Brain Metastases in Elderly Patients—The Role of Surgery in the Context of Systemic Treatment

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Demographics
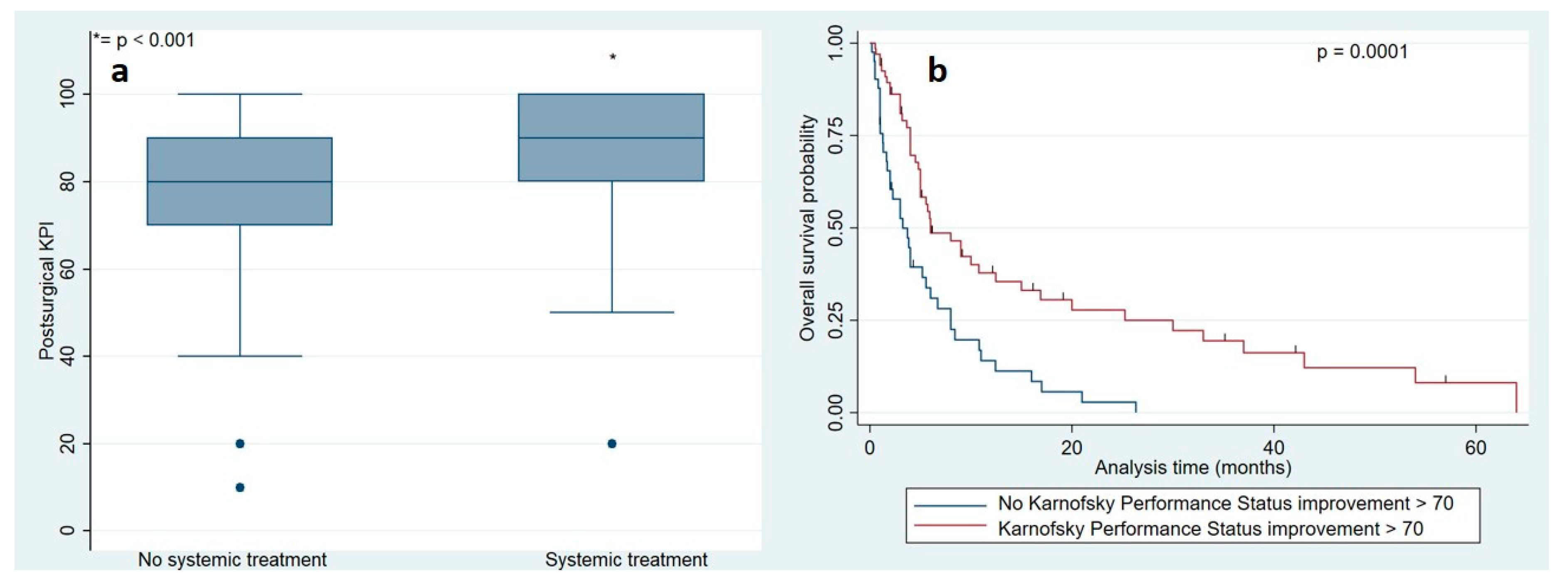
2.2. Surgical Outcome and Complications
2.3. Postsurgical Treatment Patterns
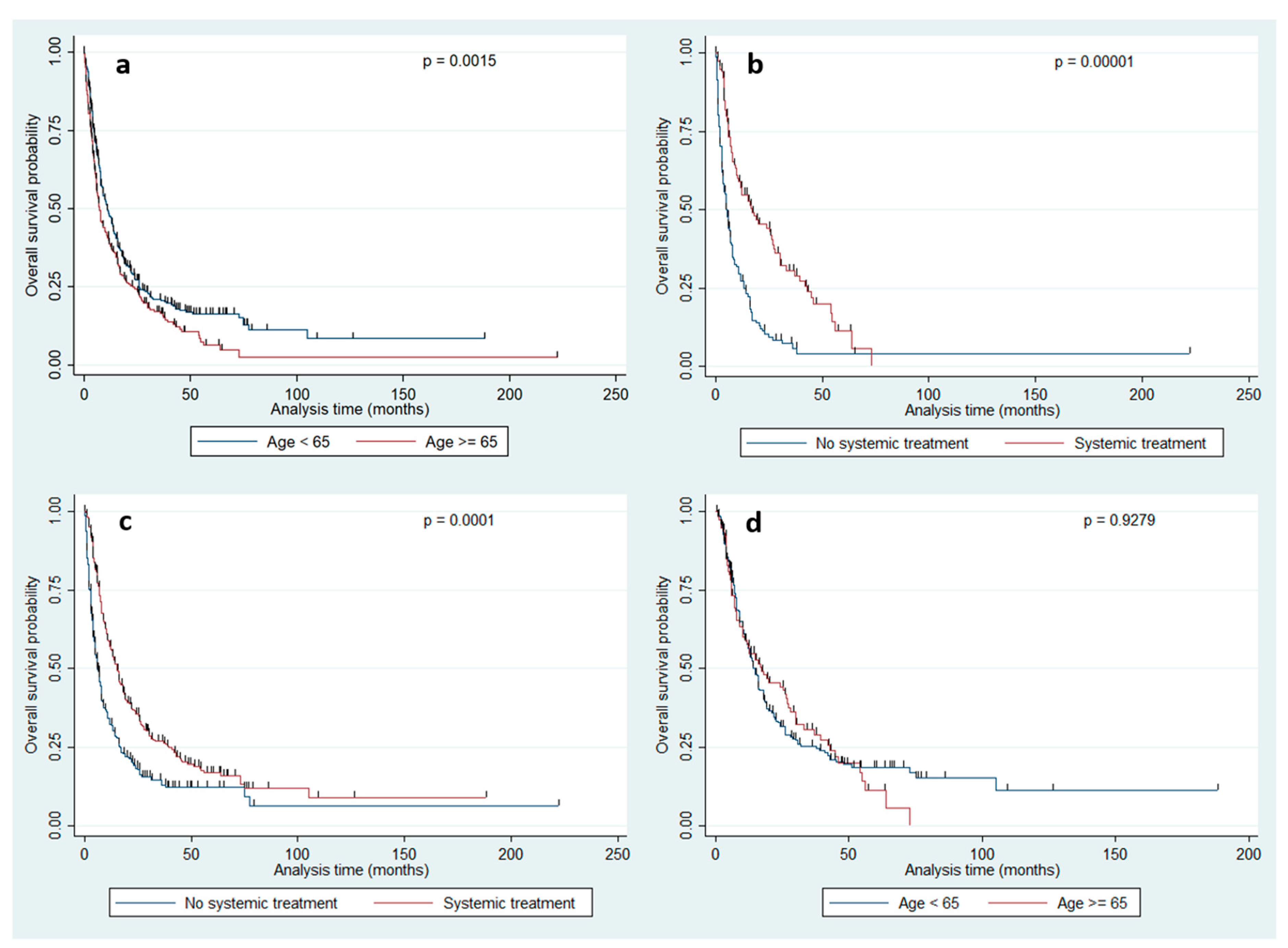
2.4. Survival Outcome
3. Discussion
4. Patients and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lehr, U. Population ageing. Online Handbook Demography; Berlin Institute for Population and Development: Berlin, Germany, 2007. [Google Scholar]
- Ershler, W.B. Cancer: A disease of the elderly. J. Support. Oncol. 2003, 1, 5–10. [Google Scholar] [PubMed]
- Ascha, M.S.; Ostrom, Q.T.; Wright, J.; Kumthekar, P.; Bordeaux, J.S.; Sloan, A.E.; Schumacher, F.R.; Kruchko, C.; Barnholtz-Sloan, J.S. Lifetime Occurrence of Brain Metastases Arising from Lung, Breast, and Skin Cancers in the Elderly: A SEER-Medicare Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Printz, C. Some elderly survivors of 3 common cancers have an increased risk of brain metastases. Cancer 2019, 125, 3286–3287. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1,960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef]
- Tendulkar, R.D.; Liu, S.W.; Barnett, G.H.; Vogelbaum, M.A.; Toms, S.A.; Jin, T.; Suh, J.H. RPA classification has prognostic significance for surgically resected single brain metastasis. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 810–817. [Google Scholar] [CrossRef]
- Paek, S.H.; Audu, P.B.; Sperling, M.R.; Cho, J.; Andrews, D.W. Reevaluation of surgery for the treatment of brain metastases: Review of 208 patients with single or multiple brain metastases treated at one institution with modern neurosurgical techniques. Neurosurgery 2005, 56, 1021–1034. [Google Scholar]
- Lee, C.H.; Kim, D.G.; Kim, J.W.; Han, J.H.; Kim, Y.H.; Park, C.K.; Kim, C.Y.; Paek, S.H.; Jung, H.W. The role of surgical resection in the management of brain metastasis: A 17-year longitudinal study. Acta Neurochir. (Wien) 2013, 155, 389–397. [Google Scholar] [CrossRef]
- Rossetto, M.; Ciccarino, P.; Lombardi, G.; Rolma, G.; Cecchin, D.; Della Puppa, A. Surgery on motor area metastasis. Neurosurg. Rev. 2016, 39, 71–78. [Google Scholar] [CrossRef]
