: A Scoping Review. J. Therm. Biol. 2022, 106, 103250. [Google Scholar] [CrossRef]
- Kozłowska, M.; Kortas, J.; Żychowska, M.; Antosiewicz, J.; Żuczek, K.; Perego, S.; Lombardi, G.; Ziemann, E. Beneficial Effects of Whole-Body Cryotherapy on Glucose Homeostasis and Amino Acid Profile Are Associated with a Reduced Myostatin Serum Concentration. Sci. Rep. 2021, 11, 7097. [Google Scholar] [CrossRef] [PubMed]
- Bouzigon, R.; Grappe, F.; Ravier, G.; Dugue, B. Whole- and Partial-Body Cryostimulation/Cryotherapy: Current Technologies and Practical Applications. J. Therm. Biol. 2016, 61, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Algafly, A.A.; George, K.P. The Effect of Cryotherapy on Nerve Conduction Velocity, Pain Threshold and Pain Tolerance. Br. J. Sports Med. 2007, 41, 365–369. [Google Scholar] [CrossRef]
- White, G.E.; Wells, G.D. Cold-Water Immersion and Other Forms of Cryotherapy: Physiological Changes Potentially Affecting Recovery from High-Intensity Exercise. Extreme Physiol. Med. 2013, 2, 26. [Google Scholar] [CrossRef] [Green Version]
- Kellogg, D.L. In Vivo Mechanisms of Cutaneous Vasodilation and Vasoconstriction in Humans during Thermoregulatory Challenges. J. Appl. Physiol. 2006, 100, 1709–1718. [Google Scholar] [CrossRef]
- Louis, J.; Theurot, D.; Filliard, J.-R.; Volondat, M.; Dugué, B.; Dupuy, O. The Use of Whole-Body Cryotherapy: Time- and Dose-Response Investigation on Circulating Blood Catecholamines and Heart Rate Variability. Eur. J. Appl. Physiol. 2020, 120, 1733–1743. [Google Scholar] [CrossRef]
- Dugué, B.; Bernard, J.P.; Bouzigon, R.; De Nardi, M.; Douzi, W.; Feirreira, J.J. Whole Body Cryotherapy/Cryostimulation, 39th Informatory Note on Refrigeration Technologies. Available online: https://iifiir.org/en/fridoc/whole-body-cryotherapy-cryostimulation-39-lt-sup-gt-th-lt-sup-gt-informatory-142805 (accessed on 20 January 2022).
- Ziemann, E.; Olek, R.A.; Kujach, S.; Grzywacz, T.; Antosiewicz, J.; Garsztka, T.; Laskowski, R. Five-Day Whole-Body Cryostimulation, Blood Inflammatory Markers, and Performance in High-Ranking Professional Tennis Players. J. Athl. Train. 2012, 47, 664–672. [Google Scholar] [CrossRef]
- Lange, U.; Uhlemann, C.; Müller-Ladner, U. Serial whole-body cryotherapy in the criostream for inflammatory rheumatic diseases. A pilot study. Med. Klin. Munich Ger. 1983 2008, 103, 383–388. [Google Scholar] [CrossRef]
- Banfi, G.; Melegati, G.; Barassi, A.; Dogliotti, G.; Melzi d’Eril, G.; Dugué, B.; Corsi, M.M. Effects of Whole-Body Cryotherapy on Serum Mediators of Inflammation and Serum Muscle Enzymes in Athletes. J. Therm. Biol. 2009, 34, 55–59. [Google Scholar] [CrossRef]
- Lubkowska, A.; Szyguła, Z.; Chlubek, D.; Banfi, G. The Effect of Prolonged Whole-Body Cryostimulation Treatment with Different Amounts of Sessions on Chosen pro- and Anti-Inflammatory Cytokines Levels in Healthy Men. Scand. J. Clin. Lab. Investig. 2011, 71, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Lubkowska, A.; Szygula, Z.; Klimek, A.J.; Torii, M. Do Sessions of Cryostimulation Have Influence on White Blood Cell Count, Level of IL6 and Total Oxidative and Antioxidative Status in Healthy Men? Eur. J. Appl. Physiol. 2010, 109, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Pournot, H.; Bieuzen, F.; Louis, J.; Fillard, J.-R.; Barbiche, E.; Hausswirth, C. Time-Course of Changes in Inflammatory Response after Whole-Body Cryotherapy Multi Exposures Following Severe Exercise. PLoS ONE 2011, 6, e22748. [Google Scholar] [CrossRef]
- Lubkowska, A.; Dołęgowska, B.; Szyguła, Z. Whole-Body Cryostimulation—Potential Beneficial Treatment for Improving Antioxidant Capacity in Healthy Men—Significance of the Number of Sessions. PLoS ONE 2012, 7, e46352. [Google Scholar] [CrossRef] [Green Version]
