
Advanced Parkinson’s Disease Treatment Simplification and Long-Term Outcomes with Levodopa Carbidopa Intestinal Gel: COSMOS Romanian Subanalysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Objectives
2.3. LCIG Monotherapy and Group Stratification
2.4. Study Population
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Study Center and Physician Characteristics
3.2. Description of the Study Population
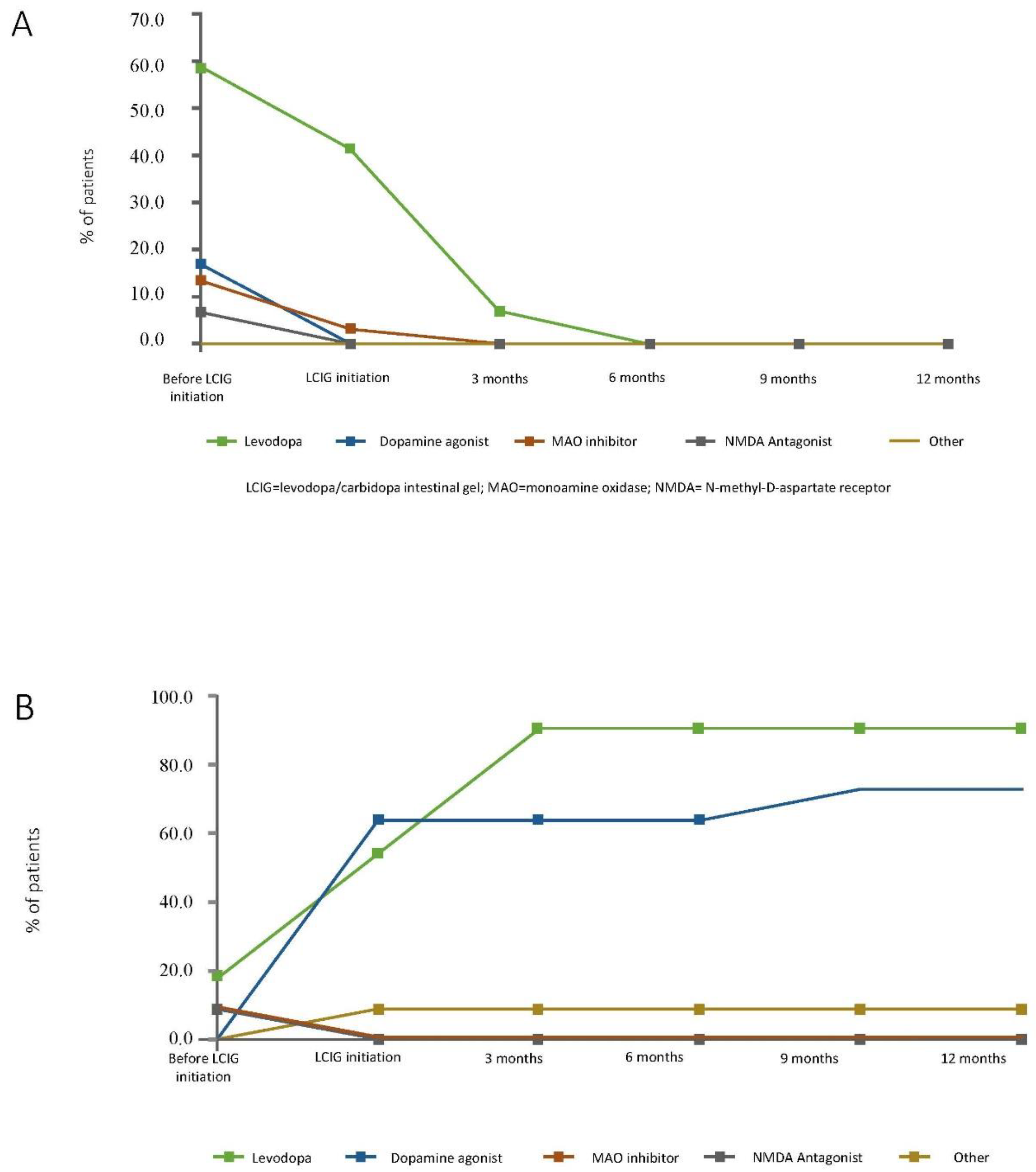
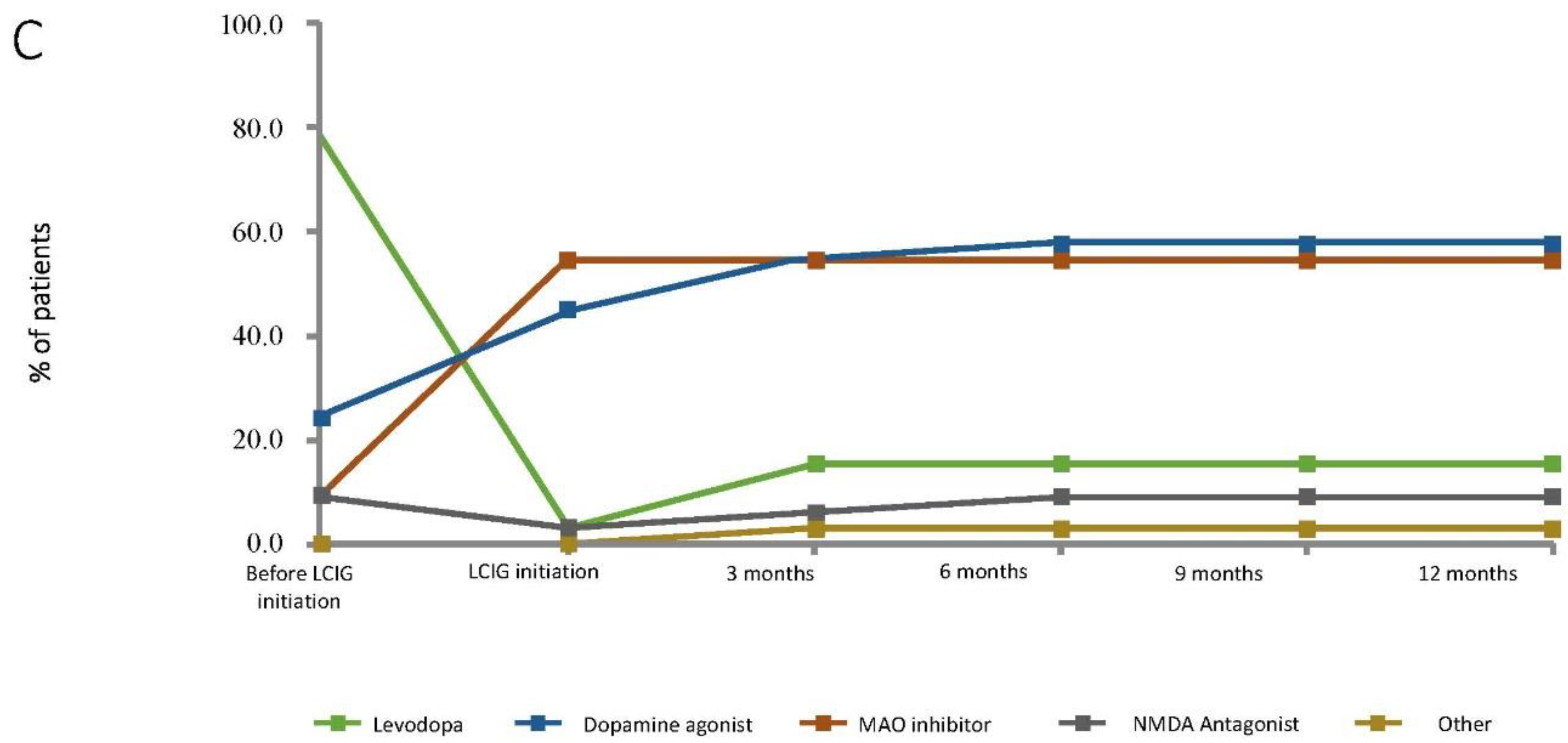
Conventional Treatment at LCIG Initiation
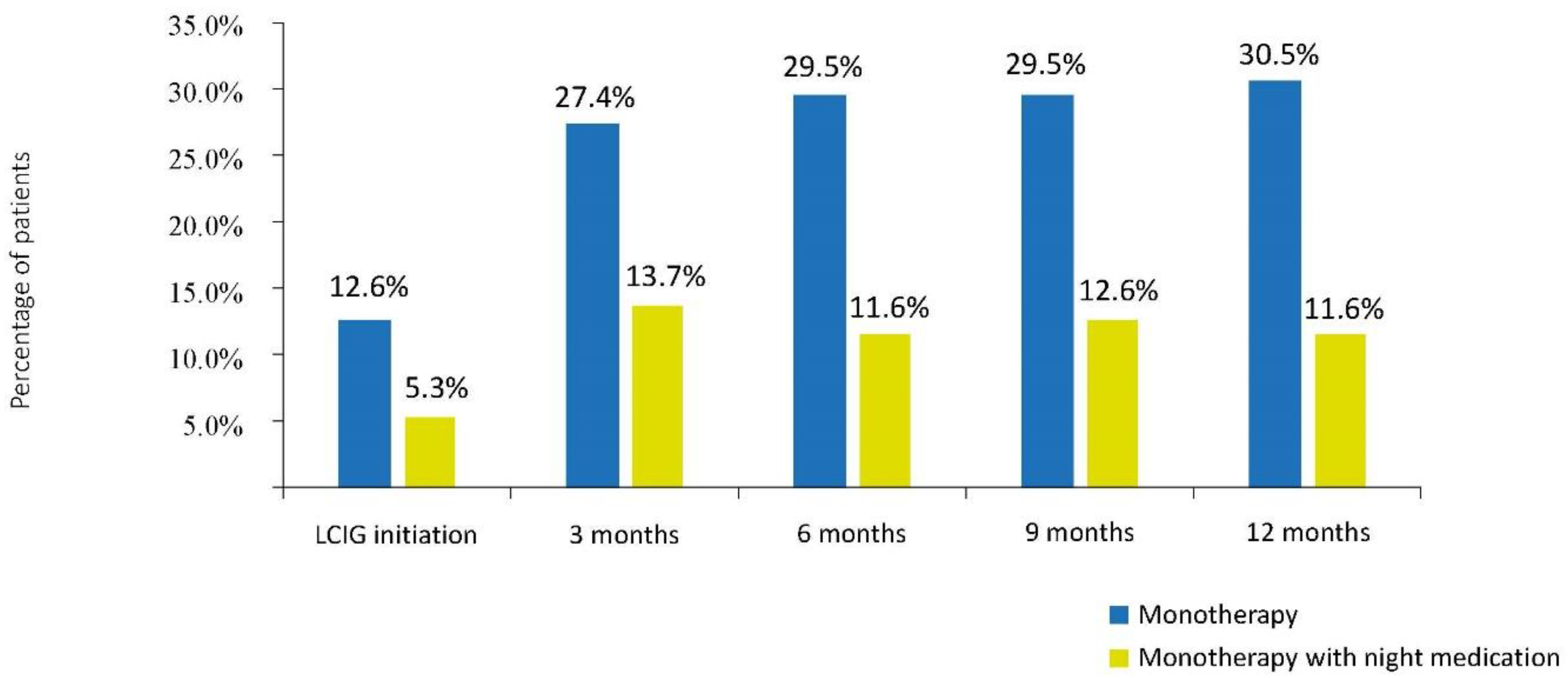
3.3. Frequency of Monotherapy, Time to Monotherapy, and Monotherapy Duration
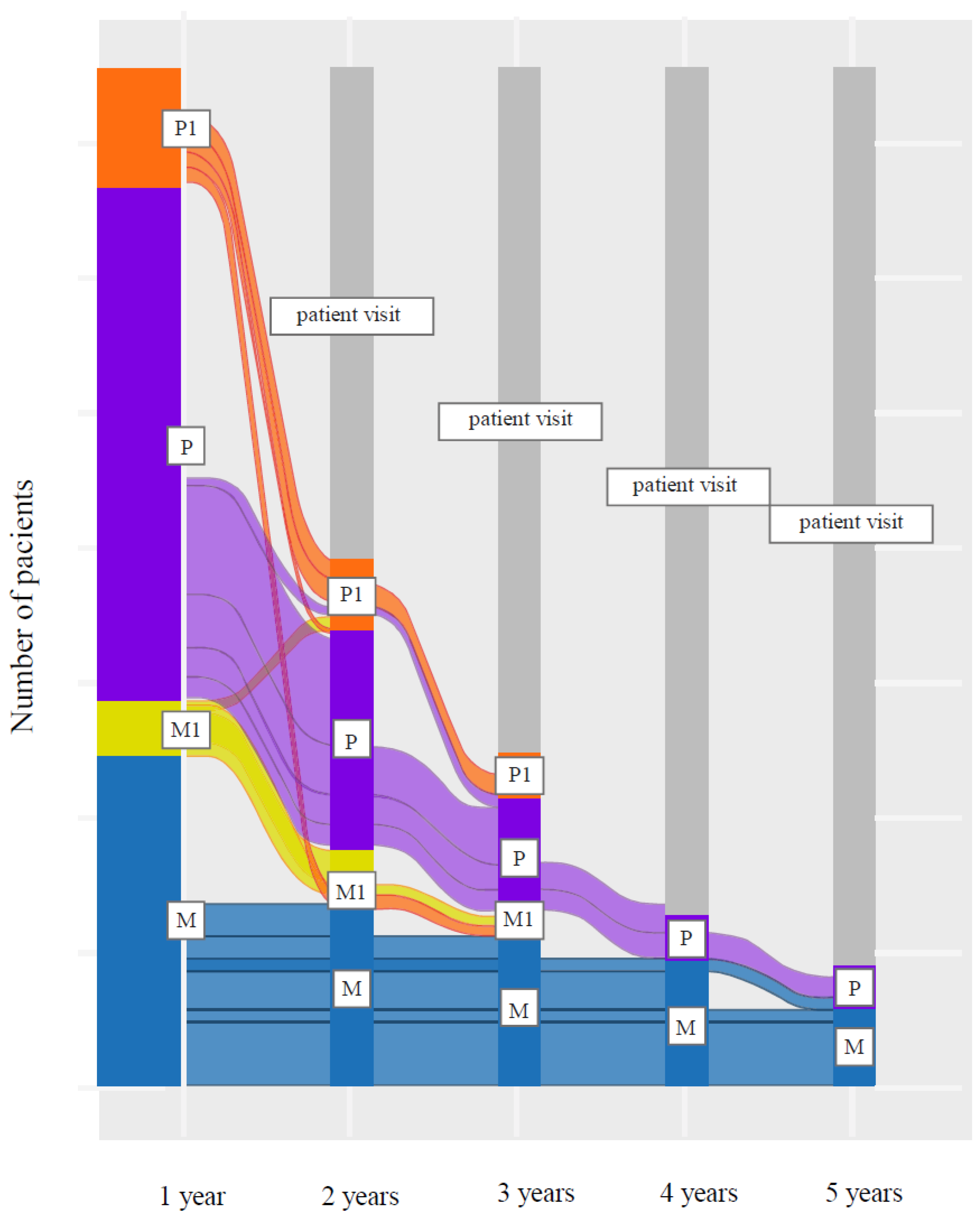
3.4. LCIG Infusion Monotherapy and Add-On Therapy during Follow-Up
3.5. Patient and Physician-Reported Outcomes
3.6. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olanow, W. Levodopa is the best symptomatic therapy for PD: Nothing more, nothing less. Mov. Disord. 2019, 34, 812–815. [Google Scholar] [CrossRef]
- Wirdefeldt, K.; Odin, P.; Nyholm, D. Levodopa/carbidopa intestinal gel in patients with Parkinson’s disease: A systematic review. CNS Drugs 2016, 30, 381–404. [Google Scholar] [CrossRef]
- Chase, T.N. Levodopa therapy: Consequences of the nonphysiologic replacement of dopamine. Neurology 1998, 50 (Suppl. 5), S17–S25. [Google Scholar] [CrossRef]
- Olanow, C.W.; Obeso, J.A. Preventing levodopa-induced dyskinesias. Ann. Neurol 2000, 47 (Suppl. 1), S167–S176. [Google Scholar] [PubMed]
- Chase, T.N.; Mouradian, M.M.; Engber, T.M. Motor response complications and the function of striatal efferent systems. Neurology 1993, 43 (Suppl. 6), S23–S27. [Google Scholar]
- Contin, M.; Martinelli, P. Pharmacokinetics of levodopa. J. Neurol 2010, 257 (Suppl. 2), S253–S261. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Poewe, W.; Chaudhuri, K.R.; Jech, R.; Pickut, B.; Pirtošek, Z.; Szasz, J.; Valldeoriola, F.; Winkler, C.; Bergmann, L.; et al. Levodopa/carbidopa intestinal gel in advanced Parkinson’s disease: Final results of the GLORIA registry. Parkinsonism Relat. Disord. 2017, 45, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyholm, D.; Askmark, H.; Gomes-Trolin, C.; Knutson, T.; Lennernas, H.; Nystrom, C.; Aquilonius, S.M. Optimizing levodopa pharmacokinetics: Intestinal infusion versus oral sustained- release tablets. Clin. Neuropharmacol. 2003, 26, 156–163. [Google Scholar] [CrossRef]
- Nyholm, D.; Odin, P.; Johansson, A.; Chatamra, K.; Locke, C.; Dutta, S.; Othman, A. Pharmacokinetics of levodopa, carbidopa, and 3-O-methyldopa following 16-hour jejunal infusion of levodopa-carbidopa intestinal gel in advanced Parkinson’s disease patients. AAPS J. 2013, 15, 316–323. [Google Scholar] [CrossRef] [Green Version]
