
The Effects of a Standardized Cognitive-Behavioural Therapy and an Additional Mindfulness-Based Training on Interoceptive Abilities in a Depressed Cohort

 , ,
, ,
Abstract
:1. Introduction
1.1. Interoceptive Dimensions and Depression
1.2. Approaches to Change Interoceptive Dimensions
1.3. The Present Study
- Mindfulness and interoceptive abilities will initially be reduced in the depressed sample compared to healthy controls. Further, these variables will increase in depressed patients over the time course of CBT.
- In an exploratory manner, the relationship between depressive symptoms, interoceptive abilities and mindfulness in the depressed sample and healthy controls will be examined.
- Depressed patients, as part of a CBT and an additional MBSR program, will experience increases in their mindfulness level and interoceptive abilities and decreases in their depressive scores over the time course.
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Instruments
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cameron, O.G. Interoception: The Inside Story—A Model for Psychosomatic Processes. Psychosom. Med. 2001, 63, 697–710. [Google Scholar] [CrossRef]
- Craig, A. Interoception: The sense of the physiological condition of the body. Curr. Opin. Neurobiol. 2003, 13, 500–505. [Google Scholar] [CrossRef]
- Garfinkel, S.N.; Seth, A.K.; Barrett, A.B.; Suzuki, K.; Critchley, H.D. Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biol. Psychol. 2015, 104, 65–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schandry, R. Heart Beat Perception and Emotional Experience. Psychophysiology 1981, 18, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Porges, S. Body Perception Questionnaire; Laboratory of Developmental Assessment, University of Maryland: College Park, MD, USA, 1993. [Google Scholar]
