
Comparison of the Immunogenicity and Protective Efficacy of Various SARS-CoV-2 Vaccines among Healthcare Workers: Are Our White Coat Armies Protected?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Neutralizing IgG Seroprevalence and Titer Rates Correlation with HCWs Demographics
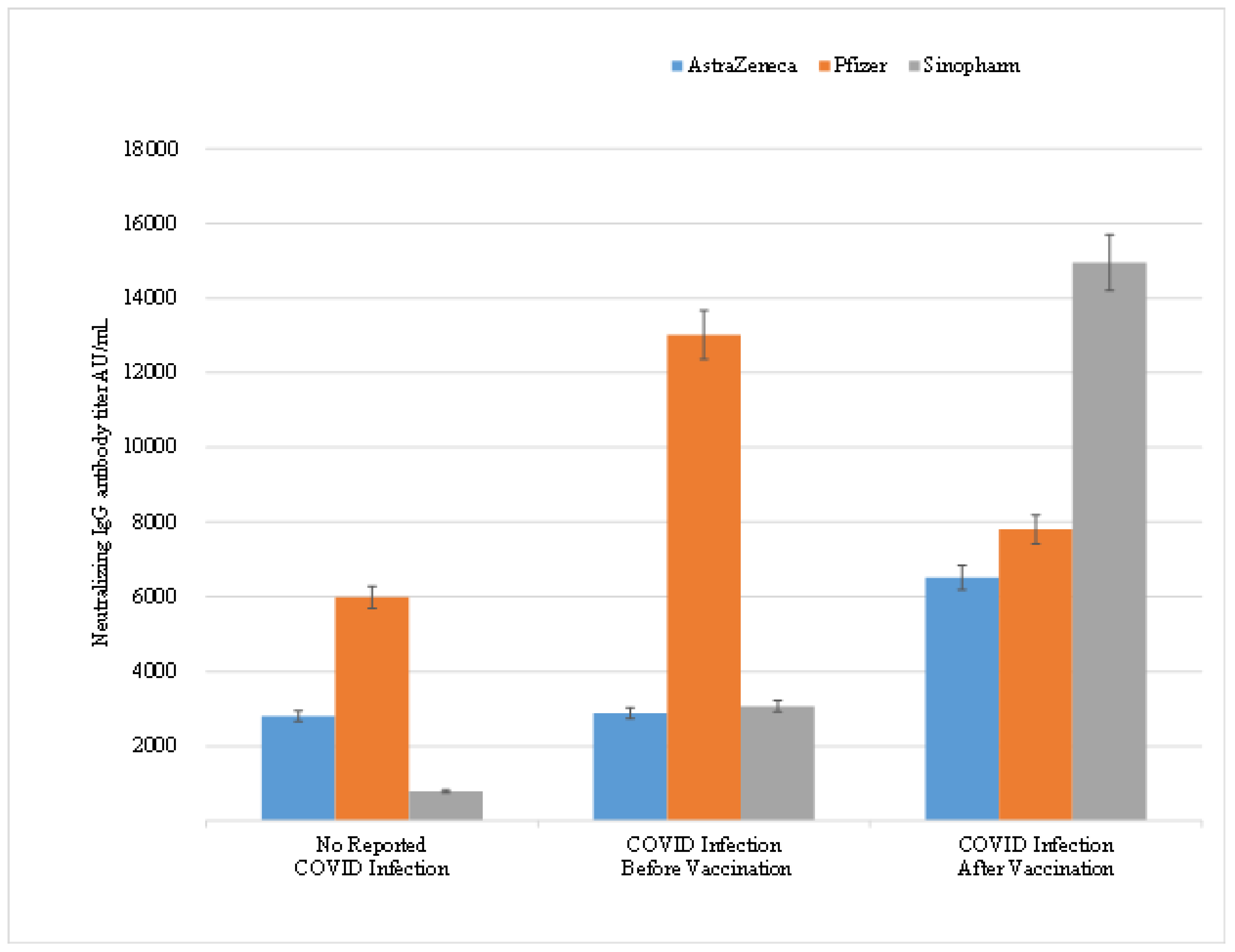
3.2. The Effect of COVID-19 Infection on Neutralizing IgG Antibodies Titer in HCWs
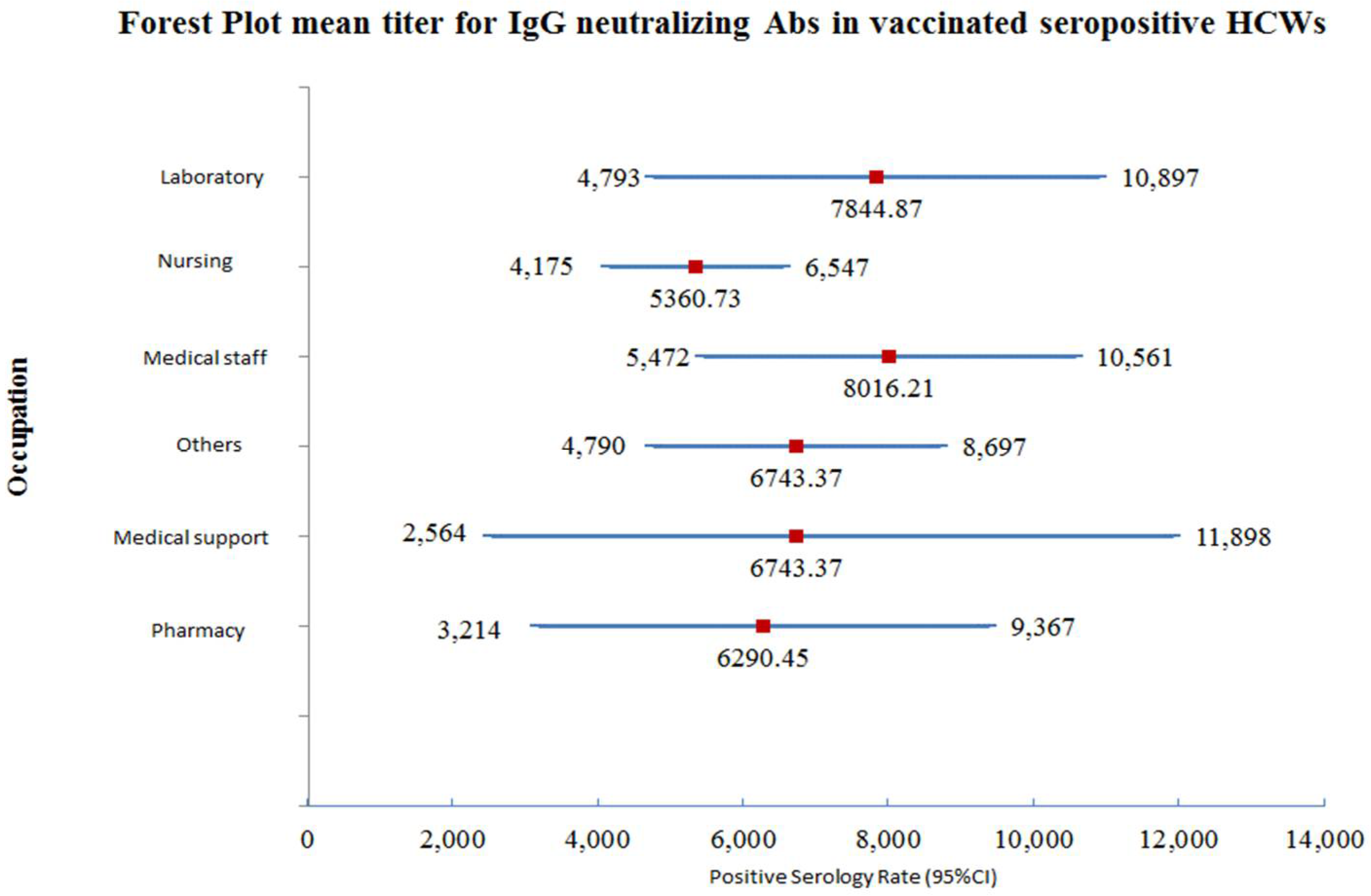
3.3. Neutralizing IgG Antibody Titer Correlation with the Occupation of HCW
3.4. Correlation between Clinicopathological Characteristics and Production of Neutralizing Antibody Titer
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Test | Age | Gender | Unit | Lower Limit of Normal Range | Upper Limit of Normal Range | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Hemoglobin (HB) | 18 | 99 | Female | g/dL | 12 | 16 |
| 18 | 99 | Male | g/dL | 13 | 18 | |
| White blood cell count (WBCs) | 18 | 99 | Both | 103/uL | 4 | 11 |
| Lymphocytes | 18 | 99 | Both | 103/uL | 0.9 | 3.4 |
| Neutrophils | 18 | 99 | Both | 103/uL | 2.2 | 7.1 |
| Platelets | 18 | 99 | Both | 103/uL | 150 | 400 |
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Team MCVT. COVID-19 Vaccine Tracker. JORDAN: 4 Vaccines Approved for Use in Jordan. McGill University McGill University Interdisciplinary Initiative in Infection and Immunity (MI4). 2021. Available online: https://covid19.trackvaccines.org/country/jordan/ (accessed on 5 November 2021).