- Nyholm, D.; Nilsson Remahl, A.I.; Dizdar, N.; Constantinescu, R.; Holmberg, B.; Jansson, R.; Aquilonius, S.M.; Askmark, H. Duodenal levodopa infusion monotherapy vs oral polypharmacy in advanced Parkinson disease. Neurology 2005, 64, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Annic, A.; Devos, D.; Seguy, D.; Dujardin, K.; Destee, A.; Defebvre, L. Continuous dopaminergic stimulation by duodopa in advanced Parkinson’s disease: Efficacy and safety. Rev. Neurol. 2009, 165, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Antonini, A.; Mancini, F.; Canesi, M.; Zangaglia, R.; Isaias, I.U.; Manfredi, L.; Pacchetti, C.; Zibetti, M.; Natuzzi, F.; Lopiano, L.; et al. Duodenal levodopa infusion improves quality of life in advanced Parkinson’s disease. Neurodegener. Dis. 2008, 5, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Nyholm, D.; Lennernas, H.; Gomes-Trolin, C.; Aquilonius, S.M. Levodopa pharmacokinetics and motor performance during activities of daily living in patients with Parkinson’s disease on individual drug combinations. Clin. Neuropharmacol. 2002, 25, 89–96. [Google Scholar] [CrossRef]
- Nyholm, D.; Lewander, T.; Johansson, A.; Lewitt, P.A.; Lundqvist, C.; Aquilonius, S.M. Enteral levodopa/carbidopa infusion in advanced Parkinson disease: Long-term exposure. Clin. Neuropharmacol. 2008, 31, 63–73. [Google Scholar] [CrossRef]
- Bajenaru, O.; Ene, A.; Popescu, B.O.; Szasz, J.A.; Sabau, M.; Muresan, D.F.; Perju-Dumbrava, L.; Popescu, C.D.; Constantinescu, A.; Buraga, I.; et al. The effect of levodopa–carbidopa intestinal gel infusion long-term therapy on motor complications in advanced Parkinson’s disease: A multicenter Romanian experience. J. Neural Transm. 2016, 123, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonini, A.; Robieson, W.Z.; Bergmann, L.; Uegin, A.; Poewe, W. Age/disease duration influence on activities of daily living and quality of life after levodopa-carbidopa intestinal gel in Parkinson’s disease. Neurodegener. Dis. Manag. 2018, 8, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, H.H.; Boyd, J.T.; Fung, V.S.C.; Lew, M.F.; Rodriguez, R.L.; Slevin, J.T.; Standaert, D.G.; Zadikoff, C.; Vanagunas, A.D.; Chatamra, K.; et al. Long-term safety and efficacy of levodopa/carbidopa intestinal gel in advanced Parkinson’s disease. Mov. Disord. 2018, 33, 928–936. [Google Scholar] [CrossRef]