- Khalsa, S.S.; Adolphs, R.; Cameron, O.G.; Critchley, H.; Davenport, P.W.; Feinstein, J.S.; Feusner, J.D.; Garfinkel, S.N.; Lane, R.D.; Mehling, W.E.; et al. Interoception and Mental Health: A Roadmap. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Dunn, B.D.; Stefanovitch, I.; Evans, D.; Oliver, C.; Hawkins, A.; Dalgleish, T. Can you feel the beat? Interoceptive awareness is an interactive function of anxiety- and depression-specific symptom dimensions. Behav. Res. Ther. 2010, 48, 1133–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, D.; Berberich, G.; Zaudig, M.; Krauseneck, T.; Weiss, S.; Pollatos, O. Interoceptive Processes in Anorexia Nervosa in the Time Course of Cognitive-Behavioral Therapy: A Pilot Study. Front. Psychiatry 2016, 7, 199. [Google Scholar] [CrossRef] [Green Version]
- Paulus, M.P.; Stein, M.B. Interoception in anxiety and depression. Brain Struct. Funct. 2010, 214, 451–463. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, M.; Egloff, B.; Gerlach, A.L.; Witthöft, M. Improving heartbeat perception in patients with medically unexplained symptoms reduces symptom distress. Biol. Psychol. 2014, 101, 69–76. [Google Scholar] [CrossRef]
- Schultchen, D.; Zaudig, M.; Krauseneck, T.; Berberich, G.; Pollatos, O. Interoceptive deficits in patients with obsessive-compulsive disorder in the time course of cognitive-behavioral therapy. PLoS ONE 2019, 14, e0217237. [Google Scholar] [CrossRef] [Green Version]
- Eschulz, A. Interoception and stress. Front. Psychol. 2015, 6, 993. [Google Scholar] [CrossRef] [Green Version]
- Füstös, J.; Gramann, K.; Herbert, B.; Pollatos, O. On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Soc. Cogn. Affect. Neurosci. 2013, 8, 911–917. [Google Scholar] [CrossRef] [Green Version]
- Herbert, B.M.; Herbert, C.; Pollatos, O. On the Relationship Between Interoceptive Awareness and Alexithymia: Is Interoceptive Awareness Related to Emotional Awareness? J. Pers. 2011, 79, 1149–1175. [Google Scholar] [CrossRef] [PubMed]
- Furman, D.J.; Waugh, C.; Bhattacharjee, K.; Thompson, R.J.; Gotlib, I.H. Interoceptive awareness, positive affect, and decision making in Major Depressive Disorder. J. Affect. Disord. 2013, 151, 780–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terhaar, J.; Viola, F.C.; Bär, K.-J.; Debener, S. Heartbeat evoked potentials mirror altered body perception in depressed patients. Clin. Neurophysiol. 2012, 123, 1950–1957. [Google Scholar] [CrossRef] [PubMed]