- Salvati, M.; Tropeano, M.P.; Maiola, V.; Lavalle, L.; Brogna, C.; Colonnese, C.; Frati, A.; D'Elia, A. Multiple brain metastases: A surgical series and neurosurgical perspective. Neurol. Sci. 2018, 39, 671–677. [Google Scholar] [CrossRef]
- Schodel, P.; Schebesch, K.M.; Brawanski, A.; Proescholdt, M.A. Surgical resection of brain metastases-impact on neurological outcome. Int. J. Mol. Sci. 2013, 14, 8708–8718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schödel, P.; Jünger, S.T.; Wittersheim, M.; Reinhardt, H.C.; Schmidt, N.O.; Goldbrunner, R.; Proescholdt, M.; Grau, S. Surgical resection of symptomatic brain metastases improves the clinical status and facilitates further treatment. Cancer Med. 2020, 9, 7503–7510. [Google Scholar] [CrossRef] [PubMed]
- Moravan, M.J.; Fecci, P.E.; Anders, C.K.; Clarke, J.M.; Salama, A.K.S.; Adamson, J.D.; Floyd, S.R.; Torok, J.A.; Salama, J.K.; Sampson, J.H.; et al. Current multidisciplinary management of brain metastases. Cancer 2020, 126, 1390–1406. [Google Scholar] [CrossRef]
- Leone, J.P.; Haraldsson, B.; Mott, S.L.; McDowell, B.D.; Chrischilles, E.A. Treatment Patterns and Survival of Elderly Patients with Breast Cancer Brain Metastases. Am. J. Clin. Oncol. 2019, 42, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Dover, L.L.; Dulaney, C.R.; Williams, C.P.; Fiveash, J.B.; Jackson, B.E.; Warren, P.P.; Kvale, E.A.; Boggs, D.H.; Rocque, G.B. Hospice care, cancer-directed therapy, and Medicare expenditures among older patients dying with malignant brain tumors. Neuro Oncol. 2018, 20, 986–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minniti, G.; Esposito, V.; Clarke, E.; Scaringi, C.; Bozzao, A.; Lanzetta, G.; De Sanctis, V.; Valeriani, M.; Osti, M.; Enrici, R.M. Stereotactic radiosurgery in elderly patients with brain metastases. J. Neurooncol. 2013, 111, 319–325. [Google Scholar] [CrossRef]
- Sankey, E.W.; Tsvankin, V.; Grabowski, M.M.; Nayar, G.; Batich, K.A.; Risman, A.; Champion, C.D.; Salama, A.K.S.; Goodwin, C.R.; Fecci, P.E. Operative and peri-operative considerations in the management of brain metastasis. Cancer Med. 2019, 8, 6809–6831. [Google Scholar] [CrossRef]