- Slevin, J.T.; Fernandez, H.H.; Zadikoff, C.; Hall, C.; Eaton, S.; Dubow, J.; Chatamra, K.; Benesh, J. Long-term safety and maintenance of efficacy of levodopa-carbidopa intestinal gel: An open-label extension of the double-blind pivotal study in advanced Parkinson’s disease patients. J. Parkinsons Dis. 2015, 5, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Fleisher, J.E.; Stern, M.B. Medication nonadherence in Parkinson’s disease. Curr. Neurol. Neurosci. Rep. 2013, 13, 382. [Google Scholar] [CrossRef] [Green Version]
- Davis, K.L.; Edin, H.M.; Allen, J.K. Prevalence and cost of medication nonadherence in Parkinson’s disease: Evidence from administrative claims data. Mov. Disord. 2010, 25, 474–480. [Google Scholar] [CrossRef]
- Olanow, C.W.; Kieburtz, K.; Odin, P.; Espay, A.J.; Standaert, D.G.; Fernandez, H.H.; Vanagunas, A.; Othman, A.A.; Widnell, K.L.; Robieson, W.Z.; et al. Continuous intrajejunal infusion of levodopa/carbidopa intestinal gel for patients with advanced Parkinson’s disease: A randomised, controlled, double-blind, double-dummy study. Lancet Neurol. 2014, 13, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, H.H.; Standaert, D.G.; Hauser, R.A.; Lang, A.E.; Fung, V.S.; Klostermann, F.; Lew, M.F.; Odin, P.; Steiger, M.; Yakupov, E.Z.; et al. Levodopa/carbidopa intestinal gel in advanced Parkinson’s disease: Final 12-month, open-label results. Mov. Disord. 2015, 30, 500–509. [Google Scholar] [CrossRef]
- Lopiano, L.; Modugno, N.; Marano, P.; Sensi, M.; Meco, G.; Solla, P.; Gusmaroli, G.; Tamma, F.; Mancini, F.; Quatrale, R.; et al. Motor and non-motor outcomes in patients with advanced Parkinson’s disease treated with levodopa/carbidopa intestinal gel: Final results of the GREENFIELD observational study. J. Neurol. 2019, 266, 2164–2176. [Google Scholar] [CrossRef] [Green Version]
- Boyd, J.; Zadikoff, C.; Benesh, J.; Zamudio, J.; Robieson, W.Z.; Kukreja, P.; Yokoyama, M.; Siddiqui, M.S. A post hoc comparison of levodopa/carbidopa intestinal gel daytime monotherapy vs polytherapy safety and efficacy in patients with advanced Parkinson’s disease: Results from 6 phase 3/3b open-label studies. Clin. Parkinsonism Relat. Disord. 2020, 2, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Bergmann, L.; Kukreja, P.; Robieson, W.Z.; Antonini, A. Levodopa/carbidopa intestinal gel monotherapy: GLORIA registry demographics, efficacy, and safety. J. Parkinsons Dis. 2019, 9, 531–541. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A.; Gurevich, T.; Jech, R.; Kovács, N.; Svenningsson, P.; Szász, J.; Parra, J.C.; Bergmann, L.; Johnson, A.; Sanchez-Soliño, O.; et al. Concomitant medication usage with levodopa/carbidopa intestinal gel: Results from the COSMOS study. Mov. Disord. 2021, 36, 1853–1862. [Google Scholar] [CrossRef]
- Jenkinson, C.; Fitzpatrick, R. Cross-cultural evaluation of the short form 8-item Parkinson’s Disease Questionnaire (PDQ-8): Results from America, Canada, Japan, Italy and Spain. Parkinsonism Relat. Disord. 2007, 13, 22–28. [Google Scholar] [CrossRef]
