
Estimating the Cost-Effectiveness of Switching to Higher-Valency Pediatric Pneumococcal Conjugate Vaccines in the United Kingdom
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
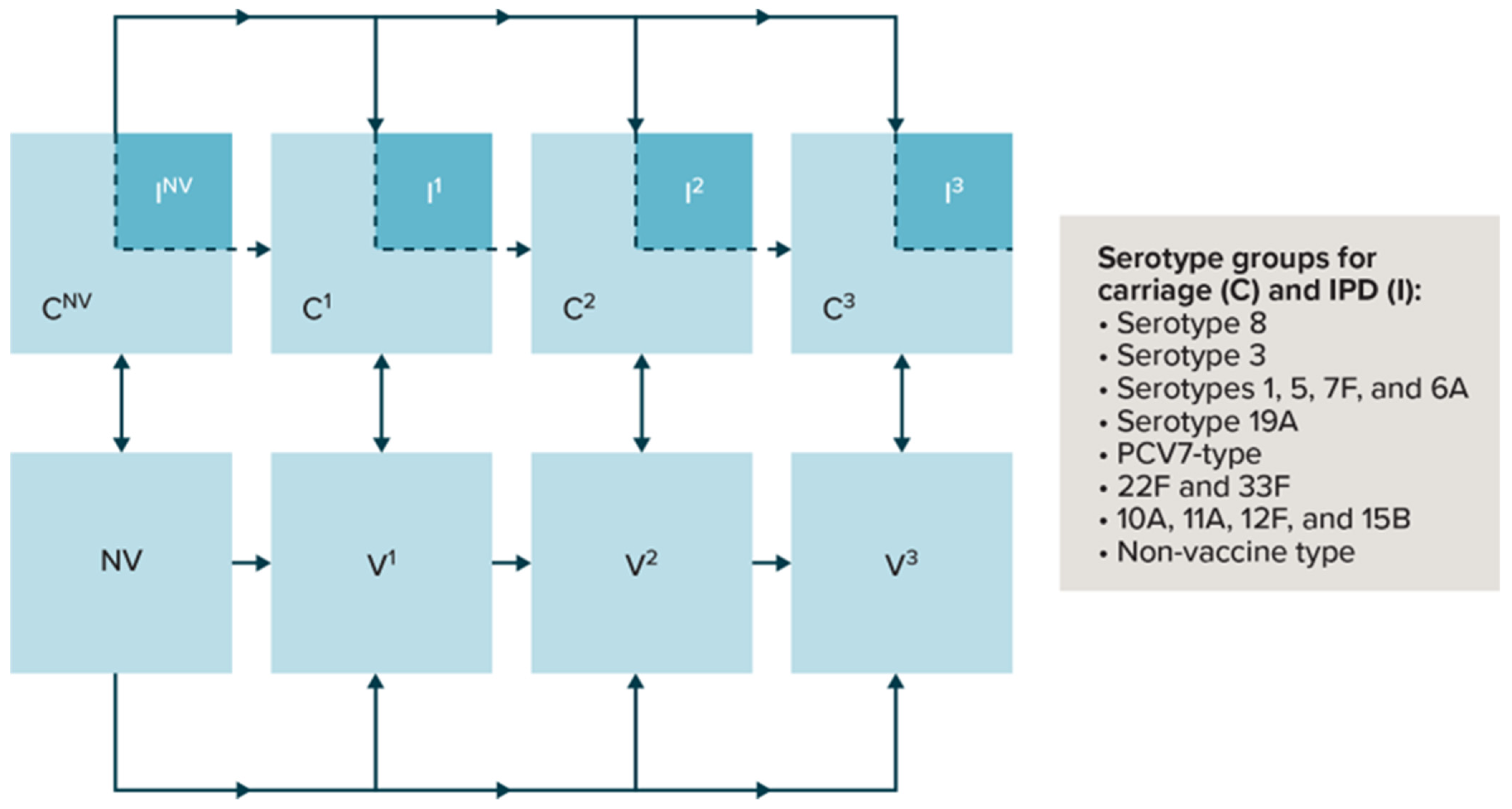
2.1. Model Structure
2.2. Model Inputs
- Table 2 displays vaccine effectiveness against overall IPD and against carriage. In the model, , where vaccine effectiveness against IPD overall, the vaccine effectiveness against IPD given carriage, and the vaccine effectiveness against carriage. We assumed the vaccine effectiveness for PCV20 minus PCV13 serotypes were equivalent to the vaccine effectiveness inputs for serotypes 1, 5, 7F, and 6A. Moreover, when vaccines had in common a particular serotype group for coverage, the protective effect was equivalent across vaccines. We calibrated these vaccine effectiveness estimates and visually inspected them so that they were within the bounds of the published literature [35].
- The probability of acquiring serotype carriage given contact with a carrier, by age and serotype group, absent vaccination.
