Initial Experience with the Safe Implementation of Transanal Total Mesorectal Excision (TaTME) as a Standardized Procedure for Low Rectal Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
- Patient data: sex, date of birth;
- Pre-operative information: tumor staging (CT/MRI), previous treatments (e.g., neoadjuvant treatment);
- Surgery specific data;
- Post-operative course;
- Long-term follow-up data (Complications—Clavien–Dindo; readmissions);
- Histopathological and oncological outcomes.
2.2. Surgical Technique
2.3. Abdominal Procedure
2.4. Transanal Phase
2.4.1. Prepping of the Transanal Access
2.4.2. Transanal Resection
2.5. Patients
2.6. Statistical analysis
3. Results
3.1. Intraoperative Data
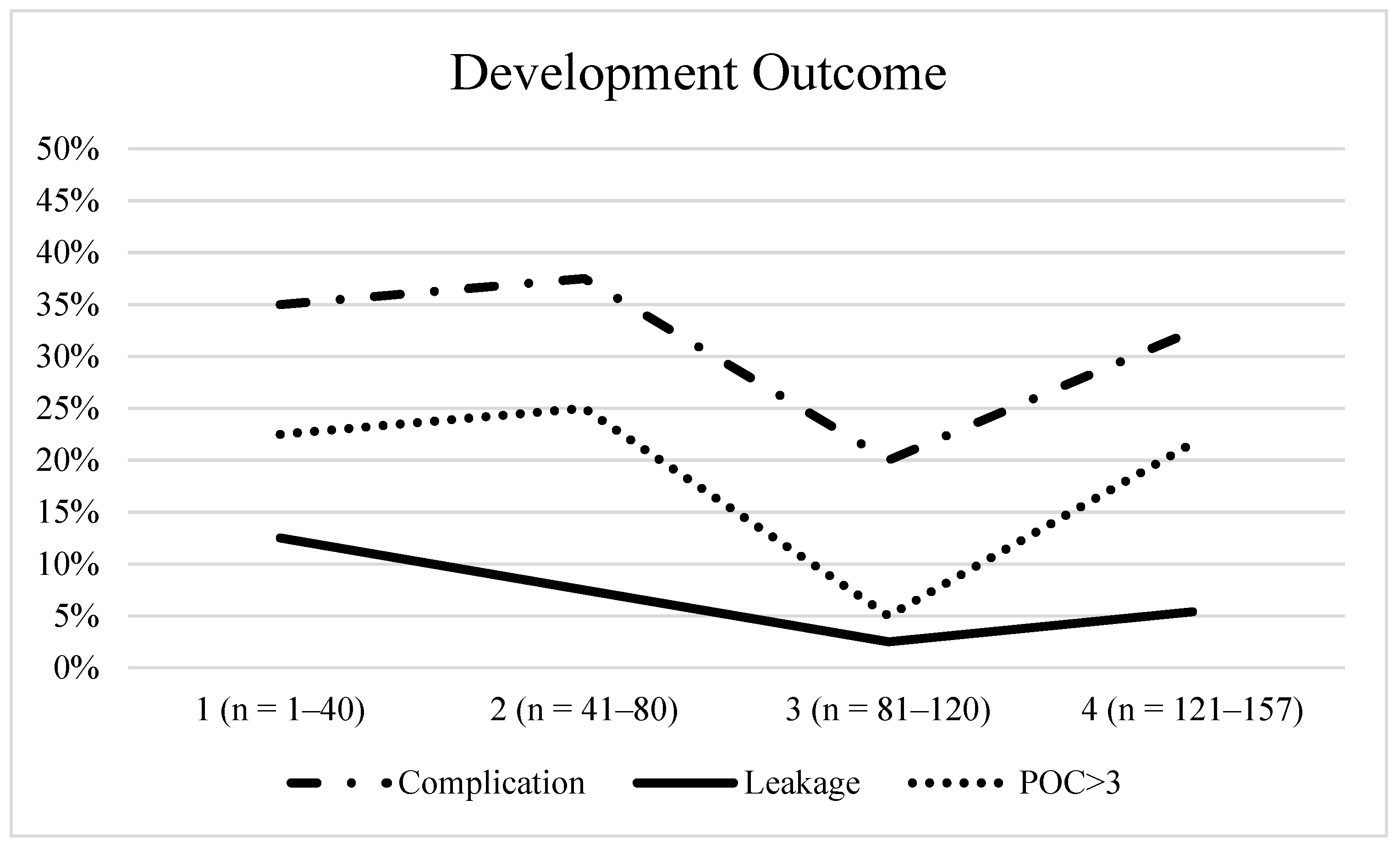
3.2. Postoperative Outcome
3.3. Histopathological Outcome
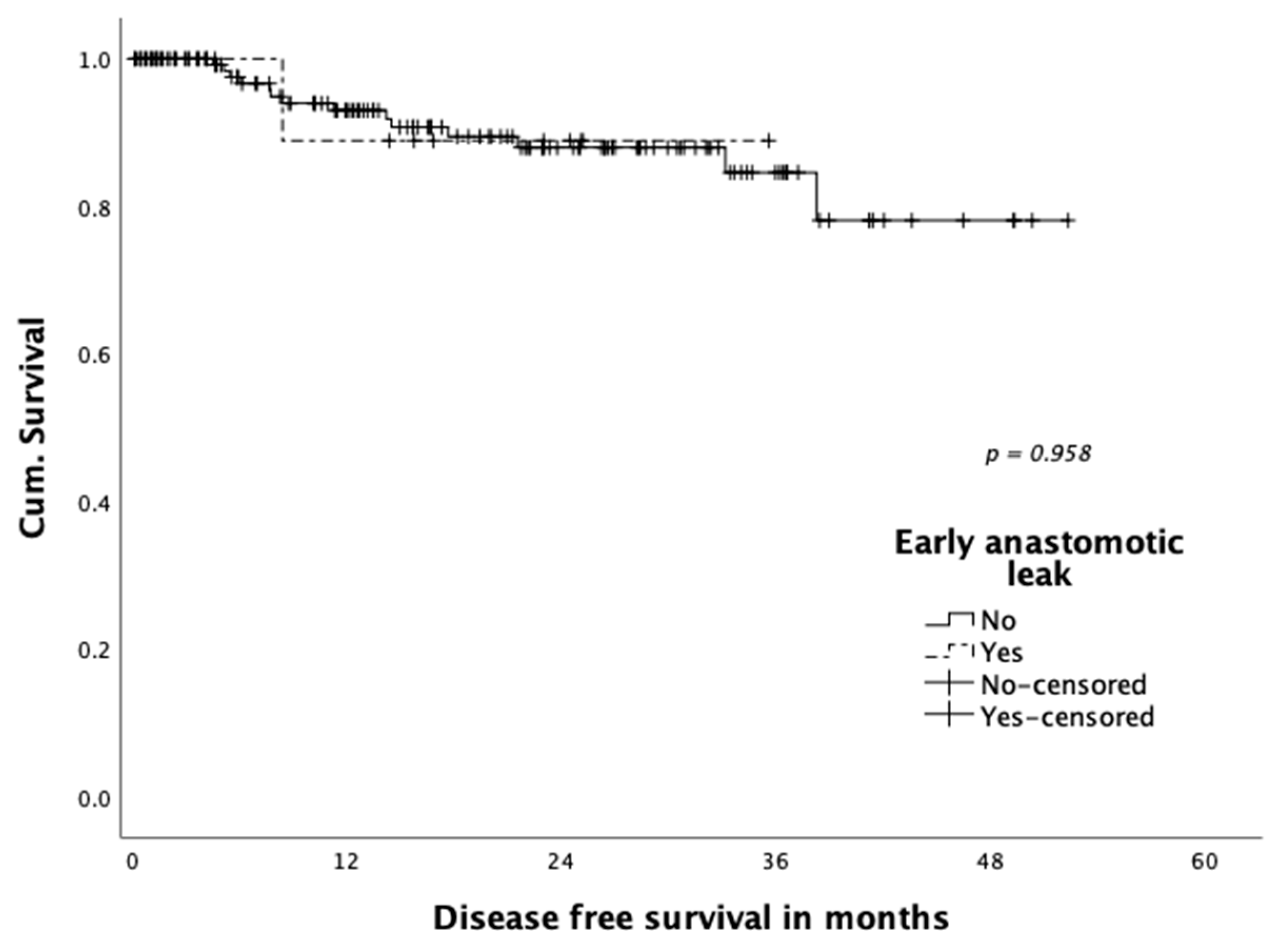
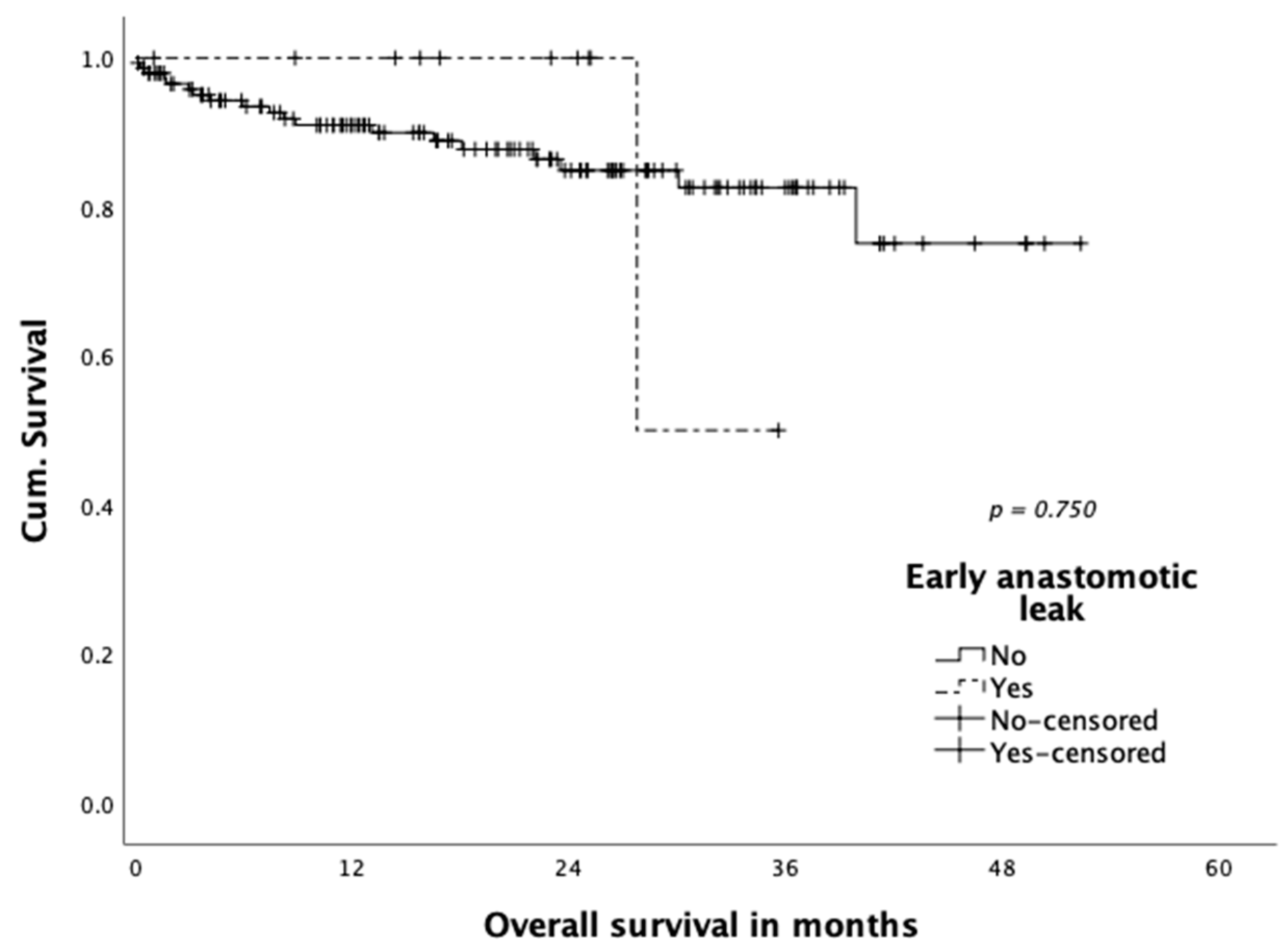
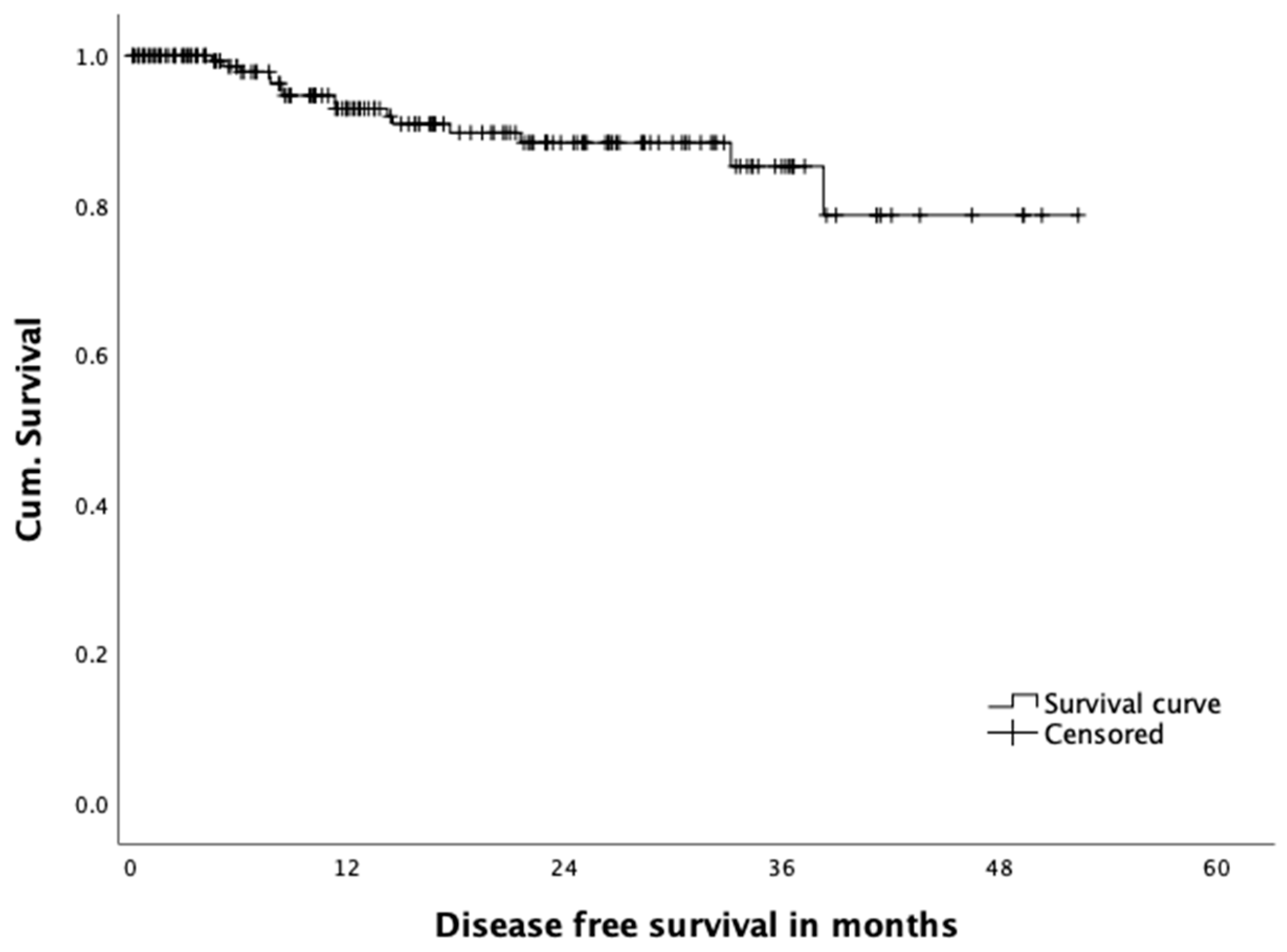