- Weintraub, D.; Mamikonyan, E.; Papay, K.; Shea, J.A.; Xie, S.X.; Siderowf, A. Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale. Mov. Disord. 2012, 27, 242–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trenkwalder, C.; Kohnen, R.; Hogl, B.; Metta, V.; Sixel-Döring, F.; Frauscher, B.; Hülsmann, J.; Martinez-Martin, P.; Chaudhuri, K.R. Parkinson’s disease sleep scale—Validation of the revised version PDSS-2. Mov. Disord. 2011, 26, 644–652. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J.; Hankins, M. The Beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Martinez-Martin, P.; Schapira, A.H.; Stocchi, F.; Sethi, K.; Odin, P.; Brown, R.G.; Koller, W.; Barone, P.; MacPhee, G.; et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: The NMSQuest study. Mov. Disord. 2006, 21, 916–923. [Google Scholar] [CrossRef]
- Molloy, D.W.; Standish, T.I. A guide to the standardized Mini-Mental State Examination. Int. Psychogeriatr. 1997, 9 (Suppl. 1), 87–94. [Google Scholar] [CrossRef]
- Szasz, J.A.; Orban-Kis, K.; Constantin, V.A.; Peter, C.; Biro, I.; Mihaly, I.; Szegedi, K.; Antal, B.; Szatmari, S. Therapeutic strategies in the early stages of Parkinson’s disease: A cross-sectional evaluation of 15 years’ experience with a large cohort of Romanian patients. Neuropsychiatr. Dis. Treat. 2019, 15, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Szasz, J.A.; Constantin, V.A.; Orban-Kis, K.; Racz, A.; Bancu, L.A.; Georgescu, D.; Szedejesi, J.; Mihaly, I.; Farr, A.-M.; Kelemen, K.; et al. Profile of patients with advanced Parkinson’s disease suitable for Device-Aided Therapies: Restrospective data of a large cohort of Romanian patients. Neuropsychiatr. Dis. Treat. 2019, 15, 3187–3195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantin, V.A.; Szasz, J.A.; Orban-Kis, K.; Rosca, E.C.; Popovici, M.; Cornea, A.; Bancu, L.A.; Ciorba, M.; Mihaly, I.; Nagy, E.; et al. Levodopa-carbidopa intestinal gel infusion therapy discontinuation: A ten-year retrospective analysis of 204 treated patients. Neuropsychiatr. Dis. Treat. 2020, 16, 1835–1844. [Google Scholar] [CrossRef] [PubMed]
- Szasz, J.A.; Constantin, V.A.; Mihaly, I.; Biro, I.; Peter, C.; Orban-Kis, K.; Szatmari, S. Dopamine agonists in Parkinson’s disease therapy—15 years of experience of the neurology clinics from Târgu Mures. A cross-sectional study. Ideggyogy Szle. 2019, 72, 187–193. [Google Scholar]
- Szasz, J.A.; Constantin, V.A.; Fazakas, P.; Blenyesi, E.; Grieb, L.; Balla, A.; Sarig, M.; Szegedi, K.; Barha, E.; Szatmári, S. The role of selective monoamine oxidase B inhibitors in the therapeutic strategy of Parkinson’s disease in the neurology clinics of Tirgu Mures County Emergency Clinical Hospital. Orv. Hetil. 2017, 158, 2023–2028. [Google Scholar] [PubMed]
