Impact of Recommended Maternal Vaccination Programs on the Clinical Presentation of SARS-CoV-2 Infection: A Prospective Observational Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
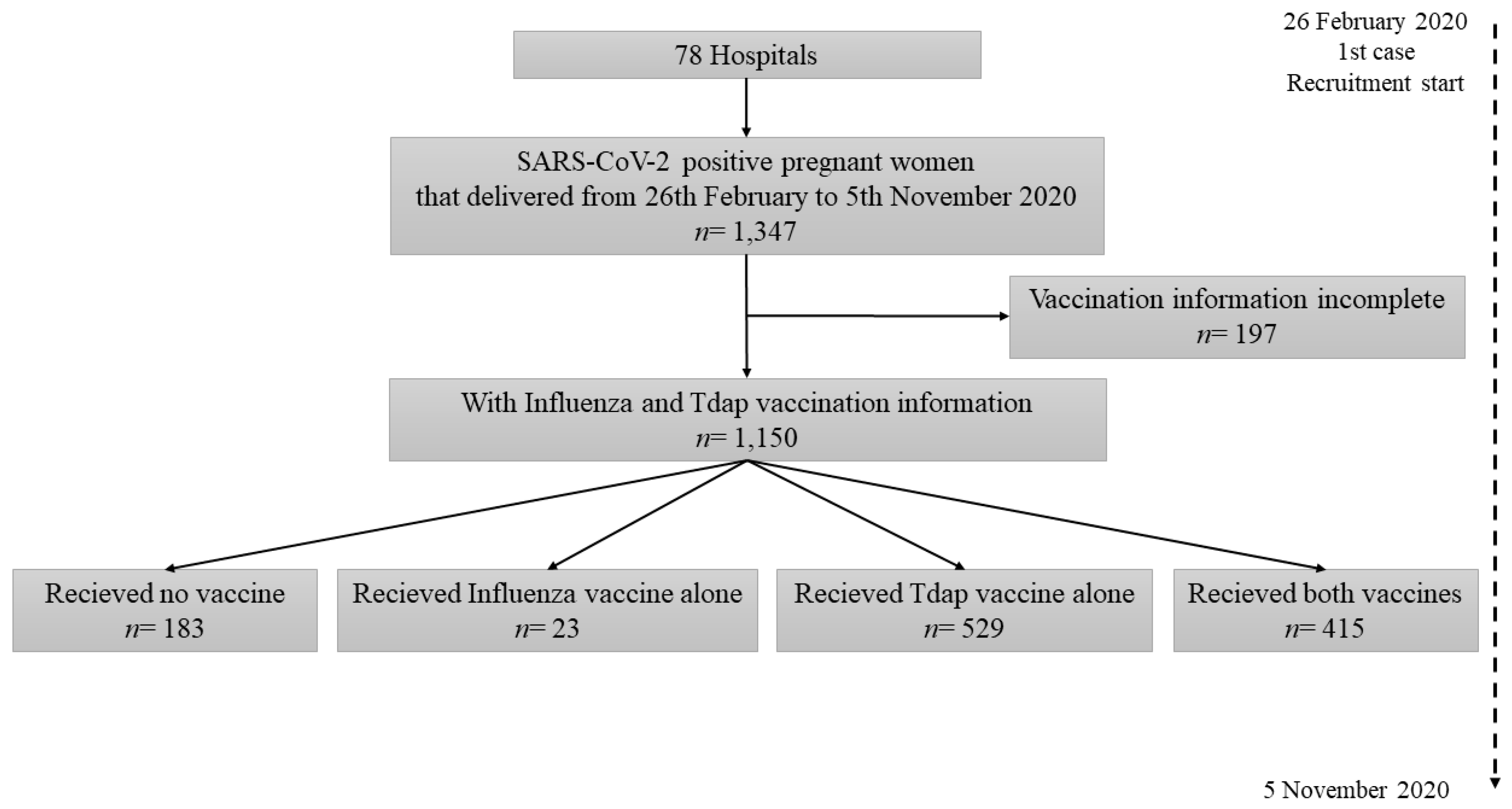
2.1. Infected Cohort
2.2. Statistical Analysis
3. Results
3.1. Description of the Infected Cohort According Their Vaccination
3.2. Clinical Presentation of SARS-CoV-2 Infection According to the Vaccination of Patients
3.3. Baseline Characteristics of Asymptomatic and Symptomatic Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jehi, L.; Ji, X.; Milinovich, A.; Erzurum, S.; Merlino, A.; Gordon, S.; Young, J.B.; Kattan, M.W. Development and validation of a model for individualized prediction of hospitalization risk in 4536 patients with COVID-19. PLoS ONE 2020, 15, e0237419. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Zamora, E.; Trujillo, X.; Huerta, M.; Ríos-Silva, M.; Mendoza-Cano, O. Male gender and kidney illness associated with an increased risk of severe laboratory-confirmed coronavirus disease. BMC Infect. Dis. 2020, 20, 674. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Prado, E.; Simbana-Rivera, K.; Diaz, A.M.; Barreto, A.; Moyano, C.; Arcos, V.; Vasconez-Gonzalez, E.; Paz, C.; Simbana-Guaycha, F.; Molestina-Luzuriaga, M.; et al. Epidemiological, Socio-Demographic and Clinical Features of the Early Phase of the COVID-19 Epidemic in Ecuador. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.05.08.20095943v2 (accessed on 18 May 2020).