- The mean duration of protection for each dose (Table 2).
- The mean duration of carriage by age and serotype group.
2.3. Model Analyses
3. Results
3.1. Calibration Results
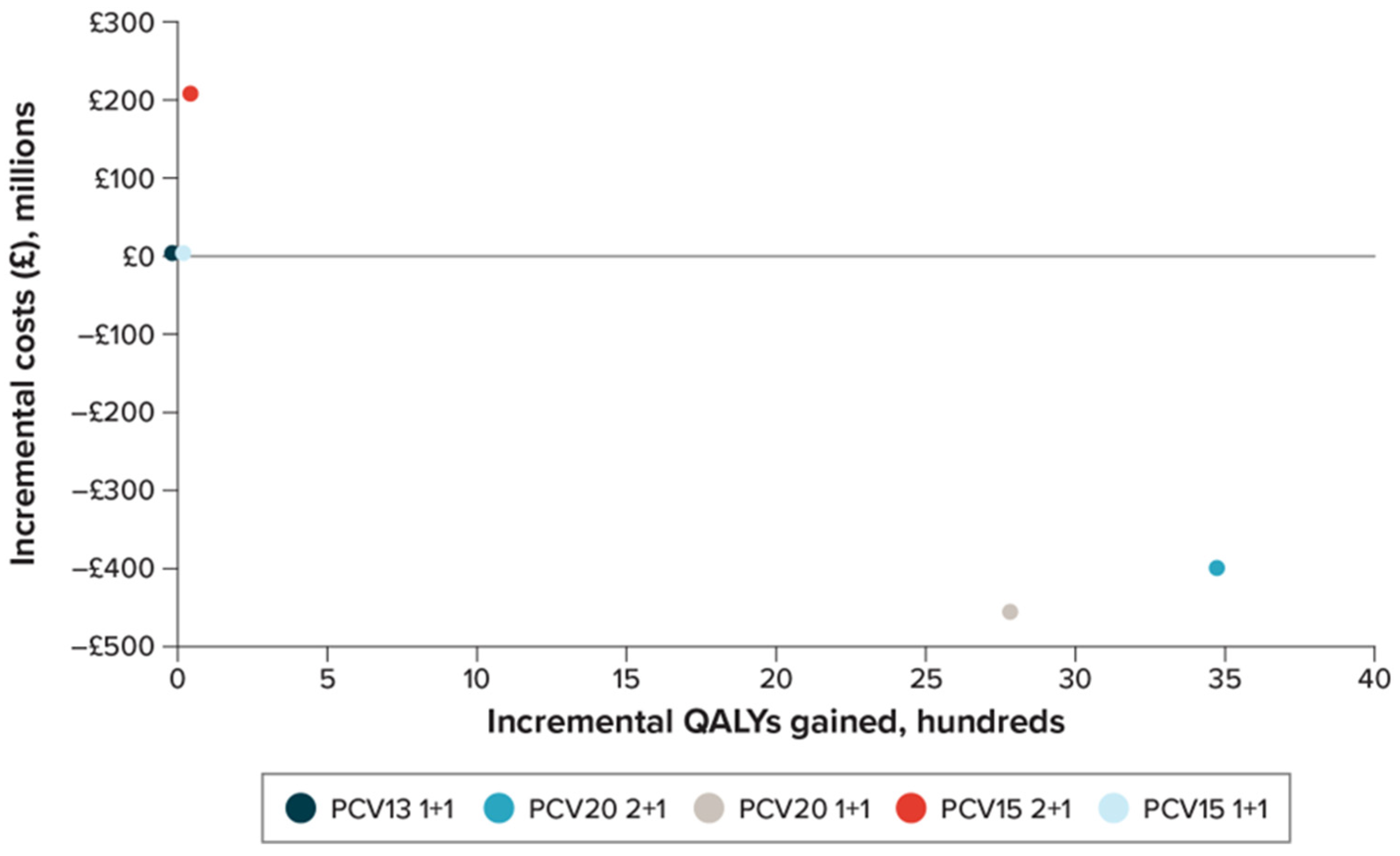
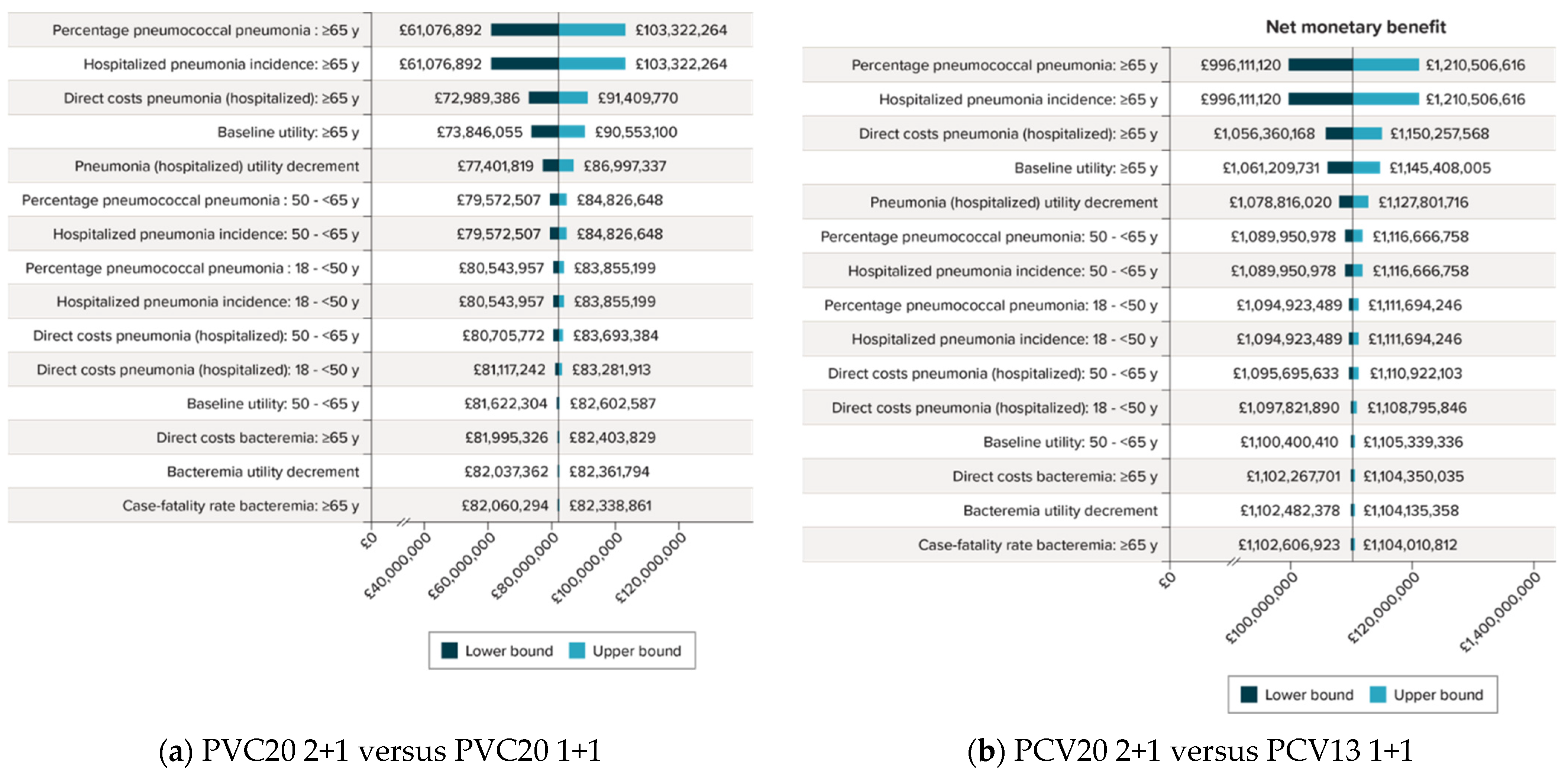
3.2. Base-Case Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chalmers, J.D.; Campling, J.; Dicker, A.; Woodhead, M.; Madhava, H. A systematic review of the burden of vaccine preventable pneumococcal disease in UK adults. BMC Pulm. Med. 2016, 16, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsaban, G.; Ben-Shimol, S. Indirect (herd) protection, following pneumococcal conjugated vaccines introduction: A systematic review of the literature. Vaccine 2017, 35, 2882–2891. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Factsheet about Pneumococcal Disease. 2023. Available online: https://www.ecdc.europa.eu/en/pneumococcal-disease/facts (accessed on 2 May 2023).
