
Heads Up! A Biomechanical Pilot Investigation of Soccer Heading Using Instrumented Mouthguards (iMGs)

Abstract
:1. Introduction
2. Materials and Methods
Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Header Kinematics by Header Type and Preceding Ball Delivery Method

{kind=link}
{kind=link}
{kind=link}
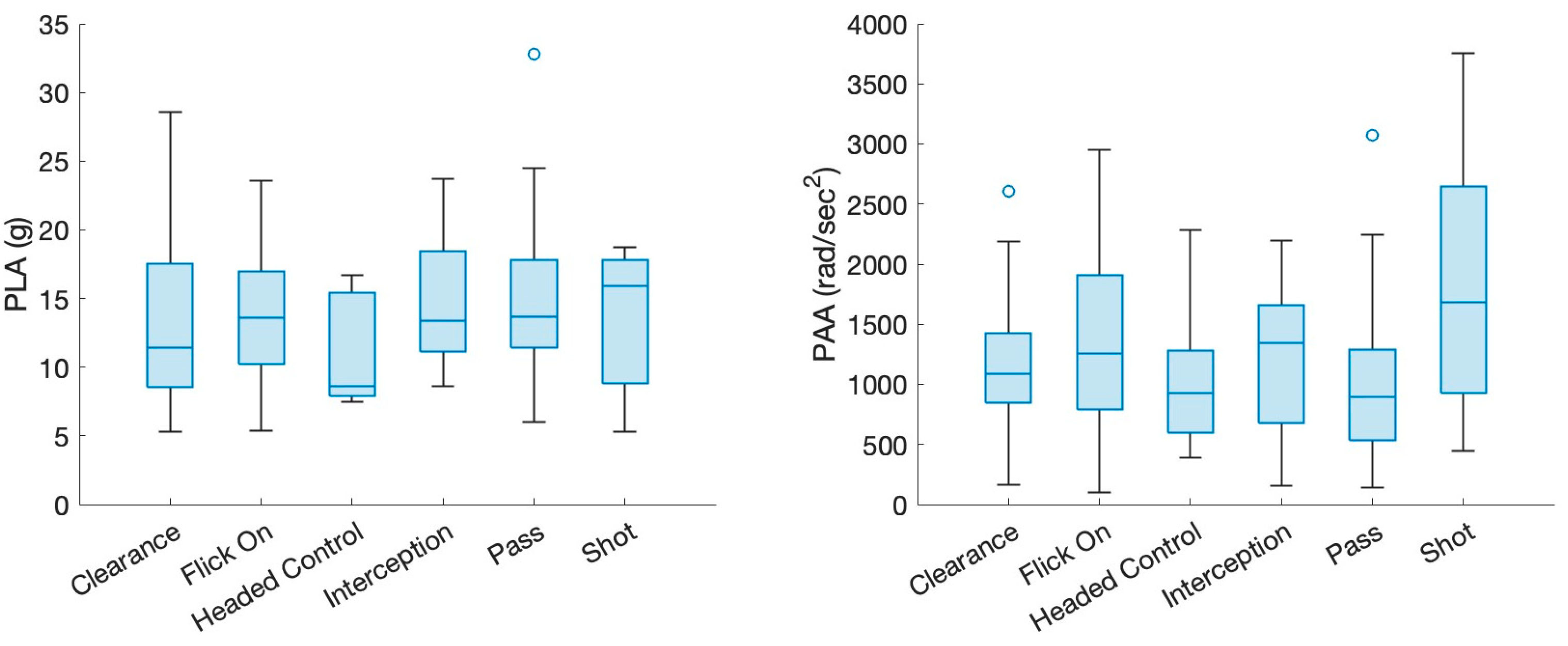
| N = 133 | PLA (g) | PAA [krad/s2] | |||
| Median | [Q1,Q3] | Median | [Q1,Q3] | ||
| Header Type | |||||
| Clearance | n = 24 | 11.4 | [8.4,17.6] | 1091.5 | [826.5,1459.5] |
| Flick-on | n = 30 | 13.6 | [10.0,17.1] | 1255 | [775.8,1925.3] |
| Headed Control | n = 5 | 8.6 | [7.8,15.9] | 930 | [529.0,1616.5] |
| Interception | n = 19 | 13.4 | [11.0,18.5] | 1349 | [675.0,1663.0] |
| Pass | n = 50 | 13.7 | [11.2,17.9] | 893.5 | [532.3,1342.8] |
| Shot | n = 5 | 15.9 | [7.7,18.1] | 1686 | [765.0,3013.5] |
| Ball Delivery Method | |||||
| Cross | n = 13 | 8.9 | [7,12.5] | 1165 | [275.0,1554.5] |
| Goal Kick | n = 18 | 15.85 | [12.08,21] | 1451.5 | [1018.5,2071.8] |
| Long Ball | n = 42 | 15.05 | [10.5,17.9] | 1002.5 | [718.3,1535.0] |
| Pass | n = 60 | 12.35 | [9.6,16.23] | 945.5 | [636.0,1368.0] |
References
- Kenny, R.; Elez, M.; Clansey, A.; Virji-Babul, N.; Wu, L.C. Head Impact Exposure and Biome-chanics in University Varsity Women’s Soccer. Ann. Biomed. Eng. 2022, 50, 1461–1472. [Google Scholar] [CrossRef]
- Kirkendall, D.T.; Jordan, S.E.; Garrett, W.E. Heading and Head Injuries in Soccer. Sports Med. 2001, 31, 369–386. [Google Scholar] [CrossRef]
- Armstrong, N.; Rotundo, M.; Aubrey, J.; Tarzi, C.; Cusimano, M.D. Characteristics of po-tential concussive events in three elite football tournaments. Inj. Prev. 2020, 26, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Cantu, R.C.; Mueller, F.O. Catastrophic football injuries: 1977–1998. Neurosurgery 2000, 47, 673–677. [Google Scholar]
- Agel, J.; Evans, T.A.; Dick, R.; Putukian, M.; Marshall, S.W. Descriptive Epidemiology of Collegiate Men’s Soccer Injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 Through 2002–2003. J. Athl. Train. 2007, 42, 270–277. [Google Scholar]
- Filben, T.M.; Pritchard, N.S.; Hanes-Romano, K.E.; Miller, L.E.; Miles, C.M.; Urban, J.E.; Stitzel, J.D. Comparison of women’s collegiate soccer header kinematics by play state, intent, and outcome. J. Biomech. 2021, 126, 110619. [Google Scholar] [CrossRef]