- Wojciak, G.; Szymura, J.; Szygula, Z.; Gradek, J.; Wiecek, M. The Effect of Repeated Whole-Body Cryotherapy on Sirt1 and Sirt3 Concentrations and Oxidative Status in Older and Young Men Performing Different Levels of Physical Activity. Antioxidants 2021, 10, 37. [Google Scholar] [CrossRef]
- Lubkowska, A.; Dudzińska, W.; Bryczkowska, I.; Dołęgowska, B. Body Composition, Lipid Profile, Adipokine Concentration, and Antioxidant Capacity Changes during Interventions to Treat Overweight with Exercise Programme and Whole-Body Cryostimulation. Oxid. Med. Cell. Longev. 2015, 2015, 803197. [Google Scholar] [CrossRef]
- Stanek, A.; Cholewka, A.; Gadula, J.; Drzazga, Z.; Sieron, A.; Sieron-Stoltny, K. Can Whole-Body Cryotherapy with Subsequent Kinesiotherapy Procedures in Closed Type Cryogenic Chamber Improve BASDAI, BASFI, and Some Spine Mobility Parameters and Decrease Pain Intensity in Patients with Ankylosing Spondylitis? BioMed Res. Int. 2015, 2015, 404259. [Google Scholar] [CrossRef] [Green Version]
- Banfi, G.; Lombardi, G.; Colombini, A.; Melegati, G. Whole-Body Cryotherapy in Athletes. Sports Med. Auckl. NZ 2010, 40, 509–517. [Google Scholar] [CrossRef]
- Lubkowska, A.; Chudecka, M.; Klimek, A.; Szyguła, Z.; Frączek, B. Acute Effect of a Single Whole-Body Cryostimulation on Prooxidant–Antioxidant Balance in Blood of Healthy, Young Men. J. Therm. Biol. 2008, 8, 464–467. [Google Scholar] [CrossRef]
- Lombardi, G.; Ziemann, E.; Banfi, G. Whole-Body Cryotherapy in Athletes: From Therapy to Stimulation. An Updated Review of the Literature. Front. Physiol. 2017, 8, 258. [Google Scholar] [CrossRef] [Green Version]
- Berk, M.; Williams, L.J.; Jacka, F.L.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So Depression Is an Inflammatory Disease, but Where Does the Inflammation Come from?|BMC Medicine|Full Text. Available online: https://0-bmcmedicine-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/1741-7015-11-200 (accessed on 7 March 2022).
- Veltri, A.; Scarpellini, P.; Piccinni, A.; Conversano, C.; Giacomelli, C.; Bombardieri, S.; Bazzichi, L.; Dell’Osso, L. Methodological Approach to Depressive Symptoms in Fibromyalgia Patients. Clin. Exp. Rheumatol. 2012, 30, 136–142. [Google Scholar]
- Ouzzani, M. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viljoen, C.T.; Rensburg, D.C.J.V.; Verhagen, E.; Mechelen, W.V. Epidemiology of Injury and Illness Among Trail Runners: A Systematic Review. Sports Med. 2021, 51, 917–943. [Google Scholar] [CrossRef] [PubMed]
- Marchand, S. Mechanisms Challenges of the Pain Phenomenon. Front. Pain Res. 2021, 1, 574370. [Google Scholar] [CrossRef]
- Yam, M.F.; Loh, Y.C.; Tan, C.S.; Khadijah Adam, S.; Abdul Manan, N.; Basir, R. General Pathways of Pain Sensation and the Major Neurotransmitters Involved in Pain Regulation. Int. J. Mol. Sci. 2018, 19, 2164. [Google Scholar] [CrossRef] [Green Version]
- Dubin, A.E.; Patapoutian, A. Nociceptors: The Sensors of the Pain Pathway. J. Clin. Investig. 2010, 120, 3760–3772. [Google Scholar] [CrossRef] [Green Version]
- Latremoliere, A.; Woolf, C.J. Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [Green Version]
- Staud, R. Peripheral Pain Mechanisms in Chronic Widespread Pain. Best Pract. Res. Clin. Rheumatol. 2011, 25, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Littlejohn, G.; Guymer, E. Neurogenic Inflammation in Fibromyalgia. Semin. Immunopathol. 2018, 40, 291–300. [Google Scholar] [CrossRef]
- Hung, A.L.; Lim, M.; Doshi, T.L. Targeting Cytokines for Treatment of Neuropathic Pain. Scand. J. Pain 2017, 17, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Vanderwall, A.G.; Milligan, E.D. Cytokines in Pain: Harnessing Endogenous Anti-Inflammatory Signaling for Improved Pain Management. Front. Immunol. 2019, 10, 3009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uçeyler, N.; Häuser, W.; Sommer, C. Systematic Review with Meta-Analysis: Cytokines in Fibromyalgia Syndrome. BMC Musculoskelet. Disord. 2011, 12, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Review process flow diagram.


