
Let Me See: Correlation between 5-ALA Fluorescence and Molecular Pathways in Glioblastoma: A Single Center Experience

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Procedure
2.3. Post-Operative Management
2.4. Statistical Analysis
3. Results
3.1. Interobserver Concordance
3.2. IDH-1/2 Mutation Status
3.3. Role of Mitotic Index, Gender, Age
3.4. MGMT Promoter Methylation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Mirimanoff, R.-O.; Gorlia, T.; Mason, W.; Bent, M.V.D.; Kortmann, R.-D.; Fisher, B.; Reni, M.; Brandes, A.; Curschmann, J.; Villa, S.; et al. Radiotherapy and Temozolomide for Newly Diagnosed Glioblastoma: Recursive Partitioning Analysis of the EORTC 26981/22981-NCIC CE3 Phase III Randomized Trial. J. Clin. Oncol. 2006, 24, 2563–2569. [Google Scholar] [CrossRef]
- Buckner, J.C. Factors influencing survival in high-grade gliomas. Semin. Oncol. 2003, 30, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Smrdel, U.; Kovac, V.; Popović, M.; Zwitter, M. Glioblastoma patients in Slovenia from 1997 to 2008. Radiol. Oncol. 2014, 48, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altieri, R.; Zeppa, P.; Melcarne, A.; Tardivo, V.; Soffietti, R.; Mantovan, C.; Rudà, R.; Chiovatero, I.; Franchino, F.; Martini, S.; et al. Supratotal resection of glioblastoma: Is less more? Surg. Technol. Int. 2019, 35, 1–9. [Google Scholar]
- Altieri, R.; Melcarne, A.; Di Perna, G.; Specchia, F.M.C.; Fronda, C.; La Rocca, G.; Cofano, F.; Sabatino, G.; Della Pepa, G.M.; Olivi, A.; et al. Intra-Operative Ultrasound: Tips and Tricks for Making the Most in Neurosurgery. Surg. Technol. Int. 2018, 33, 353–360. [Google Scholar]
- Altieri, R.; Raimondo, S.; Tiddia, C.; Sammarco, D.; Cofano, F.; Zeppa, P.; Monticelli, M.; Melcarne, A.; Junemann, C.; Zenga, F.; et al. Glioma surgery: From preservation of motor skills to conservation of cognitive functions. J. Clin. Neurosci. 2019, 70, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Monticelli, M.; Zeppa, P.; Zenga, F.; Altieri, R.; Mammi, M.; Bertero, L.; Castellano, I.; Cassoni, P.; Melcarne, A.; La Rocca, G.; et al. The post-surgical era of GBM: How molecular biology has impacted on our clinical management. A review. Clin. Neurol. Neurosurg. 2018, 170, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Altieri, R.; Zenga, F.; Ducati, A.; Melcarne, A.; Cofano, F.; Mammi, M.; Di Perna, G.; Savastano, R.; Garbossa, D. Tumor location and patient age predict biological signatures of high-grade gliomas. Neurosurg. Rev. 2017, 41, 599–604. [Google Scholar] [CrossRef]
