Vestibular Functioning in Children with Neurodevelopmental Disorders Using the Functional Head Impulse Test


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
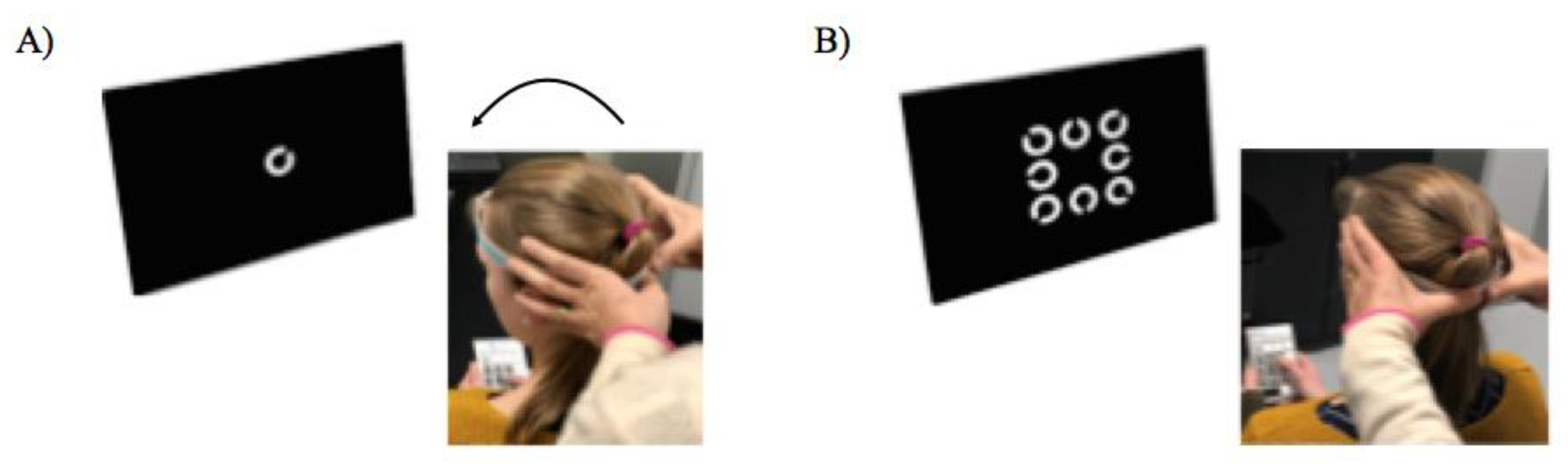
2.2. Functional Head Impulse Test (fHIT)
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Leigh, R.J.; Zee, D.S. The Neurology of Eye Movements; Oxford University Press (OUP): Oxford, UK, 2015. [Google Scholar]
- Halmagyi, G.M.; Curthoys, I.S. A Clinical Sign of Canal Paresis. Arch. Neurol. 1988, 45, 737–739. [Google Scholar] [CrossRef]
- Beh, S.C.; Frohman, T.C.; Frohman, E.M. Cerebellar Control of Eye Movements. J. Neuro Ophthalmol. 2017, 37, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-Y.; Kim, H.-J.; Kim, J.-S. Recent advances in head impulse test findings in central vestibular disorders. Neurology 2018, 90, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Kheradmand, A.; Zee, D.S. Cerebellum and Ocular Motor Control. Front. Neurol. 2011, 2, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koziol, L.L.; Budding, D.D.; Andreasen, N.N.; D’Arrigo, S.S.; Bulgheroni, S.S.; Imamizu, H.H.; Ito, M.M.; Manto, M.; Marvel, C.C.; Parker, K.K.; et al. Consensus Paper: The Cerebellum’s Role in Movement and Cognition. Cerebellum 2014, 13, 151–177. [Google Scholar] [CrossRef]
- Wang, S.S.-H.; Kloth, A.D.; Badura, A. The Cerebellum, Sensitive Periods, and Autism. Neuron 2014, 83, 518–532. [Google Scholar] [CrossRef] [Green Version]
- Goulardins, J.B.; Marques, J.C.B.; De Oliveira, J.A. Attention Deficit Hyperactivity Disorder and Motor Impairment. Percept. Mot. Ski. 2017, 124, 425–440. [Google Scholar] [CrossRef]
- Lim, Y.H.; Partridge, K.; Girdler, S.; Morris, S.L. Standing Postural Control in Individuals with Autism Spectrum Disorder: Systematic Review and Meta-analysis. J. Autism Dev. Disord. 2017, 47, 2238–2253. [Google Scholar] [CrossRef]
- Bucci, M.P.; Goulème, N.; Stordeur, C.; Acquaviva, E.; Scheid, I.; Lefebvre, A.; Gerard, C.-L.; Peyre, H.; Delorme, R. Discriminant validity of spatial and temporal postural index in children with neurodevelopmental disorders. Int. J. Dev. Neurosci. 2017, 61, 51–57. [Google Scholar] [CrossRef]
- Stins, J.F.; Emck, C. Balance Performance in Autism: A Brief Overview. Front. Psychol. 2018, 9, 901. [Google Scholar] [CrossRef] [Green Version]
- Valera, E.M.; Faraone, S.V.; Murray, K.E.; Seidman, L.J. Meta-Analysis of Structural Imaging Findings in Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2007, 61, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Stoodley, C.J. Distinct regions of the cerebellum show gray matter decreases in autism, ADHD, and developmental dyslexia. Front. Syst. Neurosci. 2014, 8, 92. [Google Scholar] [CrossRef] [PubMed]
- Bruchhage, M.M.; Bucci, M.P.; Becker, E.B.E. Cerebellar Involvement in Autism and ADHD; Elsevier BV: Amsterdam, The Netherlands, 2018; Volume 155, pp. 61–72. [Google Scholar]