{kind=link}
Table 1.
Quality assessment of the included original articles (Downs & Black quality analysis tool). Abstracts are excluded from the assessment.
Table 1.
Quality assessment of the included original articles (Downs & Black quality analysis tool). Abstracts are excluded from the assessment.
| Author | Year | Reporting | External Validity | Internal Validity | Power | Score | Comment | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Items | 1 | 2 | 3 | 6 | 7 | 9 | 10 | 11 | 12 | 16 | 17 | 18 | 20 | 26 | 27 | total | ||
| Metzger D. et al. | 2000 | 1 | 0 | 1 | 1 | 0 * | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 11/15 | * Item 7: no SD was reported for all population data description, and no estimates of variability (interquartile range of results and standard error and standard deviation and confidence intervals) were reported |
| Kurzeja R. et al. | 2003 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9/15 | |
| Bettoni L. et al. | 2013 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 10/15 | |
| Rivera J. et al. | 2018 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 13/15 | |
| Vitenet M. et al. | 2018 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 * | 1 | 0 | 10/15 | * Item 20: the outcome measures were clearly described but the control group protocol was not explained in detail so we cannot consider it valid and reliable. |
| Klemm P. et al. | 2021 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 14/15 | |
Table 2.
Summary of included studies characteristics.
| Author, Date, Country | Study Design | Experimental Population (n) | Subgroups (n, Sex) | Mean Age ± SD (Year) | WBC Exposures (n) and Protocol | Sampling Time (Measurement, Surveys) |
|---|---|---|---|---|---|---|
| Metzger D et al., 2000, Germany | Non-controlled study (Prospective observational study) | 1º FM (49), RA (21), CLBP (20), AS (13), OA (11), 2º FM (4) and AD (2). Tot. 120 (90 F/30 M) | no control group | 52.6 ± 8.9 | 6 days/weeks/twice a day for 4 weeks (48 total): −105 °C (avg 2.5 min) 2–3 patients per chamber per session | On the 1st day, then twice a week and on the last day, i.e., eight times in total |
| Kurzeja R. et al., 2003, Germany | Non-randomized controlled study (Prospective observational study) | 1º FM (66, 61 F/5 M, 2 drop-outs) | WBC (38 tot, 20 drop-outs) WT (mud bath + hot air) (28) | 50, 35–65 (WBC) 53, 35–64 (mud bath + hot air) (SD n.r.) | Once/day for 3 to 4 weeks (not clear the exact number of sessions): adaptation of 1/2 to 1 min @ −40 °C, −110 °C (avg 2 min) | After 1st, 7th, and last session |
| Drynda S. et al., 2013, Germany | Randomized-controlled trial study (Abstract only) | FM (10 tot, 9 F/1 M) | Baseline (before WBC) and post-WBC (after WBC) | 48.7 ± 9.8 | 3 sessions/3 consecutive days (3 tot): adaptation of 10 s @ −10 °C, 10 s @ −60 °C; max 3 min @ −110 °C | Blood was collected immediately prior to (baseline) and directly after the first exposure to WBC and after the third exposure |