- Gambella, A.; Senetta, R.; Collemi, G.; Vallero, S.G.; Monticelli, M.; Cofano, F.; Zeppa, P.; Garbossa, D.; Pellerino, A.; Rudà, R.; et al. NTRK Fusions in Central Nervous System Tumors: A Rare, but Worthy Target. Int. J. Mol. Sci. 2020, 21, 753. [Google Scholar] [CrossRef] [Green Version]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.-J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Valdés, P.A.; Leblond, F.; Kim, A.; Harris, B.T.; Wilson, B.C.; Fan, X.; Tosteson, T.D.; Hartov, A.; Ji, S.; Erkmen, K.; et al. Quantitative fluorescence in intracranial tumor: Implications for ALA-induced PpIX as an intraoperative biomarker. J. Neurosurg. 2011, 115, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Zeppa, P.; Neitzert, L.; Mammi, M.; Monticelli, M.; Altieri, R.; Castaldo, M.; Cofano, F.; Borrè, A.; Zenga, F.; Melcarne, A.; et al. How Reliable Are Volumetric Techniques for High-Grade Gliomas? A Comparison Study of Different Available Tools. Neurosurgery 2020, 87, 672. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, G.; Cofano, F.; Salvati, L.; Monticelli, M.; Zeppa, P.; Di Perna, G. Fluorescence-guided Surgery for High Grade Gliomas: State of The Art and New Perspectives. Technol. Cancer Res. Treat. 2021. published ahead of print. [Google Scholar] [CrossRef]
- Stummer, W.; Stepp, H.; Wiestler, O.D.; Pichlmeier, U. Randomized, Prospective Double-Blinded Study Comparing 3 Different Doses of 5-Aminolevulinic Acid for Fluorescence-Guided Resections of Malignant Gliomas. Neurosurgery 2017, 81, 230–239. [Google Scholar] [CrossRef] [Green Version]
- Riva, M. Brain tumoral epilepsy: A review. Neurol. Sci. 2005, 26, s40–s42. [Google Scholar] [CrossRef] [PubMed]