- Ramat, S.; Colnaghi, S.; Boehler, A.; Astore, S.; Falco, P.; Mandalà, M.; Nuti, D.; Colagiorgio, P.; Versino, M. A Device for the Functional Evaluation of the VOR in Clinical Settings. Front. Neurol. 2012, 3, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corallo, G.; Versino, M.; Mandalà, M.; Colnaghi, S.; Ramat, S. The functional head impulse test: Preliminary data. J. Neurol. 2018, 265, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Versino, M.; Colnaghi, S.; Corallo, G.; Mandalà, M.; Ramat, S. The functional head impulse test: Comparing gain and percentage of correct answers. Prog. Brain Res. 2019, 248, 241–248. [Google Scholar] [CrossRef]
- Chevrie-Muller, C.; Simon, A.M.; Fournier, S. Batterie Langage oral écrit. Mémoire. Attention: L2MA; Editions du Centre de Psychologie Appliquée: Paris, France, 1997. [Google Scholar]
- American Psychiatric Association APA. Diagnostic and Statistical Manual of Mental Disorders (DSM 5th ed.); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Goldman, L.S.; Genel, M.; Bezman, R.J.; Slanetz, P.J.; American Medical Association for the Council on Scientific Affairs. Diagnosis and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. JAMA 1998, 279, 1100–1107. [Google Scholar] [CrossRef]
- Du Paul, G.J.; Power, T.J.; Anastopoulos, A.D.; Reid, R. ADHD Rating Scale-IV: Checklists, Norms and Clinical Interpretation; Guilford: New York, NY, USA, 1998. [Google Scholar]
- Collett, B.R.; Ohan, J.L.; Myers, K.M. Ten-Year Review of Rating Scales. V: Scales Assessing Attention-Deficit/Hyperactivity Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 1015–1037. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Intelligence Scale for Children-Fifth Edition; Pearson: Bloomington, MN, USA, 2014. [Google Scholar]
- Böhler, A.; Mandalà, M.; Ramat, S. A software program for the Head Impulse Testing Device (HITD). In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2010; Volume 2010, pp. 6615–6618. [Google Scholar]
- Romano, F.; Bertolini, G.; Agostino, D.; Straumann, D.; Ramat, S.; Feddermann-Demont, N. Functional Head Impulse Test in Professional Athletes: Sport-Specific Normative Values and Implication for Sport-Related Concussion. Front. Neurol. 2019, 10, 387. [Google Scholar] [CrossRef]
- Van Dooren, T.S.; Lucieer, F.M.P.; Duijn, S.; Janssen, A.M.L.; Guinand, N.; Fornos, A.P.; Van Rompaey, V.; Kingma, H.; Ramat, S.; Van De Berg, R. The Functional Head Impulse Test to Assess Oscillopsia in Bilateral Vestibulopathy. Front. Neurol. 2019, 10, 365. [Google Scholar] [CrossRef] [PubMed]
- Gurvich, C.; Maller, J.J.; Lithgow, B.; Haghgooie, S.; Kulkarni, J. Vestibular insights into cognition and psychiatry. Brain Res. 2013, 1537, 244–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hecke, R.; Danneels, M.; Dhooge, I.; Van Waelvelde, H.; Wiersema, J.R.; Deconinck, F.J.A.; Maes, L. Vestibular Function in Children with Neurodevelopmental Disorders: A Systematic Review. J. Autism Dev. Disord. 2019, 49, 3328–3350. [Google Scholar] [CrossRef] [PubMed]
- Carson, T.B.; Wilkes, B.J.; Patel, K.; Pineda, J.L.; Ko, J.H.; Newell, K.M.; Bodfish, J.W.; Schubert, M.C.; Radonovich, K.; White, K.D.; et al. Vestibulo-ocular re ex function in children with high-functioning autism spectrum disorders. Autism Res. 2017, 10, 251–266. [Google Scholar] [CrossRef] [PubMed]