| Bettoni L. et al., 2012, Italy | Randomized-controlled trial study (Abstract only) | FM (98, 91 F/7 M) based on ACR criteria and Wolfe criteria | WBC (49, 46 F; 3 M) treated with antioxidants agents and analgesic CTR (49, 45 F; 4 M) treated only antioxidants agents and analgesic | WBC (37.7, SD n.r.) CTR (39.2, SD n.r.) | 5 times/week for 3 weeks (tot 15 sessions): adaptation of −60 °C for 1 min, 2 min @ −140 °C. WBC group: 30 min of rehabilitation after WBC | Beginning of four weeks and after the end of the cycle of WBC: VAS pain and Fatigue questionnaire (FSS) |
| Bettoni L. et al., 2013, Italy | Non-randomized controlled study (Clinical Qualitative study) | FM (100, 94 F/6 M) | WBC+ (46 F/4 M) WBC− (46 F/4 M) | WBC+ 17–67 WBC− 19–70 (SD n.r.) | 15 sessions (5 week for 3 weeks): adaptation of 30 s @ −60 °C and 3 min @ −140 °C WBC+ group: 30 min of aerobic exercise after WBC | At recruitment and following (or not) to WBC |
| Drynda S. et al., 2015, Germany | Non-controlled study (Experimental Research/Abstra−ct only) | FM (22, 20 F/2 M) | WBC (22) | 51.7 ± 8.9 | 3 sessions/3 consecutive days: adaptation of 10 s @ −10 °C, 10 s @ −60 °C for max 3 min @ −110 °C | Blood collected at baseline (prior the start, immediately after 1st exposure, and after 3rd exposure) |
| Meenakshi Sundaram V. et al., 2015, India | Randomized experimental study (Abstract only) | FM (40, 24 F/16 M) | A (20, were randomly allotted): Steam Therapy and Functional Rehabilitation B (20): WBC and Functional Rehabilitation) | 20–40 (SD n.r.) | n.r. | Visual Analogue Scale, SF-36, Health Questionnaire, Epworth sleepiness scale, and Fatigue and Severity Scale on the 1st day and the 14th day |
| Rivera J. et al., 2018, Spain | Randomized crossover clinical study | FM (60, F/M n.r.) | A (34, 1 drop out) B (26) group inversion after Period 1 → intervention group (WBC) and CTR Period 1 (3 weeks), Washout (1 week), Period 2 (3 weeks) | 25–80 (SD n.r.) | 15 sessions/alternate days for 3 weeks: adaptation of 30 s @ −60 °C, 3 min @ −196 °C Protocol: 10 sessions +1 week Washout +10 sessions (group inversion) | After 22 and 50 days from period start—visits 3 and 6, corresponding to the evaluation of the first and second periods, respectively |
| Vitenet M. et al., 2018, Belgium | Randomized controlled study | FM (24, 20 F/4 M) | WBC (11, 8 F; 3 M) CTR (13, 12 F; 1 M) | 55 ± 10 (WBC) 50 ± 11 (CTR) | 10 sessions/8 days (1 sessions/day for the first 4 and last 2 days, 2 sessions/day for days 5 and 6): 3 min @ −110 °C | Just before the first treatment and 1 month following the end of the last intervention |
| Klemm P. et al., 2021, Germany | Non-randomized controlled study | 89 patients screened: 32 excluded, 57 enrolled (38 F/19 M) FM (26) Healthy CTR (31) | WBC (26) CTR (31) | 46 ± 9.8 | 2 sessions/week for 3 weeks (6 sessions tot) 1st session: 90 s @ −130° 2nd sessions: 2 min @ −130° From the 3rd session onwards: 3 min @ −130° | Outcomes were measured after 3 and 6 sessions, and 3 months of discontinued therapy (follow-up). |
Table 3.
Summary of included Studies Outcomes and Results.
