Corticosteroids Contribute to Serious Adverse Events Following Live Attenuated Varicella Vaccination and Live Attenuated Zoster Vaccination


Abstract
:1. Introduction
2. Case Summaries of Viral SAEs after Live Varicella Vaccination
- 1.
- This child was 13 months old when she developed fever, jaundice, diarrhea and a papular rash [15]. Because of a Coombs-positive anemia, she received both intravenous gamma globulin and high-dosage methylprednisolone (80 mg/day). Over the next three weeks, her skin lesions became eschars. Skin biopsy subsequently revealed intranuclear inclusions typical of herpesviruses, and intravenous (IV) acyclovir therapy was initiated. She later died. Three weeks before her illness she had received her varicella vaccination. Vaccine type varicella was recovered from tissues at autopsy. A genetic analysis detected two mutations in exon 2 of the recombination activating gene 2 (RAG2), but she never had the complete picture of severe combined immunodeficiency (SCID).
- 2.
- This 13-month-old girl developed disseminated varicella with shock syndrome and death within 4 weeks of varicella vaccination [16]. During her hospitalization, vaccine virus was recovered from respiratory secretions. Genetic testing uncovered adenosine deaminase deficiency leading to SCID. During her hospitalization, she received both antiviral therapy (acyclovir and foscarnet) and antibacterial therapy (cefotaxime and clindamycin), but death ensued. A medical chart review revealed that she had a history of lung infections and oral candidiasis during the second half of her first year of life. There was no mention of corticosteroid prescriptions.
- 3.
- This 13-month old was hospitalized because of suspected sepsis. He had a past medical history of failure to thrive with multiple low grade infections [17]. He had been given varicella vaccine 2 weeks before admission. On initial examination, he had signs of pneumonia and hepatitis. He was intubated and treated with broad spectrum antibiotics. Two weeks after admission (4 weeks after vaccination), he developed a rash and the diagnosis of disseminated varicella vaccine infection was made, based on polymerase chain reaction (PCR) results from skin lesions. After 2 weeks of antiviral therapy with IV acyclovir, he improved enough to remove ventilator support. At this time, he was placed briefly on high-dosage dexamethasone (0.3 mg/kg every 6 h for 10 doses). Within 5 days, his vesicular rash returned and he required additional antiviral treatment. He survived his hospitalization and was subsequently diagnosed with SCID and adenosine deaminase deficiency.
- 4.
- This 15-month-old girl had had a prior history of pulmonary infections, global developmental delay, failure to thrive, and profound hypotonia [18]. She had a gastrostomy tube placed at 9 months due to poor feeding. She had been hospitalized several times and had been given corticosteroids during these hospitalizations. One week after varicella vaccination at age 14 months, she was hospitalized for respiratory distress. She again received IV methylprednisolone (3.5 mg every 12 h for six doses) followed by prednisolone (3.5 mg every 12 h for four doses) via g-tube for treatment of the pulmonary distress. On hospital day 14, she was discharged. A rash was noticed soon after discharge, and she was readmitted because of pulmonary distress. Vaccine virus was identified in the skin lesions. She was begun on a low-dose prolonged corticosteroid therapy protocol. Despite concomitant treatment with IV acyclovir (130 mg every 6 h) for varicella vaccine infection, she died. No specific immune deficiency was identified; genetic testing excluded SCID.
- 5.
- This 4-year-old girl was undergoing treatment for acute lymphoblastic leukemia [19]. Her therapy regimen is not described in detail but would have included either dexamethasone or prednisone. She was admitted because of rapidly progressive multi-organ failure and acute respiratory distress syndrome. Screening PCR testing detected varicella vaccine DNA in the blood. She was treated with IV acyclovir as well as piperacillin, sulbactam, tobramycin and IV immunoglobulin. The child died of varicella pneumonitis on day 10 of hospitalization. The child had received varicella vaccine 32 days before onset of the current illness. Her chemotherapy had been halted one week before vaccination and restarted one week after vaccination.
