
Intraoperative Computed Tomography-Based Navigation with Augmented Reality for Lateral Approaches to the Spine


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. General Characteristics of the Patients
3.2. Registration Accuracy
3.3. The Effective Radiation Dose
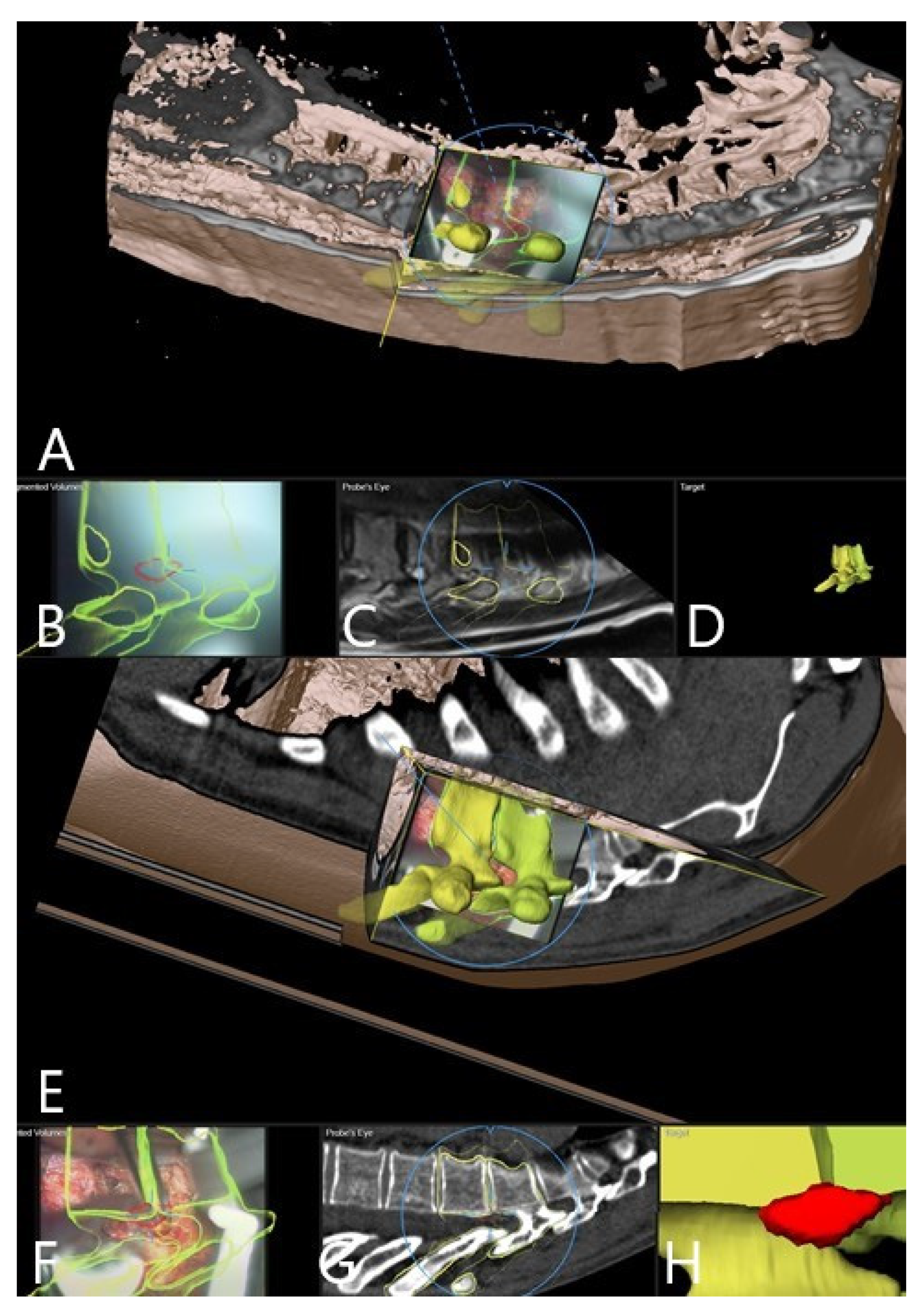
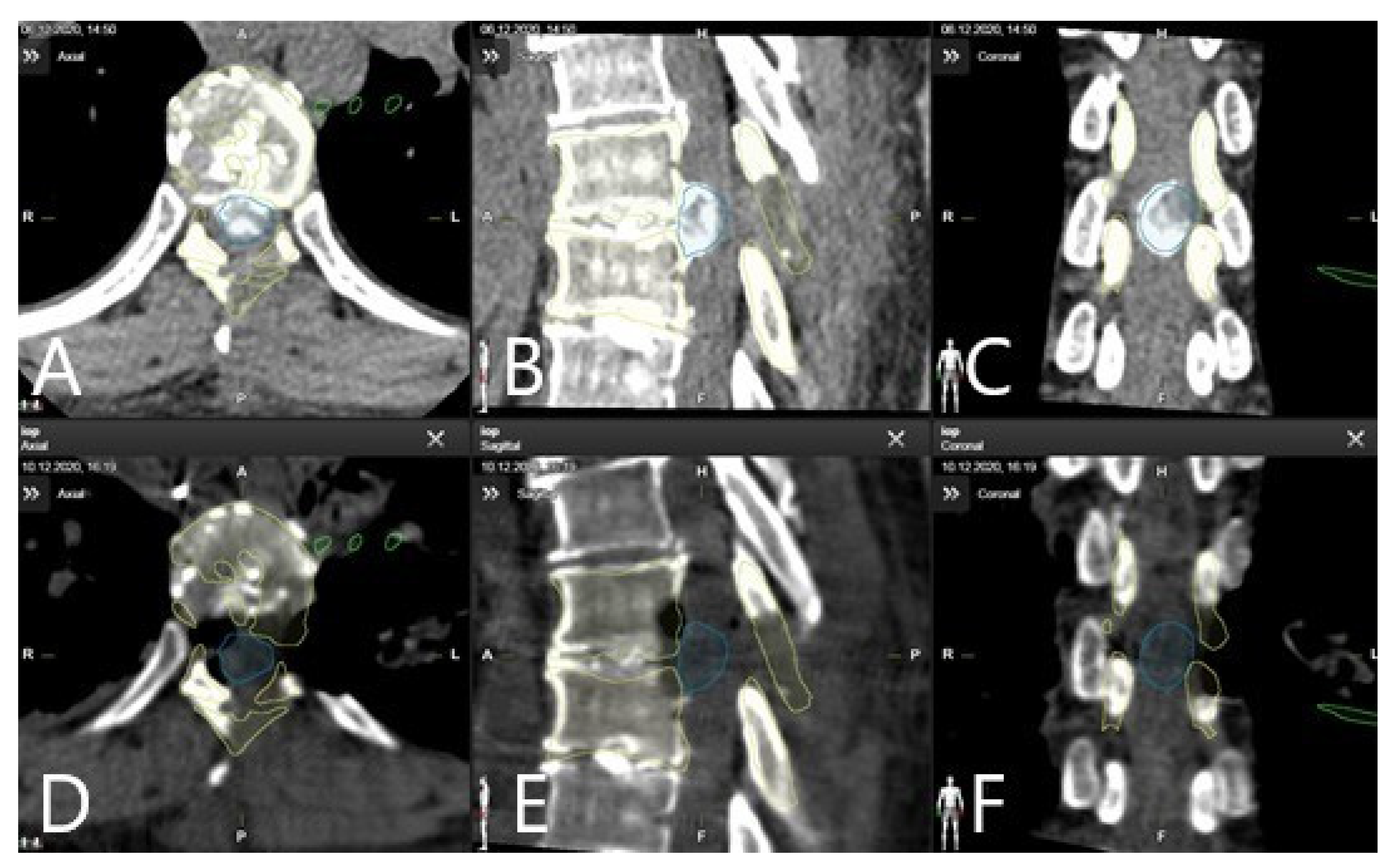
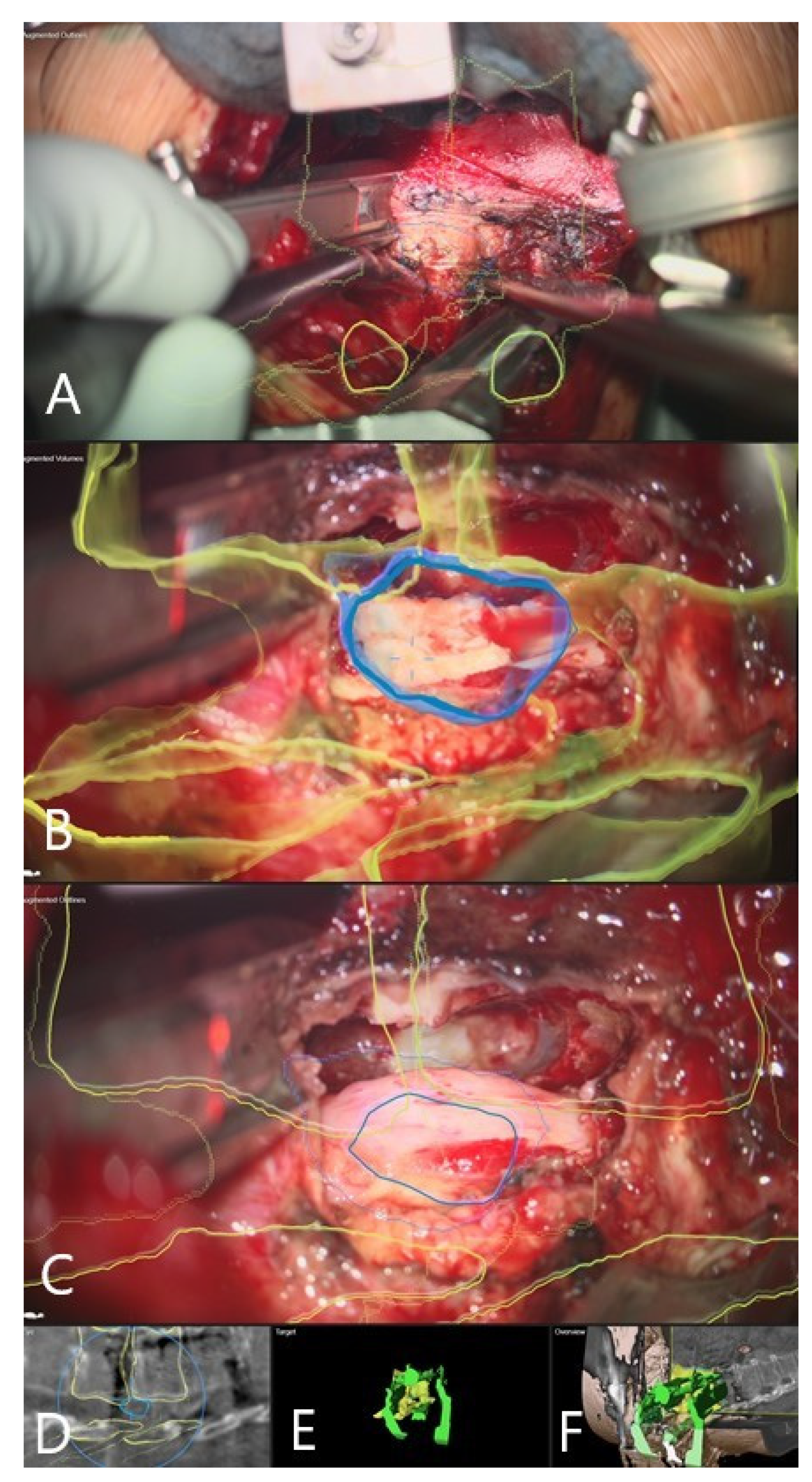
3.4. Augmented Reality
3.5. Clinical Application of iCT and AR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnold, P.M.; Anderson, K.K.; McGuire, R.A. The lateral transpsoas approach to the lumbar and thoracic spine: A review. Surg. Neurol. Int. 2012, 3 (Suppl. S3), S198–S215. [Google Scholar] [CrossRef]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme Lateral Interbody Fusion (XLIF): A novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006, 6, 435–443. [Google Scholar] [CrossRef]
- Karikari, I.O.; Nimjee, S.M.; Hardin, C.A.; Hughes, B.D.; Hodges, T.R.; Mehta, A.I.; Choi, J.; Brown, C.R.; Isaacs, R.E. Extreme lateral interbody fusion approach for isolated thoracic and thoracolumbar spine diseases: Initial clinical experience and early outcomes. J. Spinal Disord. Tech. 2011, 24, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Lang, G.; Perrech, M.; Navarro-Ramirez, R.; Hussain, I.; Pennicooke, B.; Maryam, F.; Avila, M.J.; Härtl, R. Potential and Limitations of Neural Decompression in Extreme Lateral Interbody Fusion—A Systematic Review. World Neurosurg. 2017, 101, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Meredith, D.S.; Kepler, C.K.; Huang, R.C.; Hegde, V.V. Extreme Lateral Interbody Fusion (XLIF) in the Thoracic and Thoracolumbar Spine: Technical Report and Early Outcomes. HSS J. 2013, 9, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formica, M.; Zanirato, A.; Cavagnaro, L.; Basso, M.; Divano, S.; Felli, L. Extreme lateral interbody fusion in spinal revision surgery: Clinical results and complications. Eur. Spine J. 2017, 26, 433–470. [Google Scholar] [CrossRef]
- Liu, X.; Joseph, J.R.; Smith, B.W.; Saadeh, Y.; Park, P. Analysis of Intraoperative Cone-Beam Computed Tomography Combined With Image Guidance for Lateral Lumbar Interbody Fusion. Oper. Neurosurg. 2018, 14, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Soliman, H.; Fridley, J.; Telfeian, A.; Choi, D.B.; Galgano, M.; Kosztowski, T.; Gokaslan, Z.L.; Oyelese, A.A. Minimally Invasive, Far Lateral Lumbar Microdiscectomy with Intraoperative Computed Tomography Navigational Assistance and Electrophysiological Monitoring. World Neurosurg. 2019, 122, e1228–e1239. [Google Scholar] [CrossRef]
