
Clinical and Virological Features of Patients Hospitalized with Different Types of COVID-19 Vaccination in Mexico City

 , , , , ,
, , , , ,  , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Participants and Clinical Data
2.2. SARS-CoV-2 Diagnostics
2.3. RNA Extraction and Sequencing
2.3.1. Complete Genome Sequencing
2.3.2. Spike Partial Sequencing
2.4. Phylogenetic Analysis
2.5. Statistical Analyses
3. Results
3.1. Clinical and Demographic Characteristics of the Cohort
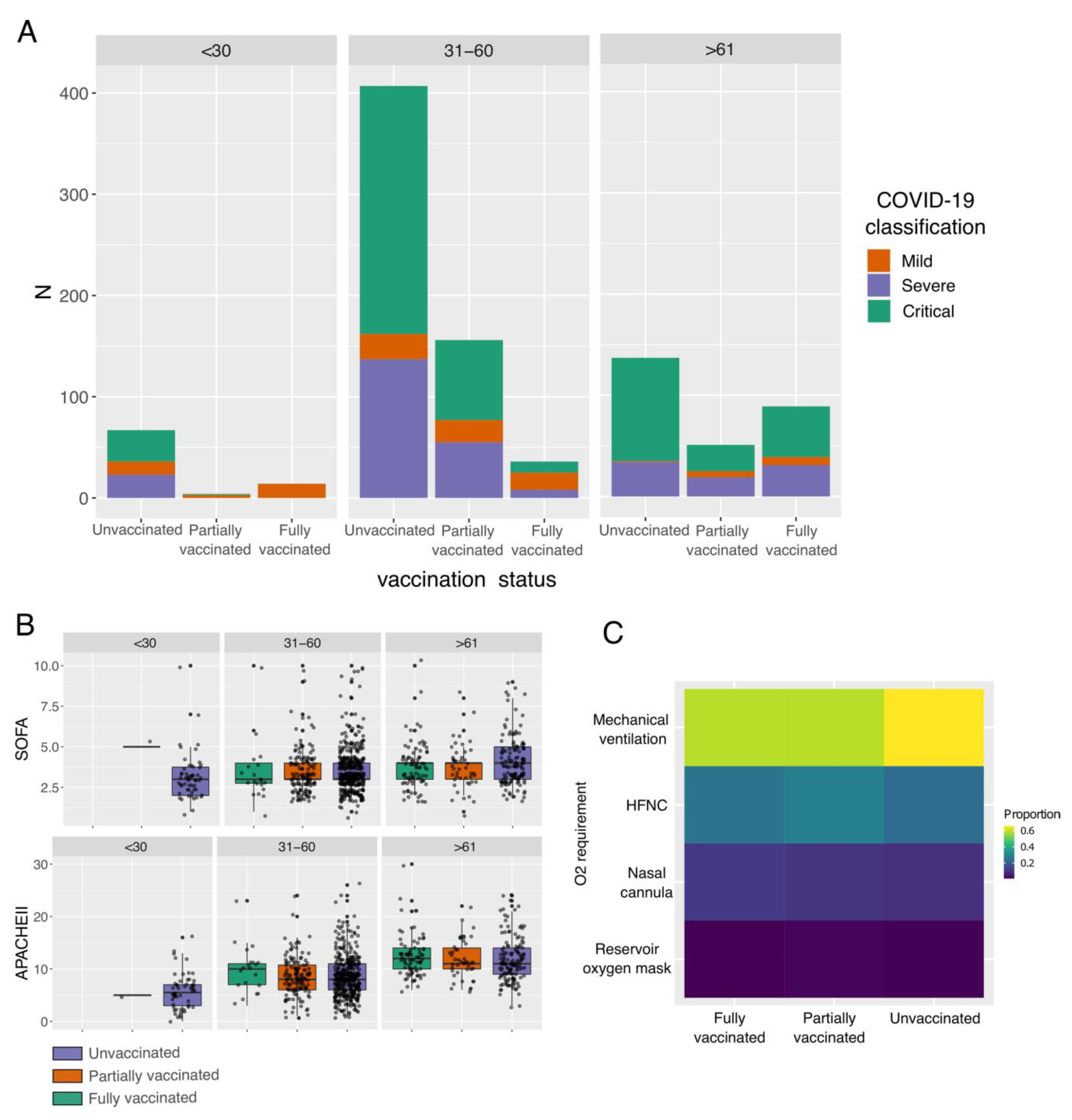
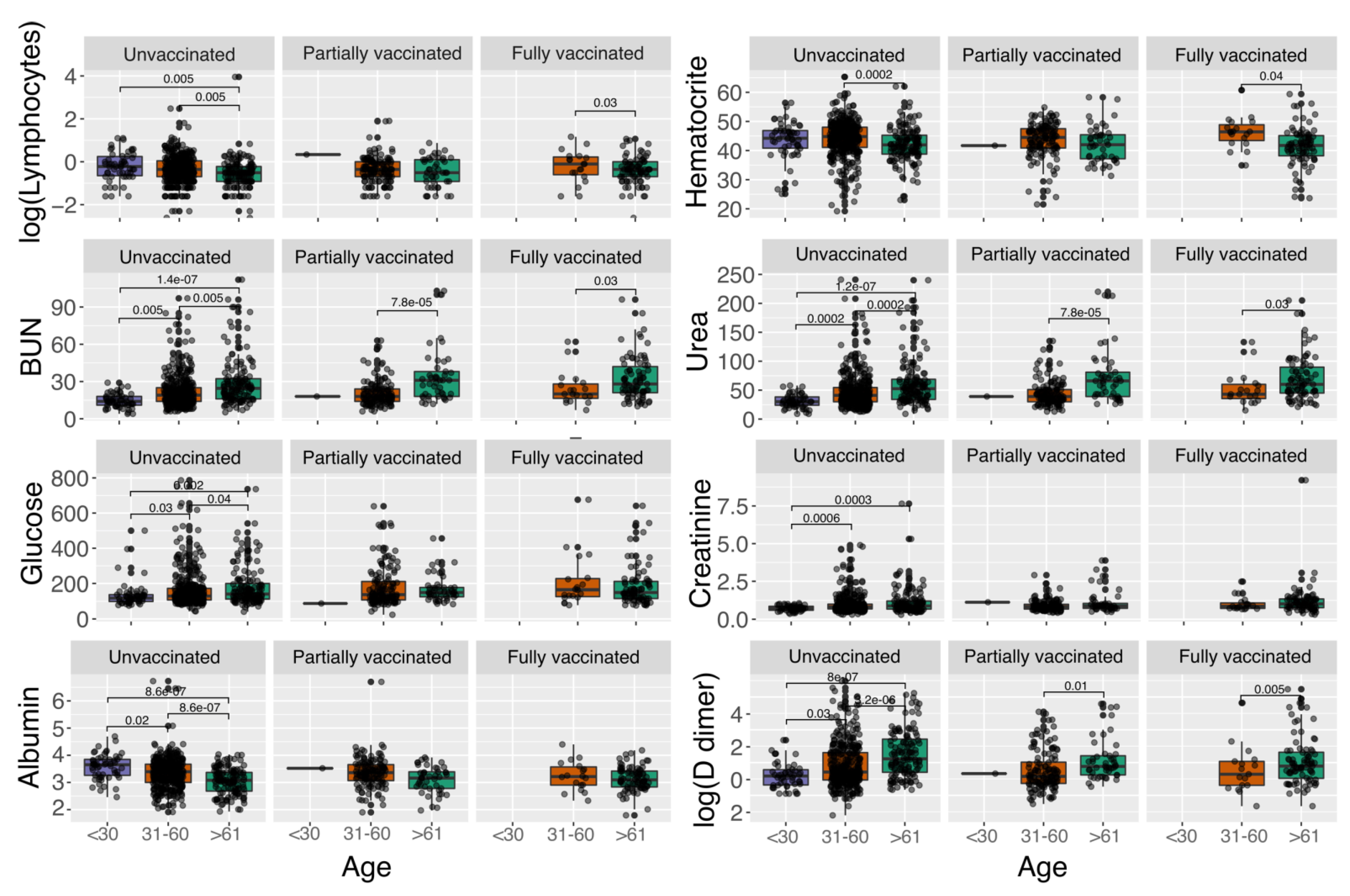
3.2. Impact of Vaccination Status and Age on the Severity and Clinical Parameters of COVID-19 Patients
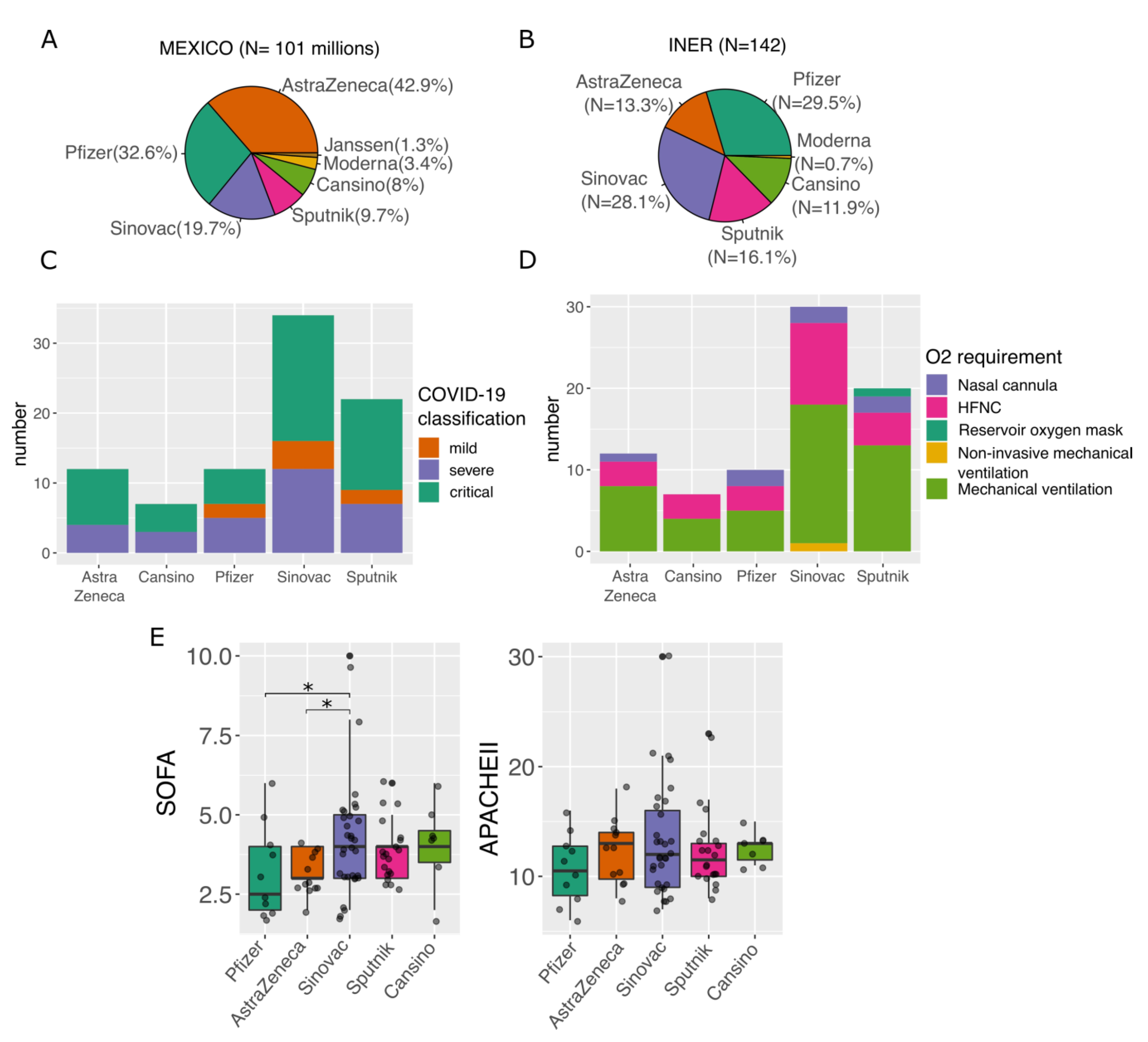
3.3. Impact of Different Vaccines on Severity of Disease
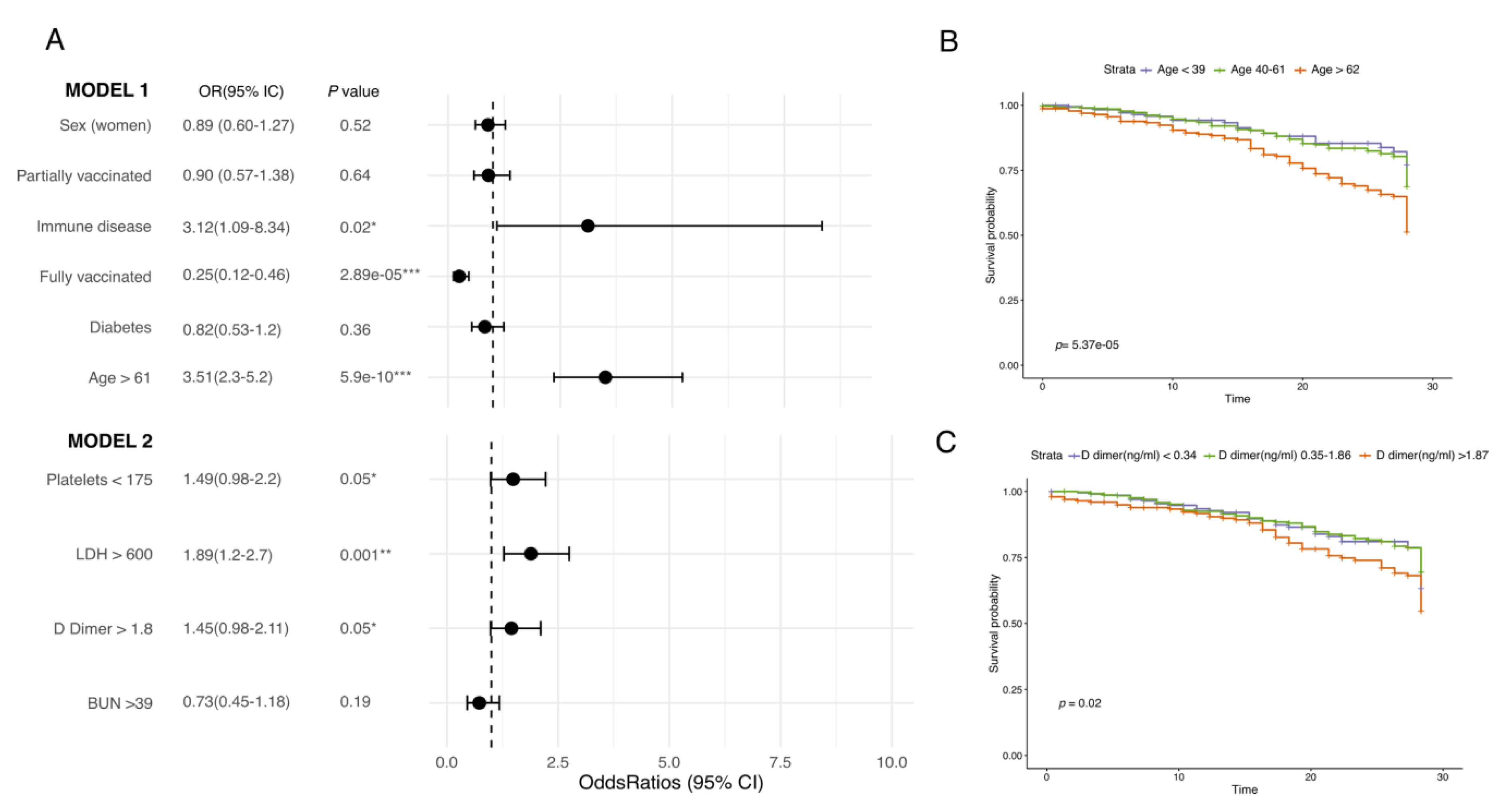
3.4. Clinical Factors Affecting COVID-19 Clinical Outcome
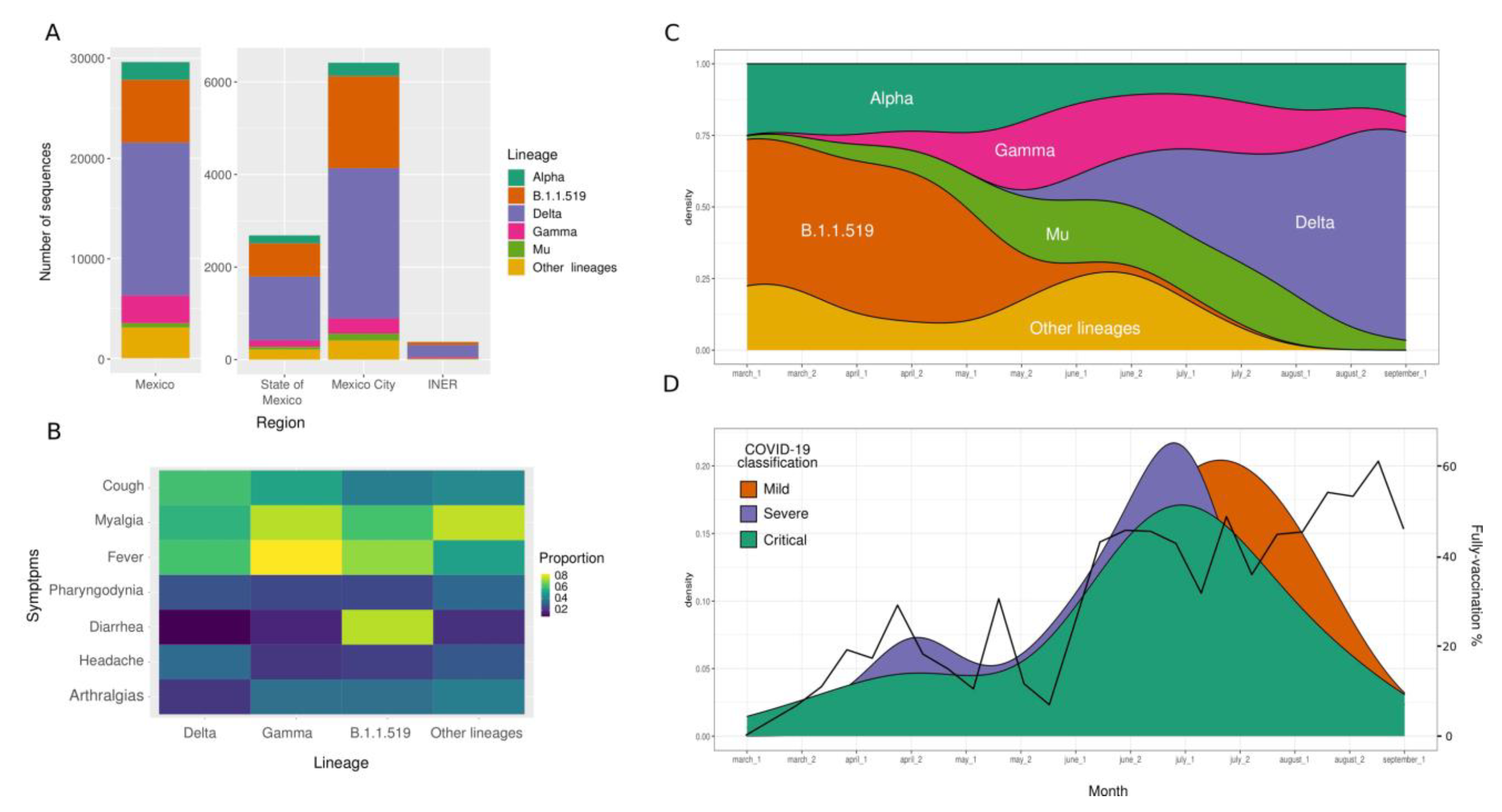
3.5. SARS-CoV-2 Lineages
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 15 April 2022).
- Isabel, S.; Graña-Miraglia, L.; Gutierrez, J.M.; Bundalovic-Torma, C.; Groves, H.E.; Isabel, M.R.; Eshaghi, A.R.; Patel, S.N.; Gubbay, J.B.; Poutanen, T.; et al. Evolutionary and structural analyses of SARS-CoV-2 D614G spike protein mutation now documented worldwide. Sci. Rep. 2020, 10, 14031. [Google Scholar] [CrossRef] [PubMed]