- Poblador-Plou, B.; Carmona-Pírez, J.; Ioakeim-Skoufa, I.; Poncel-Falcó, A.; Bliek-Bueno, K.; Cano-Del Pozo, M.; Gimeno-Feliú, L.A.; González-Rubio, F.; Aza-Pascual-Salcedo, M.; Bandrés-Liso, A.C.; et al. Baseline Chronic Comorbidity and Mortality in Laboratory-Confirmed COVID-19 Cases: Results from the PRECOVID Study in Spain. Int. J. Environ. Res. Public Health 2020, 17, 5171. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.; Daubenberger, C.; Brentani, A. Inactivated Trivalent Influenza Vaccine Is Associated with Lower Mortality among Covid-19 Patients in Brazil. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.06.29.20142505v1 (accessed on 1 July 2020).
- Reche, P.A. Potential Cross-Reactive Immunity to SARS-CoV-2 From Common Human Pathogens and Vaccines. Front. Immunol. 2020, 11, 586984. [Google Scholar] [CrossRef]
- Forster, A.S.; Rockliffe, L.; Chorley, A.J.; Marlow, L.A.V.; Bedford, H.; Smith, S.G.; Waller, J. Ethnicity-specific factors influencing childhood immunisation decisions among Black and Asian Minority Ethnic groups in the UK: A systematic review of qualitative research. J. Epidemiol. Community Health 2017, 71, 544–549. [Google Scholar] [CrossRef]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, January 22–June 7, 2020. MMWR Morb. Mortal. Wkly Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef]
- Pardilla, M.B.E.; Aguilar, A.C.; Puig, B.M.; Lorenzana, A.S.; de la Torre, I.R.; de la Manzanara, P.H.L.; Bernardo, A.F.; Pérez, Ó.M. Spanish registry of Covid-19 screening in asymptomatic pregnants. Rev. Esp. Salud. Publica. 2020, 94, e202009092. [Google Scholar]
- Ministerio de Sanidad, Consumo y Bienestar Social, Gobierno de España. Preguntas y Respuestas Sobre la Vacunación Frente a la Gripe 2020–2021. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/programasDeVacunacion/gripe/faq/Preguntas_respuestas_gripe_ciudadanos_2020-2021.htm (accessed on 14 December 2020).
