
Coverage with Timely Administered Vaccination against Hepatitis B Virus and Its Influence on the Prevalence of HBV Infection in the Regions of Different Endemicity

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Analysis of Hepatitis B Vaccination Coverage in Newborns
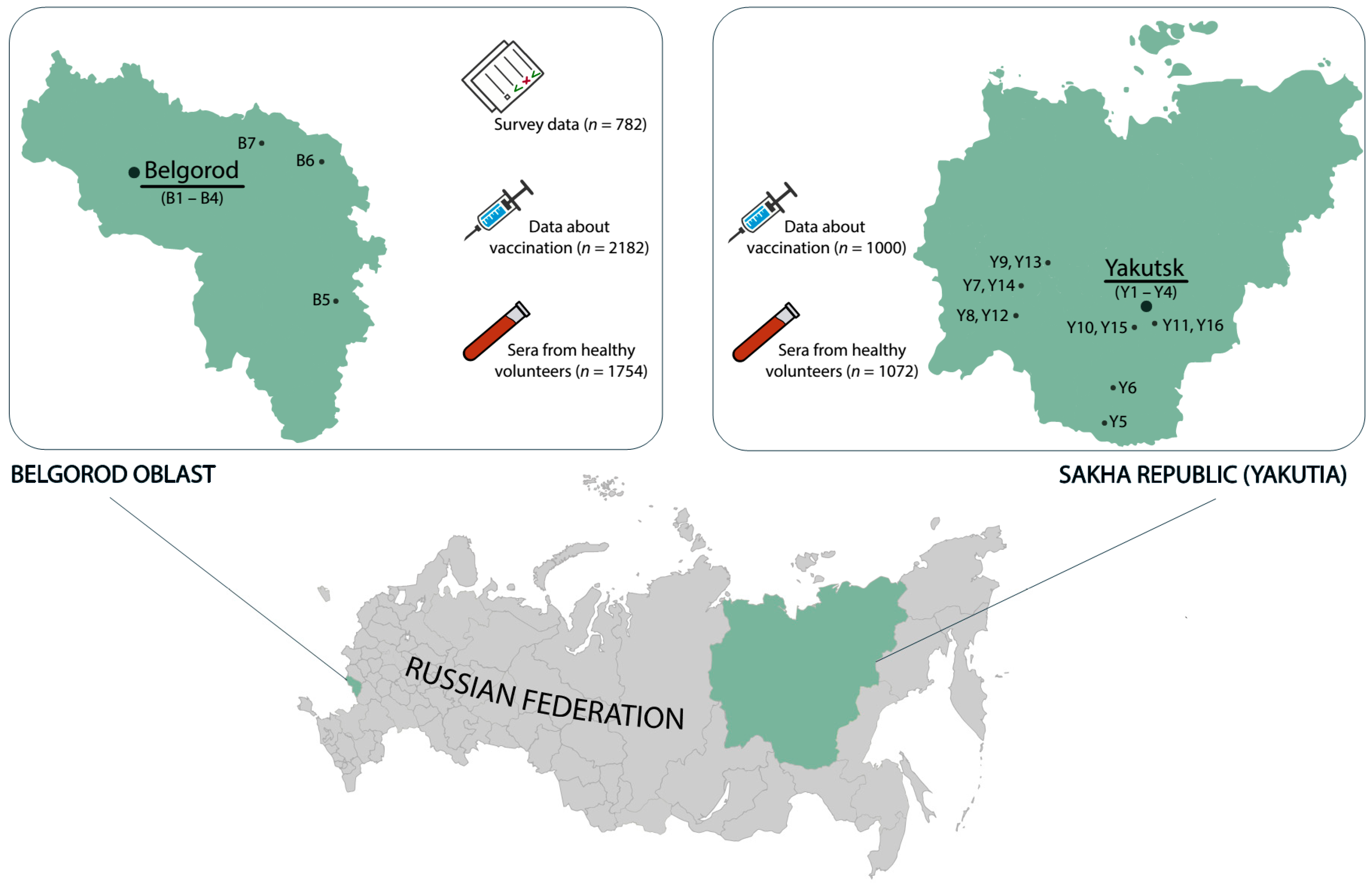
2.2. Serum Samples
2.3. HBV Testing
2.4. Survey of University Students and Teachers on Attitude to Vaccination
2.5. Statistical Analysis
3. Results