- Dunn, B.D.; Dalgleish, T.; Ogilvie, A.D.; Lawrence, A.D. Heartbeat perception in depression. Behav. Res. Ther. 2007, 45, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Ewing, D.L.; Manassei, M.; van Praag, C.G.; Philippides, A.; Critchley, H.; Garfinkel, S.N. Sleep and the heart: Interoceptive differences linked to poor experiential sleep quality in anxiety and depression. Biol. Psychol. 2017, 127, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Fava, M.; Abraham, M.; Clancy-Colecchi, K.; Pava, J.A.; Matthews, J.; Rosenbaum, J.F. Eating Disorder Symptomatology in Major Depression. J. Nerv. Ment. Dis. 1997, 185, 140–144. [Google Scholar] [CrossRef]
- Wiebking, C.; de Greck, M.; Duncan, N.; Tempelmann, C.; Bajbouj, M.; Northoff, G. Interoception in insula subregions as a possible state marker for depression—an exploratory fMRI study investigating healthy, depressed and remitted participants. Front. Behav. Neurosci. 2015, 9, 82. [Google Scholar] [CrossRef] [Green Version]
- Ainley, V.; Tajadura-Jimenez, A.; Fotopoulou, A.; Tsakiris, M. Looking into myself: Changes in interoceptive sensitivity during mirror self-observation. Psychophysiology 2012, 49, 1672–1676. [Google Scholar] [CrossRef] [Green Version]
- Meyerholz, L.; Irzinger, J.; Witthöft, M.; Gerlach, A.L.; Pohl, A. Contingent biofeedback outperforms other methods to enhance the accuracy of cardiac interoception: A comparison of short interventions. J. Behav. Ther. Exp. Psychiatry 2019, 63, 12–20. [Google Scholar] [CrossRef]
- Parkin, L.; Morgan, R.; Rosselli, A.; Howard, M.; Sheppard, A.; Evans, D.; Hawkins, A.; Martinelli, M.; Golden, A.-M.; Dalgleish, T.; et al. Exploring the Relationship Between Mindfulness and Cardiac Perception. Mindfulness 2014, 5, 298–313. [Google Scholar] [CrossRef]
- Pollatos, O.; Herbert, B.; Berberich, G.; Zaudig, M.; Krauseneck, T.; Tsakiris, M. Atypical Self-Focus Effect on Interoceptive Accuracy in Anorexia Nervosa. Front. Hum. Neurosci. 2016, 10, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weineck, F.; Messner, M.; Hauke, G.; Pollatos, O. Improving interoceptive ability through the practice of power posing: A pilot study. PLoS ONE 2019, 14, e0211453. [Google Scholar] [CrossRef] [PubMed]