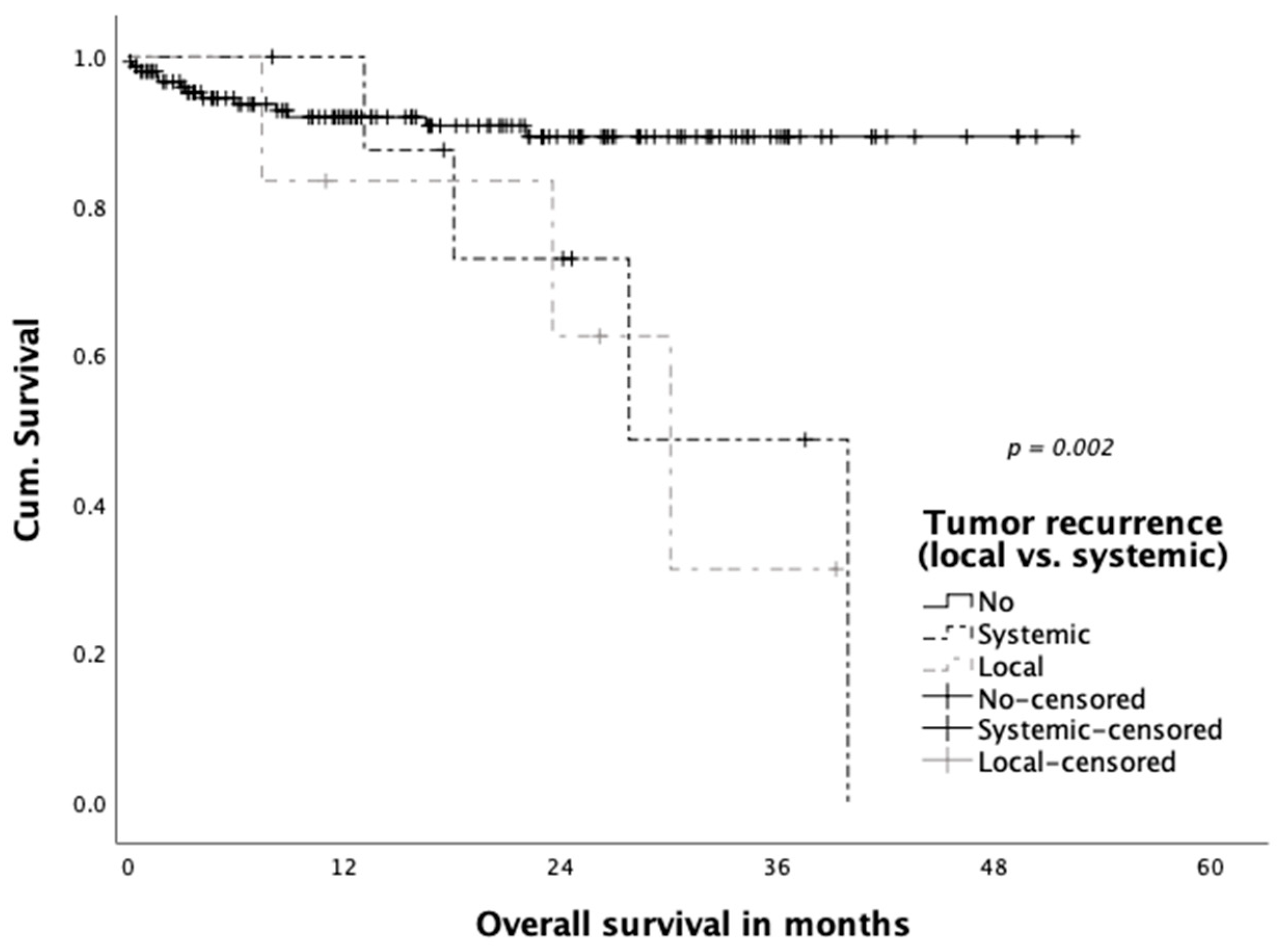
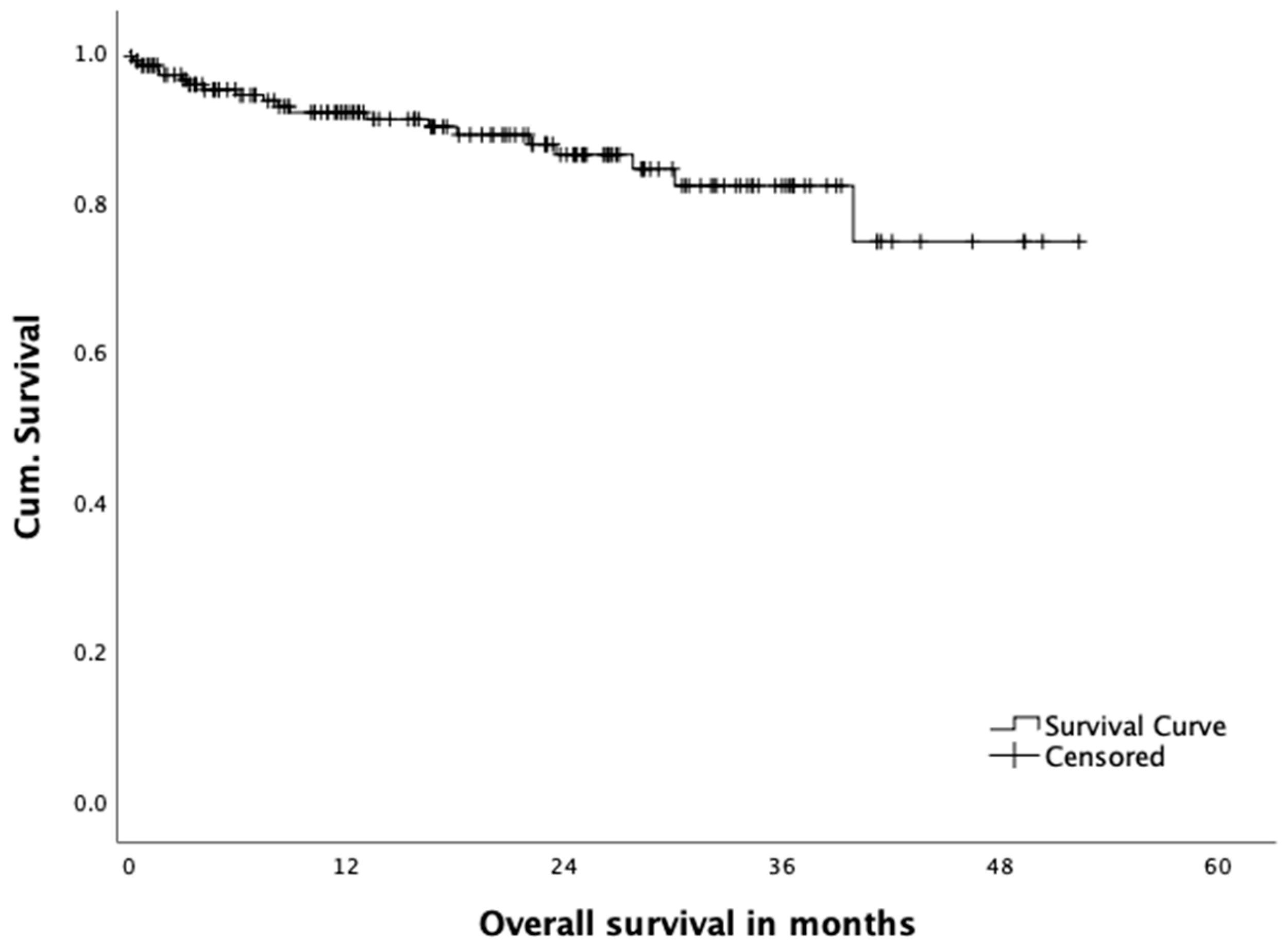
3.4. Oncological Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Cancer Observatory; International Agency for Research on Cancer by WHO. Colorectal Cancer [Internet]. 2018. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf (accessed on 11 March 2020).
- Heald, R.J.; Husband, E.M.; Ryall, R.D. The mesorectum in rectal cancer surgery--the clue to pelvic recurrence? Br. J. Surg. 1982, 69, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Quirke, P.; Steele, R.; Monson, J.; Grieve, R.; Khanna, S.; Couture, J.; O’Callaghan, C.; Myint, A.; Bessell, E.; Thompson, L.; et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: A prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet 2009, 373, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Martling, A.; Singnomklao, T.; Holm, T.; Rutqvist, L.E.; Cedermark, B. Prognostic significance