3.1. Hepatitis B Vaccination Coverage in Newborns
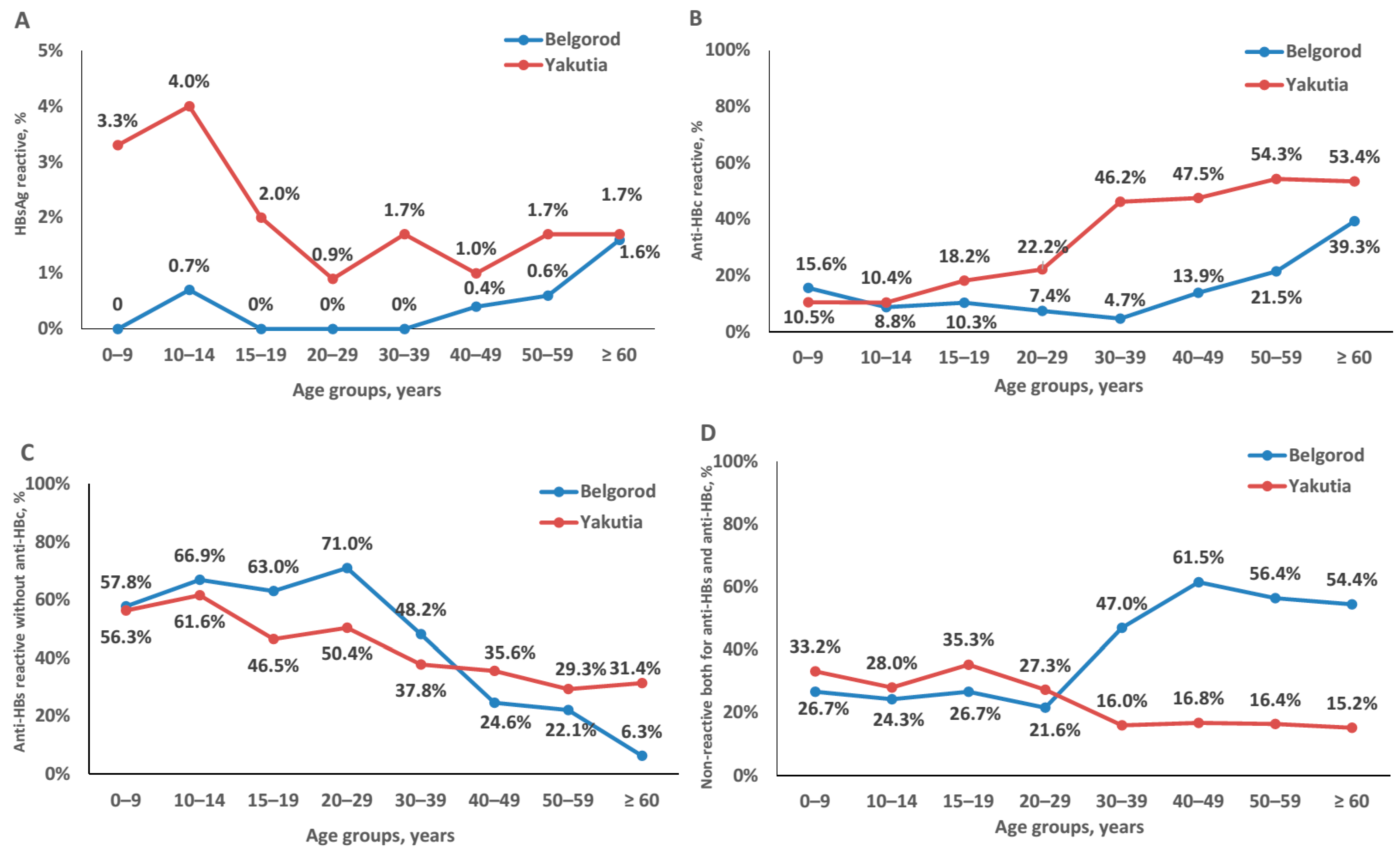
3.2. Prevalence of Hepatitis B Markers in a Conditionally Healthy Population
3.3. Attitude to Vaccination among University Students and Teachers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Hepatitis Report; World Health Organization: Geneva, Switzerland, 2017; Available online: http://apps.who.int/iris/bitstream/10665/255016/1/9789241565455-eng.pdf?ua=1 (accessed on 26 November 2020).