- Kandasamy, R.; Voysey, M.; Collins, S.; Berbers, G.; Robinson, H.; Noel, I.; Hughes, H.; Ndimah, S.; Gould, K.; Fry, N.; et al. Persistent circulation of vaccine serotypes and serotype replacement after 5 years of infant immunization with 13-valent pneumococcal conjugate vaccine in the United Kingdom. J. Infect. Dis. 2020, 221, 1361–1370. [Google Scholar] [CrossRef]
- Kent, A.; Makwana, A.; Sheppard, C.L.; Collins, S.; Fry, N.K.; Heath, P.T.; Ramsay, M.; Ladhani, S.N. Invasive pneumococcal disease in UK children < 1 year of age in the post-13-valent pneumococcal conjugate vaccine era: What are the risks now? Clin. Infect. Dis. 2019, 69, 84–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waight, P.A.; Andrews, N.J.; Ladhani, N.J.; Sheppard, C.L.; Slack, M.P.; Miller, E. Effect of the 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: An observational cohort study. Lancet Infect. Dis. 2015, 15, 629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, Y.H.; Andrews, N.; Miller, E. Estimated impact of revising the 13-valent pneumococcal conjugate vaccine schedule from 2+1 to 1+1 in England and Wales: A modelling study. PLoS Med. 2019, 16, e1002845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000–2017: A prospective national observational cohort study. Lancet Infect. Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Bertran, M.; Amin-Chowdhury, Z.; Sheppard, C.L.; Eletu, S.; Zamarreno, D.V.; Ramsay, M.E.; Litt, D.; Fry, N.K.; Ladhani, S.N. Increased incidence of invasive pneumococcal disease among children after COVID-19 pandemic, England. Emerg. Infect. Dis. 2022, 28, 1669–1672. [Google Scholar] [CrossRef]
- UK Health Security Agency. COVID-19 Vaccine Monthly Surveillance Reports. 2023. Available online: https://www.gov.uk/government/publications/covid-19-vaccine-weekly-surveillance-reports (accessed on 2 May 2023).
- Wasserman, M.; Lucas, A.; Jones, D.; Wilson, M.; Hilton, B.; Vyse, A.; Madhava, H.; Brogan, A.; Slack, M.; Farkouh, R. Dynamic transmission modelling to address infant pneumococcal conjugate vaccine schedule modifications in the UK. Epidemiol. Infect. 2018, 146, 1797–1806. [Google Scholar] [CrossRef] [Green Version]
- van Hoek, A.J.; Choi, Y.H.; Trotter, C.; Miller, E.; Jit, M. The cost-effectiveness of a 13-valent pneumococcal conjugate vaccination for infants in England. Vaccine 2012, 30, 7205–7213. [Google Scholar] [CrossRef]
- Lucas, A.; Wilson, M.; Sings, H.L.; Pugh, S.; Jones, D.; Farkouh, R.; Gessner, B.; Wasserman, M. Estimating the vaccine effectiveness against serotype 3 for the 13-valent pneumococcal conjugate vaccine: A dynamic modeling approach. Int. J. Infect. Dis. Ther. 2019, 4, 56–66. [Google Scholar] [CrossRef]
- Choi, Y.H.; Jit, M.; Flasche, S.; Gay, N.; Miller, E. Mathematical modelling long-term effects of replacing Prevnar7 with Prevnar13 on invasive pneumococcal diseases in England and Wales. PLoS ONE 2012, 7, e39927. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.; Hu, T.; Weaver, J.; Owusu-Edusei, K.; Elbasha, E. Cost-effectiveness analysis of routine use of 15-valent pneumococcal conjugate vaccine in the US pediatric population. Vaccines 2023, 11, 135. [Google Scholar] [CrossRef] [PubMed]
- Polistena, B.; Icardi, G.; Orsi, A.; Spandonaro, F.; Di Virgilio, R.; d’Angela, D. Cost-effectiveness of vaccination with the 20-valent pneumococcal conjugate vaccine in the Italian adult population. Vaccines 2022, 10, 2032. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Farrar, J.L.; Gierke, R.; Britton, A.; Childs, L.; Leidner, A.J.; Campos-Outcalt, D.; Morgan, R.L.; Long, S.S.; Talbot, H.K.; et al. Use of 15-valent pneumococcal conjugate vaccine and 20-valent pneumococcal conjugate vaccine among U.S. adults: Updated recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Mendes, D.; Averin, A.; Atwood, M.; Sato, R.; Vyse, A.; Campling, J.; Weycker, D.; Slack, M.; Ellsbury, G.; Mugwagwa, T. Cost-effectiveness of using a 20-valent pneumococcal conjugate vaccine to directly protect adults in England at elevated risk of pneumococcal disease. Expert Rev. Pharm. Outcomes Res. 2022, 22, 1285–1295. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence (NICE). Discounting of Health Benefits in Special Circumstances. 2011. Available online: https://www.nice.org.uk/guidance/ta235/resources/osteosarcoma-mifamurtide-discounting-of-health-benefits-in-special-circumstances2 (accessed on 1 June 2023).
- Mossong, J.; Hens, N.; Jit, M.; Beutels, P.; Auranen, K.; Mikolajczyk, R.; Massari, M.; Salmaso, S.; Tomba, G.S.; Wallinga, J.; et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med. 2008, 5, e74. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Podmore, B.; Cunado Moral, A.; Matthews, I.; Sarpong, E.; Lacetera, A.; Qizilbash, N. Incidence of pneumococcal disease from 2003 to 2019 in children ≤17 years in England. Pneumonia 2023, 15, 2. [Google Scholar] [CrossRef]
- Office for National Statistics (ONS). Population Estimates. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates (accessed on 6 April 2023).