- 6.
- This 6-year-old boy had a long history of atopy, asthma and eosinophilia [20]. He had received his one and only varicella vaccination at age 1 year. Because of his recurrent allergic episodes, including bouts of asthma, he had received several courses of corticosteroids. At age 6, he presented with evidence of a stroke. The stroke was treated with methylprednisolone followed by oral prednisone (2 mg/kg daily for 3 days) and subsequently prednisolone (1 mg/kg daily for 2 weeks). One month later, he developed additional CNS symptoms and vaccine varicella infection was diagnosed after testing the cerebrospinal fluid by virus-specific PCR. Genetic testing revealed a deficiency of dedicator of cytokinesis 8 (DOCK8). His serum IgE level was 472 IU/mL. He was treated with IV acyclovir and oral prednisolone (2 mg/kg daily for 2 weeks).
- 7.
- This 6-year-old boy had a history of severe developmental delay and spastic quadriplegia with epilepsy [21]. He had had no serious infectious illnesses during his first 5 years of life. He had received the measles–mumps–rubella vaccination without a problem. However, 3 weeks after his first varicella vaccination in his 6th year, he developed fever and a rash over his entire body. Later he developed pneumonitis. A diagnosis of disseminated varicella vaccine virus infection was made by PCR testing. He was treated with IV acyclovir, flucloxacillin and clindamycin. The child recovered after prolonged antiviral and antibacterial treatment. An immune assessment discovered a reduction in natural killer (NK) cell activity. There is no mention of corticosteroids in the case report.
- 8.
- This 11-year-old had a past history of severe congenital cytomegalovirus infections with intellectual disability [22]. She presented with respiratory distress and bilateral alveolar infiltrates on chest film. She had received a varicella vaccination 5 weeks before the current illness. Vaccine virus was identified by PCR in respiratory secretions. Because of the severity of the respiratory distress, she was given methylprednisolone in addition to acyclovir for treatment of her pulmonary disease and disseminated varicella vaccine infection. She improved on this regimen after 17 days and was discharged, with a prescription for one week of acyclovir tablets. However, she died 10 months after the pulmonary infection. The exact cause of death was unclear, but an embolic episode was suspected. An immune assessment uncovered diminished NK cell activity.
3. Reassessment of the above Cases
4. Case summaries of Viral SAEs after Live Zoster Vaccination
- 1.
- This case is a 79-year-old man from Scotland with chronic lymphocytic leukemia (CLL) [32]. The patient had received chemotherapy with fludarabine, cyclophosphamide and rituximab in the past, but he had not received any chemotherapy for 6 months. Then, he was given a live attenuated zoster vaccination. Within 2 weeks, he manifested signs of a disseminated zoster vaccine infection. Vaccine virus was identified in the skin vesicles. Even after receiving antiviral treatment, the patient died on day 25 of his hospitalization. There is no mention in the case report that the patient received corticosteroids for any reason during the 6-month interval between cessation of chemotherapy and administration of the zoster vaccine.
- 2.
- This case is a 71-year-old man from Australia with CLL [33]. He was not receiving active treatment for CLL because of other chronic illnesses. He was given a live attenuated zoster vaccination 3 weeks before he presented with a bilateral facial rash diagnosed as herpes zoster. Subsequently, he developed signs of a disseminated zoster vaccine infection with meningoencephalitis, confirmed by PCR testing. He died of respiratory failure secondary to varicella pneumonitis. There is no description of treatment with corticosteroids in the case report.
- 3.