- Valenzuela, P.; Medina, A.; Rutter, W.J.; Ammerer, G.; Hall, B.D. Synthesis and assembly of hepatitis B virus surface antigen particles in yeast. Nature 1982, 298, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Resolution No. 9 dated 03.11.2013 of the Chief Sanitary Doctor of the Russian Federation. Available online: https://www.rospotrebnadzor.ru/documents/details.php?ELEMENT_ID=227 (accessed on 26 November 2020). (In Russian).
- Infectious and Parasitic Diseases Morbidity in Russian Federation; Federal statistical form 1; Federal Center of Hygeine and Epidemiology: Moscow, Russia, 2019. (In Russian)
- WHO Global Health Sector Strategy on Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016; Available online: http://apps.who.int/iris/bitstream/10665/246177/1/WHO-HIV-2016.06-eng.pdf?ua=1 (accessed on 26 November 2020).
- Galina, N.P.; Mindlina, A.Y.; Polibin, R.V. Surveying children and adult vaccination program against diphtheria, tetanus, measles and viral hepatitis B in the Russian Federation. Russ. J. Infect. Immun. 2019, 9, 779–786. (In Russian) [Google Scholar] [CrossRef]
- Alexeeva, M.N.; Grinenko, L.E.; Rafailova, M.A. Viral hepatitis in Sakha Republic (Yakutia). Russ. J. Gastroenterol. Hepatol. Coloproctacol. 1998, 5, 156–159. (In Russian) [Google Scholar]
- Demography Report; Federal State Statistics Service: Moscow, Russia, 2019. Available online: https://rosstat.gov.ru/folder/12781 (accessed on 26 November 2020). (In Russian)
- Bulletin of the Russian Statistics Agency, Moscow, Russia. 2019. Available online: http://www.gks.ru/free_doc/new_site/population/demo/Popul2019.xls (accessed on 26 November 2020).
- Klushkina, V.V.; Kyuregyan, K.K.; Kozhanova, T.V.; Popova, O.E.; Dubrovina, P.G.; Isaeva, O.V.; Gordeychuk, I.V.; Mikhailov, M.I. Impact of universal hepatitis B vaccination on prevalence, infection-associated morbidity and mortality, and circulation of immune escape variants in Russia. PLoS ONE 2016, 11, e0157161. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Sample size estimation in epidemiologic studies. Casp. J. Intern. Med. 2011, 2, 289–298. [Google Scholar]
- Plotkin, S.; Leuridan, E.; Van Damme, P. Hepatitis B and the Need for a Booster Dose. Clin. Infect. Dis. 2011, 53, 68–75. [Google Scholar] [CrossRef]
- van den Ende, C.; Marano, C.; van Ahee, A.; Bunge, E.M.; De Moerlooze, L. The immunogenicity of GSK’s recombinant hepatitis B vaccine in children: A systematic review of 30 years of experience. Expert Rev. Vaccines 2017, 16, 789–809. [Google Scholar] [CrossRef]
- Hepatitis B vaccines: WHO position paper–July 2017. Wkly Epidemiol. Rec. 2017, 92, 369–392.