- Hayama, S.; Nakano, A.; Nakaya, Y.; Baba, I.; Fujiwara, K.; Fujishiro, T.; Yano, T.; Usami, Y.; Kino, K.; Obo, T.; et al. The Evaluation of Indirect Neural Decompression After Lateral Lumbar Interbody Fusion Using Intraoperative Computed Tomography Myelogram. World Neurosurg. 2018, 120, e710–e718. [Google Scholar] [CrossRef]
- Navarro-Ramirez, R.; Berlin, C.; Lang, G.; Hussain, I.; Janssen, I.; Sloan, S.; Askin, G.; Avila, M.J.; Zubkov, M.; Härtl, R. A New Volumetric Radiologic Method to Assess Indirect Decompression After Extreme Lateral Interbody Fusion Using High-Resolution Intraoperative Computed Tomography. World Neurosurg. 2018, 109, 59–67. [Google Scholar] [CrossRef]
- Oyelese, A.A.; Fridley, J.; Choi, D.B.; Telfeian, A.; Gokaslan, Z.L. Minimally invasive direct lateral, retroperitoneal transforaminal approach for large L1–2 disc herniations with intraoperative CT navigational assistance: Technical note and report of 3 cases. J. Neurosurg. Spine 2018, 29, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.Y.; Fridley, J.; Gokaslan, Z.; Telfeian, A.; Oyelese, A.A. Minimally Invasive Thoracolumbar Corpectomy and Stabilization for Unstable Burst Fractures Using Intraoperative Computed Tomography and Computer-Assisted Spinal Navigation. World Neurosurg. 2019, 122, e1266–e1274. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Saß, B.; Nimsky, C. Microscope-Based Augmented Reality in Degenerative Spine Surgery: Initial Experience. World Neurosurg. 2019, 128, e541–e551. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Chehab, S.; Bien, S.; Nimsky, C. Preoperative 3-Dimensional Angiography Data and Intraoperative Real-Time Vascular Data Integrated in Microscope-Based Navigation by Automatic Patient Registration Applying Intraoperative Computed Tomography. World Neurosurg. 2018, 113, e414–e425. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Saß, B.; Nimsky, C. Intraoperative computed tomography as reliable navigation registration device in 200 cranial procedures. Acta Neurochir. 2018, 160, 1681–1689. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Saß, B.; Voellger, B.; Nimsky, C. Implementation of augmented reality support in spine surgery. Eur. Spine J. 2019, 28, 1697–1711. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Saß, B.; Pojskic, M.; Nimsky, C. Augmented reality in intradural spinal tumor surgery. Acta Neurochir. 2019, 161, 2181–2193. [Google Scholar] [CrossRef] [PubMed]
- Elbakri, I.A.; Kirkpatrick, I.D. Dose-Length Product to Effective Dose Conversion Factors for Common Computed Tomography Examinations Based on Canadian Clinical Experience. Can. Assoc. Radiol. J. 2013, 64, 15–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huda, W.; Ogden, K.M.; Khorasani, M.R. Converting Dose-Length Product to Effective Dose at CT. Radiology 2008, 248, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Saß, B.; Pojskic, M.; Gjorgjevski, M.; Voellger, B.; Nimsky, C. Reliable navigation registration in cranial and spine surgery based on intraoperative computed tomography. Neurosurg. Focus 2019, 47, e11. [Google Scholar] [CrossRef] [Green Version]