- Lamond, L.C.; Caccese, J.B.; Buckley, T.A.; Glutting, J.; Kaminski, T.W. Linear acceleration in direct head contact across impact type, player position, and playing scenario in collegiate women’s soccer players. J. Athl. Train. 2018, 53, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Broglio, S.P.; Lapointe, A.; O’Connor, K.L.; McCrea, M. Head Impact Density: A Model To Explain the Elusive Concussion Threshold. J. Neurotrauma 2017, 34, 2675–2683. [Google Scholar] [CrossRef]
- Zhao, W.; Bartsch, A.; Benzel, E.; Miele, V.; Stemper, B.D.; Ji, S. Regional brain injury vulnera-bility in football from two finite element models of the human head. In Proceedings of the IRCOBI Conference 2019, Florence, Italy, 11–13 September 2019; pp. 619–621. [Google Scholar]
- Barnes, B.C.; Cooper, L.; Kirkendall, D.T.; McDermott, T.P.; Jordan, B.D.; Garrett, W.E. Concussion History in Elite Male and Female Soccer Players. Am. J. Sports Med. 1998, 26, 433–438. [Google Scholar] [CrossRef]
- Covassin, T.; Swanik, C.B.; Sachs, M.L. Epidemiological Considerations of Concussions Among Intercollegiate Athletes. Appl. Neuropsychol. 2003, 10, 12–22. [Google Scholar] [CrossRef]
- Levy, M.L.; Kasasbeh, A.S.; Baird, L.C.; Amene, C.; Skeen, J.; Marshall, L. Concussions in Soccer: A Current Understanding. World Neurosurg. 2012, 78, 535–544. [Google Scholar] [CrossRef]
- Jordan, S.E.; Green, G.A.; Galanty, H.L.; Mandelbaum, B.R.; Jabour, B.A. Acute and Chronic Brain Injury in United States National Team Soccer Players. Am. J. Sports Med. 1996, 24, 205–210. [Google Scholar] [CrossRef]
- Reilly, T.R. Time motion studies of soccer. J. Hum. Mov. Stud. 1976, 2, 78–97. [Google Scholar]
- Tysvaer, A.; Storli, O. Association football injuries to the brain. A preliminary report. Br. J. Sport. Med. 1981, 15, 163–166. [Google Scholar] [CrossRef] [Green Version]
- Matser, J.T.; Kessels, A.; Jordan, B.D.; Lezak, M.D.; Troost, J. Chronic traumatic brain injury in professional soccer players. Neurology 1998, 51, 791–796. [Google Scholar] [CrossRef]
- Witol, A.D.; Webbe, F.M. Soccer heading frequency predicts neuropsychological deficits. Arch. Clin. Neuropsychol. 2003, 18, 397–417. [Google Scholar] [CrossRef] [Green Version]