- Giovanetti, M.; Benedetti, F.; Campisi, G.; Ciccozzi, A.; Fabris, S.; Ceccarelli, G.; Tambone, V.; Caruso, A.; Angeletti, S.; Zella, D.; et al. Evolution patterns of SARS-CoV-2: Snapshot on its genome variants. Biochem. Biophys. Res. Commun. 2021, 538, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Peacock, S.J.; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.W.; Chiew, C.J.; Ang, L.W.; Mak, T.-M.; Cui, L.; HS Toh, M.P.; Lim, Y.D.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and virological features of SARS-CoV-2 variants of concern: A retrospective cohort study comparing B.1.1.7 (Alpha), B.1.315 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2021, 23, ciab721. [Google Scholar] [CrossRef]
- Taboada, B.; Zárate, S.; Iša, P.; Boukadida, C.; Vazquez-perez, J.A.; Muñoz-medina, J.E.; Ramírez-gonzález, J.E.; Comas-garcía, A.; Grajales-muñiz, C.; Rincón-rubio, A.; et al. Genetic analysis of SARS-CoV-2 variants in mexico during the first year of the COVID-19 pandemic. Viruses 2021, 13, 2161. [Google Scholar] [CrossRef]
- Cedro-tanda, A.; Laura, G.; De Anda-jauregui, G.; Garnica-l, D.; Alfaro-mora, Y.; Sonia, S.; Garc, E.F.; Mendoza-vargas, A.; Fr, E.J.; Moreno, B.; et al. Early genomic, epidemilogical, and clinical description of the SARS-CoV-2 omicron variant in Mexico City. Viruses 2022, 14, 545. [Google Scholar] [CrossRef]