- Tamura, Y.; Sugano, N.; Sasama, T.; Sato, Y.; Tamura, S.; Yonenobu, K.; Yoshikawa, H.; Ochi, T. Surface-based registration accuracy of CT-based image-guided spine surgery. Eur. Spine J. 2004, 14, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Tatsui, C.E.; Nascimento, C.N.G.; Suki, D.; Amini, B.; Li, J.; Ghia, A.J.; Thomas, J.G.; Stafford, R.J.; Rhines, L.D.; Cata, J.P.; et al. Image guidance based on MRI for spinal interstitial laser thermotherapy: Technical aspects and accuracy. J. Neurosurg. Spine 2017, 26, 605–612. [Google Scholar] [CrossRef] [Green Version]
- Ji, S.; Fan, X.; Paulsen, K.D.; Roberts, D.W.; Mirza, S.K.; Lollis, S.S. Intraoperative CT as a registration benchmark for intervertebral motion compensation in image-guided open spinal surgery. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 2009–2020. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Shi, B.; Chen, T.; Zhang, Y.; Geng, T.; Qiao, L.; Zhang, M.; He, L.; Zuo, H.; Wang, G. Axial MR diffusion tensor imaging and tractography in clinical diagnosed and pathology confirmed cervical spinal cord astrocytoma. J. Neurol. Sci. 2017, 375, 43–51. [Google Scholar] [CrossRef]
- Zhao, J.; Liu, Y.; Fan, M.; Liu, B.; He, D.; Tian, W. Comparison of the Clinical Accuracy Between Point-to-Point Registration and Auto-Registration Using an Active Infrared Navigation System. Spine 2018, 43, E1329–E1333. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zhao, Z.; Chen, F.; Zhang, B.; Fu, L.; Liao, H. Augmented reality surgical navigation with ultrasound-assisted registration for pedicle screw placement: A pilot study. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 2205–2215. [Google Scholar] [CrossRef] [PubMed]
- Edström, E.; Burström, G.; Omar, A.; Nachabe, R.; Söderman, M.; Persson, O.; Gerdhem, P.; Elmi-Terander, A. Augmented Reality Surgical Navigation in Spine Surgery to Minimize Staff Radiation Exposure. Spine 2020, 45, e45–e53. [Google Scholar] [CrossRef]
- Schegerer, A.; Loose, R.; Heuser, L.J.; Brix, G. Diagnostic Reference Levels for Diagnostic and Interventional X-Ray Procedures in Germany: Update and Handling. Rofo 2019, 191, 739–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilar-Palop, J.; Vilar, J.; Hernández-Aguado, I.; González-Álvarez, I.; Lumbreras, B. Updated effective doses in radiology. J. Radiol. Prot. 2016, 36, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, D.; Strelzow, J.; Dea, N.; Ford, N.L.; Batke, J.; Pennington, A.; Yang, K.; Ailon, T.; Boyd, M.; Dvorak, M.; et al. Patient and surgeon radiation exposure during spinal instrumentation using intraoperative computed tomography-based navigation. Spine J. 2016, 16, 343–354. [Google Scholar] [CrossRef]