- Office for National Statistics (ONS). Death Registration Summary Statistics, England and Wales: 2022. 2023. Available online: https://www.ons.gov.uk/releases/deathregistrationsummarystatisticsenglandandwales2022 (accessed on 2 May 2023).
- NHS Digital. Hospital Episode Statistics (HES). 2023. Available online: https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/hospital-episode-statistics (accessed on 2 May 2023).
- Mohanty, S.; Podmore, B.; Cunado Moral, A.; Weiss, T.; Matthews, I.; Sarpong, E.; Mendez, I.; Qizilbash, N. Incidence of acute otitis media from 2003 to 2019 in children ≤17 years in England. BMC Public Health 2023, 23, 201. [Google Scholar] [CrossRef] [PubMed]
- THIN-The Health Improvement Network. THIN Database—A Collaboration between In Practice Systems (INPS) and IMS Health. 2015. Available online: https://www.the-health-improvement-network.com/patient (accessed on 14 April 2015).
- Miller, E.; Andrews, N.J.; Waight, P.A.; Slack, M.P.; George, R.C. Herd immunity and serotype replacement 4 years after seven-valent pneumococcal conjugate vaccination in England and Wales: An observational cohort study. Lancet Infect. Dis. 2011, 11, 760–768. [Google Scholar] [CrossRef]
- Pick, H.; Daniel, P.; Rodrigo, C.; Bewick, T.; Ashton, D.; Lawrence, H.; Baskaran, V.; Edwards-Pritchard, R.C.; Sheppard, C.; Eletu, S.D.; et al. Pneumococcal serotype trends, surveillance and risk factors in UK adult pneumonia, 2013–2018. Thorax 2020, 75, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Delgleize, E.; Leeuwenkamp, O.; Theodorou, E.; Van de Velde, N. Cost-effectiveness analysis of routine pneumococcal vaccination in the UK: A comparison of the PHiD-CV vaccine and the PCV-13 vaccine using a Markov model. BMJ Open 2016, 6, e010776. [Google Scholar] [CrossRef]
- NHS Digital. Childhood Vaccination Coverage Statistics—England 2018–2019. 2019. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-immunisation-statistics/england-2018-19 (accessed on 6 March 2023).
- NHS Digital. 2020/21 National Cost Collection Data Publication. 2022. Available online: https://www.england.nhs.uk/publication/2020-21-national-cost-collection-data-publication/ (accessed on 2 May 2023).
- NHS Digital. Hospital Admitted Patient Care Activity 2020–2021. 2021. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/hospital-admitted-patient-care-activity/2020-21 (accessed on 2 May 2023).
- Ara, R.; Brazier, J.E. Using health state utility values from the general population to approximate baselines in decision analytic models when condition-specific data are not available. Value Health 2011, 14, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Mangen, M.J.; Huijts, S.M.; Bonten, M.J.; de Wit, G.A. The impact of community-acquired pneumonia on the health-related quality-of-life in elderly. BMC Infect. Dis. 2017, 17, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, N.; Kent, A.; Amin-Chowdhury, Z.; Sheppard, C.; Fry, N.; Ramsay, M.; Ladhani, S.N. Effectiveness of the seven-valent and thirteen-valent pneumococcal conjugate vaccines in England: The indirect cohort design, 2006–2018. Vaccine 2019, 37, 4491–4498. [Google Scholar] [CrossRef]
- Levy, C.; Varon, E.; Ouldali, N.; Wollner, A.; Thollot, F.; Corrard, F.; Werner, A.; Bechet, S.; Bonacorsi, S.; Cohen, R. Bacterial causes of otitis media with spontaneous perforation of the tympanic membrane in the era of 13 valent pneumococcal conjugate vaccine. PLoS ONE 2019, 14, e0211712. [Google Scholar] [CrossRef]
- Kaur, R.; Fuji, N.; Pichichero, M.E. Dynamic changes in otopathogens colonizing the nasopharynx and causing acute otitis media in children after 13-valent (PCV13) pneumococcal conjugate vaccination during 2015–2019. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 37–44. [Google Scholar] [CrossRef]
- Horn, E.K.; Wasserman, M.D.; Hall-Murray, C.; Sings, H.L.; Chapman, R.; Farkouh, R.A. Public health impact of pneumococcal conjugate vaccination: A review of measurement challenges. Expert Rev. Vaccines 2021, 20, 1291–1309. [Google Scholar] [CrossRef]
- Wilson, M.; Wasserman, M.; Jadavi, T.; Postma, M.; Breton, M.C.; Peloquin, F.; Earnshaw, S.; McDade, C.; Sings, H.; Farkouh, R. Clinical and economic impact of a potential switch from 13-valent to 10-valent pneumococcal conjugate infant vaccination in Canada. Infect. Dis. Ther. 2018, 7, 353–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, M.D.; Perdrizet, J.; Grant, L.; Hayford, K.; Singh, S.; Saharia, P.; Horn, E.K.; Farkouh, R.A. Clinical and economic burden of pneumococcal disease due to serotypes contained in current and investigational pneumococcal conjugate vaccines in children under five years of age. Infect. Dis. Ther. 2021, 10, 2701–2720. [Google Scholar] [CrossRef]
- Perdrizet, J.; Lai, Y.S.; Williams, S.; Struwig, V.A.; Wasserman, M. Retrospective impact analysis and cost-effectiveness of the pneumococcal conjugate vaccine infant program in Australia. Infect. Dis. Ther. 2021, 10, 507–520. [Google Scholar] [CrossRef]
- MedicinesComplete. British National Formulary. 2023. Available online: https://about.medicinescomplete.com/publication/british-national-formulary/ (accessed on 2 May 2023).