- Ministerio de Sanidad, Servicios Sociales e Igualdad, Gobierno de España. Preguntas y Respuestas sobre la Vacunación de la Tosferina en Embarazadas. Available online: https://www.mscbs.gob.es/ciudadanos/proteccionSalud/vacunaciones/docs/Vacunacion_Tosferina_Embarazadas.pdf (accessed on 14 December 2020).
- WHO. Clinical Management of COVID-19. Interim Guidance 27 May 2020. WHO/2019-nCoV/clinical/2020.5. Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 30 November 2020).
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Soft. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- WHO. Global Vaccine Action Plan 2011–2020; WHO: Geneva, Switzerland, 2013; ISBN 978 92 4 150498 0. [Google Scholar]
- Ministerio de Sanidad, Consumo y Bienestar Social, Gobierno de España. Coberturas de Vacunación, Datos Estadísticos (Actualización Enero 2020). Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/calendario-y-coberturas/coberturas/home.htm (accessed on 2 December 2020).
- Lu, P.J.; O’Halloran, A.; Bryan, L.; Kennedy, E.D.; Ding, H.; Graitcer, S.B.; Santibanez, T.A.; Meghani, A.; Singleton, J.A. Trends in racial/ethnic disparities in influenza vaccination coverage among adults during the 2007-08 through 2011-12 seasons. Am. J. Infect. Control. 2014, 42, 763–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogink, J.; Verelst, F.; Kessels, R.; Jan van Hoek, A.; Timen, A.; Willem, L.; Beutels, P.; Wallinga, J.; de Wit, G.A. Preferential differences in vaccination decision-making for oneself or one’s child in The Netherlands: A discrete choice experiment. BMC Public Health 2020, 20, 828. [Google Scholar] [CrossRef] [PubMed]
- Verelst, F.; Kessels, R.; Delva, W.; Beutels, P.; Willem, L. Drivers of vaccine decision-making in South Africa: A discrete choice experiment. Vaccine 2019, 37, 2079–2089. [Google Scholar] [CrossRef]
- Martínez-Baz, I.; Trobajo-Sanmartín, C.; Arregui, I.; Navascués, A.; Adelantado, M.; Indurain, J.; Fresán, U.; Ezpeleta, C.; Castilla, J. Influenza Vaccination and Risk of SARS-CoV-2 Infection in a Cohort of Health Workers. Vaccines 2020, 8, 611. [Google Scholar] [CrossRef]
- Berg, M.K.; Yu, Q.; Salvador, C.E.; Melani, I.; Kitayama, S. Mandated Bacillus Calmette-Guérin (BCG) Vaccination Predicts Flattened Curves for the Spread of COVID-19. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.04.05.20054163v6 (accessed on 30 December 2020). [CrossRef] [PubMed]
- Miller, A.; Reandelar, M.J.; Fasciglione, K.; Roumenova, V.; Li, Y.; Otazu, G.H. Correlation between Universal BCG Vaccination Policy and Reduced Mortality for COVID-19. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.24.20042937v2 (accessed on 30 December 2020). [CrossRef] [Green Version]
- Netea, M.G.; Joosten, L.A.B.; Latz, E.; Mills, K.H.G.; Natoli, G.; Stunnenberg, H.G.; ONeill, L.A.J.; Xavier, R.J. Trained Immunity: A Program of Innate Immune Memory in Health and Disease. Science 2016, 352, aaf1098. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Huang, H.; Wang, D.; Wang, C.; Wang, Y. Immunological strategies against spike protein: Neutralizing antibodies and vaccine development for COVID-19. Clin. Transl. Med. 2020, 10, e184. [Google Scholar] [CrossRef]
- COVID-19 Real-Time Learning Network. Vaccines in Development (Last Updated: 24 December 2020). Available online: https://www.idsociety.org/covid-19-real-time-learning-network/vaccines/vaccines/ (accessed on 30 December 2020).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; on behalf of the C4591001 Clinical Trial Group. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- How to Protect Yourself and Others. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 30 November 2020).
