
Assessment of a Reliable Fractional Anisotropy Cutoff in Tractography of the Corticospinal Tract for Neurosurgical Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Image Acquisition
2.3. Image Processing
2.4. Tractography
2.5. Statistics
2.6. Testing Different FA Cutoffs a Posteriori
3. Results
3.1. Patients
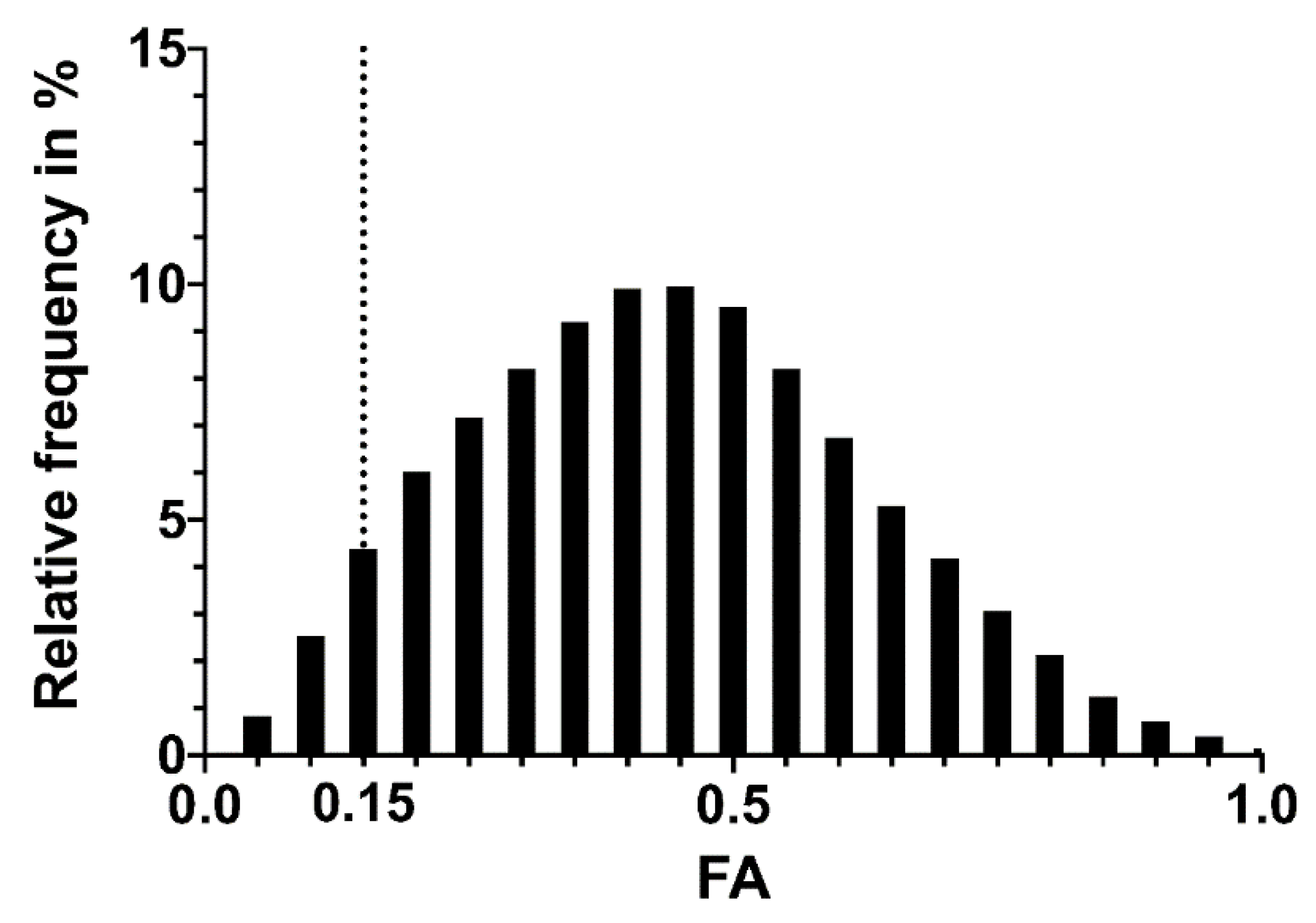
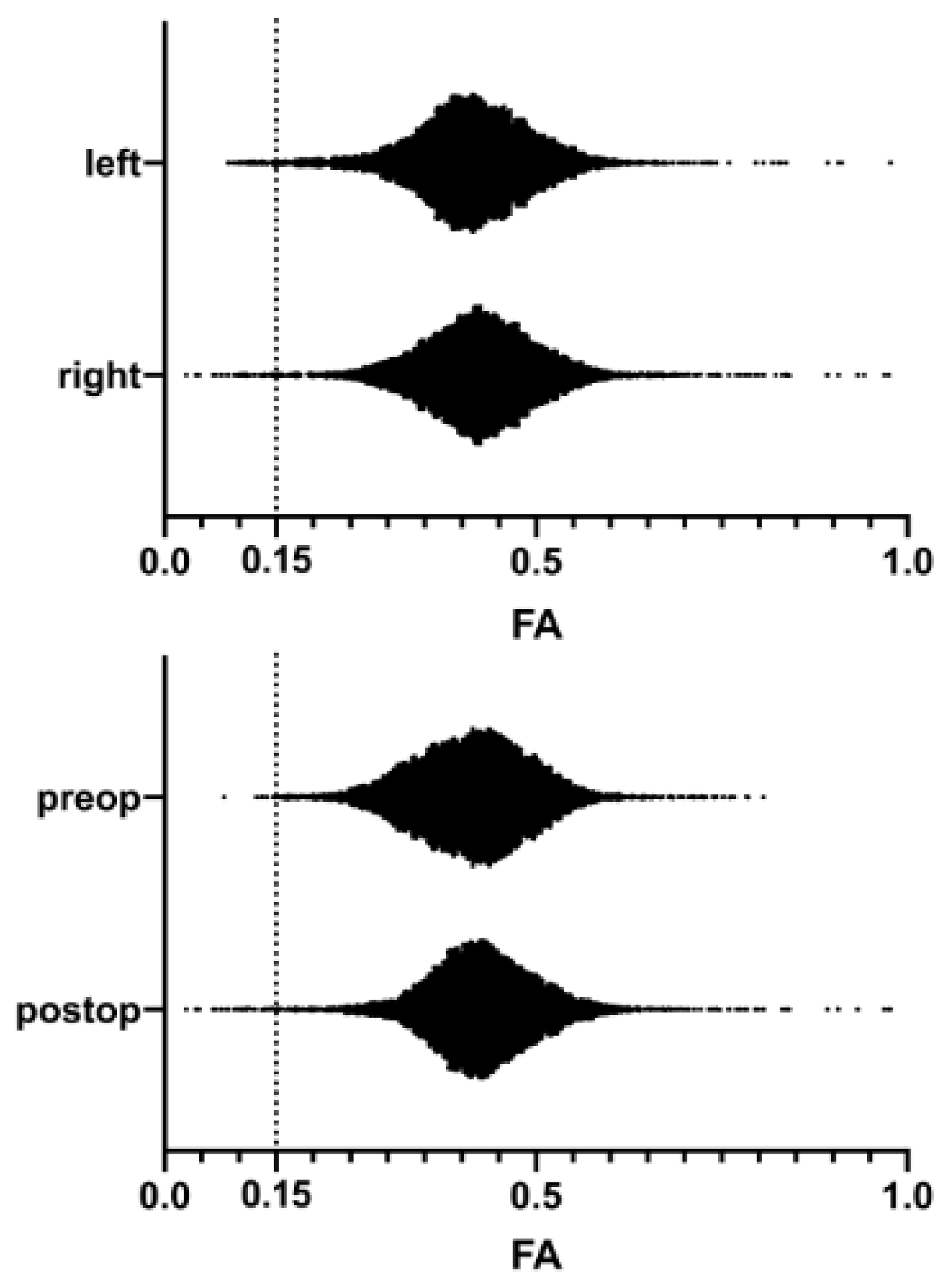
3.2. FA Distribution in the Corticospinal Tracts
3.3. Postoperative Changes in the FA Distribution
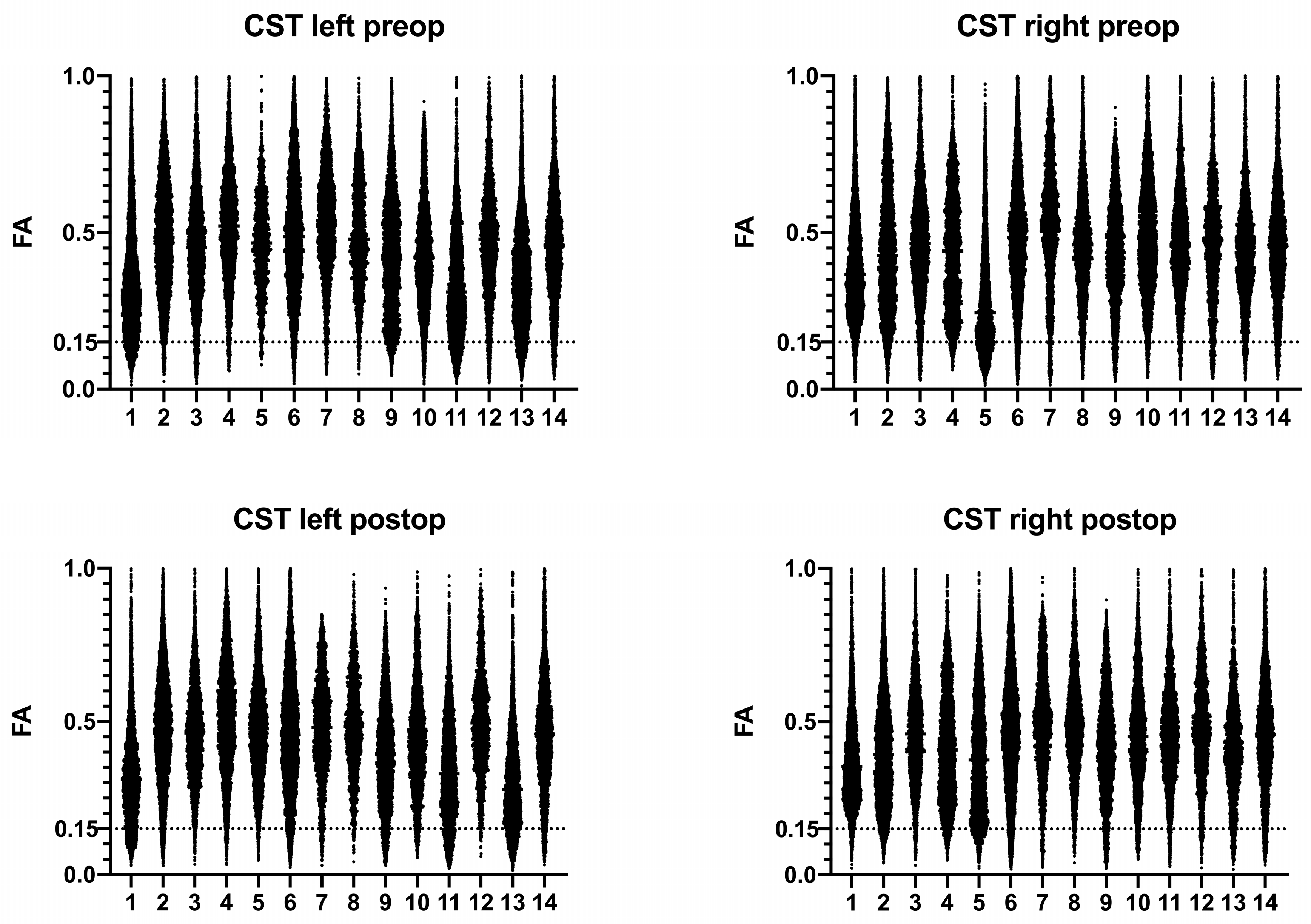
3.4. Individual Distributions of FA Values
3.5. Infiltrated or Compressed CSTs
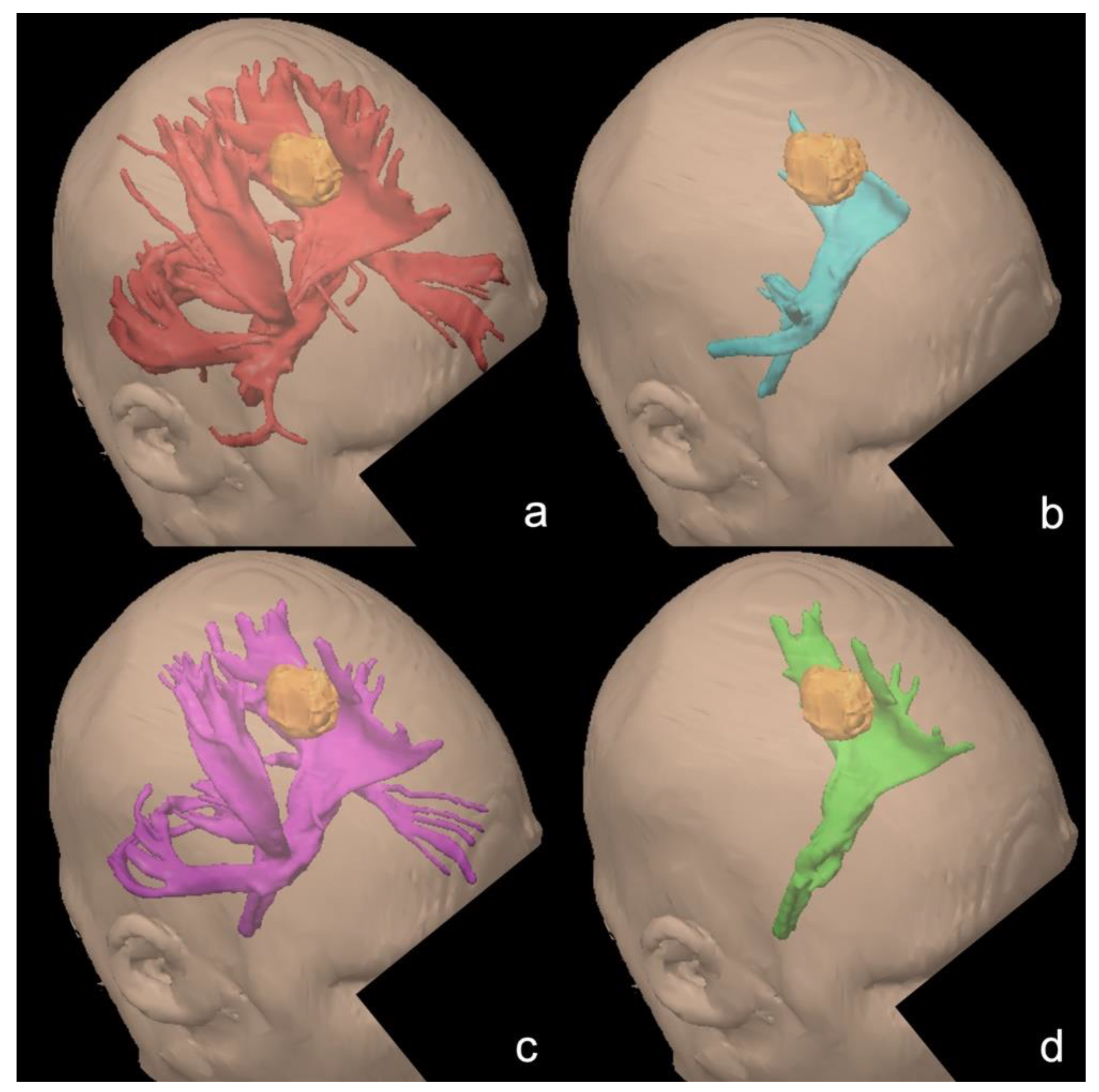
3.6. Tractography Results at Different FA Cutoffs
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azad, T.D.; Duffau, H. Limitations of functional neuroimaging for patient selection and surgical planning in glioma surgery. Neurosurg. Focus 2020, 48, E12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Essayed, W.I.; Zhang, F.; Unadkat, P.; Cosgrove, G.R.; Golby, A.J.; O’Donnell, L.J. White matter tractography for neurosurgical planning: A topography-based review of the current state of the art. Neuroimage Clin. 2017, 15, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Ashmore, J.; Pemberton, H.G.; Crum, W.D.; Jarosz, J.; Barker, G.J. Implementation of clinical tractography for pre-surgical planning of space occupying lesions: An investigation of common acquisition and post-processing methods compared to dissection studies. PLoS ONE 2020, 15, e0231440. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Zhang, H.; Schramm, S.; Ille, S.; Negwer, C.; Kreiser, K.; Meyer, B.; Krieg, S.M. Function-specific Tractography of Language Pathways Based on nTMS Mapping in Patients with Supratentorial Lesions. Clin. Neuroradiol. 2020, 30, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Umana, G.E.; Scalia, G.; Graziano, F.; Maugeri, R.; Alberio, N.; Barone, F.; Crea, A.; Fagone, S.; Giammalva, G.R.; Brunasso, L.; et al. Navigated Transcranial Magnetic Stimulation Motor Mapping Usefulness in the Surgical Management of Patients Affected by Brain Tumors in Eloquent Areas: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Fratini, A.; Zhang, H.; Zimmer, C.; Meyer, B.; Krieg, S.M. Associations between clinical outcome and tractography based on navigated transcranial magnetic stimulation in patients with language-eloquent brain lesions. J. Neurosurg. 2020, 132, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Zhang, H.; Fratini, A.; Wildschuetz, N.; Ille, S.; Schröder, A.; Zimmer, C.; Meyer, B.; Krieg, S.M. Risk assessment by presurgical tractography using navigated tms maps in patients with highly motor-or language-eloquent brain tumors. Cancers 2020, 12, 1264. [Google Scholar] [CrossRef]
