
SARS-CoV-2 Antinucleocapsid Antibody Response of mRNA and Inactivated Virus Vaccines Compared to Unvaccinated Individuals

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants, Setting, and Ethical Consideration
2.2. Demographic and Clinical Characteristics of Population Study
2.3. Sample Collection
2.4. Sample Analysis
2.5. Statistical Analysis
3. Results
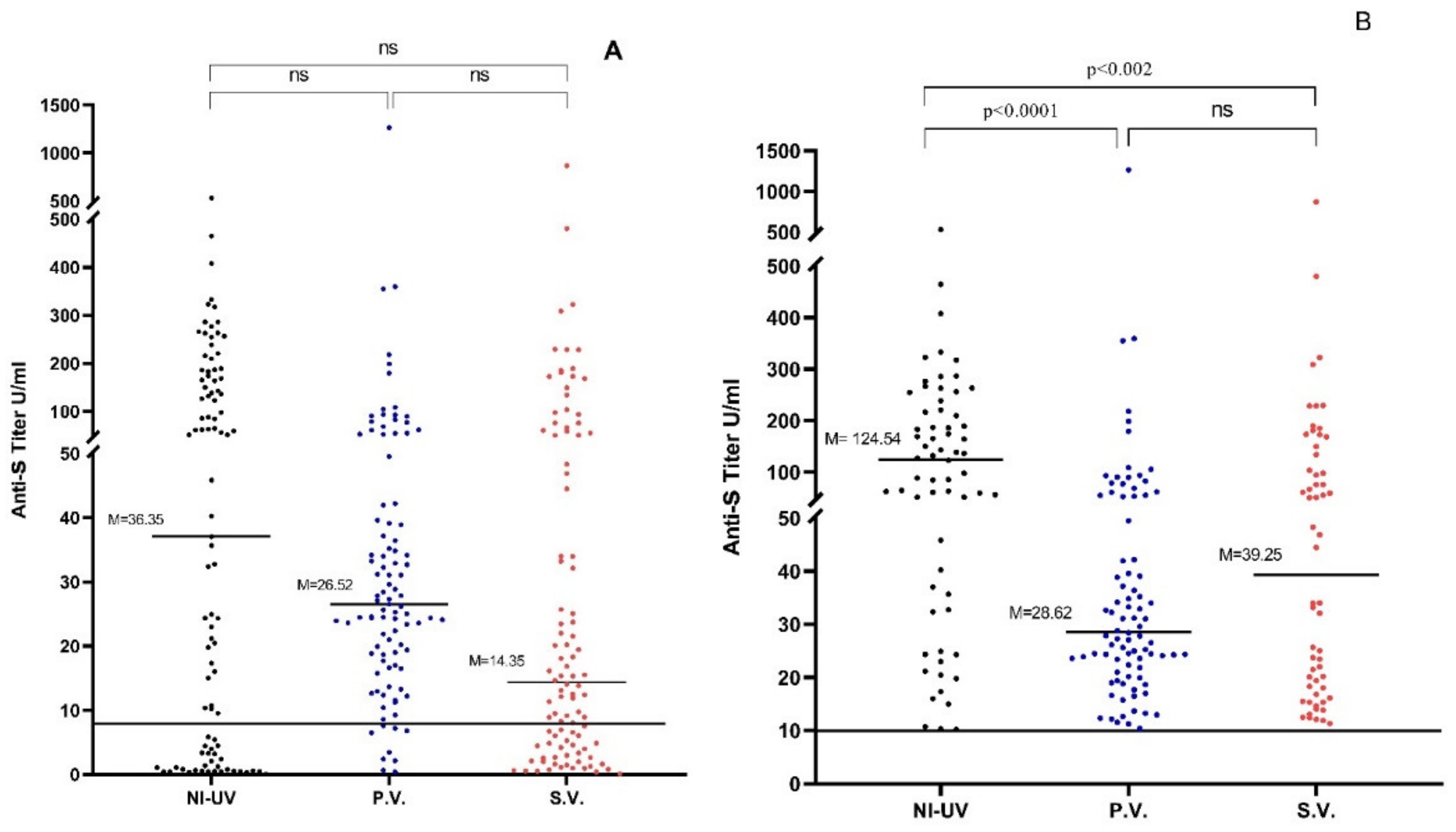
3.1. Comparing Anti-S IgG Levels in Naturally Infected Unvaccinated and Vaccinated Subjects
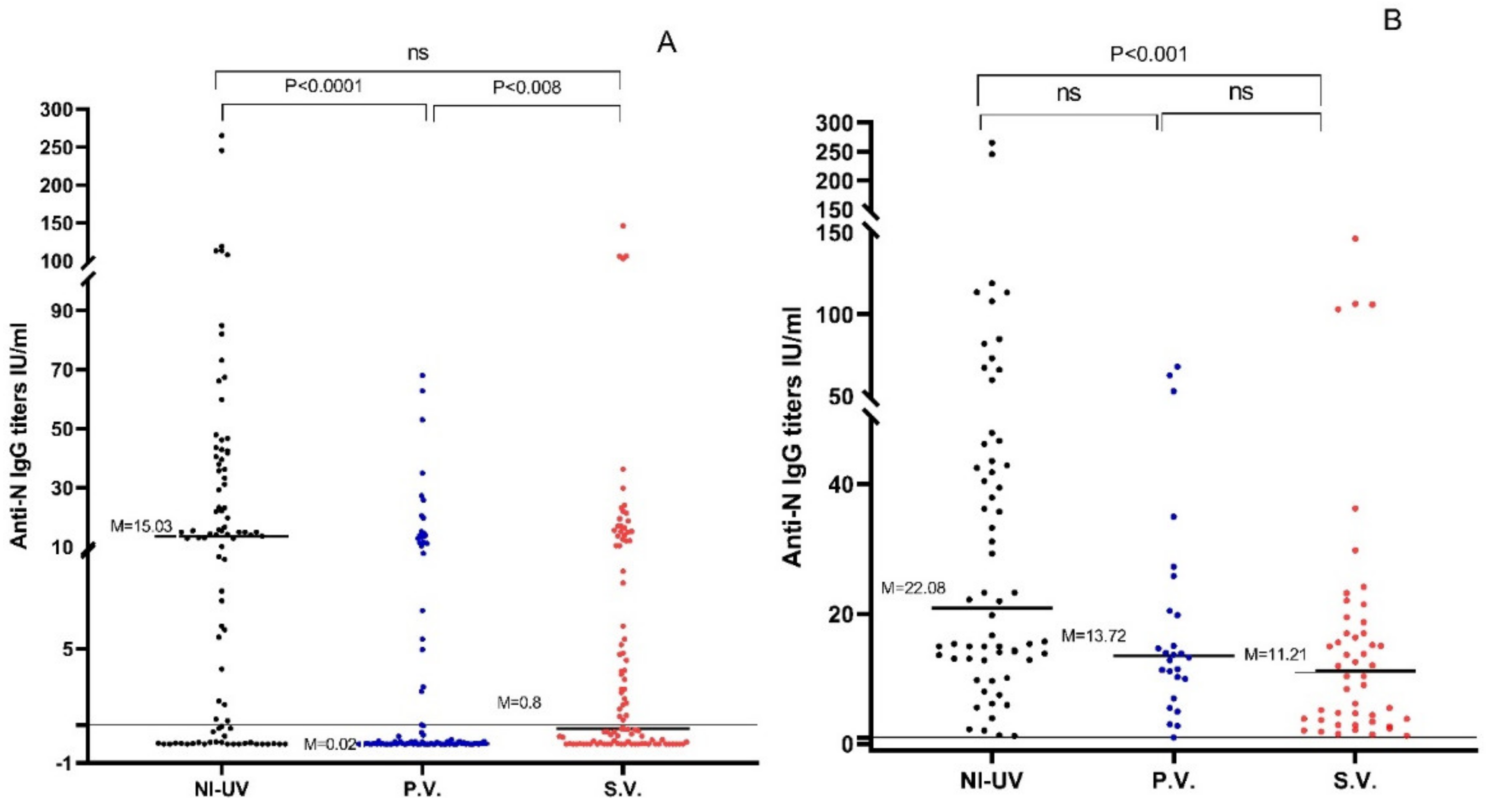
3.2. Comparing Anti-N IgG Levels in Naturally Infected Unvaccinated and Vaccinated Subjects
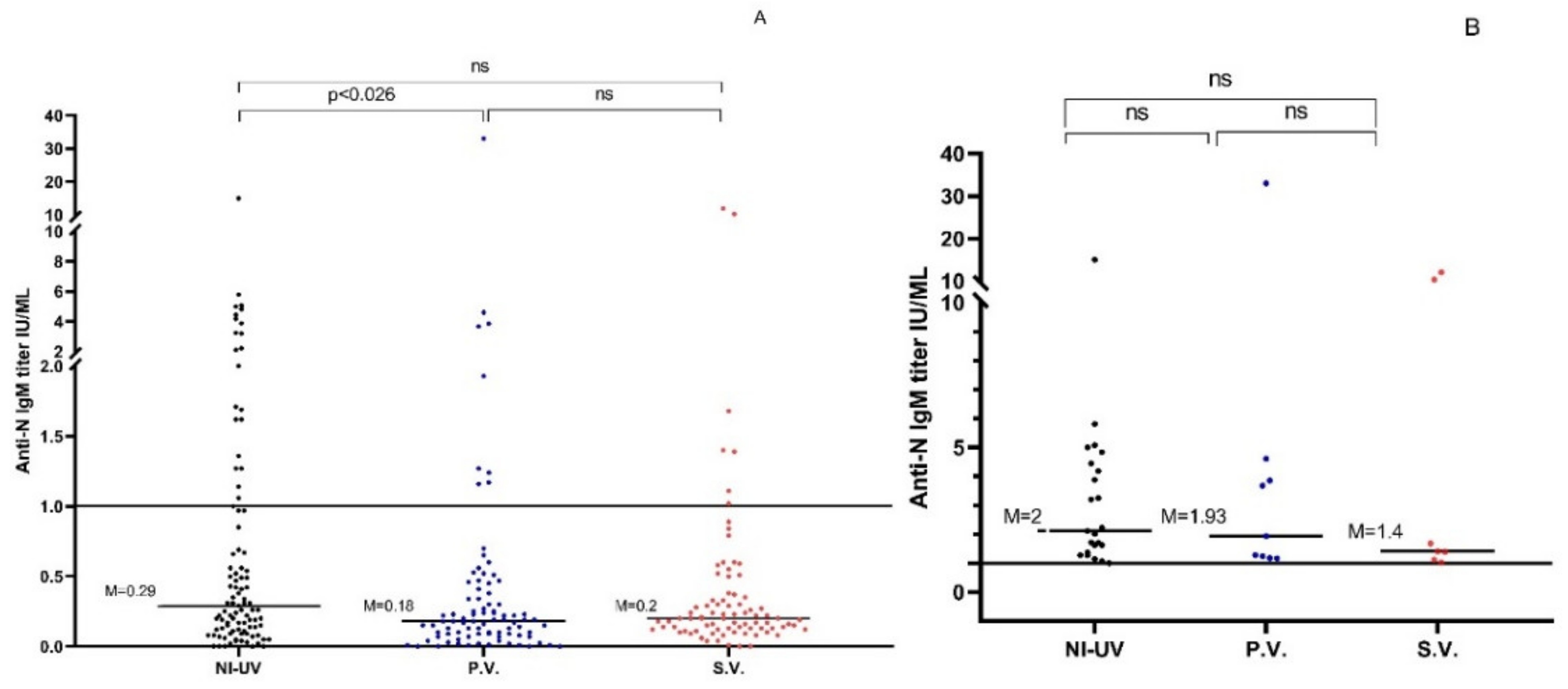
3.3. Comparing Anti-N IgM Antibody Levels in Naturally Infected Unvaccinated Group and Vaccinated Subjects
3.4. Anti-N and Anti-S IgG Titers of Anti-N IgM Positive Samples in the 3 Study Groups