- Bornemann, B.; Herbert, B.; Mehling, W.E.; Singer, T. Differential changes in self-reported aspects of interoceptive awareness through 3 months of contemplative training. Front. Psychol. 2015, 5, 1504. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.; Lazar, S.W.; Hug, K.; Mehling, W.E.; Hölzel, B.K.; Sack, A.T.; Peeters, F.; Ashih, H.; Mischoulon, D.; Gard, T. Effects of Mindfulness-Based Cognitive Therapy on Body Awareness in Patients with Chronic Pain and Comorbid Depression. Front. Psychol. 2016, 7, 967. [Google Scholar] [CrossRef] [Green Version]
- Fissler, M.; Winnebeck, E.; Schroeter, T.; Gummersbach, M.; Huntenburg, J.M.; Gaertner, M.; Barnhofer, T. An Investigation of the Effects of Brief Mindfulness Training on Self-Reported Interoceptive Awareness, the Ability to Decenter, and Their Role in the Reduction of Depressive Symptoms. Mindfulness 2016, 7, 1170–1181. [Google Scholar] [CrossRef]
- Kok, B.E.; Singer, T. Phenomenological Fingerprints of Four Meditations: Differential State Changes in Affect, Mind-Wandering, Meta-Cognition, and Interoception Before and After Daily Practice Across 9 Months of Training. Mindfulness 2017, 8, 218–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, C.J.; Hooven, C. Interoceptive Awareness Skills for Emotion Regulation: Theory and Approach of Mindful Awareness in Body-Oriented Therapy (MABT). Front. Psychol. 2018, 9, 798. [Google Scholar] [CrossRef] [Green Version]
- Dobson, K.S.; Dozois, D.J.A. Historical and Philosophical Bases of the Cognitive-Behavioral Therapies; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Dirubbo, N. Full Catastrophe Living: The program of the Stress Reduction Clinic at the University of Massachusetts Medical Center. Nurse Pr. 1992, 17, 78. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Kappen, H. Gesund Durch Meditation: Das Große Buch Der Selbstheilung; Mit MBSR; Knaur-Taschenbuch: Munich, Germany, 2013. [Google Scholar]