- National Health Service (NHS). General Medical Services Statement of Financial Entitlements (Amendment) (No. 5) Directions. 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1138355/general-medical-services-statement-of-financial-entitlements-amendment-no5-directions-2022.pdf (accessed on 16 March 2023).
- Shiri, T.; Khan, K.; Keaney, K.; Mukherjee, G.; McCarthy, N.D.; Petrou, S. Pneumococcal disease: A systematic review of health utilities, resource use, costs, and economic evaluations of interventions. Value Health 2019, 22, 1329–1344. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Givon-Lavi, N.; Dagan, R. Dose-specific effectiveness of 7- and 13-valent pneumococcal conjugate vaccines against vaccine-serotype Streptococcus pneumoniae colonization in children. Clin. Infect. Dis. 2020, 71, e289–e300. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence (NICE). Guide to the Methods of Technology Appraisal; NICE: London, UK, 2013. [Google Scholar]
- Pitman, R.; Fisman, D.; Zaric, G.S.; Postma, M.; Kretzschmar, M.; Edmunds, J.; Brisson, M.; ISPOR-SMDM Modeling Good Research Practices Task Force. Dynamic transmission modeling: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force—5. Value Health 2012, 15, 828–834. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.H.; Miller, E. Impact of COVID-19 social distancing measures on future incidence of invasive pneumococcal disease in England and Wales: A mathematical modelling study. BMJ Open 2021, 11, e045380. [Google Scholar] [CrossRef]
- Perniciaro, S.; van der Linden, M.; Weinberger, D.M. Reemergence of invasive pneumococcal disease in Germany during the spring and summer of 2021. Clin. Infect. Dis. 2022, 75, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Ouldali, N.; Deceuninck, G.; Lefebvre, B.; Gilca, R.; Quach, C.; Brousseau, N.; Tapiero, B.; De Wals, P. Increase of invasive pneumococcal disease in children temporally associated with RSV outbreak in Quebec: A time-series analysis. Lancet Reg. Health Am. 2023, 19, 100448. [Google Scholar] [CrossRef]
- Murad, C.; Dunne, E.M.; Sudigdoadi, S.; Fadlyana, E.; Tarigan, R.; Pell, C.L.; Watts, E.; Nguyen, C.D.; Satzke, C.; Hinds, J.; et al. Pneumococcal carriage, density, and co-colonization dynamics: A longitudinal study in Indonesian infants. Int. J. Infect. Dis. 2019, 86, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legg, J.; Charlotte, R. British Thoracic Society Paediatric Pneumonia Audit. National Audit Period: 1 November 2016–31 January 2017. Available online: https://www.brit-thoracic.org.uk/document-library/quality-improvement/audit-reports/paediatric-pneumonia-201617/ (accessed on 2 May 2023).
- Office for National Statistics (ONS). EARN01: Average Weekly Earnings [Dataset]. 2023. Available online: https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/earningsandworkinghours/datasets/averageweeklyearningsearn01 (accessed on 2 May 2023).