- Zausinger, S.; Scheder, B.; Uhl, E.; Heigl, T.; Morhard, D.; Tonn, J.-C. Intraoperative Computed Tomography With Integrated Navigation System in Spinal Stabilizations. Spine 2009, 34, 2919–2926. [Google Scholar] [CrossRef]
- Soldozy, S.; Montgomery, S.; Sarathy, D.; Young, S.; Skaff, A.; Desai, B.; Sokolowski, J.; Sandhu, F.; Voyadzis, J.-M.; Yağmurlu, K.; et al. Diagnostic, Surgical, and Technical Considerations for Lumbar Interbody Fusion in Patients with Osteopenia and Osteoporosis: A Systematic Review. Brain Sci. 2021, 11, 241. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N.E. Extreme lateral lumbar interbody fusion: Do the cons outweigh the pros? Surg. Neurol. Int. 2016, 7 (Suppl. S25), S692–S700. [Google Scholar] [CrossRef] [Green Version]
- Buric, J.; Conti, R.; Peressutti, S. Lumbar Lordosis Correction with Interbody Hyperlordotic Cages: Initial Experience, Learning Curve, Technical Aspects, and Complication Incidence. Int. J. Spine Surg. 2018, 12, 185–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, C.T.; Farber, S.H.; Cole, T.S.; Xu, D.S.; Godzik, J.; Whiting, A.C.; Hartman, C.; Porter, R.W.; Turner, J.D.; Uribe, J. Complications for minimally invasive lateral interbody arthrodesis: A systematic review and meta-analysis comparing prepsoas and transpsoas approaches. J. Neurosurg. Spine 2019, 30, 446–460. [Google Scholar] [CrossRef]
- Rodgers, W.B.; Gerber, E.J.; Patterson, J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: An analysis of 600 cases. Spine 2011, 36, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yingsakmongkol, W.; Wathanavasin, W.; Jitpakdee, K.; Singhatanadgige, W.; Limthongkul, W.; Kotheeranurak, V. Psoas Major Muscle Volume Does Not Affect the Postoperative Thigh Symptoms in XLIF Surgery. Brain Sci. 2021, 11, 357. [Google Scholar] [CrossRef]
- Burström, G.; Persson, O.; Edström, E.; Elmi-Terander, A. Augmented reality navigation in spine surgery: A systematic review. Acta Neurochir. 2021, 163, 843–852. [Google Scholar] [CrossRef]
- Meola, A.; Chang, S.D. Letter: Navigation-Linked Heads-Up Display in Intracranial Surgery: Early Experience. Oper. Neurosurg. 2018, 14, e71–e72. [Google Scholar] [CrossRef] [PubMed]
- Ghaednia, H.; Fourman, M.S.; Lans, A.; Detels, K.; Dijkstra, H.; Lloyd, S.; Sweeney, A.; Oosterhoff, J.H.; Schwab, J.H. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021. [Google Scholar] [CrossRef]