- Rotta, J.M.; Rodrigues, D.B.; Diniz, J.M.; Abreu, B.M.; Kamimura, F.; Sousa, U.O.; Botelho, R.V.; Oliveira, M.F. Analysis of survival in patients with brain metastases treated surgically: Impact of age, gender, oncologic status, chemotherapy, radiotherapy, number and localization of lesions, and primary cancer site. Rev. Assoc. Med. Bras. 2018, 64, 717–722. [Google Scholar] [CrossRef]
- D'Andrea, G.; Palombi, L.; Minniti, G.; Pesce, A.; Marchetti, P. Brain Metastases: Surgical Treatment and Overall Survival. World Neurosurg. 2017, 97, 169–177. [Google Scholar] [CrossRef]
- Brusselaers, N.; Lagergren, J. The Charlson Comorbidity Index in Registry-based Research. Methods Inf. Med. 2017, 56, 401–406. [Google Scholar] [CrossRef]
- Kavouridis, V.K.; Harary, M.; Hulsbergen, A.F.C.; Lo, Y.T.; Reardon, D.A.; Aizer, A.A.; Iorgulescu, J.B.; Smith, T.R. Survival and prognostic factors in surgically treated brain metastases. J. Neurooncol. 2019, 143, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Antuna, A.R.; Vega, M.A.; Sanchez, C.R.; Fernandez, V.M. Brain Metastases of Non-Small Cell Lung Cancer: Prognostic Factors in Patients with Surgical Resection. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2018, 79, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Pahernik, S.; Hadaschik, B.; Teber, D.; Duensing, S.; Jager, D.; Hohenfellner, M.; Grullich, C. Impact of resection and systemic therapy on the survival of patients with brain metastasis of metastatic renal cell carcinoma. J. Neurooncol. 2016, 130, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Leone, J.P.; Lee, A.V.; Brufsky, A.M. Prognostic factors and survival of patients with brain metastasis from breast cancer who underwent craniotomy. Cancer Med. 2015, 4, 989–994. [Google Scholar] [CrossRef]
- Stark, A.M.; Stohring, C.; Hedderich, J.; Held-Feindt, J.; Mehdorn, H.M. Surgical treatment for brain metastases: Prognostic factors and survival in 309 patients with regard to patient age. J. Clin. Neurosci. 2011, 18, 34–38. [Google Scholar] [CrossRef]
- Hwang, S.L.; Howng, S.L. Prognostic analysis in patients of lung cancer with brain metastasis under surgical removal. Kaohsiung. J. Med. Sci. 1998, 14, 126–131. [Google Scholar]
- Chen, R.C.; Royce, T.J.; Extermann, M.; Reeve, B.B. Impact of age and comorbidity on treatment and outcomes in elderly cancer patients. Semin. Radiat. Oncol. 2012, 22, 265–271. [Google Scholar] [CrossRef]