- Rodríguez-Maldonado, A.P.; Vázquez-Pérez, J.A.; Cedro-Tanda, A.; Taboada, B.; Boukadida, C.; Wong-Arámbula, C.; Nuñez-García, T.E.; Cruz-Ortiz, N.; Barrera-Badillo, G.; Hernández-Rivas, L.; et al. Emergence and spread of the potential variant of interest (VOI) B.1.1.519 of SARS-CoV-2 predominantly present in Mexico. Arch. Virol. 2021, 166, 3173–3177. [Google Scholar] [CrossRef]
- Cedro-tanda, A.; Laura, G.; De Anda-jauregui, G.; Peñaloza, F.; Moreno, B.; Escobar-arrazola, M.A.; Ramirez-vega, O.A.; Munguia-garza, P.; Garcia-cardenas, F.; Cisneros-villanueva, M.; et al. The evolutionary landscape of SARS-CoV-2 variant B.1.1.519 and its clinical impact in Mexico City. Viruses 2021, 13, 2182. [Google Scholar] [CrossRef]
- de Salud, S. COVID-19 MÉXICO: Comunicado Técnico Diario; Secretaría de Salud, Subsecretaría de Prevención y Promoción de la Salud: Mexico City, Mexico, 2021. [Google Scholar]
- Butt, A.A.; Nafady-hego, H.; Chemaitelly, H.; Abou-Samra, A.-B.; Al Khal, A.; Coyle, P.V.; Al Kanaani, Z.; Kaleeckal, A.H.; Latif, A.N.; Al Masalmani, Y.; et al. Outcomes Among Patients with Breakthrough SARS-CoV-2 Infection After Vaccination. Int. J. Infect. Dis. 2020, 110, 353–358. [Google Scholar] [CrossRef]
- Fagni, F.; Simon, D.; Tascilar, K.; Schoenau, V.; Sticherling, M.; Neurath, M.F.; Schett, G. COVID-19 and immune-mediated inflammatory diseases: Effect of disease and treatment on COVID-19 outcomes and vaccine responses. Lancet Rheumatol. 