1. Introduction
Mandibular and maxillary bones can be an occurrence place for many cysts, tumors, and other pathologies related to odontogenic or non-odontogenic origins. The first description of KCOT (keratocystic odontogenic tumor, KOT, simple form; non-syndromic OKC) was noted by H. P. Philipsen in 1956. Over the years, the WHO (World Health Organization) nomenclature on KCOT/OKC has changed [
1,
2,
3]. Today, the KCOT is an unused term for OKC because of the 2017 WHO update (odontogenic keratocyst). Because of its cystic appearance, nowadays OKC has been classified as a cystic pathology with some degree of local aggressiveness. This rare benign cystic lesion has a potential of reoccurrence in time (30–60%) and requires some monitoring in routine radiographs. The posterior mandible (angle, body, and ramus, 60–80%) is the most common occurrence side, while the anterior maxilla is the rarest (5–10%) [
4,
5]. When present in the mandible, they often tend to grow in the buccolingual diameter, while in the maxillary bones they often grow towards the maxillary sinuses. When present, typical unilocular characteristics might mostly be found. In some cases, multiple OKC (3–10%, the syndromic OKC) are present within the jaw bones. In those particular cases, a basal cell nevus syndrome (nevoid basal cell carcinoma syndrome) should be considered (NNCCS, Gorlin–Goltz syndrome, GGS) [
6,
7]. The presence of NBCCS is associated with some genetic coincidence of the patched (PTCH) tumor-suppressor gene. This syndrome is related to the inherited autosomal dominant disorder, which was first described by Gorlin and Goltz in 1960 [
6,
7].
OKCs are most commonly found in the 2nd–3rd and 6th decade of life associated with impacted or not mandibular 3rd molar teeth. A slight male predominance is noted [
6,
7,
8,
9]. Its occurrence was related to the presence of dental lamina (odontogenic epithelium) in the alveolus margin in the mandible left from the stages of teeth development. The Serre’s remnants and epithelial cell rests (stratified squamous keratinizing epithelium) seem to be most related with OKC occurrence [
5,
6,
7,
8,
9,
10].
Because most OKCs grow asymptomatically, they are found accidentally on routine panoramic radiographs. OKC commonly tends to be a cystic or polycystic lesion with clear borders. Its size and shape may vary. On a routine panoramic radiograph (panx), OKC has a characteristic solitary, radiolucent, unilocular, well-defined, expansile lesion with smooth, corticated borders if no cortical expansion is present. It might often be associated with impacted or displaced teeth, mimicking a dentigerous cyst or eruption cyst. They can rarely appear and cause some resorption of tooth apexes or form some mineralized septa within the cyst cavity, which might create more aggressive behavior and mimic ameloblastoma. Cortical expansion is not common or characteristic of OKC but might be considered a radiological sign of local aggressiveness. Occasionally, OKC can be present as a cyst-like lesion, similar to a dentigerous cyst, while rarely it can be more of an expansile solitary unilocular characteristic. Their relationship with dental roots can differentiate from periapical cysts [
10,
11,
12,
13,
14]. Some reports describe cases when, during their growth, OKC displaces teeth towards the mandibular angle or within the maxillary sinus. On the other hand, CBCT (cone-beam computed tomography) findings might easily describe their borders and estimate their expansion towards the cortical bone, tooth radices, and close proximity to the IAN (inferior alveolar nerve). When OKC is expanded through the cortical borders a possible soft tissue involvement might be seen, which requires some additional surgical excision steps during surgery. When accidentally found on MR resolutions (magnetic resonance), they can manifest as a high signal (T1-keratin contents), heterogenous signal (T2), and DWI (keratin restrictions) [
9,
10,
11,
12,
13,
14,
15,
16,
17,
18].
Another situation is present when jaw asymmetry, swelling, teeth displacement, and pain might occur. Teeth resorption, cortical expansion, trismus (inflammation-based or mechanical obstacle presence, limited mouth opening (LMO)), and purulent fistulas are rare, however paresthesia (IAN, inferior alveolar nerve, Vincent sign) and pathological fractures are less likely to occur. Rarely, OKC might become infected, and an abscess might present in their proximity. In very rare situations, OKC (<0.5–1%) tends to transform into the PIOSCC—primary intraosseous squamous cell carcinoma (PIOC) [
14,
15,
16,
17,
18].