- Noordijk, E.M.; Vecht, C.J.; Haaxma-Reiche, H.; Padberg, G.W.; Voormolen, J.H.; Hoekstra, F.H.; Tans, J.T.; Lambooij, N.; Metsaars, J.A.; Wattendorff, A.R.; et al. The choice of treatment of single brain metastasis should be based on extracranial tumor activity and age. Int. J. Radiat. Oncol. Biol. Phys. 1994, 29, 711–717. [Google Scholar] [CrossRef]
- Dale, D.C. Poor prognosis in elderly patients with cancer: The role of bias and undertreatment. J. Support. Oncol. 2003, 1, 11–17. [Google Scholar]
- Denson, A.C.; Mahipal, A. Participation of the elderly population in clinical trials: Barriers and solutions. Cancer Control 2014, 21, 209–214. [Google Scholar] [CrossRef]
- Hutchins, L.F.; Unger, J.M.; Crowley, J.J.; Coltman, C.A., Jr.; Albain, K.S. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N. Engl. J. Med. 1999, 341, 2061–2067. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.H.; Kilgore, M.L.; Goldman, D.P.; Trimble, E.L.; Kaplan, R.; Montello, M.J.; Housman, M.G.; Escarce, J.J. Participation of patients 65 years of age or older in cancer clinical trials. J. Clin. Oncol. 2003, 21, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Feliu, J.; Heredia-Soto, V.; Girones, R.; Jimenez-Munarriz, B.; Saldana, J.; Guillen-Ponce, C.; Molina-Garrido, M.J. Management of the toxicity of chemotherapy and targeted therapies in elderly cancer patients. Clin. Transl. Oncol 2020, 22, 457–467. [Google Scholar] [CrossRef]
- Grossman, R.; Nossek, E.; Sitt, R.; Hayat, D.; Shahar, T.; Barzilai, O.; Gonen, T.; Korn, A.; Sela, G.; Ram, Z. Outcome of elderly patients undergoing awake-craniotomy for tumor resection. Ann. Surg. Oncol. 2013, 20, 1722–1728. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total | Age Group | p-Value | |
|---|---|---|---|---|
| >= 65 (A) | < 65 (B) | |||
| N | 807 | 315 | 492 | |
| Age (years) Mean/median Range | 60.6/61.0 29.8–85.9 | 71.2/72.1 65–85.9 | 53.6/55.8 25.3–64.9 | |
| Gender Female (%) Male (%) | 51.05 48.95 | 45.1 54.9 | 54.9 45.1 | 0.0007 |
| Primary cancer sites (%) Lung Breast Melanoma GI tract Kidney Others | 41.5 15.4 14.6 9.2 3.7 15.6 | 44.4 12.4 11.4 11.4 5.1 15.3 | 39.6 17.9 16.7 7.7 2.9 15.2 | 0.001 |
| Presurgical Karnofsky performance status Median Range | 80 40–100 | 80 40–100 | 80 40–100 | 0.128 |