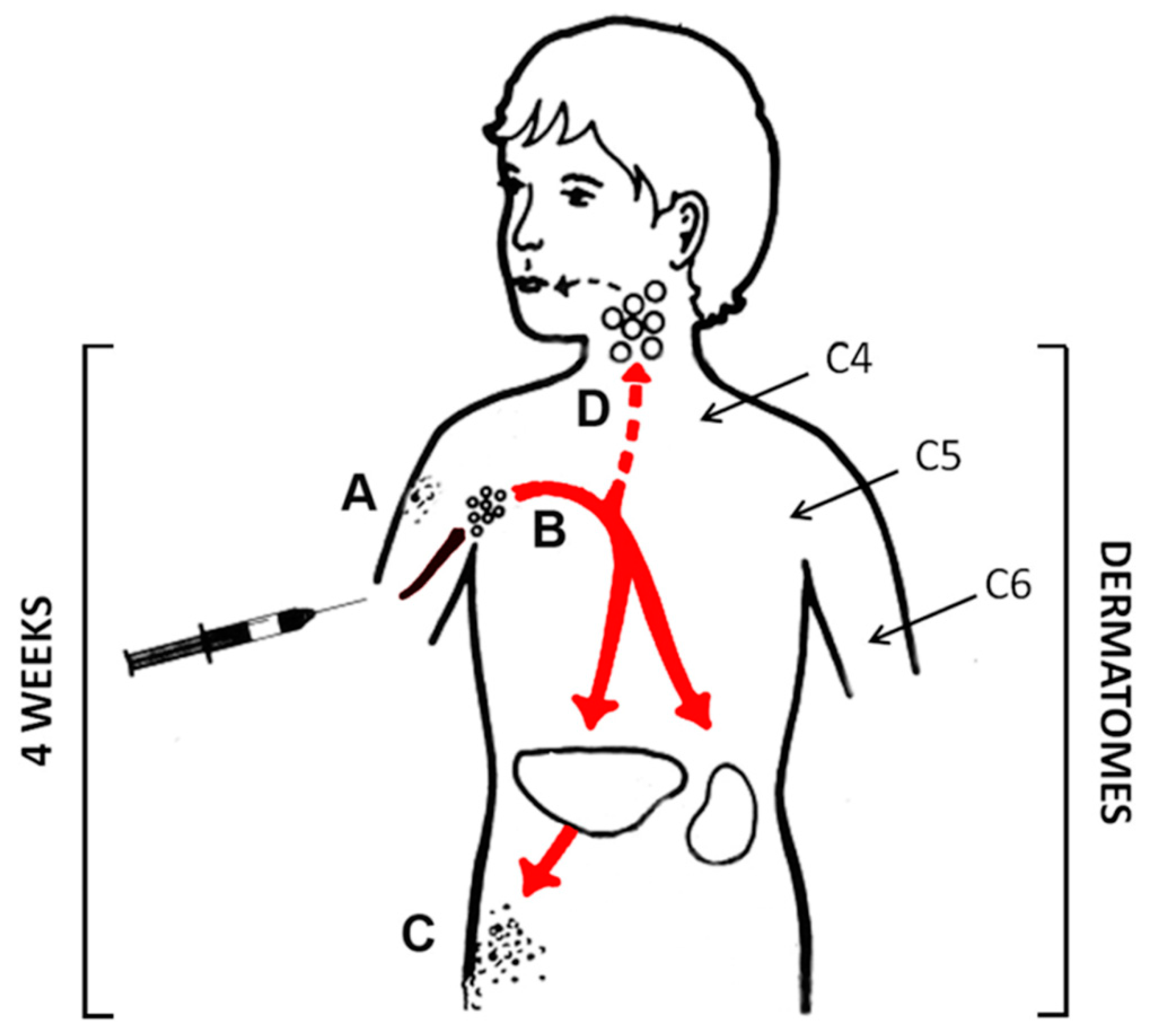
- This case is a 70-year-old man from Canada with rheumatoid arthritis [34]. He was being treated with methotrexate, hydroxychloroquine and prednisone. The prednisone dosage was 10 mg/day. He had a history of chickenpox as a child. One month after receiving a live attenuated zoster vaccine, he developed a disseminated zoster vaccine infection and died on the fifth day of his viral illness. Vaccine virus was confirmed by PCR testing of a skin vesicle. It is clearly stated in the case report that the patient continued to take prednisone on the day that he was immunized and probably until the day he developed a rash.