{kind=link}
{kind=link}
{kind=link}
| Parameter | Age Group, y | ||||
|---|---|---|---|---|---|
| 0–4 | 5–17 | 18–49 | 50–64 | ≥65 | |
| Population a | 1,342,117 | 9,874,836 | 26,085,921 | 12,601,911 | 10,297,259 |
| All-cause mortality per 100,000 b | 201 | 15 | 94 | 500 | 4322 |
| Overall IPD incidence per 100,000 c | 7.95 | 1.51 | 3.37 | 10.60 | 28.84 |
| Hospitalized CAP incidence per 100,000 d | 355.07 | 43.25 | 121.62 | 439.95 | 3105.90 |
| Mild otitis media incidence per 100,000 e | 5564.55 | N/A | N/A | N/A | N/A |
| Moderate/severe otitis media incidence per 100,000 f | 243.50 | N/A | N/A | N/A | N/A |
| Percentage of IPD that is meningitis g | 73.6% | 57.7% | 1.9% | 1.9% | 1.2% |
| Percentage of pneumonia pneumococcal h | 20% | 20% | 39.8% | 39.8% | 39.8% |
| Percentage of otitis media pneumococcal i | 20% | N/A | N/A | N/A | N/A |
| Case fatality rates j | |||||
| IPD | 0.148 | 0.063 | 0.123 | 0.159 | 0.304 |
| Hospitalized pneumonia | 0.002 | 0.016 | 0.049 | 0.140 | 0.367 |
| Vaccine adherence (%) (1st primary dose/2nd primary dose/booster dose) k | |||||
| 2006–2010 | 95.0/95.0/85.0 | ||||
| 2010 onwards | 97.0/97.0/91.0 | ||||
| Vaccine costs, per dose (GBP) | |||||
| Administration | 10.06 | ||||
| PCV13 | 49.10 | ||||
| PCV15 | 50.30 | ||||
| PCV20 | 56.50 | ||||
| Direct costs (GBP) l | |||||
| Bacteremia | 4214 | 4214 | 7010 | 7010 | 7010 |
| Meningitis | 6245 | 6245 | 8608 | 8608 | 8608 |
| Otitis media (mild) | 67 | N/A | N/A | N/A | N/A |
| Otitis media (moderate/severe) | 737 | N/A | N/A | N/A | N/A |
| Pneumonia (hospitalized) | 3756 | 3756 | 6472 | 6472 | 6472 |
| Utility weights m | |||||
| Baseline utility | 0.9564 | 0.9564 | 0.9564 | 0.9335 | 0.8900 |
| Disutility of bacteremia/meningitis | 0.13 | 0.13 | 0.13 | 0.13 | 0.13 |
| Disutility of hospitalized pneumonia | 0.13 | 0.13 | 0.13 | 0.13 | 0.13 |
| Disutility of otitis media | 0.0035 | 0.0035 | 0.0035 | 0.0035 | 0.0035 |
| Parameter | 1st Primary Dose | 2nd Primary Dose | Booster Dose |
|---|---|---|---|
| Vaccine effectiveness against IPD (overall), % a | |||
| Serotype 8 | 74.3 | 74.3 | 75.0 |
| Serotype 3 | 20.9 | 56.8 | 71.2 |
| Serotypes 1, 5, 7F, 6A | 74.3 | 74.3 | 75.0 |
| Serotype 19A | 69.4 | 98.0 | 98.6 |
| PCV7 serotypes | 81.7 | 95.5 | 98.8 |
| Serotypes 22F and 33F | 74.3 | 74.3 | 75.0 |
| Serotypes 10A, 11A, 12F, and 15B | 74.3 | 74.3 | 75.0 |
| Vaccine effectiveness against carriage, % a | |||
| Serotype 8 | 20.8 | 41.7 | 65.0 |
| Serotype 3 | 0.7 | 5.2 | 5.9 |
| Serotypes 1, 5, 7F, 6A | 20.8 | 41.7 | 65.0 |
| Serotype 19A | 2.7 | 20.8 | 21.2 |
| PCV7 serotypes | 35.0 | 77.8 | 88.8 |
| Serotypes 22F and 33F | 20.8 | 41.7 | 65.0 |
| Serotypes 10A, 11A, 12F, and 15B | 20.8 | 41.7 | 65.0 |
| Mean duration of protection, years | 0.7 | 0.7 | 1.4 |
| Scenario Description | Modified Inputs |
|---|---|
| Varying the vaccine effectiveness against carriage and against IPD for the additional serotypes covered in PCV20 versus PCV13 by +/− 10% | Vaccine effectiveness to carriage and vaccine effectiveness to IPD |
| Assuming no difference in booster dose vaccine effectiveness against carriage between 2+1 and 1+1 schedules | No reduction in booster dose effectiveness |
| Inclusion of societal costs (see Supplementary Material) | Additional inputs of hourly wages and hours of lost productivity per case for persons/caregivers (see Table S5) |
| Results | PCV13 1+1 | PCV15 1+1 | PCV15 2+1 | PCV20 1+1 | PCV20 2+1 |
|---|---|---|---|---|---|
| No. of disease cases | |||||
| Bacteremia | 8400 | 8385 | 8375 | 7599 | 7407 |
| Meningitis | 23,419 | 23,376 | 23,347 | 21,186 | 20,651 |
| Otitis media | 309,721 | 304,747 | 302,919 | 286,565 | 281,731 |
| Pneumonia | 1,018,891 | 1,017,705 | 1,016,844 | 933,585 | 913,092 |