3.5. Effect of Age, Gender, Chronic Diseases, Smoking, Previous Infection, Department Admission, and Symptom Severity on Anti-S and Anti-N Ab Levels in the 3 Study Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haidere, M.F.; Ratan, Z.A.; Nowroz, S.; Zaman, S.B.; Jung, Y.J.; Hosseinzadeh, H.; Cho, J.Y. COVID-19 Vaccine: Critical Questions with Complicated Answers. Biomol. Ther. 2021, 29, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.H.; Beiss, V.; Fiering, S.N.; Steinmetz, N.F. COVID-19 Vaccine Frontrunners and Their Nanotechnology Design. ACS Nano 2020, 14, 12522–12537. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, F.; Shen, C.; Peng, W.; Li, D.; Zhao, C.; Li, Z.; Li, S.; Bi, Y.; Yang, Y.; et al. A noncompeting pair of human neutralizing antibodies block COVID-19 virus binding to its receptor ACE2. Science 2020, 368, 1274–1278. [Google Scholar] [CrossRef]
- Lo Sasso, B.; Giglio, R.V.; Vidali, M.; Scazzone, C.; Bivona, G.; Gambino, C.M.; Ciaccio, A.M.; Agnello, L.; Ciaccio, M. Evaluation of Anti-SARS-CoV-2 S-RBD IgG Antibodies after COVID-19 mRNA BNT162b2 Vaccine. Diagnostics 2021, 11, 1135. [Google Scholar] [CrossRef] [PubMed]
- Jacofsky, D.; Jacofsky, E.M.; Jacofsky, M. Understanding Antibody Testing for COVID-19. J. Arthroplast. 2020, 35, S74–S81. [Google Scholar] [CrossRef]
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side Effects and Perceptions following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef]
- Status of COVID-19 Vaccines within WHO EUL/PQ Evaluation Process. Available online: https://www.google.com/search?client=firefox-b-d&q=7.+https%3A%2F%2Fextranet.who.int%2Fpqweb%2Fsites%2Fdefault%2Ffiles%2Fdocuments%2FStatus_COVID_VAX_23Dec2021.pdf (accessed on 23 January 2022).
- Rotondo, J.C.; Martini, F.; Maritati, M.; Mazziotta, C.; Di Mauro, G.; Lanzillotti, C.; Barp, N.; Gallerani, A.; Tognon, M.; Contini, C. SARS-CoV-2 Infection: New Molecular, Phylogenetic, and Pathogenetic Insights. Efficacy of Current Vaccines and the Potential Risk of Variants. Viruses 2021, 13, 1687. [Google Scholar] [CrossRef] [PubMed]
- Xing, K.; Tu, X.Y.; Liu, M.; Liang, Z.W.; Chen, J.N.; Li, J.J.; Jiang, L.G.; Xing, F.Q.; Jiang, Y. Efficacy and safety of COVID-19 vaccines: A systematic review. Zhongguo Dang Dai Er Ke Za Zhi Chin. J. Contemp. Pediatr. 2021, 23, 221–228. [Google Scholar]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- China’s COVID Vaccines Face Their Greatest Test yet: An Omicron Wave in Asia: ABC News. Available online: https://www.abc.net.au/news/2022-01-11/asia-omicron-and-chinas-vaccines-sinovac-and-sinopharm/100741650 (accessed on 23 January 2022).