- Matser, J.; Kessels, A.; Lezak, M.; Troost, J. A Dose-Response Relation of Headers and Concussions With Cognitive Impairment in Professional Soccer Players. J. Clin. Exp. Neuropsychol. 2001, 23, 770–774. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Marshall, S.; Broglio, S.P.; Cantu, R.C.; Kirkendall, D.T. No Evidence of Impaired Neurocognitive Performance in Collegiate Soccer Players. Am. J. Sports Med. 2002, 30, 157–162. [Google Scholar] [CrossRef]
- McCrory, P.R. Brain injury and heading in soccer. BMJ 2003, 327 (Suppl. S4), 0310351. [Google Scholar]
- Queen, R.M.; Weinhold, P.S.; Kirkendall, D.T.; Yu, B. Theoretical Study of the Effect of Ball Properties on Impact Force in Soccer Heading. Med. Sci. Sports Exerc. 2003, 35, 2069–2076. [Google Scholar] [CrossRef]
- Tierney, G. Concussion biomechanics, head acceleration exposure and brain injury criteria in sport: A review. Sports Biomech. 2022, 20, 1–29. [Google Scholar] [CrossRef]
- Tooby, J.; Weaving, D.; Al-Dawoud, M.; Tierney, G. Quantification of Head Acceleration Events in Rugby League: An Instrumented Mouthguard and Video Analysis Pilot Study. Sensors 2022, 22, 584. [Google Scholar] [CrossRef]
- Wu, L.C.; Nangia, V.; Bui, K.; Hammoor, B.; Kurt, M.; Hernandez, F.; Kuo, C.; Camarillo, D.B. In Vivo Evaluation of Wearable Head Impact Sensors. Ann. Biomed. Eng. 2016, 44, 1234–1245. [Google Scholar] [CrossRef] [Green Version]
- Kieffer, E.E.; Vaillancourt, C.; Brolinson, P.G.; Rowson, S. Using in-mouth sensors to measure head kinematics in rugby. In Proceedings of the IRCOBI Conference, Munich, Germany, 2020; Volume 13, pp. 846–858. [Google Scholar]
- Tysvaer, A.T.; Storli, O.V.; Bachen, N.I. Soccer injuries to the brain. A neurologic and electroencephalographic study of former players. Acta Neurol. Scand. 1989, 80, 151–156. [Google Scholar] [CrossRef]
- Naunheim, R.S.; Standeven, J.; Richter, C.; Lewis, L.M. Comparison of impact data in hockey, football, and soccer. J. Trauma Acute Care Surg. 2000, 48, 938–941. [Google Scholar] [CrossRef]
- Football and Dementia—Are Footballers Being Protected Enough against the Risks of Brain Injury?” Stewarts. Available online: https://www.stewartslaw.com/news/football-and-dementia-are-players-getting-enough-protection-against-the-risks-of-brain-injury/ (accessed on 23 September 2022).