- Wende, T.; Hoffmann, K.-T.; Meixensberger, J. Tractography in Neurosurgery: A Systematic Review of Current Applications. J. Neurol. Surg. Part A Cent. Eur. Neurosurg. 2020, 81, 442–455. [Google Scholar] [CrossRef]
- Rutten, G.J.M.; Landers, M.J.F.; De Baene, W.; Meijerink, T.; van der Hek, S.; Verheul, J.H.B. Executive functional deficits during electrical stimulation of the right frontal aslant tract. Brain Imaging Behav. 2021. [Google Scholar] [CrossRef] [PubMed]
- Talozzi, L.; Testa, C.; Evangelisti, S.; Cirignotta, L.; Bianchini, C.; Ratti, S.; Fantazzini, P.; Tonon, C.; Manners, D.N.; Lodi, R. Along-tract analysis of the arcuate fasciculus using the Laplacian operator to evaluate different tractography methods. Magn. Reson. Imaging 2018, 54, 183–193. [Google Scholar] [CrossRef]
- Assaf, Y.; Cohen, Y. Inferring Microstructural Information of White Matter from Diffusion MRI. In Diffusion MRI; Elsevier: Amsterdam, The Netherlands, 2013; ISBN 9780123964601. [Google Scholar]
- Zhang, H.; Schramm, S.; Schröder, A.; Zimmer, C.; Meyer, B.; Krieg, S.M.; Sollmann, N. Function-based tractography of the language network correlates with aphasia in patients with language-eloquent glioblastoma. Brain Sci. 2020, 10, 412. [Google Scholar] [CrossRef]
- Tuncer, M.S.; Salvati, L.F.; Grittner, U.; Hardt, J.; Schilling, R.; Bährend, I.; Silva, L.L.; Fekonja, L.S.; Faust, K.; Vajkoczy, P.; et al. Towards a tractography-based risk stratification model for language area associated gliomas. Neuroimage Clin. 2021, 29. [Google Scholar] [CrossRef]