5. Reassessment of the above Cases
6. Corticosteroids as a Risk Factor for Severe Varicella and Herpes Zoster
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gershon, A.A. Varicella vaccine: Its past, present and future. Pediatr Infect. Dis. J. 1995, 14, 742–744. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M. Effectiveness of live varicella vaccine. Expert Opin. Biol. Ther. 2004, 4, 199–216. [Google Scholar] [CrossRef] [PubMed]
- Grose, C. Varicella vaccination of children in the United States: Assessment after the first decade 1995–2005. J. Clin. Virol. 2005, 33, 89–95. [Google Scholar] [CrossRef]
- Seward, J.F.; Marin, M.; Vazquez, M. Varicella vaccine effectiveness in the US vaccination program: A review. J. Infect. Dis. 2008, 197 (Suppl. 2), S82–S89. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.; Marin, M. Update on trends in varicella mortality during the varicella vaccine era-United States, 1990–2016. Hum. Vaccines Immunother. 2018, 14, 2460–2463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oxman, M.N.; Levin, M.J.; Johnson, G.R.; Schmader, K.E.; Straus, S.E.; Gelb, L.D.; Arbeit, R.D.; Simberkoff, M.S.; Gershon, A.A.; Davis, L.E.; et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N. Engl. J. Med. 2005, 352, 2271–2284. [Google Scholar] [CrossRef] [Green Version]
- Kimberlin, D.W.; Whitley, R.J. Varicella-zoster vaccine for the prevention of herpes zoster. N. Engl. J. Med. 2007, 356, 1338–1343. [Google Scholar] [CrossRef] [Green Version]
- Varela, F.H.; Pinto, L.A.; Scotta, M.C. Global impact of varicella vaccination programs. Hum. Vaccines Immunother. 2019, 15, 645–657. [Google Scholar] [CrossRef] [Green Version]
- Damm, O.; Ultsch, B.; Horn, J.; Mikolajczyk, R.T.; Greiner, W.; Wichmann, O. Systematic review of models assessing the economic value of routine varicella and herpes zoster vaccination in high-income countries. BMC Public Health 2015, 15, 533. [Google Scholar] [CrossRef] [Green Version]
- Miller, E.R.; Lewis, P.; Shimabukuro, T.T.; Su, J.; Moro, P.; Woo, E.J.; Jankosky, C.; Cano, M. Post-licensure safety surveillance of zoster vaccine live (Zostavax(R)) in the United States, Vaccine Adverse Event Reporting System (VAERS), 2006–2015. Hum. Vaccines Immunother. 2018, 14, 1963–1969. [Google Scholar] [CrossRef] [Green Version]
- Baxter, R.; Tran, T.N.; Hansen, J.; Emery, M.; Fireman, B.; Bartlett, J.; Lewis, N.; Saddier, P. Safety of Zostavax—A cohort study in a managed care organization. Vaccine 2012, 30, 6636–6641. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.A.; Sweet, A.; Beninger, P.; Steinberg, S.P.; Larussa, P.S.; Gershon, A.A.; Sharrar, R.G. The safety profile of varicella vaccine: A 10-year review. J. Infect. Dis. 2008, 197 (Suppl. 2), S165–S169. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.; Elliott, S.C.; Rogers, K.L.; Cohrs, R.J.; Weinberger, M.; Jackson, W.; Carpenter, J.E.; Grose, C.; Bonthius, D.J. Varicella Vaccine Meningitis as a Complication of Herpes Zoster in Twice-Immunized Immunocompetent Adolescents. J. Child Neurol. 2020, 35, 889–895. [Google Scholar] [CrossRef]
- Woodward, M.; Marko, A.; Galea, S.; Eagel, B.; Straus, W. Varicella Virus Vaccine Live: A 22-Year Review of Postmarketing Safety Data. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2019; Volume 6. [Google Scholar]