- Molina, C.A.; Dibble, C.F.; Lo, S.-F.L.; Witham, T.; Sciubba, D.M. Augmented reality–mediated stereotactic navigation for execution of en bloc lumbar spondylectomy osteotomies. J. Neurosurg. Spine 2021, 34, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Molina, C.A.; Sciubba, D.M.; Greenberg, J.K.; Khan, M.; Witham, T. Clinical Accuracy, Technical Precision, and Workflow of the First in Human Use of an Augmented-Reality Head-Mounted Display Stereotactic Navigation System for Spine Surgery. Oper. Neurosurg. 2021, 20, 300–309. [Google Scholar] [CrossRef]
- Burström, G.; Nachabe, R.; Persson, O.; Edström, E.; Elmi Terander, A. Augmented and Virtual Reality Instrument Tracking for Minimally Invasive Spine Surgery: A Feasibility and Accuracy Study. Spine 2019, 44, 1097–1104. [Google Scholar] [CrossRef]
- Burström, G.; Buerger, C.; Hoppenbrouwers, J.; Nachabe, R.; Lorenz, C.; Babic, D.; Homan, R.; Racadio, J.M.; Grass, M.; Persson, O.; et al. Machine learning for automated 3-dimensional segmentation of the spine and suggested placement of pedicle screws based on intraoperative cone-beam computer tomography. J. Neurosurg. Spine 2019, 31, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Cosar, M.; Kirnaz, S.; Schmidt, F.A.; Wipplinger, C.; Wong, T.; Härtl, R. Evolving Navigation, Robotics, and Augmented Reality in Minimally Invasive Spine Surgery. Glob. Spine J. 2020, 10, 22S–33S. [Google Scholar] [CrossRef] [PubMed]
- Benglis, D.M.; Vanni, S.; Levi, A.D. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J. Neurosurg. Spine 2009, 10, 139–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houten, J.K.; Alexandre, L.C.; Nasser, R.; Wollowick, A.L. Nerve injury during the transpsoas approach for lumbar fusion. J. Neurosurg. Spine 2011, 15, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Dakwar, E.; Vale, F.L.; Uribe, J.S. Trajectory of the main sensory and motor branches of the lumbar plexus outside the psoas muscle related to the lateral retroperitoneal transpsoas approach. J. Neurosurg. Spine 2011, 14, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Guérin, P.; Obeid, I.; Gille, O.; Bourghli, A.; Luc, S.; Pointillart, V.; Cursolle, J.C.; Vital, J.-M. Safe working zones using the minimally invasive lateral retroperitoneal transpsoas approach: A morphometric study. Surg. Radiol. Anat. 2011, 33, 665–671. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Age | Sex | Diagnosis | Preoperative Symptoms | Procedure | Complications | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | 75 | M | Adjacent segment disease L1/2 following spondylodesis L2-5 and implantation of expandable vertebral body cage at L2 | Back pain, hip flexor paresis 4/5 | 1. Spondylodesis T9-S1 2. Removal of the L2 vertebral body implant, Corpectomy L1/2, Implantation of expandable vertebral body cage, left retroperitoneal approach | No | Regredient pain, no neurologic deficits following surgery |
| 2 | 80 | M | Spondylodiscitis L4/5 following surgery for right hip prothesis | Back pain | XLIF from right following Spondylodesis L4/5 | No | Regredient pain, no neurologic deficits following surgery |