| Postsurgical Karnofsky performance status Median Range | 90 50–100 | 90 50–100 | 90 60–100 | 0.0002 |
| Systemic disease control Yes (%) No (%) | 42.8 57.2 | 49.3 50.7 | 38.5 61.5 | 0.042 |
| Metastasis status (%) Solitary Singular Multiple | 22.9 38.9 38.2 | 30.5 38.4 31.1 | 18.1 39.2 42.7 | 0.0001 |
| Number of metastases Mean/median Range | 2.1/1 1–19 | 1.8/1 1–19 | 2.3/1 1–17 | 0.002 |
| Metastasis timing (%) Synchronous Metachronous | 36.4 63.6 | 37.5 62.5 | 35.8 64.2 | 0.327 |
| Comorbidity score Mean/median Range | 3.5/3.0 0–9 | 4.3/4.0 1–9 | 2.9/3.0 0–9 | 0.0001 |
| Interval between tumor diagnosis to BM Mean/median Range | 30.4/11.1 0–139 | 28.3/10.0 0–132 | 31.74/12.9 0–139 | 0.392 |
| Postsurgical radiation (%) | 86.6 | 80.0 | 87.6 | 0.009 |
| Postsurgical systemic treatment (%) | 49.2 | 45.1 | 59.9 | 0.0001 |
| Surgical morbidity (%) | 10.8 | 10.9 | 10.7 | 0.992 |
| Surgical mortality | 4.2 | 6.4 | 2.9 | 0.016 |
| Entire Population | Age Group | ||
|---|---|---|---|
| >= 65 (A) | < 65 (B) | ||
| Parameter | p-Value | p-Value | p-Value |
| Group A vs. B | 0.0015 | ||
| Age | 0.008 | 0.067 | 0.555 |
| Tumor location | 0.002 | 0.0005 | 0.161 |
| Gender | 0.071 | 0.159 | 0.691 |
| Comorbidity score | 0.604 | 0.859 | 0.123 |
| Primary tumor | 0.480 | 0.809 | 0.062 |
| Disease control | 0.013 | 0.129 | 0.011 |
| Metastasis timing | 0.021 | 0.035 | 0.226 |
| Metastasis status | 0.009 | 0.251 | 0.005 |
| Number of metastases | 0.152 | 0.321 | 0.173 |
| Interval between tumor diagnosis to BM | 0.225 | 0.030 | 0.962 |
| Postsurgical radiation | 0.0001 | 0.0001 | 0.0001 |
| Postsurgical systemic treatment | 0.0001 | 0.0001 | 0.0001 |
| Presurgical Karnofsky performance status | 0.0001 | 0.012 | 0.0001 |
| Postsurgical Karnofsky performance status | 0.0001 | 0.001 | 0.0001 |
| Extent of resection (complete vs. incomplete) | 0.257 | 0.219 | 0.496 |
| Parameter | Hazard Ratio | 95% CI | p-Value | |
|---|---|---|---|---|
| Presurgical Karnofsky performance status | 0.982 | 0.972 | 0.992 | 0.001 |
| Metastasis status | 1.264 | 1.076 | 1.486 | 0.004 |
| Group A/B | 1.369 | 1.070 | 1.751 | 0.012 |
| Tumor location | 1.066 | 1.014 | 1.121 | 0.012 |
| Postsurgical Karnofsky performance status | 0.990 | 0.981 | 1.000 | 0.038 |