When a biopsy is scheduled, macroscopically, a very thin-walled cyst-like appearance, with either fluid formation or greyish debris matter similar to purulent fluid or cheese-like brown masses, might be found. Differential diagnosis should include dentigerous cysts, odontogenic cysts (pericoronal position), radicular cysts, ameloblastoma, odontogenic myxoma, adenomatoid odontogenic tumor, CGCG (central giant cell granuloma), impacted tooth/pericoronal impacted tooth lesions, SBC (Stafne bone cyst, bone defect), Gorlin–Goltz syndrome, and other syndromes like [
5,
6,
7,
8,
9,
10,
15,
16,
17,
18].
There are various treatment modifications that are often related to surgeons’ preferences, size and location of the lesion, and adjacency to other vital structures like IAN, mental foramen, and maxillary sinus. In the presented case report, the authors want to focus on the usage of allograft fresh–frozen materials used in bone reconstruction after OKC as preparation for the dental implant rehabilitation process.
2. Case Description
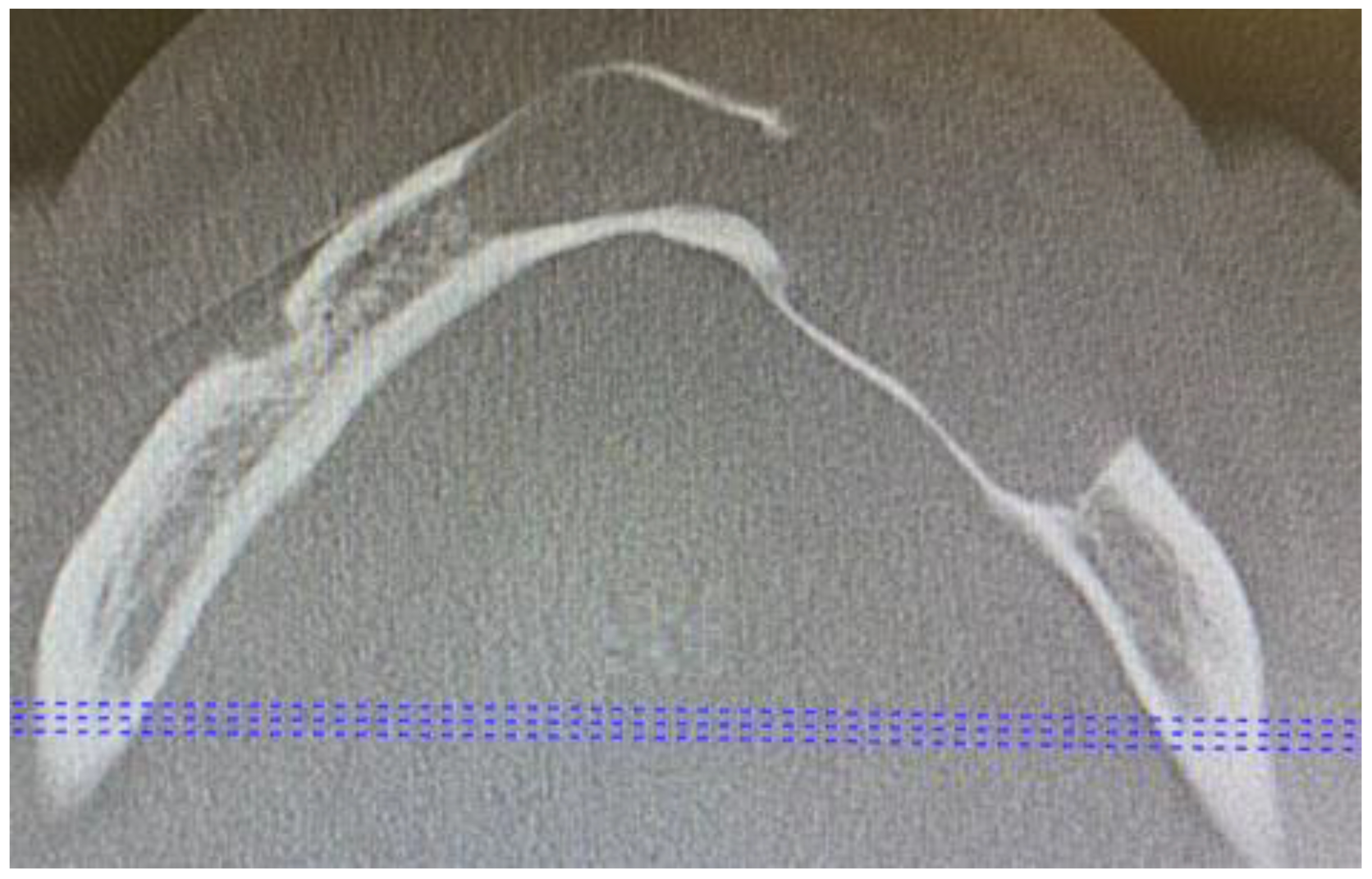
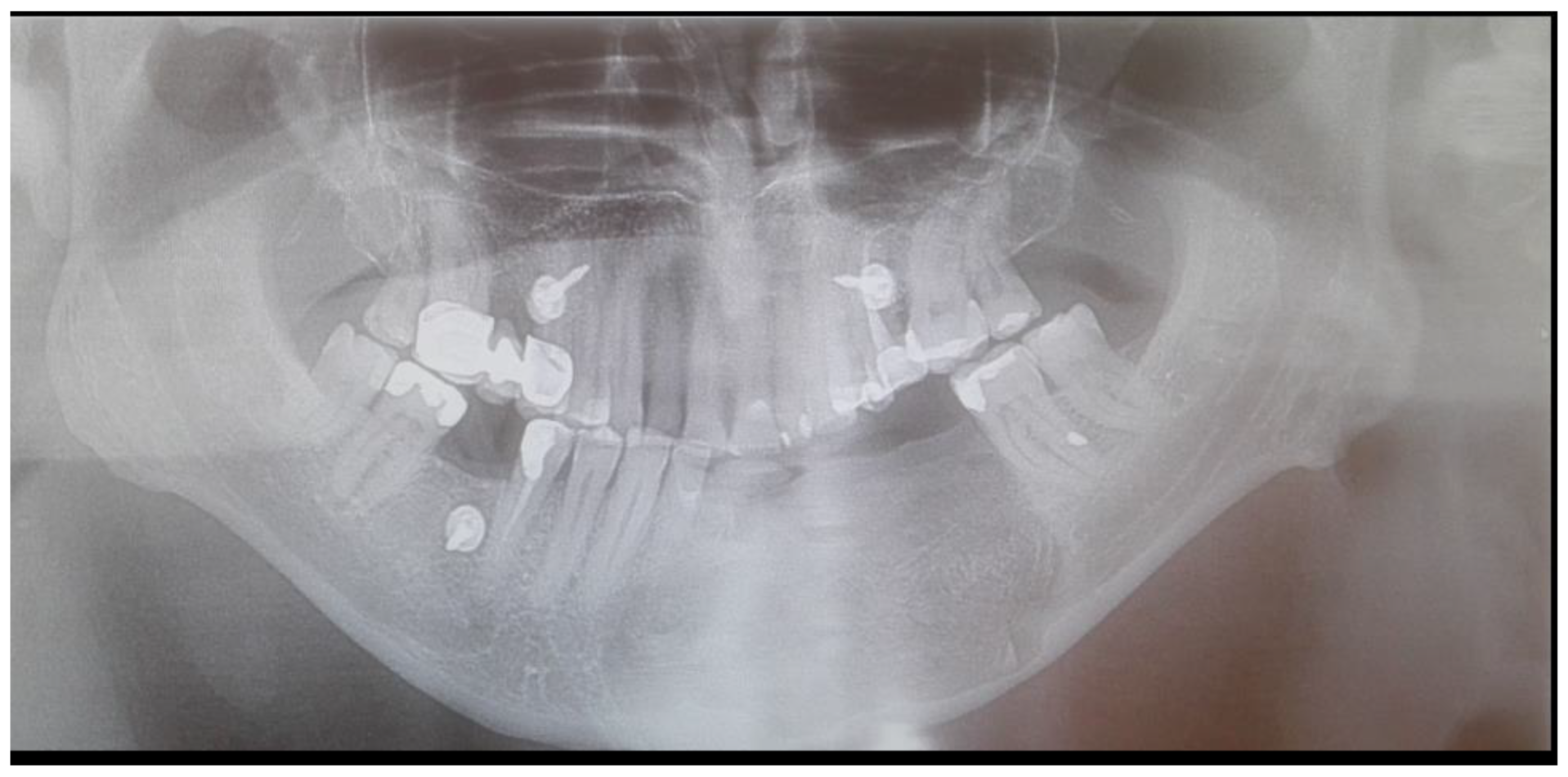
A 62-year-old Caucasian male was referred for consultation because of a cyst in the mandibular anterior and left body area associated with teeth mobility. The lesion was incidentally discovered by a dentist on a routine panoramic radiograph. On imaging, there was a polycystic lesion, quite big in diameter, with well-defined borders, visible inner cystic septa, and displaced 33,34,35 teeth. The cystic cavity ranged from tooth 43 towards 36, causing superior destruction of the alveolar ridge between teeth 33 and 34 and inferiorly spreading closely towards the inferior margin of the mandible. This expansive lesion was radiolucent with some septa with cortical buccal and alveolar ridge expansions (
