
SoundFields: A Virtual Reality Home-Based Intervention for Auditory Hypersensitivity Experienced by Autistic Children
 , , , and
, , , and
Abstract
:1. Introduction
1.1. Potential Cause of Sound Hypersensitivity for Autistic People
1.2. Treatment
1.3. This Study
2. Materials and Methods
2.1. Game Description
2.1.1. Mini-Game 1: Orb Hunt
2.1.2. Mini-Game 2: Bubble Rescue
2.1.3. Mini-Game 3: Simon Says
2.1.4. Mini-Game 4: Ghost Hunt
2.2. Participants
2.3. Ethical Considerations
2.4. Intervention Protocol
2.5. Equipment
2.6. Outcome Measures
2.6.1. Self-Reported Emotional Response
2.6.2. Tracked Interactions (In-Game)
2.6.3. Qualitative Questionnaire
3. Results
3.1. Quantitative Findings
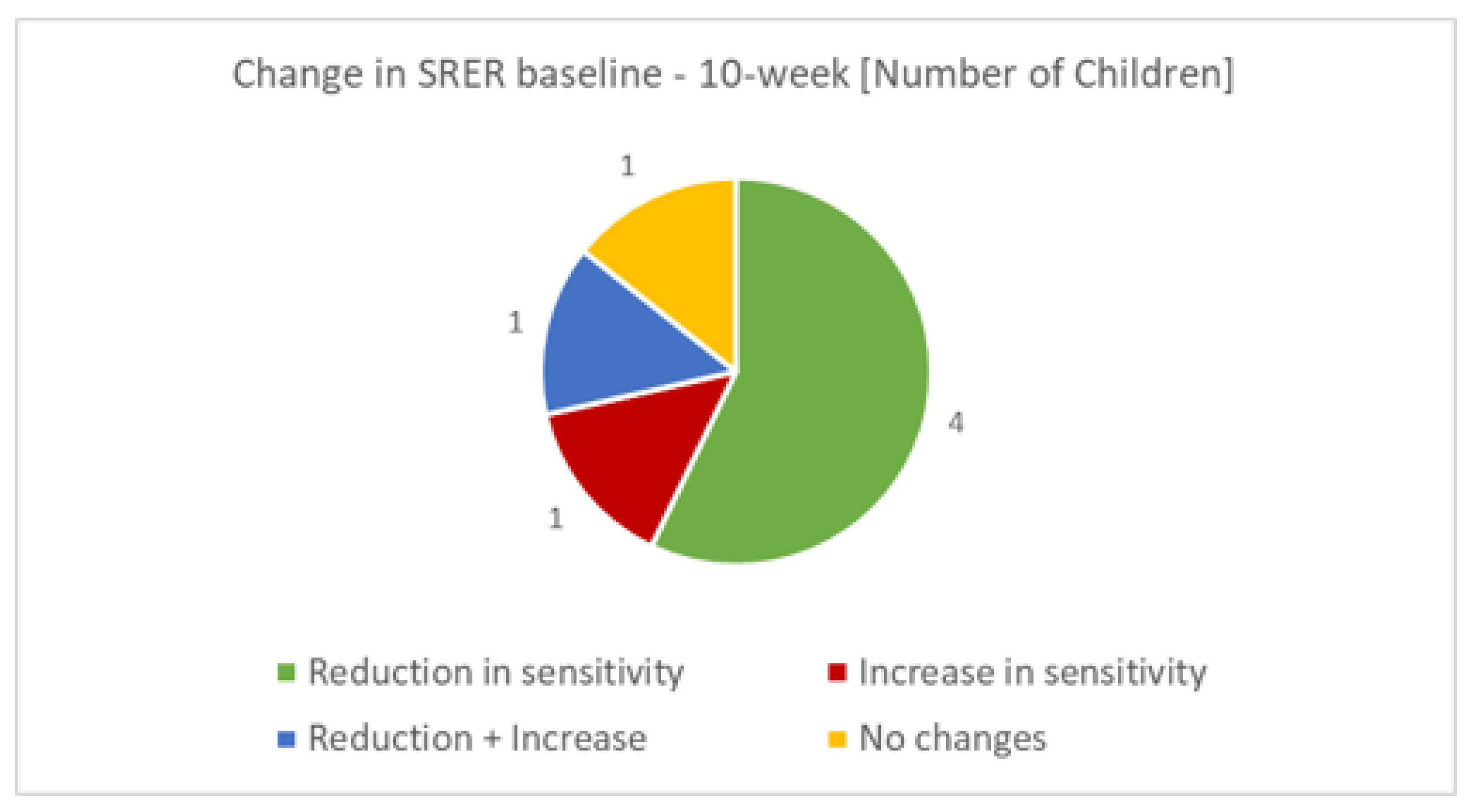
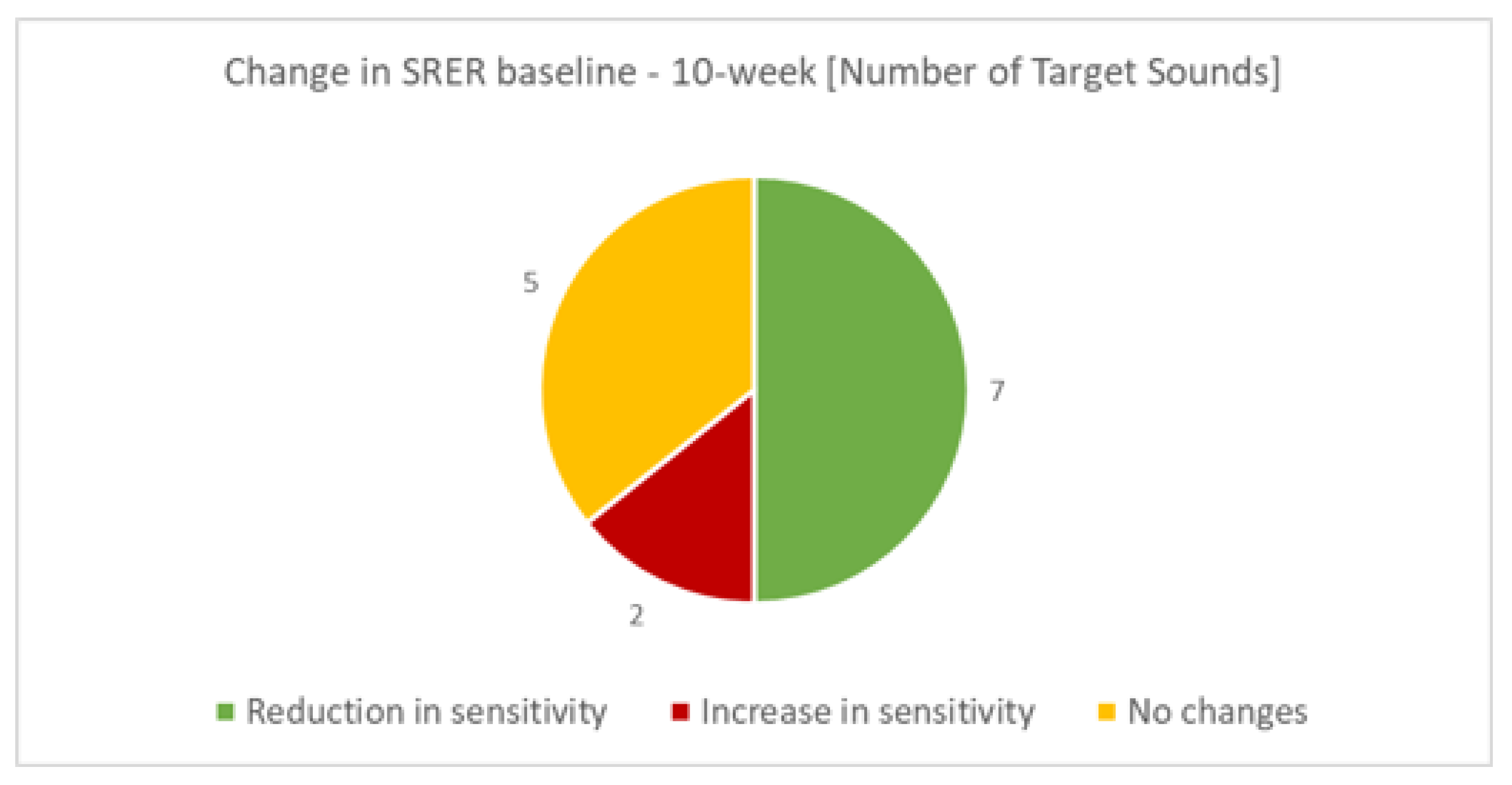
3.1.1. Self-Reported Emotional Response
3.1.2. Tracked Interactions (In-Game)
3.1.3. Qualitative Findings
‘I feel a bit better, but I don’t usually hear those things’(Participant 3).
‘He doesn’t seem to be as worried in some situations, seems more chilled out. Has gone into town no problem which has previously been hard. Doesn’t seem to be complaining about school as much but could be to do with new teacher.’(Parent 1).