- Szasz, J.A.; Constantin, V.A.; Orban-Kis, K.; Bancu, L.A.; Ciorba, M.; Mihaly, I.; Nagy, E.E.; Szasz, R.M.; Kelemen, K.; Simu, M.A.; et al. Management challenges of severe, complex dyskinesia. Data from a large cohort of patients treated with Levodopa-carbidopa intestinal gel for advanced Parkinson’s disease. Brain Sci. 2021, 11, 826. [Google Scholar] [CrossRef]
- Szasz, J.A.; Jianu, D.C.; Simu, M.A.; Constantin, V.A.; Dulamea, A.O.; Onuk, K.; Popescu, D.; Vasile, M.T.; Popescu, B.O.; Fasano, A.; et al. Characterizing advanced Parkinson’s disease: Romanian subanalysis from the OBSERVE-PD study. Parkinson’s Dis. 2021, 2021, 6635618. [Google Scholar] [CrossRef]
- Rosca, E.C.; Tudor, R.; Cornea, A.; Simu, M. Parkinson’s disease in Romania: A scoping review protocol. Brain Sci. 2021, 11, 251. [Google Scholar] [CrossRef]
- Rosca, E.C.; Tudor, R.; Cornea, A.; Simu, M. Parkinson’s disease in Romania: A scoping review. Brain Sci. 2021, 11, 709. [Google Scholar] [CrossRef] [PubMed]
- Terapia Interventionala in Boala Parkinson. Chapter in Current Diagnosis and Treatment of Parkinson’s Disease; Bajenaru, O., Ed.; Media Med Publicis: Bucharest, Romania, 2010; p. 135. (In Romanian) [Google Scholar]
- Bajenaru, O. Diagnosis and Treatment Guidelines in Neurology, 2nd ed.; Amaltea: Bucharest, Romania, 2009. (In Romanian) [Google Scholar]
- Szasz, J.A.; Szatmari, S.; Constantin, V.; Mihaly, I.; Racz, A.; Domokos, L.C.; Vajda, T.; Orban-Kis, K. Characteristics of levodopa treatment in advanced Parkinson’s disease in the experience of the neurology clinics of Târgu Mures, Romania. Orv. Hetil. 2019, 160, 662–669. [Google Scholar]
- Nyholm, D.; Johansson, A.; Lennernas, H.; Askmark, H. Levodopa infusion combined with entacapone or tolcapone in Parkinson disease: A pilot trial. Eur. J. Neurol. 2012, 19, 820–826. [Google Scholar] [CrossRef]
- Szasz, J.; Simu, M.; Perju-Dumbrava, L.; Antonini, A.; Bergmann, L.; Popescu, D.; Bajenaru, O.A. Efficacy, safety, and patient’s quality of life of long-term treatment with levodopa-carbidopa intestinal gel in advanced Parkinson’s disease in Romania: Results from GLORIA observational study. Rom. J. Neurol. 2020, 19, 27–35. [Google Scholar] [CrossRef]
- Odin, P.; Ray Chaudhuri, K.; Slevin, J.T.; Volkmann, J.; Dietrichs, E.; Martinez-Martin, P.; Krauss, J.K.; Henriksen, T.; Katzenschlager, R.; Antonini, A.; et al. Collective physician perspectives on non-oral medication approaches for the management of clinically relevant unresolved issues in Parkinson’s disease: Consensus from an international survey and discussion program. Parkinsonism Relat. Disord. 2015, 21, 1133–1144. [Google Scholar] [CrossRef] [Green Version]