- Deroualle, D.; Lopez, C. Toward a vestibular contribution to social cognition. Front. Integr. Neurosci. 2014, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Isaac, V.; Olmedo, D.; Aboitiz, F.; Délano, P.H. Altered Cervical Vestibular-Evoked Myogenic Potential in Children with Attention Deficit and Hyperactivity Disorder. Front. Neurol. 2017, 8, 90. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.-Y.; Kim, H.-J.; Kim, J.-S. Vestibular-evoked myogenic potentials in central vestibular disorders. J. Neurol. 2016, 263, 210–220. [Google Scholar] [CrossRef]
- Konicarova, J.; Bob, P. Asymmetric tonic neck reflex and symptoms of attention deficit and hyperactivity disorder in children. Int. J. Neurosci. 2013, 123, 766–769. [Google Scholar] [CrossRef]
- Taylor, B.; Hanna, D.; McPhillips, M. Motor problems in children with severe emotional and behavioural difficulties. Br. J. Educ. Psychol. 2019, 90, 719–735. [Google Scholar] [CrossRef]
- Hullar, T.E. Semicircular canal geometry, afferent sensitivity, and animal behavior. Anat. Rec. Part A Discov. Mol. Cell. Evol. Biol. 2006, 288, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Bigelow, R.T.; Agrawal, Y. Vestibular involvement in cognition: Visuospatial ability, attention, executive function, and memory. J. Vestib. Res. 2015, 25, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, N.; Arai, M.; Goto, F. Changes in cognitive function in patients with intractable dizziness following vestibular rehabilitation. Sci. Rep. 2018, 8, 9984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pineault, K.; Pearson, D.; Wei, E.; Kamil, R.; Klatt, B.; Agrawal, Y. Association Between Saccule and Semicircular Canal Impairments and Cognitive Performance Among Vestibular Patients. Ear Hear. 2020, 41, 686–692. [Google Scholar] [CrossRef]
- Ramos, T.C.; Balardin, J.B.; Sato, J.R.; Fujita, A. Abnormal Cortico-Cerebellar Functional Connectivity in Autism Spectrum Disorder. Front. Syst. Neurosci. 2019, 12, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, V.G.; Juranek, J.; Romanowska-Pawliczek, A.; Stuebing, K.K.; Williams, V.J.; Fletcher, J.M. White matter integrity of cerebellar-cortical tracts in reading impaired children: A probabilistic tractography study. Brain Lang. 2016, 161, 45–56. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Chen, S.-R.; Pan, H.-L. Muscarinic receptor subtypes differentially control synaptic input and excitability of cerebellum-projecting medial vestibular nucleus neurons. J. Neurochem. 2016, 137, 226–239. [Google Scholar] [CrossRef]
- Becker, E.B.; Stoodley, C.J. Autism spectrum of the cerebellum. Int. Rev. Neurobiol. 2013, 113, 1–34. [Google Scholar]
- Verly, M.; Verhoeven, J.; Zink, I.; Mantini, D.; Peeters, R.; Deprez, S.; Emsell, L.; Boets, B.; Noens, I.; Steyaert, J.; et al. Altered functional connectivity of the language network in ASD: Role of classical language areas and cerebellum. NeuroImage Clin. 2014, 4, 374–382. [Google Scholar] [CrossRef] [Green Version]
- D’Mello, A.M.; Crocetti, D.; Mostofsky, S.H.; Stoodley, C.J. Cerebellar gray matter and lobular volumes correlate with core autism symptoms. NeuroImage Clin. 2015, 7, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Stoodley, C.J. The Cerebellum and Neurodevelopmental Disorders. Cerebellum 2016, 15, 34–37. [Google Scholar] [CrossRef]