Figure 1).
Further examination revealed extensive vestibular swelling ranging from teeth 32–35 and crepitation sign, followed by some elevation and fluctuation between teeth 33–34 (
Figure 2). The mucosa was unaffected, and tenderness on the palpation was not noted. However, teeth 31–35 mobility was noted. Teeth 34 and 35 were treated endodontically by a local dentist because of the cyst. Teeth 33–43 remained vital and responsive to cold stimuli. There were no neurological deficiencies related to either cranial nerves or the trigeminal (no Vincent sign) or facial nerves (no palsy). The intraoral photograph reveals good hygiene, with some visible swelling in the anterior portion of the mandible (
Figure 3 and
Figure 4).
Because some clinical characteristics suggested the presence of either OKC or ameloblastoma, a small diagnostic biopsy was performed at the top of the alveolar ridge between teeth 34–35 in local anesthesia to evaluate the type of lesion microscopically. At first, the 0.1% CHX (chlorhexidine gluconate) (Eludril, Pierre-Fabre Oral care, France) solution was used in the oral cavity The surrounding area was scrubbed with alcohol–ethanol 96% solution-AHD 1000 solution (MediLab, Lysoform, Germany) and protective sterile vaseline (Unilever, England). Lignocaine with Norepinephrine 2% (ampule, 2 mL, Polfa-Warszawa, Poland) was used for local anaesthesia. A standard No 15c B surgical blade (Swann Morton, WR Swann, Owlerton Grn, Hillsborough, Sheffield, England) was used for the modified sulcular incision between two malpositioned teeth 33–34, extending towards the dental sulcus. After elevating the mucosal flap with an elevator, a sample of cystic-like tissue with keratin mass was taken for microscopic evaluation. The wound was sutured with 3-0 interrupted vertical mattress sutures (Dafilon, B Braun, Aesculap AG Am Aesculap-Platz, Tuttlingen Germany). Histopathologic (HP) evaluating indicated OKC.