- Dutmer, C.M.; Asturias, E.J.; Smith, C.; Dishop, M.K.; Schmid, D.S.; Bellini, W.J.; Tirosh, I.; Lee, Y.N.; Notarangelo, L.D.; Gelfand, E.W. Late Onset Hypomorphic RAG2 Deficiency Presentation with Fatal Vaccine-Strain VZV Infection. J. Clin. Immunol. 2015, 35, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Woo, E.J. Letter to the editor: Fatal varicella due to the vaccine-strain varicella-zoster virus. Hum. Vaccines Immunother. 2015, 11, 679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaffar, F.; Carrick, K.; Rogers, B.B.; Margraf, L.R.; Krisher, K.; Ramilo, O. Disseminated infection with varicella-zoster virus vaccine strain presenting as hepatitis in a child with adenosine deaminase deficiency. Pediatr. Infect. Dis. J. 2000, 19, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.; Siegel, S.; Jones, J.F.; Schulte, C.; Blog, D.; Schmid, D.S.; Bialek, S.R.; Marin, M. Fatal varicella due to the vaccine-strain varicella-zoster virus. Hum. Vaccines Immunother. 2014, 10, 146–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrauder, A.; Henke-Gendo, C.; Seidemann, K.; Sasse, M.; Cario, G.; Moericke, A.; Schrappe, M.; Heim, A.; Wessel, A. Varicella vaccination in a child with acute lymphoblastic leukaemia. Lancet 2007, 369, 1232. [Google Scholar] [CrossRef]
- Sabry, A.; Hauk, P.J.; Jing, H.; Su, H.C.; Stence, N.V.; Mirsky, D.M.; Nagel, M.A.; Abbott, J.K.; Dragone, L.L.; Armstrong-Wells, J.; et al. Vaccine strain varicella-zoster virus-induced central nervous system vasculopathy as the presenting feature of DOCK8 deficiency. J. Allergy Clin. Immunol. 2014, 133, 1225–1227. [Google Scholar] [CrossRef] [Green Version]
- Banovic, T.; Yanilla, M.; Simmons, R.; Robertson, I.; Schroder, W.A.; Raffelt, N.C.; Wilson, Y.A.; Hill, G.R.; Hogan, P.; Nourse, C.B. Disseminated varicella infection caused by varicella vaccine strain in a child with low invariant natural killer T cells and diminished CD1d expression. J. Infect. Dis. 2011, 204, 1893–1901. [Google Scholar] [CrossRef] [Green Version]
- Levy, O.; Orange, J.S.; Hibberd, P.; Steinberg, S.; LaRussa, P.; Weinberg, A.; Wilson, S.B.; Shaulov, A.; Fleisher, G.; Geha, R.S.; et al. Disseminated varicella infection due to the vaccine strain of varicella-zoster virus, in a patient with a novel deficiency in natural killer T cells. J. Infect. Dis. 2003, 188, 948–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballow, M.; Hirschhorn, R. Varicella pneumonia in a bone marrow-transplanted, immune-reconstituted adenosine deaminase-deficient patient with severe combined immunodeficiency disease. J. Clin. Immunol. 1985, 5, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Goda, V.; Malik, A.; Kalmar, T.; Maroti, Z.; Patel, B.; Ujhazi, B.; Csomos, K.; Hale, J.E.; Chen, K.; Bleesing, J.; et al. Partial RAG deficiency in a patient with varicella infection, autoimmune cytopenia, and anticytokine antibodies. J. Allergy Clin. Immunol. Pract. 2018, 6, 1769–1771.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biron, C.A.; Byron, K.S.; Sullivan, J.L. Severe herpesvirus infections in an adolescent without natural killer cells. N. Engl. J. Med. 1989, 320, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Heusel, E.H.; Grose, C. Twelve Children with Varicella Vaccine Meningitis: Neuropathogenesis of Reactivated Live Attenuated Varicella Vaccine Virus. Viruses 2020, 12, 1078. [Google Scholar] [CrossRef]