2021, 3, e724–e736. [Google Scholar] [CrossRef]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Z.; Tang, Y.; Li, C.; Sun, C.; Zhu, Y.; Li, Z.; Chang, T. COVID-19 vaccination in patients with myasthenia gravis: A single-center case series. Vaccines 2021, 9, 1112. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Z.; Kuan, C.C. Vaccination to reduce severe COVID-19 and mortality in COVID-19 patients: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1770–1776. [Google Scholar] [CrossRef]
- Prévost, J.; Finzi, A. The great escape? SARS-CoV-2 variants evading neutralizing responses. Cell Host Microbe 2021, 29, 322–324. [Google Scholar] [CrossRef]
- Thakur, S.; Sasi, S.; Pillai, S.G.; Nag, A.; Shukla, D.; Singhal, R.; Phalke, S.; Velu, G.S.K. SARS-CoV-2 Mutations and Their Impact on Diagnostics, Therapeutics and Vaccines. Front. Med. 2022, 9, 815389. [Google Scholar] [CrossRef]
- Bakhshandeh, B.; Jahanafrooz, Z.; Abbasi, A.; Babaee, M.; Sadeghi, M.; Sadeq, M.M.; Zamani, M. Mutations in SARS-CoV-2; consequences in structure, function, and pathogenicity of the virus. Microb. Pathog. 2020, 154, 104831. [Google Scholar] [CrossRef]
- Castillo, A.E.; Parra, B.; Tapia, P.; Acevedo, A.; Lagos, J.; Andrade, W.; Arata, L.; Leal, G.; Barra, G.; Tambley, C.; et al. Phylogenetic analysis of the first four SARS-CoV-2 cases in Chile. J. Med. Virol. 2020, 92, 1562–1566. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Stecher, G.; Li, M.; Knyaz, C.; Tamura, K. MEGA X: Molecular evolutionary genetics analysis across computing platforms. Mol. Biol. Evol. 2018, 35, 1547–1549. [Google Scholar] [CrossRef]
