
Prognostic Value of Lymph Node Density in Lingual Squamous Cell Carcinoma

 , , , ,
, , , ,  , , , ,
, , , ,
Abstract
:1. Introduction
- −
- The regional spread of the disease (number of positive lymph nodes);
- −
- The surgical treatment (total number of nodes removed during surgery);
- −
- The accuracy of the histopathological analysis.
2. Materials and Methods
2.1. Population and Study Variables
- −
- Demographic variables: gender, age, stratified age, smoker, drinker;
- −
- Clinical variables: clinical size of the tumor, location of the tumor, diagnostic CT, diagnostic MRI, size and radiological DOI of the tumor, clinical staging, reconstruction, type of dissection, radiotherapy (RT) and postoperative chemotheraphy (QT);
- −
- Histological variables: degree of tumor differentiation, perineural invasion, lymphovascular invasion, TNM and pathological staging according to the 8th edition of the AJCC, LND, neck positivity, ENE and tumor budding;
- −
- Control variables: loco-regional recurrence, distant recurrence and mortality.
- Histological confirmation of the diagnosis of primary lingual squamous cell carcinoma;
- Patients operated on by the Oral and Maxillofacial Surgery Department at Gregorio Marañón General Hospital between 9 January 2016 and 9 January 2021;
- Patients for whom surgery was the treatment of choice and whose intervention consisted of tumor resection and associated cervical lymphadenectomy;
- Negative resection surgical margins for tumor involvement.
- Disease that exceeds the anterior 2/3 of the tongue (involvement of the base of the tongue);
- Patients previously treated for carcinoma of the oral cavity (surgery, radiotherapy or chemotherapy);
- Patients whose medical records did not identify the variables under study.
2.2. Data Analysis
3. Results
3.1. Descriptive Analysis of the Total Population and Population Subgroups According to the LND
- − Neck dissection (p-value 0.021);
- − Pathologic T (p-value 0.006);
- − Pathologic N (p-value < 0.001);
- − Perineural invasion (p-value 0.005);
- − Pathologic stage (p-value < 0.001).
3.2. Analysis of Primary Objective
3.3. Overall Survival (OS)
3.4. Disease-Free Survival (DFS)
3.5. Analysis of Secondary Objectives
3.6. Perineural Invasion
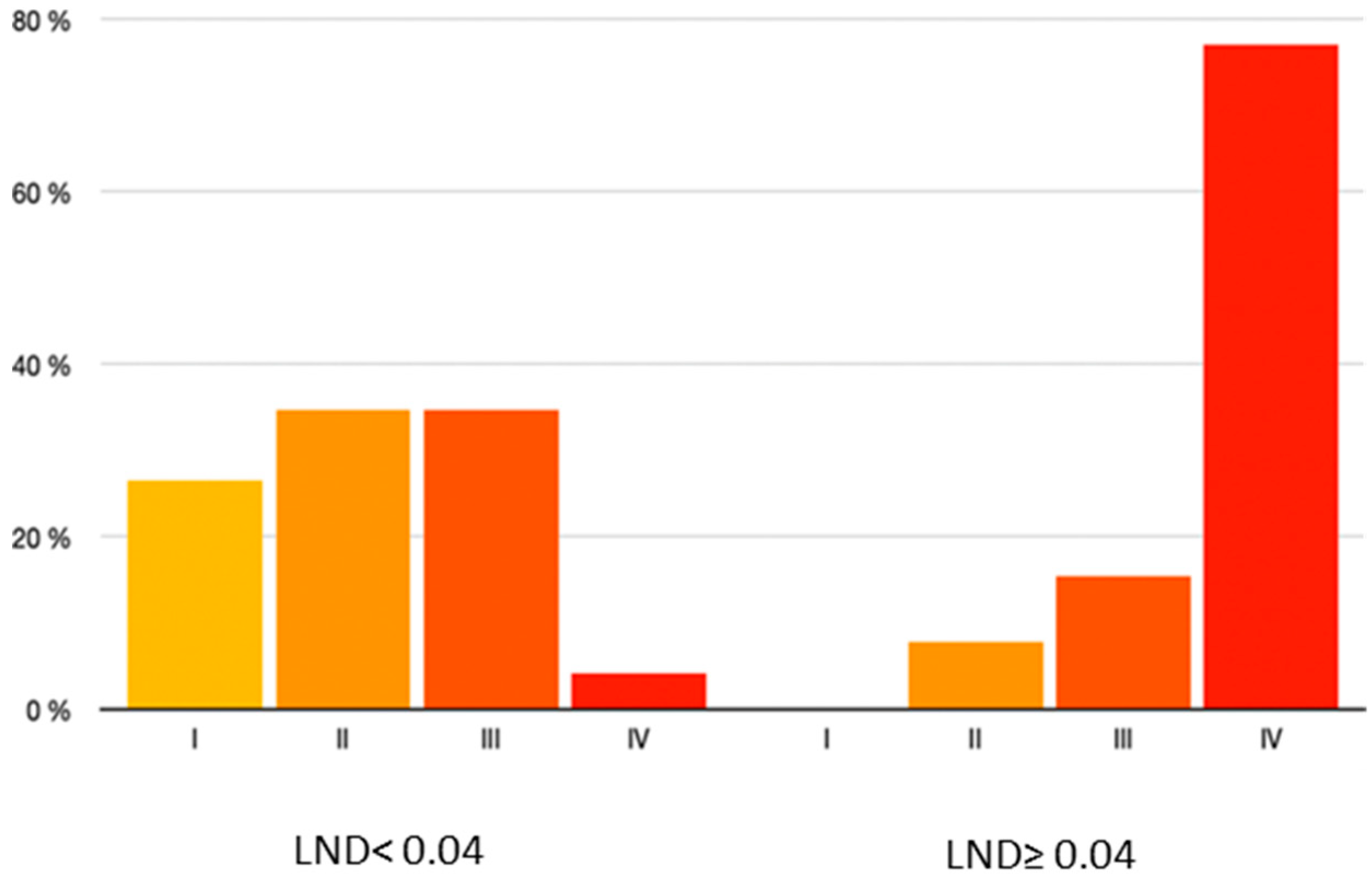
3.7. Pathologic Stage
4. Discussion
4.1. Significance and Practical Application of Results
4.2. Limitations of the Study
4.3. Relation to Similar Publications and Comparison between Terms of Agreement and Disagreement
4.4. Recommendations and Guidelines for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amin, M.B.; Edge, S.B.; Greee, F.L. AJCC Cancer Staging Manual; Springer: New York, NY, USA, 2018. [Google Scholar]