- Miao, N.; Zheng, H.; Sun, X.; Zhang, G.; Wang, F. Protective effect of vaccinating infants with a 5 µg recombinant yeast-derived hepatitis B vaccine and the need for a booster dose in China. Sci. Rep. 2020, 10, 18155. [Google Scholar] [CrossRef]
- Le, M.H.; Yeo, Y.H.; So, S.; Gane, E.; Cheung, R.C.; Nguyen, M.H. Prevalence of Hepatitis B Vaccination Coverage and Serologic Evidence of Immunity Among US-Born Children and Adolescents From 1999 to 2016. JAMA Netw. Open 2020, 3, e2022388. [Google Scholar] [CrossRef]
- Prevention of Mother-to-Child Transmission of Hepatitis B Virus: Guidelines on Antiviral Prophylaxis in Pregnancy; World Health Organization: Geneva, Switzerland, 2020; Licence: CC BY-NC-SA 3.0 IGO; Available online: https://www.who.int/publications/i/item/978-92-4-000270-8 (accessed on 9 January 2021).
- Russian National Vaccination Schedule. Available online: https://minzdrav.gov.ru/opendata/7707778246-natskalendarprofilakprivivok2015/visual (accessed on 9 January 2021).
- List of Vaccines for the Prevention of Infectious Diseases Registered and Approved for Use in the Russian Federation; Federal Service for Surveillance on Consumer Rights Protection and Human Wellbeing: Moscow, Russia, 2020. Available online: http://www.28.rospotrebnadzor.ru/activity/?p=1145&show_year=2008 (accessed on 26 November 2020). (In Russian)
- Khotova, T.Y.; Snegireva, I.I.; Darmostukova, M.A.; Zatolochina, K.E.; Ozeretskovskiy, N.A.; Shalunova, N.V.; Romanov, B.K. The interchangeability of vaccines against hepatitis B for immunization of adults. Russ. Med. J. 2016, 22, 85–89. (In Russian) [Google Scholar] [CrossRef]
- Hepatitis B Vaccine Recombinant. FS.3.3.1.0026.15; State Pharmacopoeia of the Russian Federation: Moscow, Russia, 2015; Available online: https://nevacert.ru/reestry/pharmacopoeia/fs.3.3.1.0026.15 (accessed on 26 November 2020). (In Russian)
- Galazka, A.; Milstein, J.; Zaffran, M. Thermostability of Vaccine; WHO document WHO/GPV/98. 07; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Diminsky, D.; Moav, N.; Gorecki, M.; Barenholz, Y. Physical, chemical and immunological stability of CHO-derived hepatitis B surface antigen (HBsAg) particles. Vaccine 1999, 18, 3–17. [Google Scholar] [CrossRef]
- Davaalkham, D.; Ojima, T.; Wiersma, S.; Lkhagvasuren, T.; Nymadawa, P.; Uehara, R.; Watanabe, M.; Oki, I.; Nakamura, Y. Administration of hepatitis B vaccine in winter as a significant predictor of the poor effectiveness of vaccination in rural Mongolia: Evidence from a nationwide survey. J. Epidemiol. Commun. Health 2007, 61, 578–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vylka Ravna, Z. “Catching a Child”: Giving birth under nomadic conditions. The methods of pre- and postnatal care of the Nenets mothers and babies. Int. J. Circumpolar Health 2019, 78, 1586275. [Google Scholar] [CrossRef] [Green Version]
- Tharmaphornpilas, P.; Rasdjarmrearnsook, A.O.; Plianpanich, S.; Sa-nguanmoo, P.; Poovorawan, Y. Increased risk of developing chronic HBV infection in infants born to chronically HBV infected mothers as a result of delayed second dose of hepatitis B vaccination. Vaccine 2009, 27, 6110–6115. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Wang, T.; Shao, Z.; Huang, D.; Wang, A.; Guo, Z.; Long, Y.; Zhang, L.; Su, H.; Zhang, Q.; et al. A population-based study examining hepatitis B virus infection and immunization rates in Northwest China. PLoS ONE 2014, 9, e97474. [Google Scholar] [CrossRef] [PubMed]