of both surgical and pathological assessment of curative resection for rectal cancer. Br. J. Surg. 2004, 91, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Leonard, D.; Remue, C.; Abbes Orabi, N.; van Maanen, A.; Danse, E.; Dragean, A.; Debentancour, D.; Humblet, Y.; Jouret-Mourin, A.; Maddalena, F.; et al. Lymph node ratio and surgical quality are strong prognostic factors of rectal cancer: Results from a single referral centre. Colorectal Dis. 2016, 18, O175–O184. [Google Scholar] [CrossRef]
- Breukink, S.; Pierie, J.; Wiggers, T. Laparoscopic versus open total mesorectal excision for rectal cancer. Cochrane Database Syst Rev. 2006, 4, CD005200. [Google Scholar]
- Kang, S.-B.; Park, J.W.; Jeong, S.-Y.; Nam, B.H.; Choi, H.S.; Kim, D.-W.; Lim, S.-B.; Lee, T.-G.; Kim, D.Y.; Kim, J.-S.; et al. Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): Short-term outcomes of an open-label randomised controlled trial. Lancet Oncol. 2010, 11, 637–645. [Google Scholar] [CrossRef]
- Bonjer, H.J.; Deijen, C.L.; Abis, G.A.; Cuesta, M.A.; van der Pas, M.H.G.M.; de Lange-de Klerk, E.S.M.; Lacy, A.M.; Bemelman, W.A.; Andersson, J.; Angenete, E.; et al. A randomized trial of laparoscopic versus open surgery for rectal cancer. N. Engl. J. Med. 2015, 372, 1324–1332. [Google Scholar] [CrossRef] [Green Version]
- Rickles, A.S.; Dietz, D.W.; Chang, G.J.; Wexner, S.D.; Berho, M.E.; Remzi, F.H.; Greene, F.L.; Fleshman, J.W.; Abbas, M.A.; Peters, W.; et al. High Rate of Positive Circumferential Resection Margins Following Rectal Cancer Surgery. Ann. Surg. 2015, 262, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Roodbeen, S.X.; Spinelli, A.; Bemelman, W.A.; Di Candido, F.; Cardepont, M.; Denost, Q.; D’Hoore, A.; Houben, B.; Knol, J.J.; Martín-Pérez, B.; et al. Local Recurrence After Transanal Total Mesorectal Excision for Rectal Cancer: A Multicenter Cohort Study. Ann Surg. 2020. [Google Scholar] [CrossRef]