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Van Boheemen, S.; de Graaf, M.; Lauber, C.; Bestebroer, T.M.; Raj, V.S.; Zaki, A.M.; Osterhaus, A.D.M.E.; Haagmans, B.L.; Gorbalenya, A.E.; Snijder, E.J.; et al. Genomic characterization of a newly discovered coronavirus associated with acute respiratory distress syndrome in humans. mBio 2012, 3, e00473-12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, B.; Drosten, C.; Müller, M.A. Serological assays for emerging coronaviruses: Challenges and pitfalls. Virus Res. 2014, 194, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Feng, Y.; Mo, X.; Zheng, P.; Wang, Q.; Li, P.; Peng, P.; Liu, X.; Chen, Z.; Huang, H.; et al. Kinetics of SARS-CoV-2 specific IgM and IgG responses in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 940–948. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Gao, G.F. Viral targets for vaccines against COVID-19. Nat. Rev. Immunol. 2021, 21, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Yan, R.; Zhang, J.; Zhang, G.; Zhang, Y.; Hao, M.; Zhang, Z.; Fan, P.; Dong, Y.; Yang, Y.; et al. A neutralizing human antibody binds to the N-terminal domain of the Spike protein of SARS-CoV-2. Science 2020, 369, 650–655. [Google Scholar] [CrossRef]
- De Haan, C.A.; Rottier, P.J. Molecular interactions in the assembly of coronaviruses. Adv. Virus Res. 2005, 64, 165–230. [Google Scholar]
- Atyeo, C.; Fischinger, S.; Zohar, T.; Slein, M.D.; Burke, J.; Loos, C.; McCulloch, D.J.; Newman, K.L.; Wolf, C.; Yu, J.; et al. Distinct Early Serological Signatures Track with SARS-CoV-2 Survival. Immunity 2020, 53, 524–532.e4. [Google Scholar] [CrossRef]
- Batra, M.; Tian, R.; Zhang, C.; Clarence, E.; Sacher, C.S.; Miranda, J.N.; de la Fuente, J.R.O.; Mathew, M.; Green, D.; Patel, S.; et al. Role of IgG against N-protein of SARS-CoV-2 in COVID19 clinical outcomes. Sci. Rep. 2021, 11, 3455. [Google Scholar] [CrossRef]
- Dashdorj, N.J.; Wirz, O.F.; Röltgen, K.; Haraguchi, E.; Buzzanco, A.S., 3rd; Sibai, M.; Wang, H.; Miller, J.A.; Solis, D.; Sahoo, M.K.; et al. Direct comparison of antibody responses to four SARS-CoV-2 vaccines in Mongolia. Cell Host Microbe 2021, 29, 1738–1743.e4. [Google Scholar] [CrossRef]
- Vályi-Nagy, I.; Matula, Z.; Gönczi, M.; Tasnády, S.; Bekő, G.; Réti, M.; Ajzner, É.; Uher, F. Comparison of antibody and T cell responses elicited by BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) vaccines against SARS-CoV-2 in healthy adult humans. Geroscience 2021, 43, 2321–2331. [Google Scholar] [CrossRef]
- Alqassieh, R.; Suleiman, A.; Abu-Halaweh, S.; Santarisi, A.; Shatnawi, O.; Shdaifat, L.; Tarifi, A.; Al-Tamimi, M.; Al-Shudifat, A.-E.; Alsmadi, H.; et al. Pfizer-BioNTech and Sinopharm: A Comparative Study on Post-Vaccination Antibody Titers. Vaccines 2021, 9, 1223. [Google Scholar] [CrossRef] [PubMed]
- Manaf, A.; Sujoy, B.; Abdulla, A.; Hamad Al, M.; Jaleela Al, S.; Jessica, J.; Wafaa El, S.; Jack, S.; Siddhartha, M. Morbidity and mortality from COVID-19 postvaccination breakthrough infections in association with vaccines and the emergence of variants in Bahrain. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Cristiano, A.; Pieri, M.; Sarubbi, S.; Pelagalli, M.; Calugi, G.; Tomassetti, F.; Bernardini, S.; Nuccetelli, M. Evaluation of serological anti-SARS-CoV-2 chemiluminescent immunoassays correlated to live virus neutralization test, for the detection of anti-RBD antibodies as a relevant alternative in COVID-19 large-scale neutralizing activity monitoring. Clin. Immunol. 2022, 234, 108918. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://www.nanoentek.com/theme/nanont2_en/mobile/shop/02/product01_view.php?it_id=1585699547 (accessed on 15 November 2021).
- Available online: http://www.fremm.es/portal/UserFiles/file/CORREOS%20ELECTRONICOS/2020/LABORATORIO%20FLORENCIANO%20SARS-CoV-2%20IgG%20(CLIA).pdf (accessed on 15 November 2021).