- Katoh, K.; Misawa, K.; Kuma, K.I.; Miyata, T. MAFFT: A novel method for rapid multiple sequence alignment based on fast Fourier transform. Nucleic Acids Res. 2002, 30, 3059–3066. [Google Scholar] [CrossRef] [Green Version]
- Rambaut, A. FigTree v1. 3.1. 2009. Available online: http://tree.bio.ed.ac.uk/software/figtree/ (accessed on 15 April 2022).
- Wang, J.; Tong, Y.; Li, D.; Li, J.; Li, Y. The Impact of Age Difference on the Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 758294. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Treatment Guidelines. Coronavirus Disease 2019 (COVID-19). 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 15 April 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Wickham, H.; Chang, W.; Pedersen Lin, T.; Takahashi, K.; Wilke, C.; Woo, K. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Therneu, P.M. A Package for Survival Analysis in R 2022. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwj70cXhsOP4AhUw4TgGHaBpAfcQFnoECAUQAQ&url=https%3A%2F%2Fcran.r-project.org%2Fweb%2Fpackages%2Fsurvival%2Fvignettes%2Fsurvival.pdf&usg=AOvVaw2fxLnFDufEG0EyK1Dm0eRe (accessed on 1 July 2020).
- Kassambara, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using ggplot2. 2021. Available online: http://rpkgs.datanovia.com/survminer/reference/ggsurvplot.html (accessed on 1 July 2020).