| Metastasis timing | 0.784 | 0.604 | 1.017 | 0.067 |
| Postsurgical radiation | 0.820 | 0.662 | 1.017 | 0.072 |
| Postsurgical systemic treatment | 0.845 | 0.700 | 1.020 | 0.080 |
| Disease control | 0.917 | 0.702 | 1.199 | 0.530 |
| Parameter | Hazard Ratio | 95% CI | p-Value | |
|---|---|---|---|---|
| Interval tumor diagnosis BM | 0.996 | 0.993 | 0.999 | 0.040 |
| Metastasis timing | 0.811 | 0.632 | 1.041 | 0.101 |
| Presurgical Karnofsky performance status | 0.989 | 0.980 | 0.999 | 0.041 |
| Postsurgical Karnofsky performance status | 0.983 | 0.975 | 0.992 | 0.0001 |
| Postsurgical radiation | 0.753 | 0.580 | 0.978 | 0.034 |
| Postsurgical systemic treatment | 0.636 | 0.509 | 0.795 | 0.0001 |
| Tumor location | 1.041 | 0.985 | 1.110 | 0.133 |
| Parameter | Hazard Ratio | 95% CI | p-Value | |
|---|---|---|---|---|
| Disease control | 0.653 | 0.469 | 0.910 | 0.012 |
| Metastasis status | 1.260 | 1.087 | 1.460 | 0.002 |
| Presurgical Karnofsky performance status | 0.992 | 0.983 | 1.001 | 0.102 |
| Postsurgical Karnofsky performance status | 0.984 | 0.973 | 0.996 | 0.010 |
| Postsurgical radiation | 0.707 | 0.549 | 0.910 | 0.007 |
| Postsurgical systemic treatment | 0.751 | 0.613 | 0.920 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Proescholdt, M.; Jünger, S.T.; Schödel, P.; Schebesch, K.-M.; Doenitz, C.; Pukrop, T.; Höhne, J.; Schmidt, N.-O.; Kocher, M.; Schulz, H.; et al. Brain Metastases in Elderly Patients—The Role of Surgery in the Context of Systemic Treatment. Brain Sci. 2021, 11, 123. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11010123
Proescholdt M, Jünger ST, Schödel P, Schebesch K-M, Doenitz C, Pukrop T, Höhne J, Schmidt N-O, Kocher M, Schulz H, et al. Brain Metastases in Elderly Patients—The Role of Surgery in the Context of Systemic Treatment. Brain Sciences. 2021; 11(1):123. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11010123
Chicago/Turabian StyleProescholdt, Martin, Stephanie T. Jünger, Petra Schödel, Karl-Michael Schebesch, Christian Doenitz, Tobias Pukrop, Julius Höhne, Nils-Ole Schmidt, Martin Kocher, Holger Schulz, and et al. 2021. "Brain Metastases in Elderly Patients—The Role of Surgery in the Context of Systemic Treatment" Brain Sciences 11, no. 1: 123. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11010123