- Tomasi, D.; Volkow, N.D. Abnormal Functional Connectivity in Children with Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2012, 71, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norton, E.S.; Black, J.M.; Stanley, L.M.; Tanaka, H.; Gabrieli, J.D.E.; Sawyer, C.; Hoeft, F. Functional neuroanatomical evidence for the double-deficit hypothesis of developmental dyslexia. Neuropsychologia 2014, 61, 235–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levit-Binnun, N.; Davidovitch, M.; Golland, Y. Sensory and motor secondary symptoms as indicators of brain vulnerability. J. Neurodev. Disord. 2013, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewey, D.; Bernier, F.P. The Concept of Atypical Brain Development in Developmental Coordination Disorder (DCD)—A New Look. Curr. Dev. Disord. Rep. 2016, 3, 161–169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group 1 DYS N = 20 | Group 2 ADHD N = 20 | Group 3 ASD N = 20 | Group 4 TD N = 20 | |
|---|---|---|---|---|
| Age (years) | 9.6 ± 0.2 | 9.5 ± 0.3 | 9.7 ± 0.5 | 9.2 ± 0.4 |
| ADHD-RS total score | 5.1 ± 1.8 | 38.7 ± 1.7 | 5.2 ± 1.1 | 4.8 ± 1.2 |
| L2MA standard deviation from the mean | ||||
| Oral Language | 2.8 | |||
| Written Language | 2.6 | |||
| Memory | 2.7 | |||
| Autism Diagnostic Interview-Revised (ADI-R) scores | ||||
| Social Reciprocal Interaction | 18.5 ± 1.5 | |||
| Communication | 12.5 ± 0.9 | |||
| Stereotyped Patterns of Behaviors | 5.1 ± 0.5 | |||
| Autism Diagnostic Observation Schedule (ADOS) scores | ||||
| Social Reciprocal Interaction | 8.4 ± 0.8 | |||
| Communication | 3.9 ± 0.4 | |||
| Wechsler scale (WISC-V) scores | ||||
| Verbal Comprehension subscale | 101 ± 6 | 100 ± 5 | 101 ± 2 | |
| Perceptual Reasoning subscale | 99 ± 4 | 98 ± 3 | 97 ± 2 | |
| Working Memory subscale | 93 ± 3 | 91 ± 4 | 86 ± 4 | |
| Processing Speed subscale | 89 ± 3 | 90 ± 5 | 91 ± 3 | |
| Similarity test | 12 ± 1 | 12 ± 2 | 10 ± 2 | 12 ± 1 |
| Matrix reasoning test | 11 ± 1 | 10.2 ± 1 | 10.5 ± 1 | 10.8 ± 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caldani, S.; Baghdadi, M.; Moscoso, A.; Acquaviva, E.; Gerard, C.-L.; Marcelli, V.; Peyre, H.; Atzori, P.; Delorme, R.; Bucci, M.P. Vestibular Functioning in Children with Neurodevelopmental Disorders Using the Functional Head Impulse Test. Brain Sci. 2020, 10, 887. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110887
Caldani S, Baghdadi M, Moscoso A, Acquaviva E, Gerard C-L, Marcelli V, Peyre H, Atzori P, Delorme R, Bucci MP. Vestibular Functioning in Children with Neurodevelopmental Disorders Using the Functional Head Impulse Test. Brain Sciences. 2020; 10(11):887. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110887
Chicago/Turabian StyleCaldani, Simona, Moetez Baghdadi, Ana Moscoso, Eric Acquaviva, Christophe-Loïc Gerard, Vincenzo Marcelli, Hugo Peyre, Paola Atzori, Richard Delorme, and Maria Pia Bucci. 2020. "Vestibular Functioning in Children with Neurodevelopmental Disorders Using the Functional Head Impulse Test" Brain Sciences 10, no. 11: 887. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110887