- Rudoltz, M.S.; Benammar, A.; Mohiuddin, M. Does pathologic node status affect local control in patients with carcinoma of the head and neck treated with radical surgery and postoperative radiotherapy? Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual: Head and Neck Cancers-Major 8th Edition Changes. CA Cancer J. Clin. Marzo De 2017, 67, 122–137. [Google Scholar] [CrossRef]
- Bernier, J.; Cooper, J.S.; Pajak, T.F.; van Glabbeke, M.; Bourhis, J.; Forastiere, A.; Ozsahin, E.M.; Jacobs, J.R.; Jassem, J.; Ang, K.K.; et al. Defi-ning risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (#9501). Head Neck Oct. De 2005, 27, 843–850. [Google Scholar]
- Parsons, J.T.; Mendenhall, W.M.; Stringer, S.P.; Cassisi, N.J.; Million, R.R. An analysis of factors influencing the outcome of postoperative irradiation for squamous cell carci-noma of the oral cavity. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Gavilán, J.; Prim, M.P.; De Diego, J.I.; Hardisson, D.; Pozuelo, A. Postoperative radiothe-rapy in patients with positive nodes after functional neck dissection. Ann. Otol. Rhinol. Laryngol. 2000, 109, 844–848. [Google Scholar] [CrossRef]
- Shingaki, S.; Takada, M.; Sasai, K.; Bibi, R.; Kobayashi, T.; Nomura, T.; Saito, C. Impact of lymph node metastasis on the pattern of failure and survival in oral carcinomas. Am. J. Surg. 2003, 185, 278–284. [Google Scholar] [CrossRef]
- Ghadjar, P.; Simcock, M.; Zimmermann, F.; Betz, M.; Bodis, S.; Bernier, J.; Studer, G.; Ae-bersold, D.M. Swiss Group for Clinical Cancer Research (SAKK). Predictors of severe late radiotherapy-related toxicity after hyperfractionated radiotherapy with or without concomitant cisplatin in locally advanced head and neck cancer. Secondary re-trospective analysis of a randomized phase III trial (SAKK 10/94). Radiother. Oncol. 2012, 104, 213–218. [Google Scholar] [CrossRef]
- Langendijk, J.A.; Doornaert, P.; Verdonck-de Leeuw, I.M.; Leemans, C.R.; Aaronson, N.K.; Slotman, B.J. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J. Clin. Oncol. 2008, 26, 3770–3776. [Google Scholar] [CrossRef]
- Mortensen, H.R.; Overgaard, J.; Specht, L.; Overgaard, M.; Johansen, J.; Evensen, J.F.; An-dersen, L.J.; Andersen, E.; Grau, C. Prevalence and peak incidence of acute and late normal tissue morbidity in the DAHANCA 6&7 randomised trial with accelerated radiotherapy for head and neck cancer. Radiother. Oncol. 2012, 103, 69–75. [Google Scholar] [CrossRef]