- Batchelor, M. Meditation and mindfulness. Contemp. Buddhism 2011, 12, 157–164. [Google Scholar] [CrossRef]
- Williams, J.M.G.; Kuyken, W. Mindfulness-based cognitive therapy: A promising new approach to preventing depressive relapse. Br. J. Psychiatry 2012, 200, 359–360. [Google Scholar] [CrossRef]
- Bornemann, B.; Singer, T. Taking time to feel our body: Steady increases in heartbeat perception accuracy and decreases in alexithymia over 9 months of contemplative mental training. Psychophysiology 2017, 54, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.M.; Saab, B.J.; Farb, N.A. Effects of a Mindfulness Meditation App on Subjective Well-Being: Active Randomized Controlled Trial and Experience Sampling Study. JMIR Ment. Heal. 2019, 6, e10844. [Google Scholar] [CrossRef]
- Price, C.J.; Thompson, E.A.; Crowell, S.E.; Pike, K.; Cheng, S.C.; Parent, S.; Hooven, C. Immediate effects of interoceptive awareness training through Mindful Awareness in Body-oriented Therapy (MABT) for women in substance use disorder treatment. Subst. Abus. 2018, 40, 102–115. [Google Scholar] [CrossRef]
- Internationale Klassifikation Psychischer Störungen, ICD-10 Kapitel V (F), Klinisch-diagnostische Leitlinien, 10th ed.; Dilling, H.; Mombour, W.; Schmidt, M.H. (Eds.) Hogrefe AG: Bern, Switzerland, 2015. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; TX Psychol. Corp.: San Antonio, TX, USA, 1996. [Google Scholar]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hautzinger, M.; Keller, F.; Kühner, C. BDI II Beck Depressions-Inventar Revision Manual; Pearson: New York, NY, USA, 2006. [Google Scholar]
- Erford, B.T.; Johnson, E.; Bardoshi, G. Meta-Analysis of the English Version of the Beck Depression Inventory-Second Edition. Meas. Eval. Couns. Dev. 2016, 49, 3–33. [Google Scholar] [CrossRef]
- Michalak, J.; Burg, J.; Heidenreich, T. Don’t Forget Your Body: Mindfulness, Embodiment, and the Treatment of Depression. Mindfulness 2012, 3, 190–199. [Google Scholar] [CrossRef]