- Fernández, L.; Velásquez, C.; Porrero, J.A.G.; de Lucas, E.M.; Martino, J. Heschl’s gyrus fiber intersection area: A new insight on the connectivity of the auditory-language hub. Neurosurg. Focus 2020, 48, E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadlbauer, A.; Nimsky, C.; Buslei, R.; Salomonowitz, E.; Hammen, T.; Buchfelder, M.; Moser, E.; Ernst-Stecken, A.; Ganslandt, O. Diffusion tensor imaging and optimized fiber tracking in glioma patients: Histopathologic evaluation of tumor-invaded white matter structures. Neuroimage 2007, 34, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Morgan, P.S.; Ashburner, J.; Smith, J.; Rorden, C. The first step for neuroimaging data analysis: DICOM to NIfTI conversion. J. Neurosci. Methods 2016, 264, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Tournier, J.D.; Smith, R.; Raffelt, D.; Tabbara, R.; Dhollander, T.; Pietsch, M.; Christiaens, D.; Jeurissen, B.; Yeh, C.H.; Connelly, A. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage 2019, 202, 116137. [Google Scholar] [CrossRef] [PubMed]
- Tournier, J.D.; Calamante, F.; Gadian, D.G.; Connelly, A. Direct estimation of the fiber orientation density function from diffusion-weighted MRI data using spherical deconvolution. Neuroimage 2004, 23, 1176–1185. [Google Scholar] [CrossRef]