- Oskam, I.M.; Verdonck-de Leeuw, I.M.; Aaronson, N.K.; Kuik, D.J.; de Bree, R.; Doornaert, P.; Langendijk, J.A.; Leemans, C.R. Quality of life as predictor of survival: A prospective study on patients treated with combined surgery and radiotherapy for advanced oral and oropharyngeal cancer. Radiother. Oncol. 2010, 97, 258–262. [Google Scholar] [CrossRef]
- Patel, S.G.; Amit, M.; Yen, T.C.; Liao, C.T.; Chaturvedi, P.; Agarwal, J.P.; Kowalski, L.P.; Ebrahimi, A.; Clark, J.R.; Cernea, C.R.; et al. International Consortium for Outcome Research (ICOR) in Head and Neck Cancer. Lymph node density in oral cavity cancer: Results of the International Consortium for Outcomes Research. Br. J. Cancer 2013, 109, 2087–2095. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, N.; Balasubramanian, D.; Kumar, N.; Murthy, S.; Vijayan, S.N.; Nambiar, A.; Vidhyadharan, S.; Thankappan, K.; Iyer, S. Lymph node staging systems in oral squa-mous cell carcinoma: A comparative analysis. Oral. Oncol. 2019, 97, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Gil, Z.; Carlson, D.L.; Boyle, J.O.; Kraus, D.H.; Shah, J.P.; Shaha, A.R.; Singh, B.; Wong, R.J.; Patel, S.G. Lymph node density is a significant predictor of outcome in patients with oral cancer. Cancer 2009, 115, 5700–5710. [Google Scholar] [CrossRef]
- Stein, J.P.; Cai, J.; Groshen, S.; Skinner, D.G. Risk factors for patients with pelvic lymph node metastases following radical cystectomy with en bloc pelvic lymphadenectomy: Concept of lymph node density. J. Urol. 2003, 170, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Amar, A.; Rapoport, A.; Curioni, O.A.; Dedivitis, R.A.; Cernea, C.R.; Brandão, L.G. The den-sity of metastatic lymph node as prognostic factor in squamous cell carcinoma of the tongue and floor of the mouth. Braz. J. Otorhinolaryngol. 2012, 78, 86–90, (In English and Portuguese). [Google Scholar] [CrossRef] [PubMed]
- Spoerl, S.; Gerken, M.; Mamilos, A.; Fischer, R.; Wolf, S.; Nieberle, F.; Klingelhöffer, C.; Meier, J.K.; Spoerl, S.; Ettl, T.; et al. Lymph node ratio as a predictor for outcome in oral squamous cell carcinoma: A multicenter popu-lation-based cohort study. Clin. Oral. Investig. 2021, 25, 1705–1713. [Google Scholar] [CrossRef] [PubMed]
- Lieng, H.; Gebski, V.J.; Morgan, G.J.; Veness, M.J. Important prognostic significance of lymph node density in patients with node positive oral tongue cancer. ANZ J. Surg. 2016, 86, 681–686. [Google Scholar] [CrossRef]
- Moratin, J.; Metzger, K.; Kansy, K.; Ristow, O.; Engel, M.; Hoffmann, J.; Flechtenmacher, C.; Freier, K.; Freudlsperger, C.; Horn, D. The prognostic significance of the lymph node ratio in oral cancer differs for anatomical subsites. Int. J. Oral. Maxillofac. Surg. 2020, 49, 558–563. [Google Scholar] [CrossRef]