At the time of planning for surgical intervention, a few clinical problems arise: (1) If the cortical lingual plate and mandibular inferior border were solid, should GBR (guided bone regeneration procedure) be used? (2) Will there be a necessity for additional titanium microplate usage to decrease the risk of pathological fracture of the mandible? (3) How to achieve good healing and stable suture position in such a big bone defect? (4) Is the patient’s overall condition stable for general anesthesia (GA)? (5) What teeth should be extracted, and what teeth should be treated endodontically or left for observation? (6) Is the bone cavity of this big diameter good for xenograft material or should allo-/autograft bones be used? (7) How to ensure grafted bone stable position if the labial cortical plate is missing, along with the alveolar ridge? (8) What type of incision should be placed to fully visualize the cyst and tumor cavity and enable good suturing? (9) Are there any odontogenic infections (caries, periapical lesions, gingivitis, periodontitis, or others) that might influence final results from surgery? (10) How will the patient adapt to the new situation after the procedure? (11) If the patient decides on future dental implant rehabilitation, there is a necessity to improve the bone volume. After considering all of the following topics, a decision was made for GA with GBR. Before the patient was scheduled for oral hygienisation, a necessary evaluation for any active caries/periodontitis and secondary estimation of the vitality of anterior teeth in the mandible was scheduled.