- Au, J. Higher Vaccination Rate Predicts Reduction in SARS-CoV-2 Transmission across the United States. medRxiv 2021. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, D.; Mangia, A.; Spano, M.S.; Zaffarano, L.; Vigano, M.; Di Resta, C.; Locatelli, M.; Ciceri, F.; De Vecchi, E. Quantitative serological evaluation as a valuable tool in the COVID-19 vaccination campaign. Clin. Chem. Lab. Med. 2021, 59, 2019–2026. [Google Scholar] [CrossRef]
- Glampson, B.; Brittain, J.; Kaura, A.; Mulla, A.; Mercuri, L.; Brett, S.J.; Aylin, P.; Sandall, T.; Goodman, I.; Redhead, J.; et al. Assessing COVID-19 Vaccine Uptake and Effectiveness Through the North West London Vaccination Program: Retrospective Cohort Study. JMIR Public Health Surveill. 2021, 7, e30010. [Google Scholar] [CrossRef]
- Alqutob, R.; Al Nsour, M.; Tarawneh, M.R.; Ajlouni, M.; Khader, Y.; Aqel, I.; Kharabsheh, S.; Obeidat, N. COVID-19 Crisis in Jordan: Response, Scenarios, Strategies, and Recommendations. JMIR Public Health Surveill. 2020, 6, e19332. [Google Scholar] [CrossRef]
- AlQutob, R.; Moonesar, I.A.; Tarawneh, M.R.; Al Nsour, M.; Khader, Y. Public Health Strategies for the Gradual Lifting of the Public Sector Lockdown in Jordan and the United Arab Emirates During the COVID-19 Crisis. JMIR Public Health Surveill. 2020, 6, e20478. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B. The Battle Against COVID-19 in Jordan: An Early Overview of the Jordanian Experience. Front. Public Health 2020, 8, 188. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report—83; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Luck, T. New Lockdown Measures for Jordan as Nine Doctors Die in Covid-19 Surge, The National, 1 November 2020. Available online: https://www.thenationalnews.com/world/mena/new-lockdown-measures-for-jordan-as-nine-doctors-die-in-covid-19-surge-1.1103558 (accessed on 13 January 2021).
- Erdem, H.; Lucey, D.R. Healthcare worker infections and deaths due to COVID-19: A survey from 37 nations and a call for WHO to post national data on their website. Int. J. Infect. Dis. 2021, 102, 239–241. [Google Scholar] [CrossRef]
- WHO. The Impact of COVID-19 on Health and Care Workers: A Closer Look at Deaths. World Health Organization: Geneva, Switzerland, September 2021. Contract No.: WHO reference number: WHO/HWF/WorkingPaper/2021.1. Available online: https://apps.who.int/iris/bitstream/handle/10665/345300/WHO-HWF-WorkingPaper-2021.1-eng.pdf (accessed on 13 January 2021).
- Mortgat, L.; Verdonck, K.; Hutse, V.; Thomas, I.; Barbezange, C.; Heyndrickx, L.; Fischer, N.; Vuylsteke, B.; Kabouche, I.; Ariën, K.K.; et al. Prevalence and incidence of anti-SARS-CoV-2 antibodies among healthcare workers in Belgian hospitals before vaccination: A prospective cohort study. BMJ Open 2021, 11, e050824. [Google Scholar] [CrossRef] [PubMed]
- AFP. Jordan Launches Covid Vaccination Campaign. FRANCE 24, 13 January 2021. Available online: https://medicalxpress.com/news/2021-01-jordan-covid-vaccination-campaign.html (accessed on 13 January 2021).
- Jordanian Ministry of Health. Vaccines and Medicines for Corona Virus; Jordan Food and Drug Administration: Amman, Jordan, 2021.