- Iftikhar, H.; Rozi, S.; Zahid, N.; Awan, M.S.; Nathani, K.R. Lymph node ratio as a prognos-tic marker of oral tongue squamous cell carcinoma: A cohort study. Ann. R. Coll. Surg. Engl. 2020, 102, 726–732. [Google Scholar] [CrossRef]
- Yamagata, K.; Fukuzawa, S.; Kanno, N.; Uchida, F.; Yanagawa, T.; Bukawa, H. Is Lymph Node Ratio a Prognostic Factor for Patients With Oral Squamous Cell Carcinoma? J. Oral. Maxillofac. Surg. 2019, 77, 1510–1519. [Google Scholar] [CrossRef] [PubMed]
- Sayed, S.I.; Sharma, S.; Rane, P.; Vaishampayan, S.; Talole, S.; Chaturvedi, P.; Chaukar, D.; Deshmukh, A.; Agarwal, J.P.; D’cruz, A.K. Can metastatic lymph node ratio (LNR) predict survival in oral cavity cancer patients? J. Surg. Oncol. 2013, 108, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, A.; Zhang, W.J.; Gao, K.; Clark, J.R. Nodal yield and survival in oral squamous cancer: Defining the standard of care. Cancer 2011, 117, 2917–2925. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Categories | Total Population (n = 62) | LND < 0.04 | LND ≥ 0.04 |
|---|---|---|---|---|
| * Age (years) | 60.86 ± 14.90 | 62.14 ± 14.82 | 57.57 ± 14.75 | |
| Age (years) | <40 40–60 | 4 (6.5%) 25 (40.3%) | 3 (75%) 19 (76%) | 1 (25%) 6 (24%) |
| >60 | 33 (53.2%) | 27 (81.8%) | 6 (18.2%) | |
| Gender | Male Female | 38 (61.29%) 24 (38.7%) | 30 (78.9%) 19 (79.2%) | 8 (21.1%) 5 (20.8%) |
| Smoker | No Yes | 28 (45.2%) 34 (54.8%) | 22 (78.6%) 27 (79.4%) | 6 (21.4%) 7 (20.6%) |
| Drinker | No Yes | 43 (69.4%) 19 (30.6%) | 33 (76.7%) 16 (84.2%) | 10 (23.3%) 3 (15.8%) |
| Variable | Categories | Total Population (n = 62) | LND < 0.04 | LND ≥ 0.04 |
|---|---|---|---|---|
| Clinical T | 1 | 25 (40.3%) | 21 (84%) | 3 (16%) |
| 2 | 35 (56.5%) | 26 (74.3%) | 9 (25.7%) | |
| 3 | 1 (1.6%) | 1 (100%) | 0 (0.0%) | |
| 4 | 1 (1.6%) | 0 (0.0%) | 1 (100%) | |
| Tumor location | Lateral border | 55 (88.7%) | 43 (78.2%) | 12 (21.8%) |
| Dorsal | 1 (1.6%) | 1 (100%) | 0 (0.0%) | |
| Ventral | 6 (3.2%) | 5 (83.3%) | 1 (16.7%) | |
| Side | Right | 24 (38.7%) | 18 (75%) | 6 (25%) |
| Left | 38 (61.3%) | 31 (81.6%) | 7 (18.4%) | |
| Diagnostic CT | No Yes | 1 (1.6%) | 1 (100%) | 0 (0.0%) |
| 61 (98.4%) | 48 (78.7%) | 13 (21.3%) | ||
| Diagnostic MRI | No Yes | 46 (74.2%) | 35 (76.1%) | 11 (23.9%) |
| 16 (25.8%) | 14 (87.5%) | 2 (12.5%) | ||
| Radiologic T | No valuable | 17 (27.4%) | 14 (82.4%) | 3 (17.6%) |
| 1 | 17 (27.4%) | 17 (100%) | 0 (0.0%) | |
| 2 | 20 (32.3%) | 13 (65%) | 7 (35%) | |
| 3 | 5 (8.1%) | 2 (40%) | 3 (60%) | |
| 4a | 2 (3.2%) | 2 (100%) | 0 (0.0%) | |