‘He seems calmer after playing.’(Parent 8).
‘I knew what to do so didn’t need any other instructions’(Participant 2).
‘The game was intuitive, didn’t read the instructions.’(Parent 2).
‘I chose the alarm. The music was playing over the top, so it was bearable. The music that played over the top was nice.’(Participant 9).
‘I didn’t like Simon says, I found it a bit difficult. I was fine until it started doing the double thing. I liked how the points worked.’(Participant 9).
‘He found it hard to keep attention for so long so we broke it up into smaller times’.(Parent 8)
‘Gave (NAME) a headache could be to do with her glasses, was uncomfortable with glasses on.’(Parent 3).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR); American Psychiatric Pub.: Washington, DC, USA, 2022. [Google Scholar]
- Bury, S.M.; Jellett, R.; Spoor, J.R.; Hedley, D. “It defines who I am” or “It’s something I have”: What language do [autistic] Australian adults [on the autism spectrum] prefer? J. Autism Dev. Disord. 2023, 53, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.E.; Baron-Cohen, S. Sensory perception in autism. Nat. Rev. Neurosci. 2017, 18, 671–684. [Google Scholar] [CrossRef]
- Baranek, G.T.; Boyd, B.A.; Poe, M.D.; David, F.J.; Watson, L.R. Hyperresponsive sensory patterns in young children with autism, developmental delay, and typical development. Am. J. Ment. Retard. 2007, 112, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Baranek, G.T.; Watson, L.R.; Boyd, B.A.; Poe, M.D.; David, F.J.; McGuire, L. Hyporesponsiveness to social and nonsocial sensory stimuli in children with autism, children with developmental delays, and typically developing children. Dev. Psychopathol. 2013, 25, 307–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, E.K.; Hanley, M.; Riby, D.M. Distraction, distress and diversity: Exploring the impact of sensory processing differences on learning and school life for pupils with autism spectrum disorders. Res. Autism Spectr. Disord. 2020, 72, 101515. [Google Scholar] [CrossRef]
- Serafini, G.; Gonda, X.; Canepa, G.; Pompili, M.; Rihmer, Z.; Amore, M.; Engel-Yeger, B. Extreme sensory processing patterns show a complex association with depression, and impulsivity, alexithymia, and hopelessness. J. Affect. Disord. 2017, 210, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Williams, Z.J.; Suzman, E.; Woynaroski, T.G. Prevalence of decreased sound tolerance (hyperacusis) in individuals with autism spectrum disorder: A meta-analysis. Ear Hear. 2021, 42, 1137–1150. [Google Scholar] [CrossRef]
- Birkett, L.; McGrath, L.; Tucker, I. Muting, filtering and transforming space: Autistic children’s sensory ‘tactics’ for navigating mainstream school space following transition to secondary school. Emot. Space Soc. 2022, 42, 100872. [Google Scholar] [CrossRef]
- Stefanelli, A.C.G.F.; Zanchetta, S.; Furtado, E.F. Auditory hyper-responsiveness in autism spectrum disorder, terminologies and physiological mechanisms involved: Systematic review. In CoDAS; SciELO: São Paulo, Brasil, 2020; Volume 32. [Google Scholar]
- Department for Education. Special Educational Needs in England: January 2019; Department for Education: London, UK, 2019.