- Jaber, M.; Wölfer, J.; Ewelt, C.; Holling, M.; Hasselblatt, M.; Niederstadt, T.; Zoubi, T.; Weckesser, M.; Stummer, W. The Value of 5-Aminolevulinic Acid in Low-grade Gliomas and High-grade Gliomas Lacking Glioblastoma Imaging Features: An Analysis Based on Fluorescence, Magnetic Resonance Imaging, 18F-Fluoroethyl Tyrosine Positron Emission Tomography, and Tumor Molecular Factors. Neurosurgery 2016, 78, 401–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ewelt, C.; Floeth, F.W.; Felsberg, J.; Steiger, H.J.; Sabel, M.; Langen, K.-J.; Stoffels, G.; Stummer, W. Finding the anaplastic focus in diffuse gliomas: The value of Gd-DTPA enhanced MRI, FET-PET, and intraoperative, ALA-derived tissue fluorescence. Clin. Neurol. Neurosurg. 2011, 113, 541–547. [Google Scholar] [CrossRef]
- Yamamoto, T.; Ishikawa, E.; Miki, S.; Sakamoto, N.; Zaboronok, A.; Matsuda, M.; Akutsu, H.; Nakai, K.; Tsuruta, W.; Matsumura, A.; et al. Photodynamic Diagnosis Using 5-Aminolevulinic Acid in 41 Biopsies for Primary Central Nervous System Lymphoma. Photochem. Photobiol. 2015, 91, 1452–1457. [Google Scholar] [CrossRef] [Green Version]
- Millesi, M.; Kiesel, B.; Mischkulnig, M.; Martínez-Moreno, M.; Woehrer, A.; Wolfsberger, S.; Knosp, E.; Widhalm, G. Analysis of the surgical benefits of 5-ALA–induced fluorescence in intracranial meningiomas: Experience in 204 meningiomas. J. Neurosurg. 2016, 125, 1408–1419. [Google Scholar] [CrossRef] [Green Version]
- Foster, N.; Eljamel, S. ALA-induced fluorescence image guided surgery of meningiomas: A meta-analyses. Photodiagnosis Photodyn. Ther. 2016, 15, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Kamp, M.A.; Fischer, I.; Bühner, J.; Turowski, B.; Cornelius, J.F.; Steiger, H.-J.; Rapp, M.; Slotty, P.J.; Sabel, M. 5-ALA fluorescence of cerebral metastases and its impact for the local-in-brain progression. Oncotarget 2016, 7, 66776–66789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongetta, D.; Tartara, F.; Pagella, F.; Somma, T.; Cavaliere, M.; Di Perna, G.; Zenga, F.; Cofano, F.; Garbossa, D.; Zoia, C. Fluorophores Use in Pituitary Surgery: A Pharmacokinetics and Pharmacodynamics Appraisal. Brain Sci. 2021, 11, 565. [Google Scholar] [CrossRef] [PubMed]
- Darryl, L.; Shawn, L.H.-J.; Susan, C.; Annette, M.M.; Michael, W.M.; Joanna, J.P.; Mitchel, S.B. A prospective Phase II clinical trial of 5-aminolevulinic acid to assess the correlation of intraoperative fluorescence intensity and degree of histologic cellularity during resection of high-grade gliomas. J. Neurosurg. JNS 2016, 124, 1300–1309. [Google Scholar] [CrossRef] [Green Version]