- Elliott, A.C.; Woodward, W.A. Statistical Analysis Quick Reference Guidebook: With SPSS Examples; Sage: Chicago, IL, USA, 2007. [Google Scholar]
- Available online: https://www.graphpad.com/scientific-software/prism/ (accessed on 27 February 2022).
- Locke, T. ‘No Guarantee of Anti-N Antibodies’ from COVID Infection. Available online: https://www.medscape.com/viewarticle/961933 (accessed on 23 January 2022).
- Choe, P.G.; Kang, C.K.; Suh, H.J.; Jung, J.; Song, K.H.; Bang, J.H.; Kim, E.S.; Kim, H.B.; Park, S.W.; Kim, N.J.; et al. Waning Antibody Responses in Asymptomatic and Symptomatic SARS-CoV-2 Infection. Emerg. Infect. Dis. 2021, 27, 327–329. [Google Scholar] [CrossRef]
- Kallaste, A.; Kisand, K.; Aart, A.; Kisand, K.; Peterson, P.; Lember, M. Antibody levels remain high to one-year’s follow-up after moderate and severe COVID-19, but not after mild cases. Infect. Dis. 2021, 54, 345–355. [Google Scholar] [CrossRef]
- Markmann, A.J.; Giallourou, N.; Bhowmik, D.R.; Hou, Y.J.; Lerner, A.; Martinez, D.R.; Premkumar, L.; Root, H.; van Duin, D.; Napravnik, S.; et al. Sex Disparities and Neutralizing-Antibody Durability to SARS-CoV-2 Infection in Convalescent Individuals. mSphere 2021, 6, e0027521, Erratum in mSphere 2021, 6, e0073621. [Google Scholar] [CrossRef]
- Lau, E.H.Y.; Tsang, O.T.Y.; Hui, D.S.C.; Kwan, M.Y.W.; Chan, W.H.; Chiu, S.S.; Ko, R.L.W.; Chan, K.H.; Cheng, S.M.S.; Perera, R.A.P.M.; et al. Neutralizing antibody titres in SARS-CoV-2 infections. Nat Commun. 2021, 12, 63. [Google Scholar] [CrossRef]
- Young, M.K.; Kornmeier, C.; Carpenter, R.M.; Natale, N.R.; Sasson, J.M.; Solga, M.D.; Mathers, A.J.; Poulter, M.D.; Qiang, X.; Petri, W.A. IgG Antibodies against SARS-CoV-2 Correlate with Days from Symptom Onset, Viral Load and IL-10. medRxiv 2020. [Google Scholar] [CrossRef]
- Klasse, P.J. Neutralization of Virus Infectivity by Antibodies: Old Problems in New Perspectives. Adv. Biol. 2014, 2014, 157895. [Google Scholar] [CrossRef] [Green Version]
- Arvin, A.M.; Fink, K.; Schmid, M.A.; Cathcart, A.; Spreafico, R.; Havenar-Daughton, C.; Lanzavecchia, A.; Corti, D.; Virgin, H.W. A perspective on potential antibody-dependent enhancement of SARS-CoV-2. Nature 2020, 584, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Foo, S.S.; Bruzzone, R.; Dinh, L.V.; King, N.J.; Mahalingam, S. Fc receptors in antibody-dependent enhancement of viral infections. Immunol. Rev. 2015, 268, 340–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flipse, J.; Diosa-Toro, M.A.; Hoornweg, T.E.; van de Pol, D.P.; Urcuqui-Inchima, S.; Smit, J.M. Antibody-Dependent Enhancement of Dengue Virus Infection in Primary Human Macrophages; Balancing Higher Fusion against Antiviral Responses. Sci. Rep. 2016, 6, 29201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, B.; Lin, H.; Yu, J.; Yu, J.; Hu, Z. Autophagy and the Immune Response. Adv. Exp. Med. Biol. 2019, 1206, 595–634. [Google Scholar] [PubMed]