- Tierney, G.J.; Kuo, C.; Wu, L.; Weaving, D.; Camarillo, D. Analysis of head acceleration events in collegiate-level American football: A combination of qualitative video analysis and in-vivo head kinematic measurement. J. Biomech. 2020, 110, 109969. [Google Scholar] [CrossRef]
- McHugh, M.L. Lessons in biostatistics. Biochem. Med. 2009, 19, 120–126. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Rich, A.M.; Filben, T.M.; Miller, L.E.; Tomblin, B.T.; Van Gorkom, A.R.; Hurst, M.A.; Barnard, R.T.; Kohn, D.S.; Urban, J.E.; Stitzel, J.D. Development, Validation and Pilot Field Deployment of a Custom Mouthpiece for Head Impact Measurement. Ann. Biomed. Eng. 2019, 47, 2109–2121. [Google Scholar] [CrossRef]
- Liu, Y.; Domel, A.G.; Yousefsani, S.A.; Kondic, J.; Grant, G.; Zeineh, M.; Camarillo, D.B. Validation and Comparison of Instrumented Mouthguards for Measuring Head Kinematics and Assessing Brain Deformation in Football Impacts. Ann. Biomed. Eng. 2020, 48, 2580–2598. [Google Scholar] [CrossRef]
- Kieffer, E.E.; Begonia, M.T.; Tyson, A.M.; Rowson, S. A Two-Phased Approach to Quantifying Head Impact Sensor Accuracy: In-Laboratory and On-Field Assessments. Ann. Biomed. Eng. 2020, 48, 2613–2625. [Google Scholar] [CrossRef]
- Jones, B.; Tooby, J.; Weaving, D.; Till, K.; Owen, C.; Begonia, M.; Stokes, K.A.; Rowson, S.; Phillips, G.; Hendricks, S.; et al. Ready for impact? A validity and feasibility study of instrumented mouthguards (iMGs). Br. J. Sports Med. 2022, 56, 1171–1179. [Google Scholar] [CrossRef]
- Caccese, J.B.; Lamond, L.C.; Buckley, T.A.; Kaminski, T.W. Reducing purposeful headers from goal kicks and punts may reduce cumulative exposure to head acceleration. Res. Sports Med. 2016, 24, 407–415. [Google Scholar] [CrossRef]
- Harriss, A.; Johnson, A.M.; Walton, D.M.; Dickey, J.P. Head impact magnitudes that occur from purposeful soccer heading depend on the game scenario and head impact location. Musculoskelet. Sci. Pract. 2019, 40, 53–57. [Google Scholar] [CrossRef]
- Cobb, B.R.; Urban, J.E.; Davenport, E.M.; Rowson, S.; Duma, S.M.; Maldjian, J.; Whitlow, C.T.; Powers, A.K.; Stitzel, J.D. Head Impact Exposure in Youth Football: Elementary School Ages 9–12 Years and the Effect of Practice Structure. Ann. Biomed. Eng. 2013, 41, 2463–2473. [Google Scholar] [CrossRef] [Green Version]
- Tierney, G.J.; Power, J.; Simms, C. Force experienced by the head during heading is influenced more by speed than the mechanical properties of the football. Scand. J. Med. Sci. Sports 2021, 31, 124–131. [Google Scholar] [CrossRef]
- Tierney, G.J.; Higgins, B. The incidence and mechanism of heading in European professional football players over three seasons. Scand. J. Med. Sci. Sports 2021, 31, 875–883. [Google Scholar] [CrossRef]
- Tierney, G.J.; Simms, C. Predictive capacity of the MADYMO multibody human body model applied to head kinematics during rugby union tackles. Appl. Sci. 2019, 9, 726. [Google Scholar] [CrossRef] [Green Version]
- IFAB.COM. Clarification: LAW 16, the GOAL KICK. 2 August 2022. Available online: https://theifab.com/news/claricat-ion-law-16-the-goal-kick (accessed on 12 January 2022).