The surgery took place under GA and nasotracheal intubation. Presurgical antibiotics included Kefzol 2g (Cefazolin, 1st class, Sandoz Poland, Warszawa, Poland) with 12 h prior to surgery Fraxyparine 5700 IU AXa/0.6 mL prophylaxis (low molecular weight heparin-LMWH) (Mylan, Viatris, Canonsburg, PA, USA). Similar to the biopsy, the 0.1% CHX (chlorhexidine gluconate) (Eludril, Pierre-Fabre Oral care, Paris, France) local solution was used. Additionally, the lips and skin surrounding the operating field were scrubbed with ProntOral (BRAUN, Hessen, Melsungen, Germany). Protective sterile Vaseline (Unilever, England) cream was applied to the lips. A local injection of mixed 0.25% solution that consisted of Marcaine-Adrenaline 0.5% (AspenPharma, Braine-l’Alleud, Belgium) with a mixture of Natrium Chlorate 0.9% (Natrium Chloratum 0.9% Fresenius KabiClear, Bad Homburg vor der Höhe, Germany) was used. Before the incision teeth, 41, 31–35 had been removed. Because of their stable position in the alveolar socket and their proper vitality, tooth 42 and tooth 43 were kept. A blade No 15c B (Swann Morton, WR Swann, Owlerton Grn, Hillsborough, Sheffield, England) was used for the incision. A modified gingival (envelope) incision through the sockets of removed teeth, followed by two oblique semi-vertical release incisions at the point of 42 and 36, descend far inferiorly from the mucogingival junction towards the alveolar mucosa. Full-thickness mucoperiosteal flaps were raised with Obwegeser Periosteal elevators (Obwegeser 38-630-06-07-38-630-11-07 17.5 cm/6 7/8”, KLS Martin, Tuttlingen, Germany) and Obwegeser Soft Tissue Retractor (Obwegeser 38-603-40-07, KLS Martin, Tuttlingen, Germany). The entire anterior and left portion of the mandible was exposed. A very thin labially expanded cortical bone with walls dehiscence because of a cyst spread outside of the bone was noted. The right mental nerve was exposed, while the left one was embedded into the lesion. The cystic cavity was filled with enormous amounts of keratin mass. An additional bacterial specimen was taken to investigate any possible bacteria present within the lesion. An additional lingual mucoperiosteal flap was raised to improve visualization of the entire cystic cavity. Bone debridement with curettage was performed. The left mental nerve was carefully separated from the cystic mass, along with the left IAN, and their continuity remained good. The additional ostectomy of the entire cavity was done with the usage of Lindeman burr and pear-shaped surgical burr (Aesculap AG, Tuttlingen, Germany). Because the inferior border of the mandible was intact (no pathological fracture as well), along with the lingual wall, there was no necessity for any additional titanium miniplate usage to improve bone stability. The part of the gingival mucosa covering the bone perforation was cut out. The entire bone defect was rinsed with NaCl 0.9% solution Natrium Chloratum 0.9% Fresenius KabiClear, Bad Homburg vor der Höhe, Germany). A secondary ostectomy was performed in the area near the separated nerves, the lingual plate, and within close proximity to the 36 and 42 teeth. The oral cavity was packed with sterile gauze 10 × 10 cm (KOMPRI lux S, Zarys Internationa Group, Zabrze, Poland). Following that, a mixture 1:20 solution consisting of Betadine (Braunol, povidonum iodinatum, BRAUN, Hessen, Melsungen, Germany) and -NaCl0.9% 80 mL (Natrium Chloratum 0.9% Fresenius KabiClear, Bad Homburg vor der Höhe, Germany) was used to rinse the defect ones again. After careful preparation of the field, 20 mL fresh–frozen bone (FFB) from the bone bank (RCKiK, Katowice, Poland) was first rinsed with 10 mL of NaCl 0.9%. After initial preparation, the bone was mixed with a total of 15 mL of patients’ blood drained intravenously. After the preparation of a “sticky bone” (allograft bone was crushed, cut