- Morewood, G.D.; Humphrey, N.; Symes, W. Mainstreaming autism: Making it work. Good Autism Pract. (GAP) 2011, 12, 62–68. [Google Scholar]
- Bauminger, N.; Kasari, C. Loneliness and friendship in high-functioning children with autism. Child Dev. 2000, 71, 447–456. [Google Scholar] [CrossRef]
- Demopoulos, C.; Lewine, J.D. Audiometric profiles in autism spectrum disorders: Does subclinical hearing loss impact communication? Autism Res. 2016, 9, 107–120. [Google Scholar] [CrossRef] [Green Version]
- Steigner, J.; Ruhlin, S.U. Systematic Desensitization of Hyperacusis and Vocal Pitch Disorder Treatment in a Patient with Autism. Internet J. Allied Health Sci. Pract. 2014, 12, 6. [Google Scholar] [CrossRef]
- Tyler, R.S.; Pienkowski, M.; Roncancio, E.R.; Jun, H.J.; Brozoski, T.; Dauman, N.; Coelho, C.B.; Andersson, G.; Keiner, A.J.; Cacace, A.T.; et al. A review of hyperacusis and future directions: Part I. Definitions and manifestations. Am. J. Audiol. 2014, 23, 402–419. [Google Scholar] [CrossRef] [Green Version]
- Radziwon, K.E.; Manohar, S.; Auerbach, B.; Liu, X.; Chen, G.D.; Salvi, R. Preclinical animal behavioral models of hyperacusis and loudness recruitment. In New Therapies to Prevent or Cure Auditory Disorders; Springer: Cham, Switzerland, 2020; pp. 135–157. [Google Scholar]
- Lucker, J.R. Auditory hypersensitivity in children with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2013, 28, 184–191. [Google Scholar] [CrossRef]
- Lucker, J.R.; Doman, A. Neural mechanisms involved in hypersensitive hearing: Helping children with ASD who are overly sensitive to sounds. Autism Res. Treat. 2015, 2015, 369035. [Google Scholar] [CrossRef] [Green Version]
- Kirby, A.V.; Boyd, B.A.; Williams, K.L.; Faldowski, R.A.; Baranek, G.T. Sensory and repetitive behaviors among children with autism spectrum disorder at home. Autism 2017, 21, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Hasson, N.; Camilleri, B.; Jones, C.; Smith, J.; Dodd, B. Discriminating disorder from difference using dynamic assessment with bilingual children. Child Lang. Teach. Ther. 2013, 29, 57–75. [Google Scholar] [CrossRef]
- O’Donohue, W.T.; Fisher, J.E. Cognitive Behavior Therapy: Core Principles for Practice; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Silver, M.; Oakes, P. Evaluation of a new computer intervention to teach people with autism or Asperger syndrome to recognize and predict emotions in others. Autism 2001, 5, 299–316. [Google Scholar] [CrossRef]
- White, S.W.; Oswald, D.; Ollendick, T.; Scahill, L. Anxiety in children and adolescents with autism spectrum disorders. Clin. Psychol. Rev. 2009, 29, 216–229. [Google Scholar] [CrossRef] [Green Version]
- Ince, P.; Haddock, G.; Tai, S. A systematic review of the implementation of recommended psychological interventions for schizophrenia: Rates, barriers, and improvement strategies. Psychol. Psychother. Theory, Res. Pract. 2016, 89, 324–350. [Google Scholar] [CrossRef]
- Van Der Krieke, L.; Wunderink, L.; Emerencia, A.C.; De Jonge, P.; Sytema, S. E–mental health self-management for psychotic disorders: State of the art and future perspectives. Psychiatr. Serv. 2014, 65, 33–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farr, W.J.; Green, D.; Bremner, S.; Male, I.; Gage, H.; Bailey, S.; Speller, S.; Colville, V.; Jackson, M.; Memon, A.; et al. Feasibility of a randomised controlled trial to evaluate home-based virtual reality therapy in children with cerebral palsy. Disabil. Rehabil. 2021, 43, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Menear, K.S.; Ernest, J.M. Comparison of physical activity, TV/video watching/gaming, and usage of a portable electronic devices by children with and without autism spectrum disorder. Matern. Child Health J. 2020, 24, 1464–1472. [Google Scholar] [CrossRef]
- Zakari, H.M.; Poyade, M.; Simmons, D. Sinbad and the Magic Cure: A serious game for children with ASD and auditory hypersensitivity. In Games and Learning Alliance; Springer: Cham, Switzerland, 2017; pp. 54–63. [Google Scholar]
- Maskey, M.; Rodgers, J.; Grahame, V.; Glod, M.; Honey, E.; Kinnear, J.; Labus, M.; Milne, J.; Minos, D.; McConachie, H.; et al. A randomised controlled feasibility trial of immersive virtual reality treatment with cognitive behaviour therapy for specific phobias in young people with autism spectrum disorder. J. Autism Dev. Disord. 2019, 49, 1912–1927. [Google Scholar] [CrossRef] [Green Version]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J.R. Reducing specific phobia/fear in young people with autism spectrum disorders (ASDs) through a virtual reality environment intervention. PLoS ONE 2014, 9, e100374. [Google Scholar] [CrossRef] [Green Version]
- Hacihabiboglu, H.; De Sena, E.; Cvetkovic, Z.; Johnston, J.; Smith, J.O., III. Perceptual spatial audio recording, simulation, and rendering: An overview of spatial-audio techniques based on psychoacoustics. IEEE Signal Process. Mag. 2017, 34, 36–54. [Google Scholar] [CrossRef] [Green Version]
- Begault, D.R.; Trejo, L.J. 3-D Sound for Virtual Reality and Multimedia; NASA: Washington, DC, USA, 2000.