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef]
- Grohskopf, L.A.; Sokolow, L.Z.; Broder, K.R.; Olsen, S.J.; Karron, R.A.; Jernigan, D.B.; Bresee, J.S. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices–United States, 2016-17 influenza season. MMWR Recomm. Rep. 2016, 65, 1–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poehling, K.A.; Edwards, K.M.; Weinberg, G.A.; Szilagyi, P.; Staat, M.A.; Iwane, M.K.; Bridges, C.B.; Grijalva, C.G.; Zhu, Y.; Bernstein, D.I.; et al. The underrecognized burden of influenza in young children. N. Engl. J. Med. 2006, 355, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doherty, M.; Schmidt-Ott, R.; Santos, J.I.; Stanberry, L.R.; Hofstetter, A.M.; Rosenthal, S.L.; Cunningham, A.L. Vaccination of special populations: Protecting the vulnerable. Vaccine 2016, 34, 6681–6690. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Baseline Characteristics | Total N = 1150 | Vaccination Groups | ||||
|---|---|---|---|---|---|---|
| No Vaccine N = 183 | Influenza Alone N = 23 | Tdap Alone N = 529 | Both Vaccines N = 415 | p-Value | ||
| Maternal Age (Years; Median/IQR) | 33 (28–37) | 32 (26–36) | 33 (26–39) | 33 (28–36) | 33 (29–37) | 0.013 * |
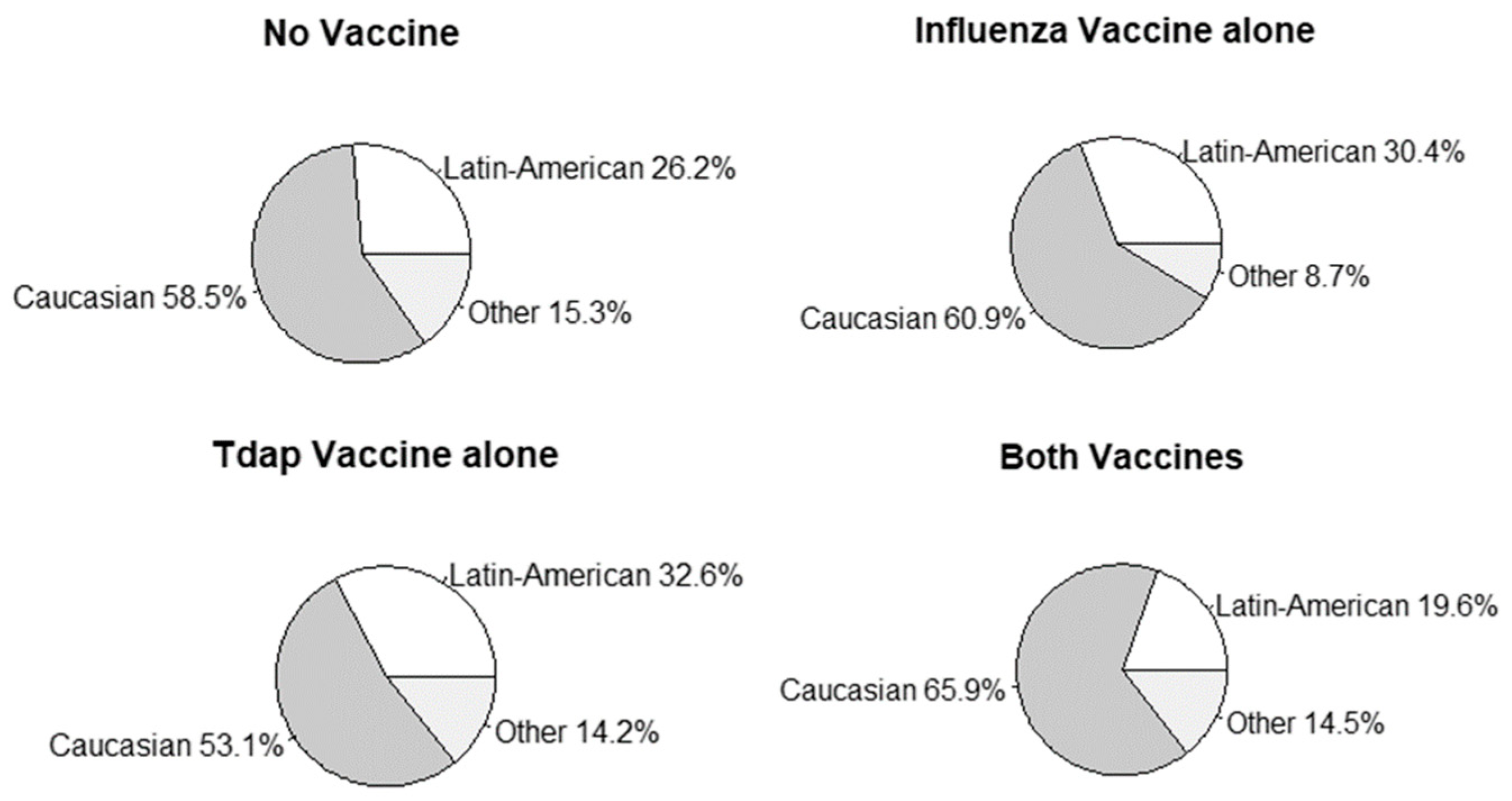
| Ethnicity | 0.001 * | |||||
| Latin-American | 308/1147 (26.9) | 48 (26.2) | 7 (30.4) | 172/527 (32.6) | 81/414 (19.6) | |
| Caucasian | 674/1147 (58.8) | 107 (58.5) | 14 (60.9) | 280/527 (53.1) | 273/414 (65.9) | |
| Other a | 165/1147 (14.4) | 28 (15.3) | 2 (8.7) | 75/527 (14.2) | 60/414 (14.5) | |
| Private hospital | 83 (7.2) | 14 (7.7) | 0 (0.0) | 31 (5.9) | 38 (9.2) | 0.131 |
| Nulliparity | 455 (39.6) | 78 (42.6) | 12 (52.2) | 206 (38.9) | 159 (38.3) | 0.457 |
| Preterm delivery (<37 weeks) | 113/1148 (9.8) | 29 (15.8) | 5 (21.7) | 37 (7.0) | 42/413 (10.2) | 0.001 * |