| 3 | 66 | F | Calcified herniated disc Th 9/10 | Ataxia Paraparesis 4/5 | Left lateral retropleural approach, sequestrectomy of the herniated disc | None | Improvement of ataxia following surgery |
| 4 | 19 | F | Giant aneurysmatic bone cyst Th 8/9 | Back pain | 1. Hemilaminectomy T8/9, Resection of the thoracic nerve origin 2. Tumor resection via left retropleural approach, Resection of 7/8 Rib with reconstruction of the thoracic wall | No | No pain, no deficits, and no recurrence at follow up |
| 5 | 80 | M | Instability following L1 vertebral body fracture and stabilization T11-L3 | Back pain, Paraparesis 4/5 | Corpectomy L1/2, Implantation of expandable vertebral body cage, left retroperitoneal approach | No | Improvement of pain, no deficits following surgery |
| 6 | 77 | M | Instability following kyphoplasty of T12 and stabilization T11-L1 due to T12 fracture | Back pain, Paraparesis 4/5 | Corpectomy T12, Implantation of expandable vertebral cage, left retropleural approach | No | Improvement of pain, no deficits following surgery |
| 7 | F | 76 | L2 breast cancer metastasis | Back pain | 1. L1-3 stabilization 2. Corpectomy L2, implantation of expandable vertebral cage, left retroperitoneal approach | No | Improvement of pain, no deficits following surgery |
| 8 | M | 51 | Herniated disc T8/9 with myelopathy | Back pain, paraparesis 3/5, urinary incontinence | 1. Partial resection of the herniated disc via posterior approach with right costotransversectomy 2. Resection of the remaining disc via left retropleural approach 3. Stabilization T8-9 | No | No pain and no deficits following surgery |
| 9 | F | 52 | L2 Neurinoma | Back and hip pain | Resection of neurinoma via left retroperitoneal approach | No | No pain, no deficits, and no tumor recurrence at follow up |
| 10 | F | 63 | Herniated disc T 7/8 with myelopathy | Worsening of back pain due to chronic pain syndrome following multiple spine surgeries, ataxia | Left lateral retropleural approach, sequestrectomy of the herniated disc | No | Chronic pain syndrome with moderate improvement, no ataxia, no deficits at follow up |
| 11 | F | 51 | Giant cell tumor of T12 | Back pain, paraparesis 3/5, urinary incontinence | Left lateral retropleural approach, corpectomy T12, implantation of expandable cage | No | No pain, no deficits, and no tumor recurrence at follow up |
| 12 | F | 71 | T12 fracture | Back pain, paraparesis 3/5 | 1. Left lateral retropleural approach, corpectomy Th12, implantation of expandable cage 2. Th11-L1 stabilization | No | Death 5 weeks following surgery due to pneumonia, exacerbation of COPD and cardiorespiratory failure |