- Salkic, N.N.; Zildzic, M.; Muminhodzic, K.; Pavlovic-Calic, N.; Zerem, E.; Ahmetagic, S.; Mott-Divkovic, S.; Alibegovic, E. Intrafamilial transmission of hepatitis B in Tuzla region of Bosnia and Herzegovina. Eur. J. Gastroenterol. Hepatol. 2007, 19, 113–118. [Google Scholar] [CrossRef]
- Ivaniushina, V.; Radjef, N.; Alexeeva, M.; Gault, E.; Semenov, S.; Salhi, M.; Kiselev, O.; Dény, P. Hepatitis delta virus genotypes I and II cocirculate in an endemic area of Yakutia, Russia. J. Gen. Virol. 2001, 82 Pt 11, 2709–2718. [Google Scholar] [CrossRef]
- Smith, P.J.; Kennedy, A.M.; Wooten, K.; Gust, D.A.; Pickering, L.K. Association between health care providers’ influence on parents who have concerns about vaccine safety and vaccination coverage. Pediatrics 2006, 118, e1287-92. [Google Scholar] [CrossRef]
- Jiles, R.B.; Daniels, D.; Yusuf, H.R.; McCauley, M.M.; Chu, S.Y. Undervaccination with hepatitis B vaccine: Missed opportunities or choice? Am. J. Prev. Med. 2001, 20 (Suppl. 4), 75–83. [Google Scholar] [CrossRef]
- Okenwa, U.J.; Dairo, M.D.; Uba, B.; Ajumobi, O. Maternal reasons for non-receipt of valid Hepatitis B birth dose among mother-infant pairs attending routine immunization clinics, South-east, Nigeria. Vaccine 2019, 37, 6894–6899. [Google Scholar] [CrossRef] [PubMed]
- Thanh Thi Le, X.; Ishizumi, A.; Thi Thu Nguyen, H.; Thi Duong, H.; Thi Thanh Dang, H.; Manh Do, C.; Thi Pham, Q.; Thi Le, H.; Iijima, M.; Tohme, R.A.; et al. Social and behavioral determinants of attitudes towards and practices of hepatitis B vaccine birth dose in Vietnam. Vaccine 2020, 38, 8343–8350. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Region | Clinic ID | Total Number of Children | Children Who Received HepB-BD | Children Who Received HepB-2nd at 4–6 Weeks | Children Who Received HepB3 before Age 1 Year | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Belgorod Oblast | B1 | 100 | 94 | 94.0 | 51 | 51.0 | 99 | 99.0 |
| B2 | 100 | 98 | 98.0 | 90 | 90.0 | 98 | 98.0 | |
| B3 | 100 | 93 | 93.0 | 67 | 67.0 | 93 | 93.0 | |
| B4 | 300 | 287 | 95.7 | 165 | 55.0 | 273 | 91.0 | |
| B5 | 100 | 98 | 98.0 | 54 | 54.0 | 98 | 98.0 | |
| B6 * | 150 | 99 | 66.0 | 25 | 16.3 | 121 | 80.7 | |
| B7 | 50 | 42 | 86.0 | 35 | 70.0 | 43 | 86.0 | |
| B8 | 100 | 83 | 83.0 | 67 | 67.0 | 86 | 86.0 | |
| Total | 1000 | 894 | 89.4 | 554 | 55.4 | 911 | 91.1 | |
| Yakutia | Y1 | 140 | 140 | 100 | 62 | 44.3 | 122 | 87.1 |
| Y2 | 208 | 205 | 98.6 | 83 | 39.9 | 187 | 89.9 | |
| Y3 | 100 | 99 | 99.0 | 46 | 46.0 | 89 | 89.0 | |
| Y4 | 363 | 359 | 98.9 | 218 | 60.1 | 324 | 89.3 | |
| Y5 | 100 | 93 | 93.0 | 46 | 46.0 | 95 | 95.0 | |
| Y6 | 100 | 100 | 100 | 54 | 54.0 | 97 | 97.0 | |
| Y7 | 100 | 100 | 100 | 72 | 72.0 | 96 | 96.0 | |
| Y8 | 100 | 100 | 100 | 86 | 86.0 | 96 | 96.0 | |
| Y9 | 104 | 104 | 100 | 79 | 76.0 | 100 | 96.2 | |
| Y10 | 148 | 148 | 100 | 108 | 73.0 | 133 | 89.9 | |
| Y11 | 100 | 100 | 100 | 82 | 82.0 | 100 | 100 | |