- Tournier, J.D.; Calamante, F.; Connelly, A. Improved probabilistic streamlines tractography by 2nd order integration over fibre orientation distributions. Proc. Int. Soc. Magn. Reson. Med. 2010, 18, 1670. [Google Scholar]
- Raffa, G.; Quattropani, M.C.; Scibilia, A.; Conti, A.; Angileri, F.F.; Esposito, F.; Sindorio, C.; Cardali, S.M.; Germanò, A.; Tomasello, F. Surgery of language-eloquent tumors in patients not eligible for awake surgery: The impact of a protocol based on navigated transcranial magnetic stimulation on presurgical planning and language outcome, with evidence of tumor-induced intra-hemispheric pl. Clin. Neurol. Neurosurg. 2018, 168, 127–139. [Google Scholar] [CrossRef]
- Rutka, J.T.; Apodaca, G.; Stern, R.; Rosenblum, M. The extracellular matrix of the central and peripheral nervous systems: Structure and function. J. Neurosurg. 1988, 69, 155–170. [Google Scholar] [CrossRef] [Green Version]
- Mori, S.; Van Zijl, P.C.M. Fiber tracking: Principles and strategies—A technical review. NMR Biomed. 2002, 15, 468–480. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Gender | Diagnosis | Side | Lobe | CST Affection |
|---|---|---|---|---|---|---|
| 1 | 54 | M | Glioblastoma WHO grade IV | Left | Parietal | Compressed |
| 2 | 33 | M | Glioblastoma WHO grade IV | Right | Parietal | Dislocated |
| 3 | 42 | M | Oligodendroglioma WHO grade III | Left | Frontal | Unaffected |
| 4 | 65 | F | Metastasis | Right | Occipital | Compressed |