- Li, W.; Zhou, J.; Wang, X.; Wu, Y.; Ye, L.; Wei, H.; Sun, R.; Tian, Z.; Peng, H. CD49a(+)CD49b(+) NK cells induced by viral infection reflect an activated state of conventional NK cells. Sci. China Life Sci. 2020, 63, 1725–1733. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Williams, M.; Nagabhushana, N.; Jani, V.; Defang, G.; Morrison, B.J. NK Cells Activated through Antibody-Dependent Cell Cytotoxicity and Armed with Degranulation/IFN-γ Production Suppress Antibody-dependent Enhancement of Dengue Viral Infection. Sci. Rep. 2019, 9, 1109. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Wiehe, K.; Pollara, J. Antibody-Dependent Cellular Phagocytosis in Antiviral Immune Responses. Front. Immunol. 2019, 10, 332. [Google Scholar] [CrossRef]
- Berger, S.; Balló, H.; Stutte, H.J. Immune complex-induced interleukin-6, interleukin-10 and prostaglandin secretion by human monocytes: A network of pro- and anti-inflammatory cytokines dependent on the antigen:antibody ratio. Eur. J. Immunol. 1996, 26, 1297–1301. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Schulert, G.S.; Volpi, S.; Lee, P.Y.; Kernan, K.F.; Caricchio, R.; Mahmud, S.; Hazen, M.M.; Halyabar, O.; et al. On the Alert for Cytokine Storm: Immunopathology in COVID-19. Arthritis Rheumatol. 2020, 72, 1059–1063. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Naturally Infected Unvaccinated Number (%) | Pfizer-Vaccinated Number (%) | Sinopharm-Vaccinated Number (%) | |
|---|---|---|---|---|
| Number of participants | 99 | 100 | 100 | |
| Age (Years) | 21–40 | 53 (53.5) | 13 (13.3) | 9 (9) |
| 41–60 | 35 (35.3) | 31 (31.6) | 31(31) | |
| 61–80 | 8 (8.1) | 54 (55.1) | 55 (55) | |
| NA | 3 | 2 | 5 | |
| Gender | Male | 57 (57.5) | 69 (69) | 68 (68) |
| Female | 42 (42.4) | 31 (31) | 32 (32) | |
| Chronic disease | Yes | NA | 57 (58.1) | 60 (60) |
| No | NA | 41 (41.8) | 35 (35) | |
| NA | NA | 2 | 5 | |
| Smoking | Yes No | NA | 63 (64.2) | 30 (30) |
| NA | 31 (31.6) | 60 (60) | ||
| NA | 2 | 10 | ||
| Previous confirmed infection with COVID-19 | Yes | N-AP | 1 (1.0) | 4 (4) |
| No | N-AP | 97 (98.9) | 91 (91) | |
| NA | N-AP | 2 | 5 |
| Naturally Infected Unvaccinated | Pfizer-Vaccinated | Sinopharm-Vaccinated | |
|---|---|---|---|
| Anti-S IgG titer U/mL | |||
| % Positive | 64.6% | 88% | 58% |
| All participants‘ median (IQR) | 36.35 (164.51) | 26.52 (24.25) | 14.35 (46.02) |
| Median number out of 100 | 31 | 45 | 39 |
| Range | 0.04–532.5 | 0.39–1265 | 0.39–870.17 |
| Only positive cases median (IQR) | 124.54 (183.30) | 28.62 (29.74) | 39.25 (119.95) |
| Anti-N IgG titer U/mL | |||
| % Positive | 60.6% | 25% | 48% |
| All participants‘ median (IQR) | 15.03 (32.21) | 0.02 (2.31) | 0.8 (10.41) |
| Median number out of 100 | 66 | 47 | 50 |
| Range | 0–265.1 | 0–68 | 0–146.3 |
| Only positive cases median (IQR) | 22.08 (32.64) | 13.72 (12.59) | 11.21 (14.6) |
| Anti-N IgM titer U/mL | |||
| % Positive | 23.2% | 9.0% | 7.0% |