- Michalak, J.; Heidenreich, T.; Ströhle, G.; Nachtigall, C. Die deutsche Version der Mindful Attention and Awareness Scale (MAAS) Psychometrische Befunde zu einem Achtsamkeitsfragebogen. Z Klin. Psychol. Psychother. 2008, 37, 200–208. [Google Scholar] [CrossRef]
- Alleva, J.; Roelofs, J.; Voncken, M.; Meevissen, Y.; Alberts, H. On the Relation Between Mindfulness and Depressive Symptoms: Rumination as a Possible Mediator. Mindfulness 2014, 5, 72–79. [Google Scholar] [CrossRef]
- Kever, A.; Pollatos, O.; Vermeulen, N.; Grynberg, D. Interoceptive sensitivity facilitates both antecedent- and response-focused emotion regulation strategies. Pers. Individ. Differ. 2015, 87, 20–23. [Google Scholar] [CrossRef]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness. PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, D.; Messner, M.; Pollatos, O. Improvement of Interoceptive Processes after an 8-Week Body Scan Intervention. Front. Hum. Neurosci. 2017, 11, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnhofer, T.; Duggan, D.S.; Griffith, J.W. Dispositional mindfulness moderates the relation between neuroticism and depressive symptoms. Pers. Individ. Differ. 2011, 51, 958–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burg, J.M.; Michalak, J. The Healthy Quality of Mindful Breathing: Associations with Rumination and Depression. Cogn. Ther. Res. 2011, 35, 179–185. [Google Scholar] [CrossRef]
- Deng, Y.-Q.; Li, S.; Tang, Y.-Y. The Relationship Between Wandering Mind, Depression and Mindfulness. Mindfulness 2014, 5, 124–128. [Google Scholar] [CrossRef]
- Pollatos, O.; Traut-Mattausch, E.; Schandry, R. Differential effects of anxiety and depression on interoceptive accuracy. Depression Anxiety 2009, 26, 167–173. [Google Scholar] [CrossRef]
- Kapfhammer, H.P. Somatic symptoms in depression. Dialogues Clin. Neurosci. 2006, 8, 227. [Google Scholar] [CrossRef]
- Wang, N.; Ren, F.; Zhou, X. Factor Structure and Psychometric Properties of the Body Perception Questionnaire–Short Form (BPQ-SF) Among Chinese College Students. Front. Psychol. 2020, 11, 1355. [Google Scholar] [CrossRef]