| Y12 | 100 | 100 | 100 | 80 | 80.0 | 89 | 89.0 | |
| Y13 | 106 | 106 | 100 | 79 | 74.5 | 100 | 94.3 | |
| Y14 | 100 | 99 | 99.0 | 63 | 63.0 | 93 | 93.0 | |
| Y15 | 213 | 212 | 99.5 | 159 | 74.6 | 189 | 88.7 | |
| Y16 | 100 | 100 | 100 | 95 | 95.0 | 98 | 98.0 | |
| Total | 2182 | 2165 | 99.2 | 1412 | 64.7 | 2008 | 92.0 | |
| Region | Type of Medical Center | Total Number of Children | Children Who Received HepB-BD | Children Who Received HepB-2nd at 4–6 Weeks | Children Who Received HepB3 before Age 1 Year | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Belgorod Oblast | City | 600 | 572 | 95.3 | 373 | 62.1 | 563 | 93.8 |
| Town | 400 | 322 | 80.5 | 181 | 45.2 | 348 | 87.0 | |
| Yakutia | City | 811 | 803 | 99.0 | 409 | 50.4 | 722 | 89.0 |
| Town | 752 | 745 | 99.1 | 527 | 70.1 | 717 | 95.3 | |
| Rural | 619 | 617 | 99.7 | 476 | 76.9 | 569 | 91.9 | |
| Questions | Medical Specialties | Non-Medical Specialties | ||
|---|---|---|---|---|
| n/N * | % | n/N * | % | |
| 1. Named vaccination among possible ways to prevent dangerous infections | 126/156 | 80.8% | 446/626 | 71.2% |
| 2. Do you know what vaccination is? Answered “Yes” | 150/156 | 96.2% | 468/626 | 74.8% |
| 3. Named hepatitis B as one of the infections prevented by vaccination (respondents were not prompted with a list of possible answers) | 71/156 | 45.5% | 164/626 | 26.1% |
| 4. Knew that hepatitis B can be prevented by vaccination (targeted refinement to those who did not mention HBV in response to Question #3). Answered “Yes” | 51/85 | 60.0% | 236/462 | 51.1% |
| 5. Heard about the National Vaccination Schedule. Answered ”Yes” | 87/156 | 55.8% | 229/626 | 36.6% |
| 6. Vaccination fears (multiple answer choices. a list of possible answers was read out) | ||||
| a. Have no fears about vaccination | 59/156 | 37.8% | 196/626 | 31.3% |
| b. Children receive too many vaccines in the first two years of life | 12/156 | 7.7% | 62/626 | 9.9% |
| c. Vaccines can cause side effects or complications | 84/156 | 53.8% | 370/626 | 59.1% |
| d. Vaccines can weaken the immune system of children and adults | 42/156 | 26.9% | 235/626 | 37.5% |
| e. Vaccines can cause disease | 31/156 | 19.9% | 155/626 | 24.8% |
| f. The ingredients in vaccines are unsafe | 12/156 | 7.7% | 83/626 | 13.3% |
| g. The long-term effects of vaccines on humans have not been studied | 10/156 | 6.4% | 72/626 | 11.5% |
| h. Vaccination is against my religious beliefs | 1/156 | 0.6% | 7/626 | 1.1% |
| j. The quality of vaccines is low | 4/156 | 2.6% | 46/626 | 7.3% |
| k. Other | 5/156 | 3.2% | 21/626 | 3.4% |
| 7. Have you or your relatives/acquaintances encountered illness/medical complications in children caused by vaccination? Answered “Yes” | 61/156 | 39.1% | 224/626 | 35.8% |
| 8. Have you or your relatives/acquaintances encountered serious illness that could have been prevented by vaccination? Answered “Yes” | 21/156 | 13.5% | 94/626 | 15.0% |
| 9. There are people/groups of people who refuse to vaccinate themselves and their children. How do you feel about their decision? | ||||
| a. I disagree. They risk the health of their children and contribute to the spread of disease | 78/155 | 50.3% | 189/617 | 30.6% |