| All participants‘ median (IQR) | 0.29 (0.86) | 0.18 (0.3) | 0.2 (0.23) |
| Median number out of 100 | 49 | 43 | 40 |
| Range | 0–15 | 0–33 | 0–12.02 |
| Only positive cases median (IQR) | 2.1 (3.08) | 1.93 (3.16) | 1.4 (9.22) |
| Medians of Anti-S and Anti-N IgG Titers for Anti IgM +ve Samples | |||
|---|---|---|---|
| Naturally Infected Unvaccinated (23 Samples) | Pfizer-Vaccinated (9 Samples) | Sinopharm-Vaccinated (7 Samples) | |
| Anti-S IgG | 189.06 | 21 | 189.19 |
| Anti-N IgG | 35.75 | 0.14 | 21.47 |
| Age (Years) | Gender | Chronic Disease | Smoking Status | Previous COVID-19 Infection | ||
|---|---|---|---|---|---|---|
| Anti-N IgG for Pfizer-vaccinated group | Correlation Coefficient | 0.022 | 0.016 | 0.050 | 0.165 | 0.108 |
| Sig. (2-tailed) | 0.832 | 0.879 | 0.631 | 0.113 | 0.301 | |
| Anti-S IgG for Pfizer-vaccinated group | Correlation Coefficient | −0.214 * | 0.078 | −0.156 | −0.163 | 0.131 |
| Sig. (2-tailed) | 0.035 | 0.444 | 0.127 | 0.110 | 0.200 | |
| Anti-N IgG for Sinopharm-vaccinated group | Correlation Coefficient | −0.152 | −0.015 | −0.167 | 0.085 | 0.101 |
| Sig. (2-tailed) | 0.142 | 0.883 | 0.109 | 0.418 | 0.333 | |
| Anti-S IgG for Sinopharm-vaccinated group | Correlation Coefficient | −0.270 ** | 0.111 | −0.272 ** | −0.098 | 0.185 |
| Sig. (2-tailed) | 0.008 | 0.0 | 0.008 | 0.348 | 0.072 | |
| Anti-N IgG for naturally infected unvaccinated subjects | Correlation Coefficient | 0.174 | 0.035 | NA | NA | NA |
| Sig. (2-tailed) | 0.096 | 0.735 | NA | NA | NA | |
| Anti-S IgG for naturally infected unvaccinated subjects | Correlation Coefficient | 0.216 * | 0.087 | NA | NA | NA |
| Sig. (2-tailed) | 0.040 | 0.407 | NA | NA | NA |
| Symptoms | Department *** | Duration | Severity | ||
|---|---|---|---|---|---|
| Anti-N | Correlation Coefficient | 0.050 | 0.246 * | 0.292 ** | −0.035 |
| Sig. (2-tailed) | 0.641 | 0.019 | 0.006 | 0.739 | |
| Anti-S | Correlation Coefficient | −0.043 | 0.296 ** | 0.301 ** | −0.090 |
| Sig. (2-tailed) | 0.683 | 0.004 | 0.004 | 0.391 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qaqish, A.; Abbas, M.M.; Al-Tamimi, M.; Abbas, M.A.; Al-Omari, M.; Alqassieh, R. SARS-CoV-2 Antinucleocapsid Antibody Response of mRNA and Inactivated Virus Vaccines Compared to Unvaccinated Individuals. Vaccines 2022, 10, 643. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050643
Qaqish A, Abbas MM, Al-Tamimi M, Abbas MA, Al-Omari M, Alqassieh R. SARS-CoV-2 Antinucleocapsid Antibody Response of mRNA and Inactivated Virus Vaccines Compared to Unvaccinated Individuals. Vaccines. 2022; 10(5):643. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050643
Chicago/Turabian StyleQaqish, Arwa, Manal Mohammad Abbas, Mohammad Al-Tamimi, Manal Ahmad Abbas, Mariam Al-Omari, and Rami Alqassieh. 2022. "SARS-CoV-2 Antinucleocapsid Antibody Response of mRNA and Inactivated Virus Vaccines Compared to Unvaccinated Individuals" Vaccines 10, no. 5: 643. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050643