- Grose, C. Pathogenesis of infection with varicella vaccine. Infect. Dis. Clin. N. Am. 1996, 10, 489–505. [Google Scholar] [CrossRef]
- Hill, G.; Chauvenet, A.R.; Lovato, J.; McLean, T.W. Recent steroid therapy increases severity of varicella infections in children with acute lymphoblastic leukemia. Pediatrics 2005, 116, e525–e529. [Google Scholar] [CrossRef] [Green Version]
- Ozaki, T.; Masuda, S.; Asano, Y.; Kondo, K.; Namazue, J.; Yamanishi, K. Investigation of varicella-zoster virus DNA by the polymerase chain reaction in healthy children with varicella vaccination. J. Med. Virol. 1994, 42, 47–51. [Google Scholar] [CrossRef]
- Su, J.R.; Ng, C.; Lewis, P.W.; Cano, M.V. Adverse events after vaccination among HIV-positive persons, 1990–2016. PLoS ONE 2018, 13, e0199229. [Google Scholar] [CrossRef] [Green Version]
- Kramer, J.M.; LaRussa, P.; Tsai, W.C.; Carney, P.; Leber, S.M.; Gahagan, S.; Steinberg, S.; Blackwood, R.A. Disseminated vaccine strain varicella as the acquired immunodeficiency syndrome-defining illness in a previously undiagnosed child. Pediatrics 2001, 108, E39. [Google Scholar] [CrossRef] [Green Version]
- Costa, E.; Buxton, J.; Brown, J.; Templeton, K.E.; Breuer, J.; Johannessen, I. Fatal disseminated varicella zoster infection following zoster vaccination in an immunocompromised patient. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, K.E.; Tong, P.L.; Macartney, K.; Beresford, R.; Sheppeard, V.; Gupta, M. Live zoster vaccination in an immunocompromised patient leading to death secondary to disseminated varicella zoster virus infection. Vaccine 2018, 36, 3890–3893. [Google Scholar] [CrossRef] [PubMed]
- Dubey, V.; MacFadden, D. Disseminated varicella zoster virus infection after vaccination with a live attenuated vaccine. CMAJ 2019, 191, E1025–E1027. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, N.L.; Eberhardt, C.S.; Wieland, A.; Vora, K.A.; Pulendran, B.; Ahmed, R. Understanding the immunology of the Zostavax shingles vaccine. Curr. Opin. Immunol. 2019, 59, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, M.L. Herpes zoster with a varicelliform eruption and parotitis in chronic leukemia. J. Am. Med. Assoc. 1951, 145, 560–561. [Google Scholar] [CrossRef]
- Carter-Timofte, M.E.; Paludan, S.R.; Mogensen, T.H. RNA Polymerase III as a Gatekeeper to Prevent Severe VZV Infections. Trends Mol. Med. 2018, 24, 904–915. [Google Scholar] [CrossRef]
- Dowell, S.F.; Bresee, J.S. Severe varicella associated with steroid use. Pediatrics 1993, 92, 223–228. [Google Scholar]
- Zhang, W.; Ruan, Q.L.; Yan, F.; Hu, Y.K. Fatal hemorrhagic varicella in a patient with abdominal pain: A case report. BMC Infect. Dis. 2020, 20, 54. [Google Scholar] [CrossRef]
- Shee, J.C.; Fehrsen, P. Reactivation of varicella virus by cortisone therapy. Br. Med. J. 1953, 2, 82. [Google Scholar] [CrossRef] [Green Version]
- Fauci, A.S. Mechanisms of corticosteroid action on lymphocyte subpopulations. II. Differential effects of in vivo hydrocortisone, prednisone and dexamethasone on in vitro expression of lymphocyte function. Clin. Exp. Immunol. 1976, 24, 54–62. [Google Scholar]
- Cupps, T.R.; Fauci, A.S. Corticosteroid-mediated immunoregulation in man. Immunol. Rev. 1982, 65, 133–155. [Google Scholar] [CrossRef] [PubMed]