| Author, Date, Country | Subgroups | Outcomes and Assessment | Results |
|---|---|---|---|
| Metzger D et al., 2000, Germany | no control group | Pain Intensity: 10-item numerical rating scale Well-being: 5-item verbal rating scale Effectiveness and importance of WBC: 4-level verbal rating scales Rewarming time Duration of pain relief (hrs) Duration of stay in the chamber | ↓ Pain Intensity (constant during 4-weeks) (p = 0.000); ↓ Pain Intensity afternoon vs. morning between the different treatment periods: Beginning (p = 0.001), middle (p = 0.007) and end (p = 0.01) of the four-week treatment); ↓ Pain Intensity immediately after WBC (p = 0.000); = duration of pain relief during 4-weeks follow-up; = rewarming time; ↑ Well-being (p = 0.000); ↑ stay in chamber from middle of treatment onwards (p = 0.000); ↑ stay in cryochamber afternoon vs. morning in week 1, 2 (p = 0.000). |
| Kurzeja R. et al., 2003, Germany | WBC WT (mud bath + hot air) | Pain, general conditions, vegetative and functional: Patient self-assessment (PSE) Pain Intensity: VAS Number of painful tender points Duration of pain relief (hrs) | WBC vs. WT: ↓ VAS in WBC & WT (p < 0.01); ↑ PSEWBC > ↑ PSEWT (p < 0.01); ↓ TPWBC > ↓ TPCTR in middle and end of discharge (p < 0.01); Avg duration of pain relief after WBC = 2 h 45 min |
| Drynda S. et al., 2013, Germany | Baseline (before WBC) post-WBC (after WBC) | Pain Intensity: VAS Transcriptome analyses (gene expression): Affymetrix GeneChip® Human Gene 1.0 ST arrays | ↓ VAS 90 out of 33.297 transcripts: >1.2 fold up-regulation < 1.2 fold down-regulation vs. baseline (72 down-regulated, 18 up-regulated, 34 changed after 1st session); up-regulated genes: PBX1, SFRP2, MAP2K3, and SLC25A39; down-regulated genes: SNORD p-value n.r. |
| Bettoni L. et al., 2012, Italy | WBC (antioxidants andanalgesics) CTR(antioxidants and analgesics) | Pain Intensity: VAS Fatigue: fatigue score Blood pressure Heart rate Oxygen saturation Axillary temperature | WBC vs. CTR: ↓ VASWBC > ↓ VASCTR (p < 0.05) ↓ FatigueWBC > ↓ FatigueCTR = blood pressure, heart rate, oxygen saturation, axillary temperature (p < 0.05) |
| Bettoni L. et al., 2013, Italy | WBC+ WBC− | Pain: VAS Physical and Mental health: SF-36 Global Health Status: VAS-GH Fatigue: FSS | WBC+ vs. WBC−: ↓ VASWBC+ > ↓ VASWBC−−(p < 0.0001); ↑ (SF)-36WBC+ > ↑ (SF)-36WBC− (p < 0.0001) ↑ (SF)-36 in WBC− (for almost of all the (SF)-36 items) (p < 0.05, p < 0.01, p < 0.0001) ↓ VAS-GHWBC+ > ↓ VAS-GHWBC− (p < 0.0001) ↓ FSSWBC+ > ↓ FSSWBC− (p < 0.0001) |
| Drynda S. et al., 2015, Germany | WBC | Gene expression: Real-Time PCR (TaqMan) | ↓ CCL4 (−67%) in 19 out of 22 Ps ↓ CD69 (−59%) in 16 out of 22 Ps 13 patients: ↑ mRNA MAP2K3 (+180%); 9 patients: = mRNA MAP2K3 p-value n.r. |
| Meenakshi Sundaram V. et al., 2015, India | A: Steam Therapy and Functional Rehabilitation) B: WBC and Functional Rehabilitation) | Pain: VAS Sleep disturbances: Epworth sleepiness scale Fatigue: FSS Health: SF-36 | B vs. A: ↓ Pain-B > ↓ Pain-A ↓ Fatigue-B > ↓ Fatigue-A ↓ Sleep disturbances-B > ↓ Sleep disturbances-A ↑ SF-36-B > ↑ SF-36-A p-value n.r. |