- COVID-19 Statistical Report—Amman, Jordan 2021. Available online: https://corona.moh.gov.jo/en (accessed on 5 November 2021).
- Sughayer, M.A.; Mansour, A.; Al Nuirat, A.; Souan, L.; Ghanem, M.; Siag, M. Dramatic rise in seroprevalence rates of SARS-CoV-2 antibodies among healthy blood donors: The evolution of a pandemic. Int. J. Infect. Dis. 2021, 107, 116–120. [Google Scholar] [CrossRef] [PubMed]
- ABBOTT. AdviseDx SARS-CoV-2 IgG II. Abbott Ireland: ABBOTT; March 2021. Available online: https://www.fda.gov/media/146372/download.
- Brehm, T.T.; Thompson, M.; Ullrich, F.; Schwinge, D.; Addo, M.M.; Spier, A.; Knobloch, J.K.; Aepfelbacher, M.; Lohse, A.W.; Lütgehetmann, M.; et al. Low SARS-CoV-2 infection rates and high vaccine-induced immunity among German healthcare workers at the end of the third wave of the COVID-19 pandemic. Int. J. Hyg. Environ. Health 2021, 238, 113851. [Google Scholar] [CrossRef] [PubMed]
- Badano, M.N.; Sabbione, F.; Keitelman, I.; Pereson, M.; Aloisi, N.; Colado, A.; Ramos, M.V.; Wilczyñski, J.M.O.; Pozner, R.G.; Castillo, L.; et al. Humoral response to the BBIBP-CorV vaccine over time in healthcare workers with or without exposure to SARS-CoV-2. Mol. Immunol. 2022, 143, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Dashdorj, N.J.; Wirz, O.F.; Roltgen, K.; Haraguchi, E.; Buzzanco, A.S., 3rd; Sibai, M.; Wang, H.; Miller, J.A.; Solis, D.; Sahoo, M.K.; et al. Direct comparison of antibody responses to four SARS-CoV-2 vaccines in Mongolia. Cell Host Microbe 2021, 29, 1738–1743. [Google Scholar] [CrossRef] [PubMed]


| Label | Total N = 510 | COVID Vaccinated N = 474 (92.9%) | Not Vaccinated N = 36 (7.1%) | p-Value |
|---|---|---|---|---|
| F | 229 (44.9%) | 219 (95.6%) | 10 (4.4%) | 0.0321 |
| M | 281 (55.1%) | 255 (90.7%) | 26 (9.2%) |
| Value | Mean Titer (Range) AU/mL | p-Value |
|---|---|---|
| F | 5827.2 (0.0, 40,000) | 0.762 |
| M | 6687.4 (11.4, 40,000) |
| Vaccinated HCWs N = 466 95.88% | Seropositive/Immune | * p-Value | Negative | ||
| 452 (96.99%) | 14 (3.00%) | ||||
| * Previous COVID-19 infection | * No reported Infection | Previous COVID-19 Infection | No Reported Infection | ||
| 209 (46.23%) | 242 (53.53%) | 0.12 | 0 (0%) | 14 (100%) | |
| Unvaccinated HCWs N = 19 3.90% | Seropositive/Immune | ** p-value | Negative | ||
| 13 (68.42%) | 6 (31.57%) | ||||
| ** Previous COVID-19 infection | ** No reported Infection | Previous COVID-19 infection | No reported Infection | ||
| 8 (61.53%) | 5 (38.46%) | 0.41 | 0 (0%) | 6 (100%) | |
| COVID-19 Infection. | Mean Titer (Range) AU/mL | p-Value |
|---|---|---|
| No | 3774.6 (0.0–40,000) | <0.0001 |
| Yes | 9414.1 (131.6–40,000) |
| Vaccine Type | COVID-19 Infection (Yes/No) | Mean (Min, Max) Titer AU/mL | p-Value |
|---|---|---|---|
| AstraZeneca | No | 2805 (38.1–27,965) | 0.005 |
| Yes | 3019 (251.0–9006) | ||
| Pfizer/BioNTech | No | 4702 (0.0–36,213) | <0.0001 |
| Yes | 10,925 (760.9–39,441) | ||
| Sinopharm | No | 778.2 (11.4–17,813) | <0.0001 |
| Yes | 3261 (131.6–31,159) |
| Vaccine Type | No Reported COVID-19 Infection | COVID-19 Infection before Vaccination | COVID-19 Infection after Vaccination | p-Value | |