- Antonini, A.; Stoessl, A.J.; Kleinman, L.S.; Skalicky, A.M.; Marshall, T.S.; Sail, K.R.; Onuk, K.; Odin, P.L.A. Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson’s disease: A multi-country Delphi-panel approach. Curr. Med. Res. Opin. 2018, 34, 2063–2073. [Google Scholar] [CrossRef]
- Tandberg, E.; Larsen, J.P.; Karlsen, K. A community-based study of sleep disorders in patients with Parkinson’s disease. Mov. Disord. 1998, 13, 895–899. [Google Scholar] [CrossRef]
- Thorpy, M.J. Sleep disorders in Parkinson’s disease. Clin. Cornerstone 2004, 6 (Suppl. 1A), S7–S15. [Google Scholar] [CrossRef]
- Friedman, J.H.; Chou, K.L. Sleep and fatigue in Parkinson’s disease. Parkinsonism Relat. Disord. 2004, 10 (Suppl. 1), S27–S35. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.D. Sleep in Parkinson’s disease. J. Psychosom. Res. 1998, 44, 613–617. [Google Scholar] [PubMed]
- Kurtis, M.M.; Rodriguez-Blazquez, C.; Martinez-Martin, P.; ELEP Group. Relationship between sleep disorders and other non-motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2013, 19, 1152–1155. [Google Scholar] [CrossRef] [PubMed]
- Zibetti, M.; Rizzone, M.; Merola, A.; Angrisano, S.; Rizzi, L.; Montanaro, E.; Cicolin, A.; Lopiano, L. Sleep improvement with levodopa/carbidopa intestinal gel infusion in Parkinson disease. Acta Neurol. Scand. 2013, 127, e28–e32. [Google Scholar] [CrossRef] [PubMed]
- Zibetti, M.; Romagnolo, A.; Merola, A.; Priano, L.; Montanaro, E.; Angrisano, S.; Tribolo, A.; Cicolin, A.; Lopiano, L. A polysomnographic study in parkinsonian patients treated with intestinal levodopa infusion. J. Neurol. 2017, 264, 1085–1090. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LCIG Monotherapy without Night Medication at 12 Months N = 29 | LCIG Monotherapy with Night Medication at 12 Months N = 11 | LCIG + Add-on Medication at 12 Months N = 33 | p-Value | |
|---|---|---|---|---|
| Before LCIG initiation | ||||
| Men, n (%) | 19 (65.5%) | 10 (90.9%) | 15 (45.5%) | 0.1083 * 0.1132 # |
| Education, n (%) | ||||
| Primary school Secondary school Professional education University | 8 (27.6%) 14 (48.3%) 3 (10.3%) 4 (13.8%) | 0 (0.0%) 4 (36.4%) 5 (45.5%) 2 (18.2%) | 13 (39.4%) 16 (48.5%) 2 (6.1%) 2 (6.1%) | 0.0401 * 0.5848 # |
| Primary occupation | ||||
| Retired On sick leave Unemployed Working full time | 27 (93.1) 0 (0.0) 2 (6.9) 0 (0.0) | 10 (90.9) 0 (0.0) 0 (0.0) 1 (9.1) | 29 (87.9) 1 (3.0) 3 (9.1) 0 (0.0) | 0.1828 * 0.6012 # |
| Age at PD diagnosis, years | 56.7 ± 10.0 | 57.7 ± 10.4 | 56.0 ± 8.4 | 0.8921 * 0.5004 # |