| r-DOI | No valuable | 32 (51.6%) | 26 (81.2%) | 6 (18.8%) |
| <5 cm | 3 (4.8%) | 3 (100%) | 0 (0.0%) | |
| 5–10 cm | 16 (25.8%) | 12 (75%) | 4 (25%) | |
| >10 cm | 9 (14.5%) | 6 (66.7%) | 3 (33.3%) | |
| LOST | 2 (3.2%) | 2 (100%) | 0 (0.0%) | |
| Clinical Stage | I | 21 (33.9%) | 20 (95.2%) | 1 (4.8%) |
| II | 27 (43.6%) | 20 (74.1%) | 7 (25.9%) | |
| III | 10 (16.1%) | 6 (60%) | 4 (40%) | |
| IVa | 4 (6.5%) | 3 (75%) | 1 (25%) | |
| Reconstruction | Direct closure | 26 (41.9%) | 23 (88.5%) | 3 (11.5%) |
| Local flap | 16 (25.8%) | 13 (81.3%) | 3 (18.7%) | |
| Microsurgery | 20 (32.3%) | 13 (65%) | 7 (35%) | |
| Neck dissection | Unilateral | 32 (51.6%) | 29 (90.6%) | 3 (9.4%) |
| Bilateral | 30 (48.4%) | 20 (66.7%) | 10 (33.3%) | |
| Type of neck dissection | Selective | 27 (43.5%) | 23 (85.2%) | 4 (14.8%) |
| Functional | 35 (56.5%) | 26 (74.3%) | 9 (25.7%) | |
| Postoperative radiotherapy | No Yes | 31 (50%) | 29 (93.5%) | 2 (6.5%) |
| 31 (50%) | 20 (64.5%) | 11 (35.5%) | ||
| Postoperative chemotherapy | No Yes | 57 (91.9%) | 45 (78.9%) | 12 (21.1%) |
| 5 (8.1%) | 4 (80%) | 1 (20%) |
| Variable | Categories | Total Population (n = 62) | LND < 0.04 | LND ≥ 0.04 |
|---|---|---|---|---|
| Differentiation | Well | 4 (6.5%) | 3 (75%%) | 1 (25%) |
| Moderate | 48 (77.4%) | 38 (79.2%) | 10 (20.8%) | |
| Poor | 10 (16.1%) | 8 (80%) | 2 (20%) | |
| Margin Status | Near | 13 (21%) | 9 (69.2%) | 4 (30.8%) |
| Clear | 49 (79%) | 40 (81.6%) | 9 (18.4%) | |
| Pathologic T | 1 | 15 (24.2%) | 14 (93.3%) | 1 (6.7%) |
| 2 | 23 (37.1%) | 22 (95.7%) | 2 (4.3%) | |
| 3 | 23 (37.1%) | 14 (60.9%) | 9 (39.1%) | |
| 4 | 1 (1.6%) | 0 (0.0%) | 1 (100%) | |
| DOI | No valuable | 2 (3.2%) | 1 (50%) | 1 (50%) |
| <5 cm | 15 (24.2%) | 14 (93.3%) | 1 (6.7%) | |
| 5–10 cm | 24 (38.7%) | 21 (87.5%) | 3 (12.5%) | |
| >10 cm | 21 (33.9%) | 13 (61.9%) | 8 (38.1%) | |
| Positive neck | No Yes | 42 (67.7%) 20 (32.3%) | 42 (100%) 7 (35%) | 0 (0.0%) 13 (65%) |
| Histological neck | pN0 | 42 (67.7%) | 42 (100%) | 0 (0.0%) |
| pN+ ipsilateral | 13 (21%) | 6 (46.2%) | 7 (53.8%) | |
| pN+ contralateral | 2 (3.2%) | 0 (0.0%) | 2 (100%) | |
| pN+ bilateral | 5 (8.1%) | 0 (0.0%) | 4 (100%) | |
| Extracapsular extension | No Yes | 58 (93.6%) | 47 (81%) | 11 (19%) |
| 4 (6.5%) | 2 (50%) | 2 (50%) | ||
| Pathologic N | N0 | 42 (67.7%) | 42 (100%) | 0 (0.0%) |
| N1 | 8 (12.9%) | 5 (62.5%) | 3 (37.5%) | |
| N2a | 1 (1.6%) | 0 (0.0%) | 1 (100%) | |
| N2b | 5 (8.1%) | 1 (20%) | 4 (80%) | |
| N2c | 4 (6.5%) | 0 (0.0%) | 4 (100%) | |
| N3a | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| N3b | 2 (3.2%) | 1(50%) | 1 (50%) | |