|---|---|---|---|---|---|
| AstraZeneca | Total number of HCWs | 59 | 33 | 2 | |
| Total N = 94 | Titer Mean AU/mL | 2805.117 | 2891.245 | 6512.25 | 0.443 |
| (95% CI) LL-UL | 1549.3–4060.9 | 2185.61–3596.87 | 1333.836–11,690.66 | ||
| Pfizer/BioNTech | Total number of HCWs | 117 | 128 | 2 | |
| Total N = 248 | Titer Mean AU/mL | 5981.834 | 13,018.115 | 7802.15 | 0.00 |
| (95% CI) LL-UL | 4359.53–7604.13 | 10,962.22–15,074.01 | −23,642.5–39,246.83 | ||
| Sinopharm | Total number of HCWs | 73 | 38 | 4 | |
| Total N = 116 | Titer Mean AU/mL | 787.9931507 | 3074.884211 | 14,947.45 | 0.00 |
| (95% CI) LL-UL | 148.55–1427.43 | 632.87–5516.899 | −12,034.3–41,929.2 |
| Occupation | Vaccinated, Seropositive HCWs | Unvaccinated, Seropositive HCWs | |||
|---|---|---|---|---|---|
| Previous COVID-19 Infection * | No Reported Infection * | p-Value * | Previous COVID-19 Infection | No Reported Infection | |
| Laboratory | 17 (41.46%) | 23 (56.09%) | 0.34 | 0 (0.00%) | 0 (0.00%) |
| Nursing | 87 (50.28%) | 86 (49.71%) | 0.94 | 3 (75%) | 1 (25%) |
| Medical Staff | 45 (50%) | 45 (50%) | 1 | 2 (50%) | 2 (50%) |
| Others | 40 (40%) | 60 (60%) | 0.05 | 3 (60%) | 2 (40%) |
| Support Staff | 10 (50%) | 10 (50%) | 1 | 0 (0.00%) | 0 (0.00%) |
| Pharmacy | 10 (35.71%) | 18 (64.28%) | 0.13 | 0 (0.00%) | 0 (0.00%) |
| Variant | Mean Titer (Range) AU/mL | p-Value | |
|---|---|---|---|
| Blood Group | A | 6217.8 (15.9–40,000) | 0.241 |
| AB | 8276.9 (354.7–40,000) | ||
| B | 6082.8 (33.6–40,000) | ||
| O | 6157.5 (0.0–40,000) | ||
| HB | Normal | 6051.0 (0.0–40,000) | 0.368 |
| Not Normal | 7386.9 (39.4–40,000) | ||
| WBCs | Normal | 6221.0 (11.4–40,000) | 0.492 |
| Not Normal | 3607.2 (23.3–18,178) | ||
| Lymphocytes 103/uL | Normal | 6350.5 (11.4–40,000) | 0.106 |
| Not Normal | 4996.3 (23.3–40,000) | ||
| Platelets | Normal | 6120.5 (11.4–40,000) | 0.491 |
| Not Normal | 5837.9 (74.4–40,000) | ||
| Neutrophils 103/uL | Normal | 6254.6 (11.4–40,000) | 0.571 |
| Not Normal | 5920.1 (15.9–23,779) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souan, L.; Sughayer, M.A.; Abualhour, M.M.; Siag, M.; Al-Badr, S.; Al-Atrash, T. Comparison of the Immunogenicity and Protective Efficacy of Various SARS-CoV-2 Vaccines among Healthcare Workers: Are Our White Coat Armies Protected? Vaccines 2022, 10, 642. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050642
Souan L, Sughayer MA, Abualhour MM, Siag M, Al-Badr S, Al-Atrash T. Comparison of the Immunogenicity and Protective Efficacy of Various SARS-CoV-2 Vaccines among Healthcare Workers: Are Our White Coat Armies Protected? Vaccines. 2022; 10(5):642. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050642
Chicago/Turabian StyleSouan, Lina, Maher A. Sughayer, Maha M. Abualhour, Mahmoud Siag, Sara Al-Badr, and Tareq Al-Atrash. 2022. "Comparison of the Immunogenicity and Protective Efficacy of Various SARS-CoV-2 Vaccines among Healthcare Workers: Are Our White Coat Armies Protected?" Vaccines 10, no. 5: 642. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050642