| 13 | F | 50 | Calcified herniated disc T10/11 with myelopathy and spinal canal stenosis | Back pain, paraparesis 2/5, urinary and stool incontinence | 1. Dorsal stabilization T10-11 with spinal canal decompression | Pleural effusion in the field of the lateral operative approach, treated with thorax drainage | Improvement of back pain and paraparesis (4/5) with urinary incontinence, no stool incontinence 6 months following surgery |
| 2. Left lateral retropleural approach, partial resection of the herniated disc | Hematoma on 10th day following surgery with evacuation of hematoma in the dorsal operative field | ||||||
| 3. Reoperation through left retropleural approach, placement of thorax drainage due to chambered pleural effusion and complete resection of the calcified disc | Dorsal wound revision due to healing deficit 4 weeks following surgery; | ||||||
| 14 | F | 48 | Schwannoma Th11/12 | Back pain | 1. Resection of T12 nerve root via dorsal approach. 2. Left lateral transpleural approach, resection of the tumor | None | Improvement of back pain following surgery |
| 15 | F | 46 | Calcified herniated disc Th 7/8 | Back, pain, paraparesis | Left lateral retropleural approach, constotransversectomy, total resection of the herniated disc | None | Improvement of back pain and paraparesis following surgery |
| 16 | M | 38 | Calcified herniated disc Th 9/10 | Back pain, paraparesis | Left lateral retropleural approach, costotransversectomy, subtotal resection of the herniated disc | None | Improvement of back pain and paraparesis following surgery |
| Number | Protocol | Scout Scan DLP (mm) | Scout Scan Length (mm) | iCT Scan DLP (mGy.cm) | iCT Scan Length (mm) | Total DLP (mGy.cm) | Total ED (mSv) | Visualized Objects in Augmented Reality |
|---|---|---|---|---|---|---|---|---|
| 1 | L-spine | 82.00944 | 265.9999 | 639.47850 | 126 | 721.48794 | 14.29 | - |
| 2 | L-Spine 50% | 34.18377 | 286 | 210.19560 | 94.999888 | 244.37937 | 4.84 | - |
| 3 | T-Spine 30% | 27.81074 | 223 | 242.90090 | 104 | 270.71164 | 4.82 | - |
| 4 | T-spine 30% | 21.53883 | 160.9999 | 315.9917 | 160 | 337.53053 | 6.01 | - |
| 5 | L-spine 30% | 18.20057 | 127.9999 | 438.00650 | 127 | 456.20707 | 9.03 | - |
| 6 | T-Spine | 107.99710 | 273 | 437.70600 | 93 | 545.7031 | 9.71 | - |
| 7 | L-Spine 70% | 12.34 | 192.00 | 167.04 | 167.00 | 179.38 | 3.55 | vertebral body replacement, screws and rods, T12, L1, L2, L3, L4, |
| 8 | T-Spine 70% | 35.59999 | 300.00 | 164.75950 | 188.00 | 200.36 | 3.57 | spinal cord, spinal canal, C1, C2, C3, C4, C5, C6, C7, T1, T2, T3, T4,T5, T6, T7, T8, T9, T10, T11, T12, disc hernation |
| 9 | L-Spine 70% | 13.80420 | 221.00 | 127.95180 | 168.00 | 141.76 | 2.81 | tumor, T12,L1, L2, L3, L4, kidney, vessels |
| 10 | T-Spine 70% | 51.66633 | 286.00 | 437.57950 | 248.00 | 489.25 | 8.71 | T7, T8 |