| In vitro fertilization | 69 (6.0) | 7 (3.8) | 0 (0.0) | 26 (4.9) | 36 (8.7) | 0.025 * |
| Respiratory comorbidities | 44 (3.8) | 8 (4.4) | 4 (17.4) | 17 (3.2) | 15 (3.6) | 0.007 * |
| Chronic lung disease | 3 (0.3) | 1 (0.5) | 0 (0.0) | 1 (0.2) | 1 (0.2) | 0.863 |
| Asthma | 43 (3.7) | 8 (4.4) | 4 (17.4) | 17 (3.2) | 14 (3.4) | 0.005 * |
| Clinical Presentation of SARS-CoV-2 infection | No Vaccine N = 183 | Influenza Alone N = 23 | Tdap Alone N = 529 | Both Vaccines N = 415 | p-Value |
|---|---|---|---|---|---|
| Asymptomatic | 85 (46.4) | 6 (26.1) | 276 (52.2) | 217 (52.3) | 0.051 |
| Symptomatic | 98 (53.6) | 17 (73.9) | 253 (47.8) | 198 (47.7) | |
| Mild-moderate symptoms | 70/98 (71.4) | 10/17 (58.8) | 182/253 (71.9) | 147/198 (74.2) | 0.433 |
| Pneumonia | 22/98 (22.4) | 5/17 (29.4) | 62/253 (24.5) | 46/198 (23.2) | |
| Complicated pneumonia a/shock | 6/98 (6.1) | 2/17 (11.8) | 9/253 (3.6) | 5/198 (2.5) |
| Baseline Characteristics | All Patients N = 1150 | Symptomatic Patients N = 566 | |||||
|---|---|---|---|---|---|---|---|
| Asymptomatic Patients N = 584 | Symptomatic Patients N = 566 | p-Value | Mild–Moderate Symptoms N = 409 | Pneumonia N = 135 | Complicated Pneumonia c/Shock N = 22 | p-Value | |
| Maternal Age (Years; Median/IQR) | 32 (28–36) | 33 (28–37) | 0.153 | 33 (28–37) | 33 (28–37) | 32 (26–38) | 0.848 |
| Ethnicity | <0.001 * | 0.032 * | |||||
| Latin-American | 106/583 (18.2) | 202/564 (35.8) | 131/407 (32.2) | 63 (46.7) | 8 (36.4) | ||
| Caucasian | 375/583 (64.3) | 299/564 (53.0) | 231/407 (56.8) | 56 (41.5) | 12 (54.5) | ||
| Other a | 102/583 (17.5) | 63/564 (11.2) | 45/407 (11.1) | 16 (11.9) | 2 (9.1) | ||
| Private hospital | 58 (9.9) | 25 (4.4) | <0.001 * | 19 (4.6) | 6 (4.4) | 0 (0.0) | 0.586 |
| Nulliparity | 235 (40.2) | 220 (38.9) | 0.635 | 167 (40.8) | 46 (34.1) | 7 (31.8) | 0.297 |