- Slade, J.D.; Hepburn, B. Prednisone-induced alterations of circulating human lymphocyte subsets. J. Lab. Clin. Med. 1983, 101, 479–487. [Google Scholar] [PubMed]
- Takiguchi, H.; Chen, V.; Obeidat, M.; Hollander, Z.; FitzGerald, J.M.; McManus, B.M.; Ng, R.T.; Sin, D.D. Effect of short-term oral prednisone therapy on blood gene expression: A randomised controlled clinical trial. Respir. Res. 2019, 20, 176. [Google Scholar] [CrossRef] [Green Version]
- Good, R.A.; Smith, R.T.; Vernier, R.L. Serious untoward reactions to therapy with cortisone and adrenocorticotropin in pediatric practice. I. Pediatrics 1957, 19, 95–118. [Google Scholar]
- Bacon, G.E.; Oliver, W.J.; Shapiro, B.A. Factors contributing to severity of herpes zoster in children. J. Pediatrics 1965, 67, 763–771. [Google Scholar] [CrossRef]
- Haggerty, R.J.; Eley, R.C. Varicella and cortisone. Pediatrics 1956, 18, 160–162. [Google Scholar] [PubMed]
- Wu, C.T.; Tsai, S.C.; Lin, J.J.; Hsia, S.H. Disseminated varicella infection in a child receiving short-term steroids for asthma. Pediatrics Dermatol. 2008, 25, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.C.; Marques, H.H.; Ferriani, M.P.; Gormezano, N.W.; Terreri, M.T.; Pereira, R.M.; Magalhaes, C.S.; Campos, L.M.; Bugni, V.; Okuda, E.M.; et al. Herpes zoster infection in childhood-onset systemic lupus erythematosus patients: A large multicenter study. Lupus 2016, 25, 754–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, S.A.J.; Vestergaard, M.; Baggesen, L.M.; Pedersen, L.; Schonheyder, H.C.; Sorensen, H.T. Prevaccination epidemiology of herpes zoster in Denmark: Quantification of occurrence and risk factors. Vaccine 2017, 35, 5589–5596. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.W.; Chen, Y.H.; Wang, K.H.; Wang, C.Y.; Lin, H.W. Risk of herpes zoster among patients with chronic obstructive pulmonary disease: A population-based study. CMAJ 2011, 183, E275–E280. [Google Scholar] [CrossRef] [Green Version]
- Pappas, D.A.; Hooper, M.M.; Kremer, J.M.; Reed, G.; Shan, Y.; Wenkert, D.; Greenberg, J.D.; Curtis, J.R. Herpes Zoster Reactivation in Patients With Rheumatoid Arthritis: Analysis of Disease Characteristics and Disease-Modifying Antirheumatic Drugs. Arthritis Care Res. 2015, 67, 1671–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamora, L.D.; Collante, M.T.M.; Navarra, S.V. Risk factors for herpes zoster infection among Filipinos with systemic lupus erythematosus. Int. J. Rheum. Dis. 2020, 23, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Kahl, L.E. Herpes zoster infections in systemic lupus erythematosus: Risk factors and outcome. J. Rheumatol. 1994, 21, 84–86. [Google Scholar] [PubMed]
- Choi, W.S. Herpes zoster vaccine in Korea. Clin. Exp. Vaccine Res. 2013, 2, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Harpaz, R.; Leung, J.W. The Epidemiology of Herpes Zoster in the United States During the Era of Varicella and Herpes Zoster Vaccines: Changing Patterns Among Children. Clin. Infect. Dis. 2019, 69, 345–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodley, A.; Swanson, J.; Grose, C.; Bonthius, D.J. Severe Herpes Zoster Following Varicella Vaccination in Immunocompetent Young Children. J. Child Neurol. 2019, 34, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, P.G.; Rovnak, J.; Badani, H.; Cohrs, R.J. A comparison of herpes simplex virus type 1 and varicella-zoster virus latency and reactivation. J. Gen. Virol. 2015, 96 Pt 7, 1581–1602. [Google Scholar] [CrossRef]