| Rivera J. et al., 2018, Spain | Group A Group B → Groups inverted after Period 1: WBC and CTR Period 1 (3 weeks), Washout (1 week), Period 2 (3 weeks) | Pain: VAS Impact of disease: FIQ Severity of disease: ICAF Physical and Mental health: (SF)-36 | WBC vs. CTR first period (V1–V3): ∆VASWBC > ∆VASCTR (p < 0.0001) ∆FIQWBC > ∆FIQCTR (p < 0.0001) ∆ICAFWBC scores > ∆ICAFCTR scores (all p < 0.0001) SF-36WBC physical function > SF-36CTR physical function (p < 0.0001) SF-36WBC emotional function > SF-36CTR emotional function (p < 0.0002) Linear regression confirmed significance independently of baseline values: VAS (β = 2.56); FIQ (β = 29.7); ICAF (β = 12.8) Period 2 VAS (p = 0.015) and FIQ (p = 0.003) of period 1 did not return to baseline → washout period too short |
| Vitenet M. et al., 2018, Belgium | WBC CTR | Health-reported quality of life (physical and mental) MOS SF-36-physical (PCS) MOS SF-36-mental (MCS) | WBC vs. CTR: ↑ PCSWBC > ↑ PCSCTR (p = 0.017) ↑ MCS WBC > ↑ MCSCTR (p = 0.017) |
| Klemm P. et al., 2021, Germany | WBC CTR | Pain intensity: VAS Disease activity: FIQ Cytokine levels: ELISA | FM after 3 WBC sessions vs. FM baseline: ↓ VAS (p = 0.0016); MCIDFM for VAS not achieved; ↓ IL-1 (p = 0.0001); ↓ IL-6 (p = 0.0028); ↓ IL-10 (p = 0.0014); =TNF-α (p = 0.1320); FM after 6 WBC sessions vs. FM baseline: ↓ VAS(p < 0.0001); MCID for VAS achieved; ↓ FIQ (p = 0.0006); ↓IL-1 (p = 0.0001); ↓ IL-6 (p = 0.0038); = IL-10 (p = 0.0735); = TNF-α (p = 0.5950) FM after 3 month of last WBC sessions vs. FM baseline: ↑ VAS (p = 0.0037); = FIQ (p = 0.2142); MCID for FIQ not achieved; ↓ IL-1 (p < 0.0001); ↓ IL-6 (p < 0.0088); ↑ IL-10 (p = 0.0008); =TNF-α (p = 0.4100) CTR after 3 WBC sessions vs. CTR baseline: = IL-1 (p = 0.2429); =IL-6 (p = 0.4247); =IL-10 (0.2053); =TNF-α (p = 0.3943) CTR after 6 WBC sessions vs. CTR baseline: = IL-1 (p = 0.1080); =IL-6 (p = 0.1279); =IL-10 (0.1092); =TNF-α (p = 0.5647) CTR after 3 month of last WBC sessions vs. CTR baseline: ↓ IL-1 (p = 0.0021); =IL-6 (p = 0.7883); =IL-10 (p = 0.1154); =TNF-α (p = 0.7716) FM vs. CTR at baseline: IL-1FM > IL-1CTR (p < 0.0001); IL-6FM > IL-6CTR (p < 0.0017); IL-10FM > IL-10CTR (p < 0.0001); TNF-α FM = TNF-αCTR (p = 0.1240); FM vs. CTR after 3 WBC sessions: IL-1FM > IL-1CTR (p < 0.0001) IL-6FM > IL-6CTR (p < 0.0023); IL-10FM = IL-10CTR (p = 0.6581); TNF-α FM >TNF-αCTR (p = 0.0009); FM vs. CTR after 6 WBC sessions: IL-1FM < IL-1CTR (p < 0.0403); IL-6FM > IL-6CTR (p < 0.0077); IL-10FM > IL-10CTR (p < 0.0059); TNF-α FM = TNF-αCTR (p = 0.0167); FM vs. CTR after 3 months from last WBC sessions: IL-1FM > IL-1CTR (p < 0.0086); IL-6FM > IL-6CTR (p < 0.0231); IL-10FM > IL-10CTR (p < 0.0001); TNF-α FM = TNF-αCTR (p = 0.0699); |
↑ Increase; ↓ decrease; = no changes.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Fontana, J.M.; Gobbi, M.; Piterà, P.; Giusti, E.M.; Capodaglio, P. Whole-Body Cryostimulation in Fibromyalgia: A Scoping Review. Appl. Sci. 2022, 12, 4794. https://0-doi-org.brum.beds.ac.uk/10.3390/app12094794
AMA Style
Fontana JM, Gobbi M, Piterà P, Giusti EM, Capodaglio P. Whole-Body Cryostimulation in Fibromyalgia: A Scoping Review. Applied Sciences. 2022; 12(9):4794. https://0-doi-org.brum.beds.ac.uk/10.3390/app12094794
Chicago/Turabian StyleFontana, Jacopo Maria, Michele Gobbi, Paolo Piterà, Emanuele Maria Giusti, and Paolo Capodaglio. 2022. "Whole-Body Cryostimulation in Fibromyalgia: A Scoping Review" Applied Sciences 12, no. 9: 4794. https://0-doi-org.brum.beds.ac.uk/10.3390/app12094794
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.