| 5 | 36 | F | Glioblastoma WHO grade IV | Right | Parietal | Compressed |
| 6 | 69 | M | Metastasis | Left | Frontal | Unaffected |
| 7 | 40 | F | Glioblastoma WHO grade IV | Left | Frontal | Dislocated |
| 8 | 63 | F | Meningioma WHO grade III | Left | Parietal | Compressed |
| 9 | 70 | M | Glioblastoma WHO grade IV | Left | Temporal | Compressed |
| 10 | 67 | F | Glioblastoma WHO grade IV | Left | Temporal | Compressed |
| 11 | 32 | F | Astrocytoma WHO grade III | Left | Frontal | Infiltrated |
| 12 | 30 | F | Astrocytoma WHO grade I | Left | Temporal | Unaffected |
| 13 | 45 | F | Glioblastoma WHO grade IV | Left | Frontal | Infiltrated |
| 14 | 55 | M | Glioblastoma WHO grade IV | Left | Temporal | Dislocated |
| Patient | Side | CST Affection | Preop Left | Postop Left | Preop Right | Postop Right |
|---|---|---|---|---|---|---|
| 1 | Left | Compressed | 0.1153 | 0.1076 | 0.1653 | 0.1701 |
| 2 | Right | Dislocated | 0.1897 | 0.1744 | 0.1567 | 0.1517 |
| 3 | Left | Unaffected | 0.1559 | 0.2098 | 0.1714 | 0.1923 |
| 4 | Right | Compressed | 0.2148 | 0.21.04 | 0.1697 | 0.1577 |
| 5 | Right | Compressed | 0.2068 | 0.2094 | 0.0812 | 0.1314 |
| 6 | Left | Unaffected | 0.1783 | 0.1542 | 0.1641 | 0.1476 |
| 7 | Left | Dislocated | 0.2296 | 0.1798 | 0.1759 | 0.1945 |
| 8 | Left | Compressed | 0.2128 | 0.2113 | 0.1811 | 0.2162 |
| 9 | Left | Compressed | 0.1514 | 0.1278 | 0.1960 | 0.1422 |