- Wiebking, C.; Bauer, A.; de Greck, M.; Duncan, N.; Tempelmann, C.; Northoff, G. Abnormal body perception and neural activity in the insula in depression: An fMRI study of the depressed “material me”. World J. Biol. Psychiatry 2010, 11, 538–549. [Google Scholar] [CrossRef]
- Quadt, L.; Critchley, H.; Garfinkel, S.N. The neurobiology of interoception in health and disease. Ann. N. Y. Acad. Sci. 2018, 1428, 112–128. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Depressive Patients (n = 60) | Healthy Controls (n = 52) | t(df) | p | d | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Age | 41.35 | 11.16 | 40.85 | 11.19 | −24(110) | 0.406 | −0.05 |
| BDI | 22.25 | 8.77 | 5.19 | 4.61 | −13.11(91.87) | 0.001 | −2.39 |
| MAAS | 3.16 | 0.81 | 4.29 | 0.73 | 7.75(110) | 0.001 | 1.45 |
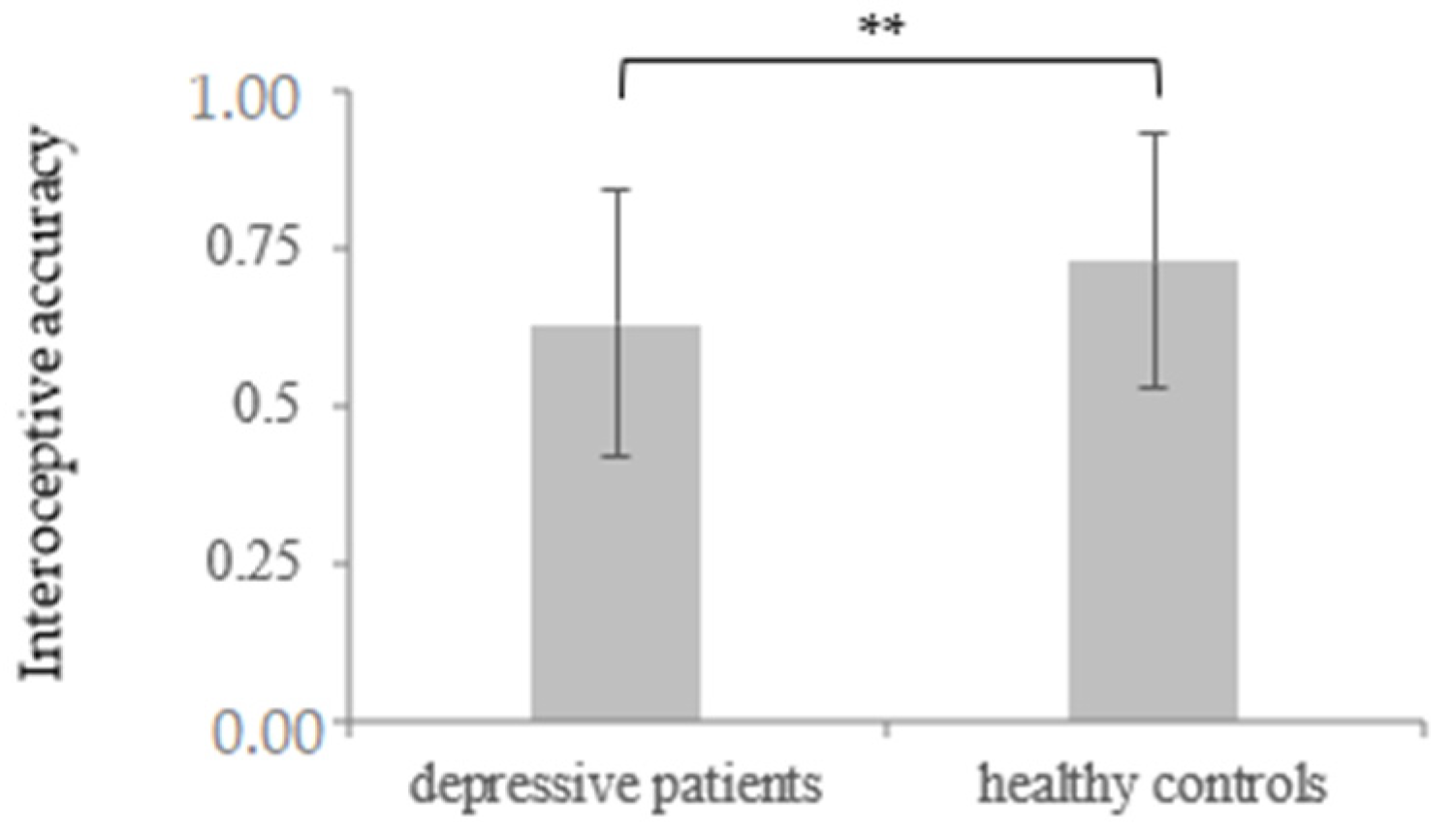
| IAcc | 0.63 | 0.21 | 0.73 | 0.19 | 2.64(110) | 0.005 | 0.50 |
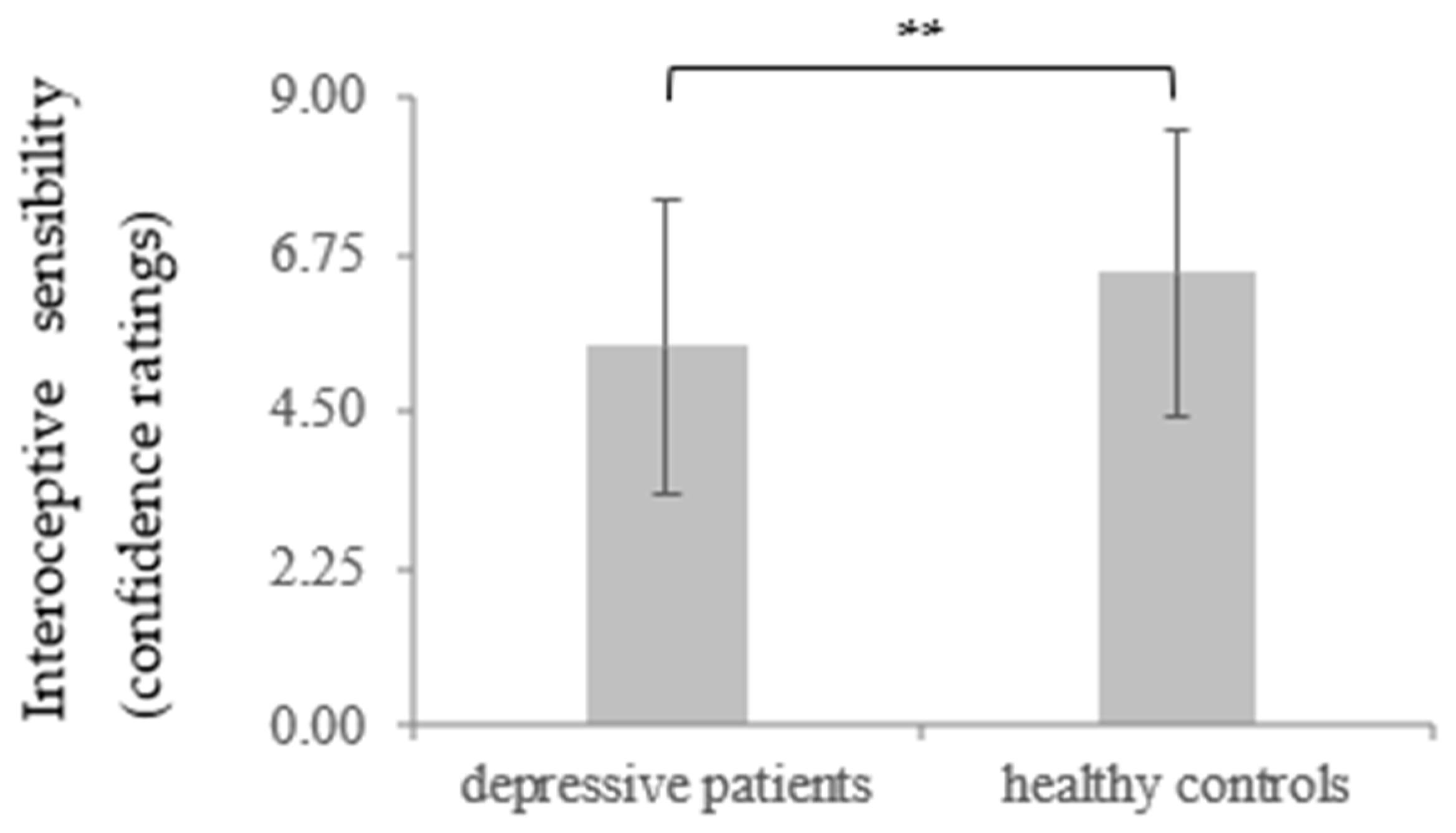
| IS conf | 5.43 | 2.08 | 6.49 | 2.02 | 2.75(110) | 0.004 | 0.52 |
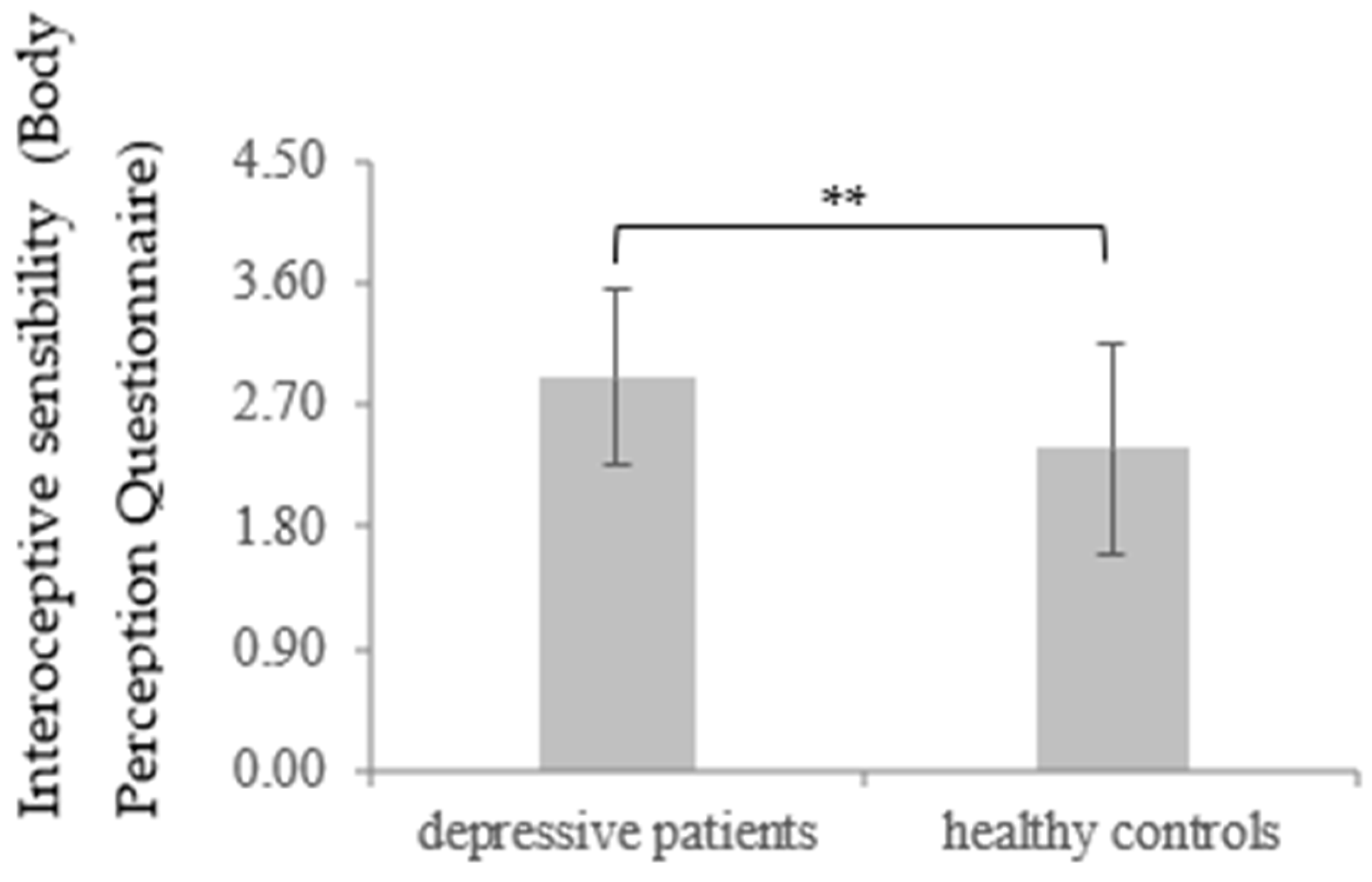
| IS BPQ | 2.91 | 0.66 | 2.38 | 1.01 | −3.23(85.97) | 0.001 | −0.63 |
| Depressive Patients (n = 60) | Healthy Controls (n = 52) | |||||
|---|---|---|---|---|---|---|
| t1 | t2 | |||||
| M | SD | M | SD | M | SD | |
| BDI | 22.25 | 8.77 | 15.58 | 9.15 | 5.19 | 4.61 |
| MAAS | 3.16 | 0.81 | 3.66 | 0.81 | 4.29 | 0.73 |
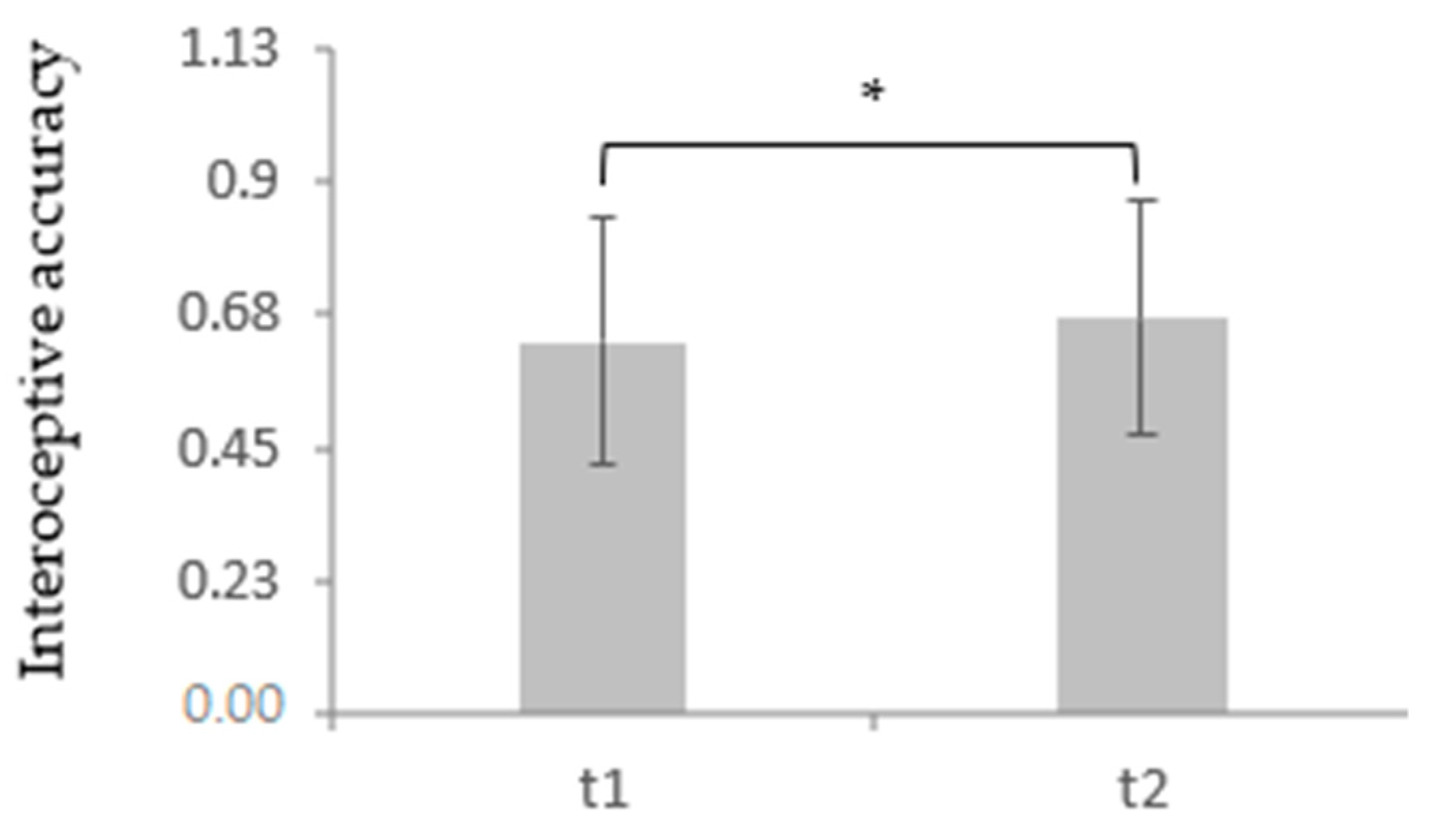
| IAcc | 0.63 | 0.21 | 0.67 | 0.20 | 0.73 | 0.19 |
| IS conf | 5.43 | 2.08 | 5.90 | 2.05 | 6.50 | 2.02 |
| IS BPQ | 2.91 | 0.66 | 2.78 | 0.78 | 2.38 | 1.01 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. BDI t1 | 1 | 0.727 ** | −0.408 ** | −0.473 ** | −0.220 * | −0.034 | −0.082 | −0.253 * | 0.306 * | 0.299 * |
| 2. BDI t2 | 1 | −0.417 ** | −0.614 ** | −0.209 | −0.008 | −0.257 * | −0.195 | 0.215 * | 0.351 ** | |
| 3. MAAS t1 | 1 | 0.622 ** | 0.007 | −0.137 | −0.038 | −0.158 | −0.143 | −0.219 * | ||
| 4. MAAS t2 | 1 | −0.023 | −0.094 | −0.019 | 0.087 | −0.154 | 0.318 ** | |||
| 5. IAcc t1 | 1 | 0.678 ** | 0.359 ** | 0.349 ** | −0.114 | 0.186 | ||||
| 6. IAcc t2 | 1 | 0.061 | 0.303 ** | −0.110 | 0.152 | |||||
| 7. IS conf t1 | 1 | 0.541 ** | 0.117 | −0.048 | ||||||