| In vitro fertilization | 31 (5.3) | 38 (6.7) | 0.316 | 30 (7.3) | 5 (3.7) | 3 (13.6) | 0.143 |
| Respiratory comorbidities | 15 (2.6) | 29 (5.1) | 0.024 * | 22 (5.4) | 5 (3.7) | 2 (9.1) | 0.515 |
| Chronic lung disease | 1 (0.2) | 2 (0.4) | 0.619 | 0 (0.0) | 2 (1.5) | 0 (0.0) | 0.041 * |
| Asthma | 15 (2.6) | 28 (4.9) | 0.034 * | 22 (5.4) | 4 (3.0) | 2 (9.1) | 0.351 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Cruz Conty, M.L.; Encinas Pardilla, M.B.; Garcia Sanchez, M.; Gonzalez Rodriguez, L.; Muner-Hernando, M.L.; Royuela Vicente, A.; Pintado Recarte, P.; Martinez Varea, A.; Martinez Diago, C.; Cruz Melguizo, S.; et al. Impact of Recommended Maternal Vaccination Programs on the Clinical Presentation of SARS-CoV-2 Infection: A Prospective Observational Study. Vaccines 2021, 9, 31. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010031
de la Cruz Conty ML, Encinas Pardilla MB, Garcia Sanchez M, Gonzalez Rodriguez L, Muner-Hernando ML, Royuela Vicente A, Pintado Recarte P, Martinez Varea A, Martinez Diago C, Cruz Melguizo S, et al. Impact of Recommended Maternal Vaccination Programs on the Clinical Presentation of SARS-CoV-2 Infection: A Prospective Observational Study. Vaccines. 2021; 9(1):31. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010031
Chicago/Turabian Stylede la Cruz Conty, Maria Luisa, Maria Begoña Encinas Pardilla, Marta Garcia Sanchez, Laura Gonzalez Rodriguez, Marta Luisa Muner-Hernando, Ana Royuela Vicente, Pilar Pintado Recarte, Alicia Martinez Varea, Clara Martinez Diago, Sara Cruz Melguizo, and et al. 2021. "Impact of Recommended Maternal Vaccination Programs on the Clinical Presentation of SARS-CoV-2 Infection: A Prospective Observational Study" Vaccines 9, no. 1: 31. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9010031