| 10 | Left | Compressed | 0.1674 | 0.1704 | 0.1471 | 0.1761 |
| 11 | Left | Infiltrated | 0.1022 | 0.0930 | 0.1871 | 0.1891 |
| 12 | Left | Unaffected | 0.1547 | 0.2200 | 0.1458 | 0.1916 |
| 13 | Left | Infiltrated | 0.3663 | 0.0944 | 0.1665 | 0.1453 |
| 14 | Left | Dislocated | 0.1595 | 0.1886 | 0.1430 | 0.1601 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wende, T.; Kasper, J.; Wilhelmy, F.; Dietel, E.; Hamerla, G.; Scherlach, C.; Meixensberger, J.; Fehrenbach, M.K. Assessment of a Reliable Fractional Anisotropy Cutoff in Tractography of the Corticospinal Tract for Neurosurgical Patients. Brain Sci. 2021, 11, 650. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050650
Wende T, Kasper J, Wilhelmy F, Dietel E, Hamerla G, Scherlach C, Meixensberger J, Fehrenbach MK. Assessment of a Reliable Fractional Anisotropy Cutoff in Tractography of the Corticospinal Tract for Neurosurgical Patients. Brain Sciences. 2021; 11(5):650. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050650
Chicago/Turabian StyleWende, Tim, Johannes Kasper, Florian Wilhelmy, Eric Dietel, Gordian Hamerla, Cordula Scherlach, Jürgen Meixensberger, and Michael Karl Fehrenbach. 2021. "Assessment of a Reliable Fractional Anisotropy Cutoff in Tractography of the Corticospinal Tract for Neurosurgical Patients" Brain Sciences 11, no. 5: 650. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050650