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Cockburn, J.; Mcdonald, H.I.; et al. OpenSAFELY: Factors associated with COVID-19 death in 17 million patients. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Martos-Benítez, F.D.; Soler-Morejón, C.D.; García-del Barco, D. Chronic comorbidities and clinical outcomes in patients with and without COVID-19: A large population-based study using national administrative healthcare open data of Mexico. Intern. Emerg. Med. 2021, 16, 1507–1517. [Google Scholar] [CrossRef]
- Collier, D.A.; Ferreira, I.A.T.M.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; Baker, S.; Dougan, G.; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-González, E.; Cantero-Escribano, J.M.; Redondo-Bravo, L.; San Juan-Sanz, I.; Robustillo-Rodela, A.; Cendejas-Bueno, E.; Influenza Working Group. Effect of vaccination, comorbidities and age on mortality and severe disease associated with influenza during the season 2016–2017 in a Spanish tertiary hospital. J. Infect. Public Health 2019, 12, 486–491. [Google Scholar] [CrossRef]
- Gasmi, A.; Peana, M.; Pivina, L.; Srinath, S.; Gasmi Benahmed, A.; Semenova, Y.; Menzel, A.; Dadar, M.; Bjørklund, G. Interrelations between COVID-19 and other disorders. Clin. Immunol. 2021, 224, 108651. [Google Scholar] [CrossRef]
- Honardoost, M.; Janani, L.; Aghili, R.; Emami, Z.; Khamseh, M.E. The Association between Presence of Comorbidities and COVID-19 Severity: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2021, 50, 132–140. [Google Scholar] [CrossRef]
- Tseng, Y.H.; Chen, T.H. Care for Patients With Neuromuscular Disorders in the COVID-19 Pandemic Era. Front. Neurol. 2021, 12, 607790. [Google Scholar] [CrossRef]
- Lupica, A.; Di Stefano, V.; Iacono, S.; Pignolo, A.; Quartana, M.; Gagliardo, A.; Fierro, B.; Brighina, F. Impact of COVID-19 in AChR Myasthenia Gravis and the Safety of Vaccines: Data from an Italian Cohort. Neurol. Int. 2022, 14, 406–416. [Google Scholar] [CrossRef]
- Asano, T.; Boisson, B.; Onodi, F.; Daniela, M.; Moncada-Velez, M.; Renkilaraj, M.R.L.M. X-linked recessive TLR7 deficiency in ~1% of men under 60 years old with life-threatening COVID-19. Sci. Immunol. 2021, 4348, eabl4348. [Google Scholar] [CrossRef]
- Zeberg, H. The major genetic risk factor for severe COVID-19 is associated with protection against HIV. Proc. Natl. Acad. Sci. USA 2022, 119, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Kahn, F.; Bonander, C.; Moghaddassi, M.; Rasmussen, M.; Malmqvist, U.; Inghammar, M.; Björk, J. Risk of severe COVID-19 from the Delta and Omicron variants in relation to vaccination status, sex, age and comorbidities—Surveillance results from southern Sweden. medRxiv 2022, 27. [Google Scholar] [CrossRef]
- Markanday, A. Acute phase reactants in infections: Evidence-based review and a guide for clinician. Open Forum Infect. Dis. 2015, 2, 2200121. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.H.; Bijol, V.; Sparks, M.A.; Sise, M.E.; Izzedine, H.; Jhaveri, K.D. Pathophysiology and Pathology of Acute Kidney Injury in Patients With COVID-19. Adv. Chronic Kidney Dis. 2020, 27, 365–376. [Google Scholar] [CrossRef]
- Wu, M.A.; Fossali, T.; Pandolfi, L.; Carsana, L.; Ottolina, D.; Frangipane, V.; Rech, R.; Tosoni, A.; Lopez, G.; Agarossi, A.; et al. Hypoalbuminemia in COVID-19: Assessing the hypothesis for underlying pulmonary capillary leakage. J. Intern. Med. 2021, 289, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Choi, W.S.; Cheong, H.J. COVID-19 vaccination for people with comorbidities. Infect. Chemother. 2021, 53, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, L. Implication of SARS-CoV-2 Immune Escape Spike Variants on Secondary and Vaccine Breakthrough Infections. Front. Immunol. 2021, 12, 4563. [Google Scholar] [CrossRef]
- Lou, F.; Li, M.; Pang, Z.; Jiang, L.; Guan, L.; Tian, L.; Hu, J.; Fan, J.; Fan, H. Understanding the Secret of SARS-CoV-2 Variants of Concern/Interest and Immune Escape. Front. Immunol. 2021, 12, 4326. [Google Scholar] [CrossRef]
- Moghaddar, M.; Radman, R.; Macreadie, I. Severity, pathogenicity and transmissibility of delta and lambda variants of SARS-CoV-2, toxicity of spike protein and possibilities for future prevention of COVID-19. Microorganisms 2021, 9, 2167. [Google Scholar] [CrossRef]