| b. I do not care. They are entitled to their opinion | 65/155 | 41.9% | 354/617 | 57.4% |
| c. I agree with them | 10/155 | 6.5% | 62/617 | 10.0% |
| d. I haven’t heard anything about this | 2/155 | 1.3% | 6/617 | 1.0% |
| e. Other | 0 | 0.0% | 6/617 | 1.0% |
| 10. Do you trust healthcare providers who vaccinate? (Choose one answer from the list) | ||||
| a. I completely trust them | 53/156 | 34.0% | 180/623 | 28.9% |
| b. I mostly trust them | 79/156 | 50.6% | 310/623 | 49.8% |
| c. No opinion | 9/156 | 5.8% | 37/623 | 5.9% |
| d. I mostly do not trust them | 12/156 | 7.7% | 81/623 | 13.0% |
| e. I do not trust them at all | 3/156 | 1.9% | 15/623 | 2.4% |
| 11. Do you trust the quality of vaccines? (Choose one answer from the list) | ||||
| a. I completely trust the quality of vaccines | 39/156 | 25.0% | 129/619 | 20.8% |
| b. I mostly trust the quality of vaccines | 74/156 | 47.4% | 265/619 | 42.8% |
| c. No opinion | 24/156 | 15.4% | 96/619 | 15.5% |
| d. I mostly do not trust the quality of vaccines | 14/156 | 9.0% | 106/619 | 17.1% |
| e. I do not trust the quality of vaccines at all | 5/156 | 3.2% | 23/619 | 3.7% |
| 12. What information about vaccinations would you like to receive? (Choose any answers from the list) | ||||
| a. Information about the usefulness and benefits of vaccination | 97/156 | 62.2% | 421/626 | 67.3% |
| b. Information about additional vaccines | 81/156 | 51.9% | 268/626 | 42.8% |
| c. Information about vaccine composition | 89/156 | 57.1% | 347/626 | 55.4% |
| d. Information about contraindications to vaccination | 110/156 | 70.5% | 483/626 | 77.2% |
| e. Information about complications after vaccination | 107/156 | 68.6% | 488/626 | 78.0% |
| f. Information about the manufacturers of vaccines | 51/156 | 32.7% | 269/626 | 43.0% |
| g. Other | 1/156 | 0.6% | 9/626 | 1.4% |
| h. I have enough information | 17/156 | 10.9% | 45/626 | 7.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyuregyan, K.K.; Kichatova, V.S.; Isaeva, O.V.; Potemkin, I.A.; Malinnikova, E.Y.; Lopatukhina, M.A.; Karlsen, A.A.; Asadi Mobarhan, F.A.; Mullin, E.V.; Slukinova, O.S.; et al. Coverage with Timely Administered Vaccination against Hepatitis B Virus and Its Influence on the Prevalence of HBV Infection in the Regions of Different Endemicity. Vaccines 2021, 9, 82. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9020082
Kyuregyan KK, Kichatova VS, Isaeva OV, Potemkin IA, Malinnikova EY, Lopatukhina MA, Karlsen AA, Asadi Mobarhan FA, Mullin EV, Slukinova OS, et al. Coverage with Timely Administered Vaccination against Hepatitis B Virus and Its Influence on the Prevalence of HBV Infection in the Regions of Different Endemicity. Vaccines. 2021; 9(2):82. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9020082
Chicago/Turabian StyleKyuregyan, Karen K., Vera S. Kichatova, Olga V. Isaeva, Ilya A. Potemkin, Elena Yu. Malinnikova, Maria A. Lopatukhina, Anastasia A. Karlsen, Fedor A. Asadi Mobarhan, Eugeniy V. Mullin, Olga S. Slukinova, and et al. 2021. "Coverage with Timely Administered Vaccination against Hepatitis B Virus and Its Influence on the Prevalence of HBV Infection in the Regions of Different Endemicity" Vaccines 9, no. 2: 82. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9020082