| Time from PD diagnosis to motor fluctuation onset, years | 6.3 ± 3.9 | 7.3 ± 5.6 | 5.5 ± 2.6 | 0.8846 * 0.3851 # |
| Time from PD diagnosis to morning akinesia, years | 7.6 ± 5.7 | 3.5 ± 1.7 | 6.8 ± 2.5 | 0.1486 * 1.0000 # |
| Time from PD diagnosis to dyskinesia, years | 7.9 ± 5.1 | 6.6 ± 5.3 | 8.1 ± 3.0 | 0.3731 * 0.5456 # |
| Morning akinesia | 17 (58.6) | 5 (45.5) | 28 (84.8) | 0.6915 * 0.0369 # |
| LCIG initiation | ||||
| Age at LCIG therapy initiation, years | 65.3 ± 7.8 | 67.0 ± 8.9 | 63.6 ± 8.6 | 0.5653 * 0.5154 # |
| Time from PD diagnosis to LCIG initiation, years | 10.7 ± 5.2 | 11.3 ± 6.0 | 9.5 ± 3.6 | 0.8723 * 0.5036 # |
| Reason for LCIG therapy initiation, n (%) | ||||
| Disabling motor fluctuations/Off periods Uncontrolled dyskinesia Lack of efficacy of previous treatment Decrease in quality of life | 28 (96.6%) 14 (48.3%) 5 (7.2%) 5 (17.2%) | 11 (100.0%) 6 (54.5%) 9 (81.8%) 9 (81.8%) | 33 (100.0%) 23 (69.7%) 3 (9.1%) 2 (6.1%) | |
| Dopamine agonists discontinued prior to considering LCIG initiation, n (%) | 14 (48.3%) | 7 (63.6%) | 8 (24.2%) | 0.385 * 0.0484 # |
| Study visit | ||||
| Age at study visit, years | 68.3 ± 7.1 | 69.5 ± 9.2 | 65.9 ± 8.4 | 0.8213 * 0.3549 # |
| Morning akinesia | 10 (34.5) | 0 (0.0) | 3 (9.1) | 0.0387 0.0301 |
| Wearing off, n (%) | 22 (75.9%) | 10 (90.9%) | 32 (97.0%) | 0.2881 * 0.0134 # |
| Dyskinesia, n (%) | 19 (65.5%) | 8 (72.7%) | 25 (75.8%) | 0.6638 * 0.3754 # |
| Co-morbidities at patient visit, n (%) | ||||
| Hypertension Cardiovascular disease Depression Cognitive dysfunction Sleep disorders Diabetes mellitus Chronic gastrointestinal disease Orthostatic hypotension Chronic pulmonary disease Fatigue Polyneuropathy/Neuropathy Any malignancy Skin disease | 5 (17.2%) 2 (6.9%) 4 (13.8%) 3 (10.3%) 1 (3.4%) 1 (3.4%) 0 (0.0%) 1 (3.4%) 0 (0.0%) 2 (6.9%) 1 (3.4%) 1 (3.4%) 0 (0.0%) | 7 (63.6%) 4 (36.4%) 3 (27.3%) 3 (27.3%) 5 (45.5%) 1 (9.1%) 2 (18.2%) 1 (9.1%) 1 (9.1%) 1 (9.1%) 0 (0.0%) 1 (9.1%) 1 (9.1%) | 7 (21.2%) 7 (21.2%) 2 (6.1%) 2 (6.1%) 1 (3.0%) 2 (6.1%) 1 (3.0%) 0 (0.0%) 2 (6.1%) 0 (0.0%) 1 (3.0%) 0 (0.0%) 0 (0.0%) | |
| Disease Characteristics | ≥1 to <2 Years | ≥2 to <3 Years | ≥3 to <4 Years | ≥4 to <5 Years | ≥5 Years |
|---|---|---|---|---|---|
| Duration of PD at LCIG initiation, mean number of years (SD) | 9.2 (4.7) N = 46 | 9.4 (5.1) N = 20 | 10.4 (5.8) N = 12 | 11.1 (8.0) N = 7 | 9.4 (3.6) N = 10 |
| “Off” time duration at LCIG initiation, mean number of hours/day (SD) | 6.7 (3.8) N = 35 | 6.0 (3.4) N = 10 | 6.5 (4.3) N = 10 | 5.0 (0.9) N = 6 | 4.8 (0.8) N = 5 |
| Duration of dyskinesia at LCIG initiation, mean number of hours/day (SD) | 2.0 (2.0) N = 36 | 3.9 (5.3) N = 11 | 2.7 (2.3) N = 10 | 2.2 (1.7) N = 6 | 3.4 (2.1) N = 5 |