- Hu, Z.; Huang, X.; Zhang, J.; Fu, S.; Ding, D.; Tao, Z. Differences in Clinical Characteristics Between Delta Variant and Wild-Type SARS-CoV-2 Infected Patients. Front. Med. 2022, 8, 792135. [Google Scholar] [CrossRef] [PubMed]
- Paredes, M.I.; Lunn, S.M.; Famulare, M.; Frisbie, L.A.; Painter, I.; Burstein, R.; Roychoudhury, P.; Xie, H.; Bakash, S.A.M.; Perez, R.; et al. Associations between SARS-CoV-2 variants and risk of COVID-19 hospitalization among confirmed cases in Washington State: A retrospective cohort study. Clin. Infect. Dis. 2000, 12, 1–18. [Google Scholar]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; Mcneal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, COVID-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef] [PubMed]
- Everett, J.; Hokama, P.; Roche, A.M.; Reddy, S.; Hwang, Y.; Kessler, L.; Glascock, A.; Li, Y.; Whelan, J.N.; Weiss, S.R.; et al. SARS-CoV-2 genomic variation in space and time in hospitalized patients in Philadelphia. MBio 2021, 12, e03456-20. [Google Scholar] [CrossRef]
- Boukadida, C.; Taboada, B.; Escalera-Zamudio, M.; Isa, P.; Ramírez-González, J.E.; Vazquez-Perez, J.A.; Muñoz-Medina, J.E.; Grajales-Muñiz, C.; González-Torres, C.; Gaytán-Cervantes, F.J.; et al. Genomic Characterization of SARS-CoV-2 Isolated from Patients with Distinct Disease Outcomes in Mexico. Microbiol. Spectr. 2022, 10, e01249-21. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef]
- Stupica, D.; Collinet-Adler, S.; Kejžar, N.; Jagodic, Z.; Poljak, M.; Klevišar, M.N. The Impact of SARS-CoV-2 Primary Vaccination in a Cohort of Patients Hospitalized for Acute COVID-19 during Delta Variant Predominance. J. Clin. Med. 2022, 11, 1191. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccination Status | Outpatients (n = 111) | Hospitalized (n = 855) | ||||||
|---|---|---|---|---|---|---|---|---|
| Unvaccinated (n = 39) [35.1%] | Partially Vaccinated (n = 32) [28.8%] | Fully Vaccinated (n = 40) [36%] | p | Unvaccinated (n = 572) [66.9%] | Partially Vaccinated (n = 178) [20.8%] | Fully Vaccinated (n = 105) [12.2%] | p | |
| Age | ||||||||
| <30, n (%) | 13 (33.3%) | 4 (12.5%) | 14 (35%) | 0.03 | 54 (9.4%) | 1 (0.5%) | 0 | <0.001 |
| 31–60, n (%) | 25 (64.1%) | 22 (68.7%) | 18 (45%) | 0.04 | 382 (66.7%) | 132 (74.1%) | 21 (20%) | <0.001 |
| =/> 60, n (%) | 1 (2.50%) | 6 (18.7%) | 8 (20%) | 0.03 | 135 (23.6%) | 45 (25.2%) | 82 (78%) | <0.001 |
| NA | 0 | 0 | 0 | 1 | 0 | 2 | ||
| Gender | ||||||||
| Female, n (%) | 17 (43.5%) | 20 (62.5%) | 16 (40%) | ns | 200 (34.9%) | 65 (36.5%) | 52 (49.5%) | 0.02 |
| NA | 0 | 0 | 0 | 0 | 0 | 0 | ||
| Vaccine type | ||||||||
| Total of vaccinated patients | 32 (100%) | 40 (100%) | 179 (100%) | 104 (100%) | ||||
| Pfizer, n (%) | na | 12 (37%) | 28 (70%) | 0.01 | na | 34 (19%) | 14 (13.3%) | ns |
| AztraZeneca, n (%) | na | 13(40.6%) | 4 (10%) | 0.02 | na | 69 (38.7%) | 15 (14.2%) | <0.001 |
| SinoVac, n (%) | na | 3 (9.3%) | 5 (12%) | ns | na | 18 (10.1%) | 35 (33.3%) | <0.001 |
| Sputnik, n (%) | na | 2 (6.2%) | 2 (5%) | ns | na | 51 (28.6%) | 21 (20%) | ns |
| Cansino, n (%) | na | 0 | 1 (2.5%) | na | na | na | 18 (17.1%) | na |
| J&J, n (%) | na | 0 | 0 | na | na | 1 (0.56%) | 0 | ns |
| Moderna, n (%) | na | 0 | 0 | na | na | 0 | 1 (0.95%) | ns |
| NA | na | 2 | 0 | na | 5 | 1 | ||
| Comorbidities | ||||||||
| Diabetes, n (%) | 2 (5.1%) | 4 (12.5%) | 1 (2.5%) | ns | 115 (20.1%) | 44 (24.7%) | 42 (40%) | <0.001 |
| Hypertension, n (%) | 5 (12.8%) | 4 (12.5%) | 5 (12.5%) | ns | 147 (25.6%) | 45 (25.2%) | 53 (53.3%) | <0.001 |
| Obesity, n (%) | 5 (12.8%) | 7 (21.8%) | 4 (10%) | ns | 255 (44.5%) | 82 (46%) | 47 (44.7%) | ns |
| Smoking, n (%) | 2 (5.1%) | 1 (3.1%) | 2 (5%) | ns | 177 (30.9%) | 57 (32%) | 25 (23.8%) | ns |
| COPD, n (%) | 0 | 0 | 2 (5%) | na | 12 (2%) | 2 (1.1%) | 4 (3.8%) | ns |
| Immune disease, n (%) | 0 | 0 | 2 (5%) | na | 12 (2%) | 1 (0.5%) | 3 (2.8%) | ns |
| NA | 89 | 85 | 105 | 33 | 13 | 10 | ||
| Number of comorbidities | ||||||||
| None, n (%) | 22 (56.4%) | 13 (40.6%) | 25 (62.1%) | 0.05 | 97 (16.9%) | 34 (19.1%) | 10 (9.5%) | 0.05 |
| 1, n (%) | 9 (23.07%) | 2 (6.2%) | 4 (10%) | ns | 217 (37.9%) | 58 (32.5%) | 21 (20%) | <0.001 |
| 2, n (%) | 2 (5.1%) | 1 (3.1%) | 4 (10%) | ns | 170 (29.7%) | 55 (30.8%) | 35 (33.3%) | ns |