| Perineural invasion | No Yes | 26 (41.9%) | 25 (96.2%) | 1 (3.8%) |
| 36 (58.1%) | 24 (66.7%) | 12 (33.3%) | ||
| Lymphovascular invasion | No Yes | 55 (88.7%) | 45 (81.8%) | 10 (18.2%) |
| 7 (11.3%) | 4 (57.1%) | 3 (42.9%) | ||
| Pathological Stage | I | 13 (21.0%) | 13 (100%) | 0 (0.0%) |
| II | 18 (29.0%) | 17 (94.4%) | 1 (5.6%) | |
| III | 19 (30.6%) | 17 (89.5%) | 2 (10.5%) | |
| IV | 12 (19.4%) | 2 (16.7%) | 10 (83.3%) | |
| Dissection > 18 lymph nodes | No Yes | 25 (40.3%) | 20 (80%) | 5 (20%) |
| 37 (59.7%) | 29 (78.4%) | 8 (21.6%) |
| Variable | Category | Total Population (n = 62) | LND < 0.04 | LND ≥ 0.04 |
|---|---|---|---|---|
| Loco- regional recurrence | No Yes | 45 (69.35%) | 38 (84.4%) | 7 (15.6%) |
| 17 (27.42%) | 11 (64.7%) | 6 (35.3%) | ||
| Distant disease | No Yes | 51 (82.26%) | 41 (80.4%) | 10 (19.6%) |
| 11 (17.74%) | 8 (72.7%) | 3 (27.3%) | ||
| Exitus | No Yes | 47 (75.8%) | 39 (83%) | 8 (17%) |
| 15 (24.2%) | 10 (66.7%) | 5 (33.3%) |
| LND | Mean ± Standard Error of Mean (S.E.M.) | Log Rank (Mantel-Cox) (p-Value) |
|---|---|---|
| <0.04 | 76.97 ± 5.27 months | |
| ≥0.04 | 56.67 ± 10.53 months | 0.147 |
| LND | Mean ± Standard Error of Mean (S.E.M.) | Log Rank (Mantel-Cox) (p-Value) |
|---|---|---|
| <0.04 | 76.13 ± 5.72 months | |
| ≥0.04 | 45.22 ± 10.59 months | 0.099 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro Cuéllar, C.; Sada Urmeneta, Á.; Lorenzo Marcos, R.; Antúnez-Conde, R.; López López, A.; del Castillo Pardo de Vera, J.L.; González Martín-Moro, J.; Cebrián Carretero, J.L.; Alijo Serrano, F.; Dell’Aversana Orabona, G.; et al. Prognostic Value of Lymph Node Density in Lingual Squamous Cell Carcinoma. Appl. Sci. 2023, 13, 5611. https://0-doi-org.brum.beds.ac.uk/10.3390/app13095611
Navarro Cuéllar C, Sada Urmeneta Á, Lorenzo Marcos R, Antúnez-Conde R, López López A, del Castillo Pardo de Vera JL, González Martín-Moro J, Cebrián Carretero JL, Alijo Serrano F, Dell’Aversana Orabona G, et al. Prognostic Value of Lymph Node Density in Lingual Squamous Cell Carcinoma. Applied Sciences. 2023; 13(9):5611. https://0-doi-org.brum.beds.ac.uk/10.3390/app13095611
Chicago/Turabian StyleNavarro Cuéllar, Carlos, Ángela Sada Urmeneta, Raquel Lorenzo Marcos, Raúl Antúnez-Conde, Ana López López, José Luis del Castillo Pardo de Vera, Javier González Martín-Moro, José Luis Cebrián Carretero, Francisco Alijo Serrano, Giovanni Dell’Aversana Orabona, and et al. 2023. "Prognostic Value of Lymph Node Density in Lingual Squamous Cell Carcinoma" Applied Sciences 13, no. 9: 5611. https://0-doi-org.brum.beds.ac.uk/10.3390/app13095611