| 8. IS conf t2 | 1 | 0.005 | −0.049 | |||||||
| 9. IS BPQ t1 | 1 | 0.806 ** | ||||||||
| 10. IS BPQ t2 | 1 |
| Variable | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. BDI | 1 | −0.365 ** | −0.112 | −0.014 | 0.080 |
| 2. MAAS | 1 | −0.079 | 0.265 * | 0.100 | |
| 3. IAcc | 1 | 0.338 ** | 0.028 | ||
| 4. IS conf | 1 | 0.047 | |||
| 5. IS BPQ | 1 |
| CBT (n = 30) | CBT + MBSR (n = 30) | t (df = 58) | p | d | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| BDI t1 | 21.70 | 9.09 | 22.80 | 8.56 | −0.48 | 0.315 | −0.13 |
| BDI t2 | 14.87 | 9.03 | 16.30 | 9.37 | −0.60 | 0.275 | −0.16 |
| MAAS t1 | 3.41 | 0.68 | 2.91 | 0.86 | 2.51 | 0.008 | 0.65 |
| MAAS t2 | 3.89 | 0.87 | 3.42 | 0.69 | 2.32 | 0.012 | 0.60 |
| IAcc t1 | 0.62 | 0.23 | 0.63 | 0.20 | −0.14 | 0.444 | −0.04 |
| IAcc t2 | 0.67 | 0.21 | 0.66 | 0.19 | 0.19 | 0.424 | 0.05 |
| IS conf t1 | 5.56 | 2.13 | 5.29 | 2.05 | 0.49 | 0.312 | 0.13 |
| IS conf t2 | 6.08 | 1.85 | 5.72 | 2.25 | 0.69 | 0.247 | 0.18 |
| IS BPQ t1 | 3.06 | 0.72 | 2.75 | 0.57 | 1.81 | 0.038 | 0.47 |
| IS BPQ t2 | 2.85 | 0.91 | 2.70 | 0.63 | 0.74 | 0.232 | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karanassios, G.; Schultchen, D.; Möhrle, M.; Berberich, G.; Pollatos, O. The Effects of a Standardized Cognitive-Behavioural Therapy and an Additional Mindfulness-Based Training on Interoceptive Abilities in a Depressed Cohort. Brain Sci. 2021, 11, 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101355
Karanassios G, Schultchen D, Möhrle M, Berberich G, Pollatos O. The Effects of a Standardized Cognitive-Behavioural Therapy and an Additional Mindfulness-Based Training on Interoceptive Abilities in a Depressed Cohort. Brain Sciences. 2021; 11(10):1355. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101355
Chicago/Turabian StyleKaranassios, Georgios, Dana Schultchen, Matthias Möhrle, Götz Berberich, and Olga Pollatos. 2021. "The Effects of a Standardized Cognitive-Behavioural Therapy and an Additional Mindfulness-Based Training on Interoceptive Abilities in a Depressed Cohort" Brain Sciences 11, no. 10: 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101355