into pieces, and carefully mixed with blood), the entire bone cavity was filled tightly with the FFB. On the superficial layer of the defect, a collagen resorbable dressing (Spongostan Standard, Ethicon, Somerville, NY, USA), along with two resorbable collagen membranes 30 × 40 mm (Jason R, Biotiss Bioematerials Dental, Straumann Group, Zossen, Germany), was sutured tightly to the superior part of the lingual flap and the far inferiorly placed (near the lower border of the mandible) labial flap with 4-0 Vicryl single sutures (Ethicon, Johnson & Johnson Medical N.V., Machelen, Belgium). Their role was to stabilize the graft with dressings. The second layer of sutures was sutured with 3-0 interrupted vertical mattress sutures (Dafilon, B Braun, Aesculap AG Am Aesculap-Platz, Tuttlingen, Germany). Furthermore, 3-0 Dafilon horizontal mattress sutures were placed around teeth 43 and 36 to tighten the edges. An additional continuous 5.0 Prolene (Polypropylene, Ethicon, Somerville, NY, USA) suture was placed on the entire length of the wound (
Figure 5). Because of the major amount of used FFB, a decision was made to use four IMF screws (intermaxillary fixation—Medartis, IMF Modus 2.0 Speed Tip Cortical Screws, Basel, Switzerland) (
Figure 6) for decreased mouth opening, decreased oral intake of food and drinks, and to ensure stable graft position for 14 days. Second to that, a nasogastric tube (Suction catheter, Zarys Internationa Group, Zabrze, Poland) was placed for 7 days. The left mandibular IMF screw, because of its fracture during a checkup, was removed, and the patient continued the fixation on elastic orthodontic wires (AO, American Orthodontics, Medium ½; Sheboygan, WI, USA).
The operating period went uneventfully. The patient continued intravenous antibiotics Taromentin (3 × 1.2 g, Polfa Tarchomin, Warszawa, Poland), Metronidazole (3 × 500 mg, Polpharma, Starogard Gdański, Poland), and NSAIDs: Ketonal (2 × 0.1 g, Sandoz Poland, Warszawa, Poland) with Paracetamolum Kabi (3 × 1 g, Fresenius Kabi, Warszawa, Poland) and Pyralgin (3 × 1 g, Metamisolum kalceks, Polpharma, Starogard Gdański, Poland). The patient was discharged home on the second day of post-surgery with a prescription to continue the same medication for 10 days. Oral hygiene was continued by rinsing the oral cavity with 0.1% CHX solution three times per day after its mixture with mineral water 1:7. Additional Elugel (Pierre-Fabre Oral care, Paris, France) and Solcoseryl dental adhesive paste (Meda, Berlin, Germany) were prescribed to be applied on the wound. The second irrigation of the oral cavity was related to the appliance of H202 (hydrogen peroxidation) to ensure enough plaque or debris-free sutures. Because of a slight sensation loss to the part of left lip, additional Nurovit 320 mg for two times a day was prescribed (1 table. Consists of: 100 mg wit. B1, 200 mg wit. B6, 0.2 mg wit. B12; 100 tabl.; G.L. Pharma, Gerot-Lannah, Wien, Austria).
The final HP examination revealed the presence of OKC. During routine check-ups the healing was good, the swelling was normal, and sutures were removed after 14 days. The follow-up examination was made four years after surgery. During the consultation, the clinical and radiological appearance of the bone and surrounding soft tissue was normal. Proper bone healing was achieved clinically and on routine CBCT (
Figure 7,
Figure 8 and
Figure 9). Four dental implants, Neodent 3.5/8 mm and 4.0/10 mm (Straumann Group, Arlington, TX, USA), were scheduled. The patient was supposed to be scheduled for FMT (full mouth therapy) and dental implant placement, however, because of the SARS-CoV-2 pandemic, the patient used partial acrylic removable dentures for over two years. By that time, the patient got used to the dentures and decided to reject the proposed further implant placement (
Figure 10,
Figure 11 and
Figure 12).