- Rita, H.; Kinoshita, M.; Kagawa, N.; Fujimoto, Y.; Kishima, H.; Hashimoto, N.; Yoshimine, T. 11C-methionine uptake and intraoperative 5-aminolevulinic acid-induced fluorescence as separate index markers of cell density in glioma. Cancer 2011, 118, 1619–1627. [Google Scholar] [CrossRef]
- Rampazzo, E.; Della Puppa, A.; Frasson, C.; Battilana, G.; Bianco, S.; Scienza, R.; Basso, G.; Persano, L. Erratum to: Phenotypic and functional characterization of Glioblastoma cancer stem cells identified through 5-aminolevulinic acid-assisted surgery. J. Neuro-Oncol. 2014, 120, 221. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Nakada, M.; Hayashi, Y.; Nakada, S.; Sawada-Kitamura, S.; Furuyama, N.; Suzuki, T.; Kamide, T.; Hayashi, Y.; Yano, S.; et al. Epithelioid glioblastoma changed to typical glioblastoma: The methylation status of MGMT promoter and 5-ALA fluorescence. Brain Tumor Pathol. 2010, 28, 59–64. [Google Scholar] [CrossRef]
- Reitman, Z.J.; Yan, H. Isocitrate Dehydrogenase 1 and 2 Mutations in Cancer: Alterations at a Crossroads of Cellular Metabolism. J. Natl. Cancer Inst. 2010, 102, 932–941. [Google Scholar] [CrossRef] [Green Version]
- Toedt, G.; Barbus, S.; Wolter, M.; Felsberg, J.; Tews, B.; Blond, F.; Sabel, M.C.; Hofmann, S.; Becker, N.; Hartmann, C.; et al. Molecular signatures classify astrocytic gliomas byIDH1mutation status. Int. J. Cancer 2010, 128, 1095–1103. [Google Scholar] [CrossRef]
- Rudà, R.; Trevisan, E.; Soffietti, R. Epilepsy and brain tumors. Curr. Opin. Oncol. 2010, 22, 611–620. [Google Scholar] [CrossRef]
- Toledo, M.; Sarria-Estrada, S.; Quintana, M.; Maldonado, X.; Martinez-Ricarte, F.; Rodon, J.; Auger, C.; Aizpurua, M.; Salas-Puig, J.; Santamarina, E.; et al. Epileptic features and survival in glioblastomas presenting with seizures. Epilepsy Res. 2017, 130, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Toledo, M.; Sarria-Estrada, S.; Quintana, M.; Maldonado, X.; Martinez-Ricarte, F.; Rodon, J.; Auger, C.; Salas-Puig, J.; Santamarina, E.; Martinez-Saez, E. Prognostic implications of epilepsy in glioblastomas. Clin. Neurol. Neurosurg. 2015, 139, 166–171. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| IDH-1/2 Mutation | IDH-1/2 Wild-Type | ||
|---|---|---|---|
| n = 28 | n = 16 | p | |
| Male (n = 28) | 20 (71.4%) | 8 (50%) | 0.24 |