| =/> 3, n (%) | 1 (2.5%) | 3 (9.3%) | 2 (5%) | ns | 87 (15.2%) | 31 (17.4%) | 39 (37.1%) | <0.001 |
| NA | 5 | 13 | 5 | 1 | 0 | 0 | ||
| In-hospital treatment | ||||||||
| Dexamethasone, n (%) | 5 (12.8%) | 2 (6.2%) | 1 (2.5%) | ns | 554 (96.8%) | 169 (94.9%) | 98 (93.3%) | ns |
| Remdesivir/Baricitinib, n (%) | 0 | 0 | 0 | na | 11 (1.9%) | 3 (1.6%) | 3 (2.8%) | 0.02 |
| Remdesivir/Dexamethasone, n (%) | 0 | 0 | 0 | na | 4 (0.6%) | 0 | 1 (0.95%) | ns |
| Dexamethasone/Baricitinib, n (%) | 0 | 0 | 0 | na | 1 (0.1%) | 2 (1.1%) | 0 | ns |
| NA | 5 | 13 | 6 | 0 | 0 | 2 | ||
| Previous steroid | ||||||||
| Dexamethasone, n (%) | 0 | 0 | 0 | na | 202 (35.3%) | 66 (37%) | 40 (38%) | ns |
| Prednisone, n (%) | 0 | 0 | 0 | na | 28 (4.8%) | 0 | 5 (4.7%) | 0.001 |
| Betamethasone, n (%) | 0 | 0 | 0 | na | 12 (2%) | 7 (3.9%) | 2 (1.9%) | ns |
| Dexamethasone/Prednisone, n (%) | 0 | 0 | 0 | na | 6 (1.04%) | 2 (1.1%) | 0 | ns |
| Dexamethasone/Betamethasone, n (%) | 0 | 0 | 0 | na | 5 (0.87%) | 4 (2.2%) | 0 | ns |
| NA | 5 | 13 | 6 | 0 | 0 | 2 | ||
| Symptoms | ||||||||
| Fever, n (%) | 19 (48.7%) | 10 (31.2%) | 12 (30%) | 0.01 | 409 (71.5%) | 134 (75.2%) | 57 (54.2%) | <0.001 |
| Cough, n (%) | 19 (48.7%) | 19 (59.3%) | 15 (37.5%) | ns | 333 (58.2%) | 107 (60.1%) | 68 (64.7%) | ns |
| Diarrhea, n (%) | 4 (10.2%) | 1 (3.1%) | 4 (10%) | 0.01 | 61 (10.6%) | 17 (9.5%) | 6 (5.7%) | ns |
| Myalgias, n (%) | 9 (23%) | 7 (21.8%) | 11 (27.5%) | ns | 382 (66.7%) | 111 (62.3%) | 65 (61.9%) | ns |
| Arthralgias, n (%) | 10 (25.6%) | 10 (31.2%) | 8 (20%) | 0.002 | 163 (28.4%) | 47 (26.4%) | 24 (22.8%) | ns |
| Nasal congestion, n (%) | 0 | 0 | 2 (5%) | na | 51 (8.9%) | 21 (11.7%) | 11 (10.4%) | ns |
| Pharyngodynia, n (%) | 7 (17.9%) | 7 (21.8%) | 11 (27.5%) | ns | 140 (24.4%) | 57 (32%) | 29 (27.6%) | 0.05 |
| Anosmia, n (%) | 2 (5.1%) | 3 (9.3%) | 2 (5%) | ns | 43 (7.5%) | 14 (7.8%) | 3 (2.8%) | ns |
| Headache, n (%) | 13 (33.3%) | 7 (21.8%) | 13 (32.5%) | <0.001 | 190 (33.2) | 60 (33.7%) | 33 (31.4%) | ns |
| NA | 5 | 20 | 14 | 0 | 0 | 18 | ||
| Vaccination Status | Hospitalized (n = 855) | |||
|---|---|---|---|---|
| Unvaccinated (n = 572) [66.9%] | Partially Vaccinated (n = 178) [20.8%] | Fully Vaccinated (n = 105) [12.2%] | p Value | |
| Outcome | ||||
| Recovered, n (%) | 433 (71.6%) | 139 (78%) | 88 (83.8%) | 0.05 |
| Deceased, n (%) | 129 (22.5%) | 37 (20.7%) | 16 (15.2%) | ns |
| NA | 10 | 2 | 1 | |
| Severity indexes | ||||
| APACHE II, med(IQR) | 8.5 (6–11) | 9 (6.2–11) | 11 (9–14) | <0.001 |
| SOFA, med(IQR) | 3 (3–4) | 3 (3–4) | 4 (3–4) | ns |
| GLASGOW, med(IQR) | 15 (15–15) | 15 (15–15) | 15 (15–15) | ns |
| O2 requirement | ||||
| Nasal cannula, n (%) | 54 (9.4%) | 19 (10.6%) | 12 (11.4%) | ns |
| HFNC, n (%) | 135 (23.6%) | 50 (28%) | 28 (26.6%) | ns |
| Mechanical ventilation, n (%) | 375 (65.5%) | 105 (58.9%) | 61 (58%) | ns |
| Reservoir oxygen mask, n (%) | 7 (1.2%) | 3 (1.6%) | 1 (0.9%) | ns |
| Non-invasive mechanical ventilation, n (%) | 1 (0.1%) | 1 (0.5%) | 1 (0.9%) | ns |
| NA | 0 | 0 | 2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Terán, A.; Garcíadiego-Fossas, P.; Villanueva-Reza, M.; Boukadida, C.; Taboada, B.; Porras, E.; Ahumada-Topete, V.; Tapia-Diaz, K.E.; Matías-Florentino, M.; Pérez-García, M.; et al. Clinical and Virological Features of Patients Hospitalized with Different Types of COVID-19 Vaccination in Mexico City. Vaccines 2022, 10, 1181. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10081181
Hernández-Terán A, Garcíadiego-Fossas P, Villanueva-Reza M, Boukadida C, Taboada B, Porras E, Ahumada-Topete V, Tapia-Diaz KE, Matías-Florentino M, Pérez-García M, et al. Clinical and Virological Features of Patients Hospitalized with Different Types of COVID-19 Vaccination in Mexico City. Vaccines. 2022; 10(8):1181. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10081181
Chicago/Turabian StyleHernández-Terán, Alejandra, Pamela Garcíadiego-Fossas, Marco Villanueva-Reza, Celia Boukadida, Blanca Taboada, Eduardo Porras, Victor Ahumada-Topete, Kathia Elizabeth Tapia-Diaz, Margarita Matías-Florentino, Marissa Pérez-García, and et al. 2022. "Clinical and Virological Features of Patients Hospitalized with Different Types of COVID-19 Vaccination in Mexico City" Vaccines 10, no. 8: 1181. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10081181