3. Discussion
The occurrence and presence of odontogenic keratocysts (OKCs) might vary. OKC are most commonly found in the mandible and are less commonly found in the maxillary bones. Because of their local aggressive behavior, many studies on treatment modalities and approaches have been reported. OKC nomenclature is constantly changing, ranging from a cyst (odontogenic keratocyst—OKC) to an odontogenic tumor (keratocystic odontogenic tumor-KCOT). Nowadays, its proper form is OKC, as their treatment is slightly less aggressive but still mostly related to its size, localization, spread towards the cortical bone, and infiltration towards soft tissues [
11,
12,
13,
14,
15]. While small bone defects might heal on their own, or sometimes require some guided bone regenerative techniques (GBR), larger ones might require a different approach. For bigger defects, it is advisable to restore bone integrity in one of the known possible methods, especially to gain faster bone healing, decrease possible pathological fracture occurrence, and improve adequate early dental implant rehabilitation.
A correlation with the shape and size of OKC influences the type of approach and any possible bone reconstruction used. Secondly, if OKC is in reoccurrence or extends from a cortical layer of the bone, a more radical approach is used. Surgical resection is rarely used, and is reserved for special cases [
15,
16,
17,
18]. There are many known treatment possibilities in OKC [
15,
16,
17,
18,
19,
20,
21,
22,
23]:
- -
surgical enucleation;
- -
marsupialization followed by enucleation;
- -
curettage after lesion removal;
- -
appliance of Carnoy’s solution fixative (it is a mixture of the following: ethanol, chloroform, and acetic acid) combined with excision and curettage;
- -
marsupialization, a two-step procedure to reduce the size of OKC then remove it;
- -
bone ostectomy after curettage and/or enucleation;
- -
simple excisional biopsy;
- -
enucleation and cryotherapy (physical method) or Carnoy solution (chemical method);
- -
application of 5FU (five-fluoro-uracyl) after enucleation;
- -
ostectomy with high-speed bone burrs after enucleation/curettage;
- -
bone resection (only for reoccurrence, large bone defects, and destructions; OKC was unresponsive to treatment);
- -
combination of methods.
After each procedure, a decision should be made on what to do with the bone cavity defect. Some authors advise that bone ostectomy improves local outcomes, while others prefer more conservative approaches. Both approaches do not yet have any consensus. Moreover, the type of surgical or conservative approach influences later possible GBR techniques if necessary. On the other hand, the type of keratinization in the OKCs walls influences its recurrence rate. Histopathological evaluation should include the type of ortho- or parakeratinzation within the cyst walls, which is also related to the scope of the radical procedure. Since local aggressiveness is known and reported widely, possible reoccurrence is related to the type of OKC, possible remnants of thin layered cyst membrane or some microcysts, and epithelial islands embedded onto the bone or cyst walls. When treated with chemical or physical methods, the cavity should be easily accessible for those substances so that all of the bony walls will be exposed to Carnoy solution or other substances [
20,
21,
22,
23]. Therefore, because of possible remnants of cysts within the bone cavity walls, a wide discussion focused on the best method for OKC removal. This removal is sometimes limited by some vital structures like IAN, the mental nerve, the maxillary sinus, or others [
18,
19,
20,
21,
22,
23]. Mohanty et al.’s study emphasizes that bone ostectomy has a good overall success rate [
21].
Despite the method used, each bone cavity can be healed by various methods. Small lesions can be left intact to heal on their own in time, based on blood clots, if the bone cavity is tightly sutured after closure. Bigger ones should be considered for treatment with various GBR techniques. Some limitations are related to no valuable bony walls or the inability to use some collagen membranes to support the bone grafts. Furthermore, any inflammation or purulent formation within the OKC should be carefully evaluated. This situation is most troublesome when the inflammation of grafted material occurs. Therefore, good cavity rinsing after OKC removal, followed by good patient hygiene after surgery, is very important. When the grafted material is placed in the cavity, a centrifuge is helpful to use the PRF or simply connect the bone fragments with the patient’s blood or NaCl. The scope of possibilities is surgeon-related, as is the size of OKC. Thus far, no direct guidelines for surgical approaches and reconstructive measures are known [
5,
6,
7,
8,
13,
14,
15,
16,
17,
18,
23].


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}