| Female (n = 16) | 8 (28.6%) | 8 (50%) | 0.24 |
| Age | 66.4 ± 2.5 | 63.3 ± 3 | 0.43 |
| Presentation | |||
| Progressive neurological deficit | 21 (75%) | 12 (80%) | 0.96 |
| Pure motor deficit | 1 (3.6%) | 3 (20%) | 0.11 |
| Headache | 3 (10.7%) | 4 (26.7%) | 0.22 |
| Seizures | 7 (25%) | 0 | 0.08 |
| Methylation of MGMT Promoter | 17 (60.7%) | 7 (46.7%) | 0.38 |
| Methylation degree | n = 14 | n = 7 | 0.72 |
| High | 5 (35.7%) | 2 (28.6%) | |
| Intermediate | 4 (28.6%) | 1 (14.3%) | |
| Low | 5 (35.7%) | 4 (57.1%) | |
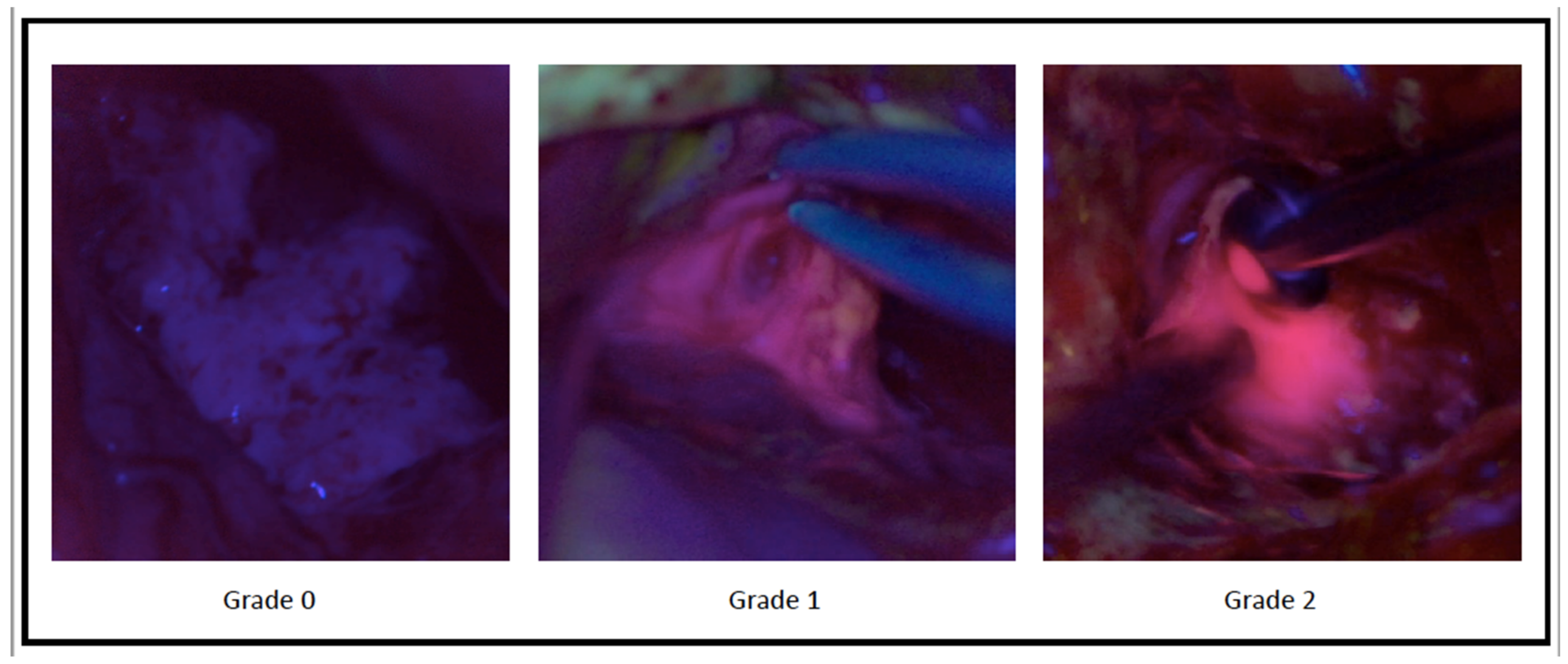
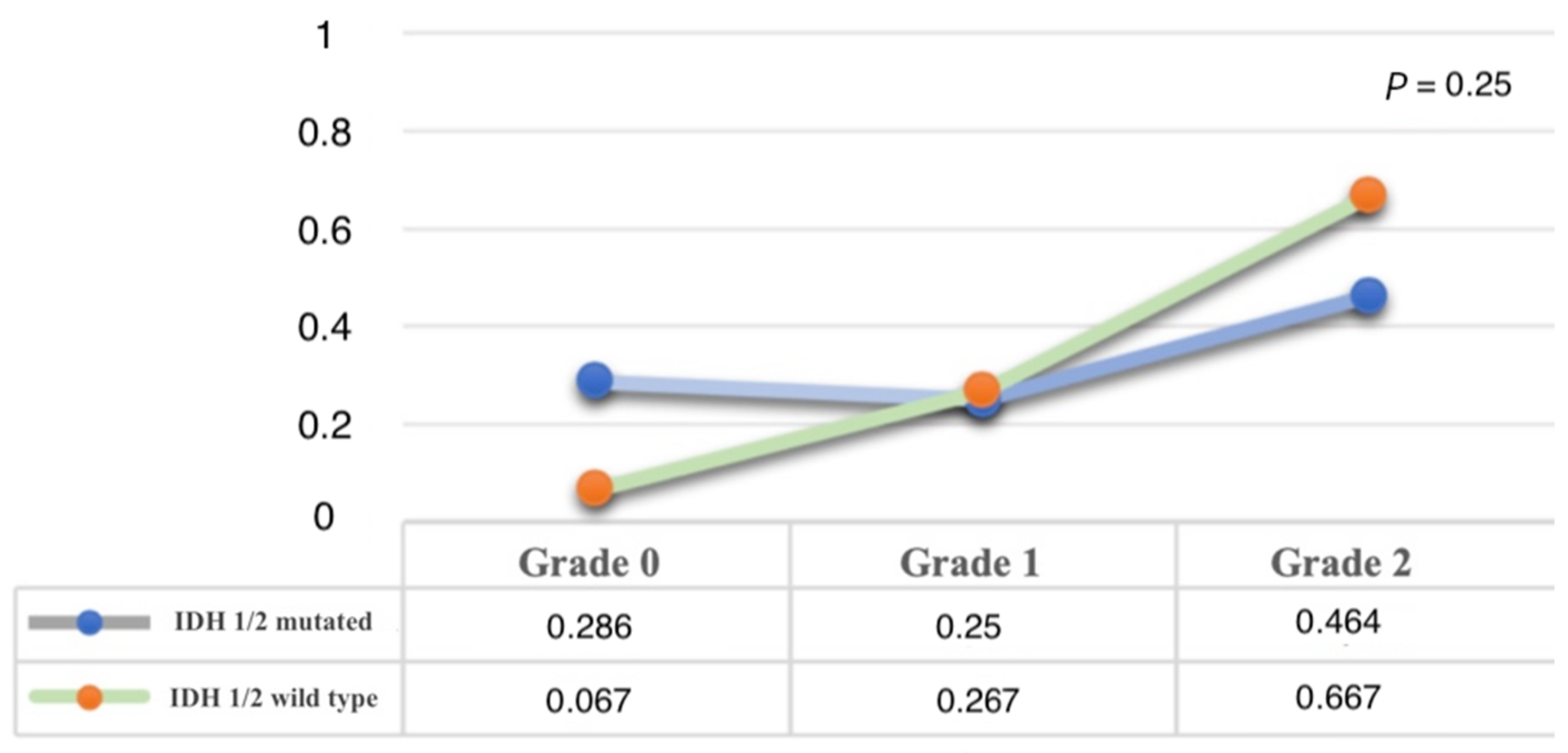
| Fluorescence Grade | 0.25 | ||
| Grade 0—No fluorescence | 8 (28.6%) | 1 (6.7%) | |
| Grade 1—“Weak” fluorescence | 7 (25%) | 4 (26.7%) | |
| Grade 2—“Strong” fluorescence | 13 (46.4%) | 10 (66.7%) | |
| Mitotic Index | 31.8 ± 11 | 43.9 ± 21.1 | 0.13 |
| Mitosis | 11.2 ± 7.4 | 11.0 ± 6.7 | 0.96 |
| Correlation between Fluorescence Grade and Mitotic Index | p = 0.93 |
|---|---|
| Grade 0—No fluorescence | 34.8 ± 12.1 |
| Grade 1—“Weak” fluorescence | 37.2 ± 19.3 |
| Grade 2—“Strong” fluorescence | 35.0 ± 15.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Specchia, F.M.C.; Monticelli, M.; Zeppa, P.; Bianconi, A.; Zenga, F.; Altieri, R.; Pugliese, B.; Di Perna, G.; Cofano, F.; Tartara, F.; et al. Let Me See: Correlation between 5-ALA Fluorescence and Molecular Pathways in Glioblastoma: A Single Center Experience. Brain Sci. 2021, 11, 795. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060795
Specchia FMC, Monticelli M, Zeppa P, Bianconi A, Zenga F, Altieri R, Pugliese B, Di Perna G, Cofano F, Tartara F, et al. Let Me See: Correlation between 5-ALA Fluorescence and Molecular Pathways in Glioblastoma: A Single Center Experience. Brain Sciences. 2021; 11(6):795. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060795
Chicago/Turabian StyleSpecchia, Francesco Maria Calamo, Matteo Monticelli, Pietro Zeppa, Andrea Bianconi, Francesco Zenga, Roberto Altieri, Beatrice Pugliese, Giuseppe Di Perna, Fabio Cofano, Fulvio Tartara, and et al. 2021. "Let Me See: Correlation between 5-ALA Fluorescence and Molecular Pathways in Glioblastoma: A Single Center Experience" Brain Sciences 11, no. 6: 795. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060795