| 11 | T-Spine 70% | 19.82 | 144.00 | 145.00 | 117.00 | 164.82 | 3.10 | L3, L4, nerve root |
| 12 | T-Spine 70% | 24.74 | 190 | 201.82 | 164 | 226.56000 | 4.03 | Vertebral body T10, T11, T12, L1, L2, implant, clamp |
| 13 | T-Spine 90% | 18.1 | 127 | 54.11 | 79 | 72.21000 | 1.29 | Vertebral body T10,11, T10, T11, screws, disc herniation |
| 14 | T-Spine 70% | - | - | 112.11 | 116 | 112.11 | 2.00 | Vertebral body T10, T11, T12, L1, tumor, aorta, spinal cord |
| 15 | T-Spine 70% | - | - | 423.83 | 202 | 423.83 | 7.54 | Vertebral body T7,8, herniated disc |
| 16 | T-Spine 70% | - | - | 748.1259 | 162 | 748.1259 | 13.32 | Vertebral body T9, T10, disc herniation, spinal cord |
| Number | Control Scan | Protocol | Scout Scan DLP (mGy.cm) | Scout Scan Length (mm) | iCT Scan DLP (mGy.cm) | iCT Scan Length (mm) | Total DLP (mGy.cm) | Total ED (mSv) |
|---|---|---|---|---|---|---|---|---|
| 1 | - | - | - | - | - | - | - | - |
| 2 | - | - | - | - | - | - | - | - |
| 3 | Herniated disc extent of resection control | T-Spine 30% | 25.99 | 205 | 289.63 | 134 | 315.62000 | 5.62 |
| 4 | - | |||||||
| 5 | Implant control | L-spine 30% | 18.20057 | 127.9999 | 438.00650 | 127 | 456.20707 | 9.03 |
| 6 | - | |||||||
| 7 | Implant control | L-Spine 70% | 13.7 | 219 | 150.26 | 145 | 163.96000 | 3.25 |
| 8 | - | T-Spine 70% | 19.52 | 141 | 106.39 | 103 | 125.91000 | 2.24 |
| 9 | - | - | - | - | - | - | - | - |
| 10 | - | - | - | - | - | - | - | - |
| 11 | Tumor resection and implant control | T-Spine 70% | 23.56 | 181 | 161.31 | 136 | 184.87000 | 3.29 |
| 12 | Implant control | T-Spine 70% | 23.66 | 182 | 180.32 | 141 | 203.98000 | 3.63 |
| 13 | - | - | - | - | - | - | - | - |
| 14 | - | - | - | - | - | - | - | - |
| 15 | Herniated disc extent of resection control | T-Spine | - | - | 935.32 | 133 | 935.32 | 16.65 |
| 16 | - | - | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pojskić, M.; Bopp, M.; Saß, B.; Kirschbaum, A.; Nimsky, C.; Carl, B. Intraoperative Computed Tomography-Based Navigation with Augmented Reality for Lateral Approaches to the Spine. Brain Sci. 2021, 11, 646. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050646
Pojskić M, Bopp M, Saß B, Kirschbaum A, Nimsky C, Carl B. Intraoperative Computed Tomography-Based Navigation with Augmented Reality for Lateral Approaches to the Spine. Brain Sciences. 2021; 11(5):646. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050646
Chicago/Turabian StylePojskić, Mirza, Miriam Bopp, Benjamin Saß, Andreas Kirschbaum, Christopher Nimsky, and Barbara Carl. 2021. "Intraoperative Computed Tomography-Based Navigation with Augmented Reality for Lateral Approaches to the Spine" Brain Sciences 11, no. 5: 646. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050646