- Hope-Simpson, R.E. The Nature of Herpes Zoster: A Long-Term Study and a New Hypothesis. Proc. R. Soc. Med. 1965, 58, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krause, P.R.; Klinman, D.M. Varicella vaccination: Evidence for frequent reactivation of the vaccine strain in healthy children. Nat. Med. 2000, 6, 451–454. [Google Scholar] [CrossRef] [PubMed]
- Mainka, C.; Fuss, B.; Geiger, H.; Hofelmayr, H.; Wolff, M.H. Characterization of viremia at different stages of varicella-zoster virus infection. J. Med. Virol. 1998, 56, 91–98. [Google Scholar] [CrossRef]
- Gershon, M.; Gershon, A. Varicella-Zoster Virus and the Enteric Nervous System. J. Infect. Dis. 2018, 218 (Suppl. 2), S113–S119. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case | Age | Gender | Diagnosis | Steroids | Outcome | Reference |
|---|---|---|---|---|---|---|
| 1 | 13 months | Girl | RAG2 | Yes | Survived | [15] |
| 2 | 13 months | Girl | SCID/ADA | No | Death | [16] |
| 3 | 13 months | Boy | SCID/ADA | Yes | Survived | [17] |
| 4 | 15 months | Girl | Tcell | Yes | Death | [18] |
| 5 | 4 years | Girl | ALL | Probable | Death | [19] |
| 6 | 6 years | Boy | DOCK8 | Yes | Encephalitis | [20] |
| 7 | 6 years | Boy | NKcells | Unknown | Survived | [21] |
| 8 | 11 years | Girl | NKcells | Yes | Death | [22] |
| Case | Age | Gender | Diagnosis | Steroids | Outcome | Reference |
|---|---|---|---|---|---|---|
| 1 | 79 | Male | CLL | No | Death | [32] |
| 2 | 71 | Male | CLL | No | Death | [33] |
| 3 | 70 | Male | RA | Yes | Death | [34] |
| Geography | Age | Condition | Prednisone/Day | Complication | Reference |
|---|---|---|---|---|---|
| England | 11 years | Competent | 20 mg | Disseminated Varicella (WT) | [40] |
| Brazil | Children | Lupus | 20 mg | Herpes Zoster (WT) | [46] |
| Philippines | Adults | Lupus | 20 mg | Herpes Zoster (WT) | [50] |
| USA | Adults | Lupus | 20 mg | Herpes Zoster (WT) | [51] |
| China | 19 years | Lupus | 30 mg | Fatal Dissemination (WT) | [39] |
| USA | Adults | Arthritis | 7.5 mg | Herpes Zoster (WT) | [49] |
| Canada | 70 years | Arthritis | 10 mg | Fatal Dissemination (VAC) | [34] |
| USA | 14 years | Asthma | 20 mg | Meningitis (VAC) | [13] |
| Time Zero: Zostavax | 2 Weeks Later | 4 Weeks Later | 5 Weeks Later |
|---|---|---|---|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Price, N.B.; Grose, C. Corticosteroids Contribute to Serious Adverse Events Following Live Attenuated Varicella Vaccination and Live Attenuated Zoster Vaccination. Vaccines 2021, 9, 23. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010023
Price NB, Grose C. Corticosteroids Contribute to Serious Adverse Events Following Live Attenuated Varicella Vaccination and Live Attenuated Zoster Vaccination. Vaccines. 2021; 9(1):23. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010023
Chicago/Turabian StylePrice, Nathan B., and Charles Grose. 2021. "Corticosteroids Contribute to Serious Adverse Events Following Live Attenuated Varicella Vaccination and Live Attenuated Zoster Vaccination" Vaccines 9, no. 1: 23. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010023