| Total cases | 1,360,432 | 1,354,212 | 1,351,485 | 1,248,936 | 1,222,881 |
| No. of deaths | |||||
| IPD | 7348 | 7337 | 7330 | 6702 | 6547 |
| Pneumonia | 329,334 | 329,044 | 328,812 | 303,356 | 297,104 |
| Outcomes | |||||
| Life-years | 292,019,917 | 292,020,179 | 292,020,392 | 292,043,082 | 292,048,735 |
| QALYs | 249,069,025 | 249,069,386 | 249,069,665 | 249,097,121 | 249,104,034 |
| Costs | |||||
| Vaccination | GBP 389,480,098 | GBP 397,380,303 | GBP 601,882,252 | GBP 427,783,464 | GBP 605,082,671 |
| IPD | GBP 199,208,904 | GBP 198,880,014 | GBP 198,654,045 | GBP 180,839,611 | GBP 176,372,013 |
| Pneumonia | GBP 5,910,059,997 | GBP 5,904,041,761 | GBP 5,899,346,527 | GBP 5,432,747,000 | GBP 5,316,351,443 |
| Otitis media | GBP 25,105,771 | GBP 24,677,615 | GBP 24,526,927 | GBP 23,292,008 | GBP 22,921,733 |
| Total | GBP 6,523,854,771 | GBP 6,524,979,693 | GBP 6,724,409,752 | GBP 6,064,662,083 | GBP 6,120,727,860 |
| ICER | |||||
| vs. PCV13 | GBP 3112 | GBP 313,229 | Dominant | Dominant | |
| vs. PCV15 1+1 | GBP 715,179 | Dominant | Dominant | ||
| vs. PCV15 2+1 | Dominant | Dominant | |||
| vs. PCV20 1+1 | GBP 8110 |
| Scenario | Outcome | PCV20 2+1 | PCV13 1+1 | PCV15 1+1 | PCV20 1+1 | PCV15 2+1 |
|---|---|---|---|---|---|---|
| Base case | Total cost | GBP 6,116,860,165 | GBP 6,523,854,771 | GBP 6,517,281,841 | GBP 6,060,729,843 | GBP 6,717,270,837 |
| Total QALYs | 249,104,034 | 249,069,025 | 249,069,477 | 249,097,121 | 249,069,665 | |
| ICER | Dominant | Dominant | GBP 8119 | Dominant | ||
| PCV20-13 VE 10% higher | Total cost | GBP 6,096,801,176 | GBP 6,523,854,771 | GBP 6,524,319,132 | GBP 6,037,091,426 | GBP 6,723,498,496 |
| Total QALYs | 249,105,398 | 249,069,025 | 249,069,421 | 249,098,684 | 249,069,715 | |
| ICER | Dominant | Dominant | GBP 8893 | Dominant | ||
| PCV20-13 VE 10% lower | Total cost | GBP 6,148,586,783 | GBP 6,523,854,771 | GBP 6,525,643,282 | GBP 6,095,526,080 | GBP 6,725,327,097 |
| Total QALYs | 249,102,447 | 249,069,025 | 249,069,351 | 249,095,372 | 249,069,615 | |
| ICER | Dominant | Dominant | GBP 7500 | Dominant | ||
| Equal booster VEc | Total cost | GBP 6,116,860,165 | GBP 6,523,854,771 | GBP 6,523,427,466 | GBP 5,993,157,158 | GBP 6,717,270,837 |
| Total QALYs | 249,104,034 | 249,069,025 | 249,069,477 | 249,101,199 | 249,069,665 | |
| ICER | Dominant | Dominant | GBP 44,994 | Dominant | ||
| Societal perspective | Total cost | GBP 6,370,442,692 | GBP 6,806,691,873 | GBP 6,806,783,657 | GBP 6,320,777,968 | GBP 7,005,697,126 |
| Total QALYs | 249,104,034 | 249,069,025 | 249,069,386 | 249,097,121 | 249,069,665 | |
| ICER | Dominant | Dominant | GBP 7184 | Dominant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, M.; Lucas, A.; Mendes, D.; Vyse, A.; Mikudina, B.; Czudek, C.; Ellsbury, G.F.; Perdrizet, J. Estimating the Cost-Effectiveness of Switching to Higher-Valency Pediatric Pneumococcal Conjugate Vaccines in the United Kingdom. Vaccines 2023, 11, 1168. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11071168
Wilson M, Lucas A, Mendes D, Vyse A, Mikudina B, Czudek C, Ellsbury GF, Perdrizet J. Estimating the Cost-Effectiveness of Switching to Higher-Valency Pediatric Pneumococcal Conjugate Vaccines in the United Kingdom. Vaccines. 2023; 11(7):1168. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11071168
Chicago/Turabian StyleWilson, Michele, Aaron Lucas, Diana Mendes, Andrew Vyse, Boglarka Mikudina, Carole Czudek, Gillian Frances Ellsbury, and Johnna Perdrizet. 2023. "Estimating the Cost-Effectiveness of Switching to Higher-Valency Pediatric Pneumococcal Conjugate Vaccines in the United Kingdom" Vaccines 11, no. 7: 1168. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11071168