| No or mild dyskinesia at LCIG initiation, N (%) | 9 (64.3%) N = 14 | 2 (66.6%) N = 3 | 0 N = 2 | 0 N = 4 | 1 (12.5%) N = 8 |
| Moderate to severe dyskinesia at LCIG initiation, N (%) | 4 (28.6%) N = 14 | 1 (33.3%) N = 3 | 2 (100%) N = 2 | 3 (75%) N = 4 | 5 (62.5%) N = 8 |
| UPDRS 5 at LCIG initiation—Stage 3 and 4, N (%) | 22 (100%) N = 22 | 8 (88.9%) N = 9 | 8 (100%) N = 8 | 4 (100%) N = 4 | 6 (85.7%) N = 7 |
| UPDRS 5 at LCIG initiation—Stage 5, N (%) | 0 N = 22 | 1 (11.1%) N = 9 | 0 N = 8 | 0 N = 4 | 1 (14.3%) N = 7 |
| n | % | Mean Change (Hours) | SD | Mean Change (%) | SD | |
|---|---|---|---|---|---|---|
| Change in “Off” time at 12 months from LCIG initiation | ||||||
| LCIG monotherapy | 13 | 31.7 | −3.2 | 2.5 | −56.3 | 30.6 |
| LCIG monotherapy + night medication | 3 | 7.3 | −8.0 | 2.6 | −80.6 | 4.8 |
| LCIG + add-on without night medication | 19 | 46.3 | −4.0 | 1.6 | −77.1 | 21.6 |
| LCIG + add-on including night medication | 6 | 14.6 | −9.0 | 4.8 | −74.0 | 23.9 |
| Total population | 41 | 100 | −4.8 | 3.3 | −70.3 | 25.7 |
| Change in time with dyskinesia at 12 months from LCIG initiation | ||||||
| LCIG monotherapy | 24 | 35.8 | 0.0 | 3.6 | 0.9 | 178.1 |
| LCIG monotherapy + night medication | 2 | 3.0 | 2.0 | 0.0 | 25.0 | N/A |
| LCIG + add-on without night medication | 33 | 49.2 | −1.0 | 1.9 | −56.6 | 36.1 |
| LCIG + add-on including night medication | 8 | 11.9 | −1.5 | 6.9 | 2.4 | 110.7 |
| Total population | 67 | 100 | −0.6 | 3.4 | −25.2 | 118.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simu, M.A.; Jianu, D.C.; Dulamea, A.O.; Constantin, V.A.; Popescu, D.; Parra, J.C.; Szász, J.A. Advanced Parkinson’s Disease Treatment Simplification and Long-Term Outcomes with Levodopa Carbidopa Intestinal Gel: COSMOS Romanian Subanalysis. Brain Sci. 2021, 11, 1566. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121566
Simu MA, Jianu DC, Dulamea AO, Constantin VA, Popescu D, Parra JC, Szász JA. Advanced Parkinson’s Disease Treatment Simplification and Long-Term Outcomes with Levodopa Carbidopa Intestinal Gel: COSMOS Romanian Subanalysis. Brain Sciences. 2021; 11(12):1566. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121566
Chicago/Turabian StyleSimu, Mihaela Adriana, Dragoș Cătălin Jianu, Adriana Octaviana Dulamea, Viorelia Adelina Constantin, Diana Popescu, Juan Carlos Parra, and József Attila Szász. 2021. "Advanced Parkinson’s Disease Treatment Simplification and Long-Term Outcomes with Levodopa Carbidopa Intestinal Gel: COSMOS Romanian Subanalysis" Brain Sciences 11, no. 12: 1566. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11121566