- Shibukawa, K.; Hoshikawa, Y. Decrease in aerial challenges after revision of goal kick rules in Japan Pro-fessional Soccer League: Explorative study of the possibility of a risk reduction for head injury, concussion, and brain damage by a rule revision. Sci. Med. Footb. 2022, 6, 1–6. [Google Scholar]
- Collet, C. The possession game? A comparative analysis of ball retention and team success in European and interna-tional football, 2007–2010. J. Sport. Sci. 2013, 31, 123–136. [Google Scholar] [CrossRef]
- Football Association. Updated Heading Guidance Announced for Youth Training Sessions; Football Association: London, UK, 2020. [Google Scholar]
- Lynall, R.C.; Clark, M.D.; Grand, E.E.; Stucker, J.C.; Littleton, A.C.; Aguilar, A.J.; Petschauer, M.A.; Teel, E.F.; Mihalik, J.P. Head Impact Biomechanics in Women’s College Soccer. Med. Sci. Sport. Exerc. 2016, 48, 1772–1778. [Google Scholar] [CrossRef]
- Nevins, D.; Hildenbrand, K.; Vasavada, A.; Kensrud, J.; Smith, L. In-Game Head Impact Exposure of Male and Female High School Soccer Players. Athl. Train. Sports Health Care 2019, 11, 174–182. [Google Scholar] [CrossRef]
- Hanlon, E.M.; Bir, C.A. Real-Time Head Acceleration Measurement in Girls’ Youth Soccer. Med. Sci. Sports Exerc. 2012, 44, 1102–1108. [Google Scholar] [CrossRef]
- Tierney, G.; Weaving, D.; Tooby, J.; Al-Dawoud, M.; Hendricks, S.; Phillips, G.; Stokes, K.A.; Till, K.; Jones, B. Quantifying head acceleration exposure via instrumented mouthguards (iMG): A validity and fea-sibility study protocol to inform iMG suitability for the TaCKLE project. BMJ Open Sport Exerc. Med. 2021, 7, e001125. [Google Scholar] [CrossRef]
- Mackay, D.F.; Russell, E.R.; Stewart, K.; MacLean, J.A.; Pell, J.P.; Stewart, W. Neurodegenerative Disease Mortality among Former Professional Soccer Players. N. Engl. J. Med. 2019, 381, 1801–1808. [Google Scholar] [CrossRef]
- Kaminski, T.W.; Wikstrom, A.M.; Gutierrez, G.; Glutting, J.J. Purposeful heading during a season does not influence cognitive function or balance in female soccer players. J. Clin. Exp. Neuropsychol. 2007, 29, 742–751. [Google Scholar] [CrossRef]
- Wu, S.; Zhao, W.; Rowson, B.; Rowson, S.; Ji, S. A network-based response feature matrix as a brain injury metric. Biomech. Model. Mechanobiol. 2020, 19, 927–942. [Google Scholar] [CrossRef]
- Bian, K.; Mao, H. Mechanisms and variances of rotation-induced brain injury: A parametric investigation between head kinematics and brain strain. Biomech. Model. Mechanobiol. 2020, 19, 2323–2341. [Google Scholar] [CrossRef]
- Prosser, H. Perceptions, Attitudes, Self-Efficacy, and Behaviors of Mouthguard Use Among Collegiate Athletes; Minnesota State University: Mankato, MN, USA, 2020. [Google Scholar]
- Collins, C.L.; McKenzie, L.B.; Roberts, K.J.; Fields, S.K.; Comstock, R.D. Mouthguard BITES (Behavior, Impulsivity, Theory Evaluation Study): What Drives Mouthguard Use Among High School Basketball and Baseball/Softball Athletes. J. Prim. Prev. 2015, 36, 323–334. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Maeda, Y.; Yang, T.C.; Ando, T.; Tauchi, Y.; Miyanaga, H. Prevention of orofacial injury via the use of mouthguards among young male rugby players. Int. J. Sports Med. 2015, 36, 254–261. [Google Scholar] [CrossRef]
- Dursun, E.; Ilarslan, Y.D.; Ozgul, O.; Donmez, G. Prevalence of dental trauma and mouthguard awareness among weekend warrior soccer players. J. Oral Sci. 2015, 57, 191–194. [Google Scholar] [CrossRef] [Green Version]



| Pre-Head Contact | Head Contact |
|---|---|
Ball Delivery Method
| Header Type
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sokol-Randell, D.; Stelzer-Hiller, O.W.; Allan, D.; Tierney, G. Heads Up! A Biomechanical Pilot Investigation of Soccer Heading Using Instrumented Mouthguards (iMGs). Appl. Sci. 2023, 13, 2639. https://0-doi-org.brum.beds.ac.uk/10.3390/app13042639
Sokol-Randell D, Stelzer-Hiller OW, Allan D, Tierney G. Heads Up! A Biomechanical Pilot Investigation of Soccer Heading Using Instrumented Mouthguards (iMGs). Applied Sciences. 2023; 13(4):2639. https://0-doi-org.brum.beds.ac.uk/10.3390/app13042639
Chicago/Turabian StyleSokol-Randell, Darek, Oscar W. Stelzer-Hiller, David Allan, and Gregory Tierney. 2023. "Heads Up! A Biomechanical Pilot Investigation of Soccer Heading Using Instrumented Mouthguards (iMGs)" Applied Sciences 13, no. 4: 2639. https://0-doi-org.brum.beds.ac.uk/10.3390/app13042639