- Potisk, T. Head-related transfer function. In Seminar Ia; Faculty of Mathematics and Physics, University of Ljubljana: Ljubljana, Slovenia, 2015. [Google Scholar]
- Cheng, C.I.; Wakefield, G.H. Introduction to head-related transfer functions (HRTFs): Representations of HRTFs in time, frequency, and space. In Proceedings of the Audio Engineering Society Convention 107, New York, NY, USA, 24–27 September 1999. [Google Scholar]
- Hayes, S.T.; Adams, J.A. Device Motion via Head Tracking for Mobile Interaction. In Proceedings of the Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Gold Coast, Australia, 6–9 November 2016; SAGE Publications Sage: Los Angeles, CA, USA, 2016; Volume 60, pp. 774–778. [Google Scholar]
- Zotkin, D.N.; Duraiswami, R.; Davis, L.S. Rendering localized spatial audio in a virtual auditory space. IEEE Trans. Multimed. 2004, 6, 553–564. [Google Scholar] [CrossRef] [Green Version]
- Johnston, D.; Egermann, H.; Kearney, G. SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder. Appl. Sci. 2020, 10, 2996. [Google Scholar] [CrossRef]
- Johnston, D.; Egermann, H.; Kearney, G. The Use of Binaural Based Spatial Audio in the Reduction of Auditory Hypersensitivity in Autistic Young People. Int. J. Environ. Res. Public Health 2022, 19, 12474. [Google Scholar] [CrossRef]
- Whyte, E.M.; Smyth, J.M.; Scherf, K.S. Designing serious game interventions for individuals with autism. J. Autism Dev. Disord. 2015, 45, 3820–3831. [Google Scholar] [CrossRef]
- Kwon, J.; Lee, Y. Serious games for the job training of persons with developmental disabilities. Comput. Educ. 2016, 95, 328–339. [Google Scholar] [CrossRef]
- Green, M.C.; Murphy, D. EigenScape: A database of spatial acoustic scene recordings. Appl. Sci. 2017, 7, 1204. [Google Scholar] [CrossRef] [Green Version]
- Koegel, R.L.; Openden, D.; Koegel, L.K. A systematic desensitization paradigm to treat hypersensitivity to auditory stimuli in children with autism in family contexts. Res. Pract. Pers. Sev. Disabil. 2004, 29, 122–134. [Google Scholar] [CrossRef]
- Kuo, M.H.; Orsmond, G.I.; Cohn, E.S.; Coster, W.J. Friendship characteristics and activity patterns of adolescents with an autism spectrum disorder. Autism 2013, 17, 481–500. [Google Scholar] [CrossRef]
- Orsmond, G.I.; Kuo, H.Y. The daily lives of adolescents with an autism spectrum disorder: Discretionary time use and activity partners. Autism 2011, 15, 579–599. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposure Level | Virtual Distance between Player and Stimulus |
|---|---|
| 1 | 25 m |
| 2 | 15 m |
| 3 | 5 m |
| 4 | 2.5 m |
| Stimuli | Participant |
|---|---|
| Fire Alarm | P01, P02, P03, P09 |
| Children Fighting | P01 |
| Fireworks | P02, P03 |
| Hairdryer | P02, P03, P04, P05 |
| Car Engine | P04 |
| Baby Crying | P05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parkinson, S.; Schumann, S.; Taylor, A.; Fenton, C.; Kearney, G.; Garside, M.; Johnston, D. SoundFields: A Virtual Reality Home-Based Intervention for Auditory Hypersensitivity Experienced by Autistic Children. Appl. Sci. 2023, 13, 6783. https://0-doi-org.brum.beds.ac.uk/10.3390/app13116783
Parkinson S, Schumann S, Taylor A, Fenton C, Kearney G, Garside M, Johnston D. SoundFields: A Virtual Reality Home-Based Intervention for Auditory Hypersensitivity Experienced by Autistic Children. Applied Sciences. 2023; 13(11):6783. https://0-doi-org.brum.beds.ac.uk/10.3390/app13116783
Chicago/Turabian StyleParkinson, Sarah, Sophie Schumann, Amelia Taylor, Clare Fenton, Gavin Kearney, Megan Garside, and Daniel Johnston. 2023. "SoundFields: A Virtual Reality Home-Based Intervention for Auditory Hypersensitivity Experienced by Autistic Children" Applied Sciences 13, no. 11: 6783. https://0-doi-org.brum.beds.ac.uk/10.3390/app13116783