- Muratore, A.; Mellano, A.; Marsanic, P.; De Simone, M. Transanal total mesorectal excision (taTME) for cancer located in the lower rectum: Short- and mid-term results. Eur. J. Surg. Oncol. 2015, 41, 478–483. [Google Scholar] [CrossRef]
- Perdawood, S.K.; Kroeigaard, J.; Eriksen, M.; Mortensen, P. Transanal total mesorectal excision: The Slagelse experience 2013–2019. Surg. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Perdawood, S.K.; Thinggaard, B.S.; Bjoern, M.X. Effect of transanal total mesorectal excision for rectal cancer: Comparison of short-term outcomes with laparoscopic and open surgeries. Surg. Endosc. 2018, 32, 2312–2321. [Google Scholar] [CrossRef] [PubMed]
- Hajibandeh, S.; Hajibandeh, S.; Eltair, M.; George, A.T.; Thumbe, V.; Torrance, A.W.; Budhoo, M.; Joy, H.; Peravali, R. Meta-analysis of transanal total mesorectal excision versus laparoscopic total mesorectal excision in management of rectal cancer. Int. J. Colorectal Dis. 2020, 35, 575–593. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.G.; Pfeffer, F.; Korner, H. Norwegian moratorium on transanal total mesorectal excision. Br. J. Surg. 2019, 106, 1120–1121. [Google Scholar] [CrossRef]
- Hol, J.C.; van Oostendorp, S.E.; Tuynman, J.B.; Sietses, C. Long-term oncological results after transanal total mesorectal excision for rectal carcinoma. Technol. Coloproctol. 2019, 23, 903–911. [Google Scholar] [CrossRef] [Green Version]
- Zorron, R.; Phillips, H.N.; Coelho, D.; Flach, L.; Lemos, F.B.; Vassallo, R.C. Perirectal NOTES access: “down-to-up” total mesorectal excision for rectal cancer. Surg. Innov. 2012, 19, 11–19. [Google Scholar] [CrossRef]
- De Simone, V.; Persiani, R.; Biondi, A.; Litta, F.; Parello, A.; Campennì, P.; Orefice, R.; Marra, A.; Costa, A.; D’Ugo, D.; et al. One-year evaluation of anorectal functionality and quality of life in patients affected by mid-to-low rectal cancer treated with transanal total mesorectal excision. Updates Surg. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Filips, A.; Haltmeier, T.; Kohler, A.; Candinas, D.; Brügger, L.; Studer, P. LARS is Associated with Lower Anastomoses, but not with the Transanal Approach in Patients Undergoing Rectal Cancer Resection. World J. Surg. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- van der Heijden, J.A.G.; Koëter, T.; Smits, L.J.H.; Sietses, C.; Tuynman, J.B.; Maaskant-Braat, A.J.G.; Klarenbeek, B.R.; de Wilt, J.H.W. Functional complaints and quality of life after transanal total mesorectal excision: A meta-analysis. Br. J. Surg. 2020, 107, 489–498. [Google Scholar] [CrossRef]
- Deijen, C.L.; Velthuis, S.; Tsai, A.; Mavroveli, S.; de Lange-de Klerk, E.S.M.; Sietses, C.; Tuynman, J.B.; Lacy, A.M.; Hanna, G.B.; Bonjer, H.J.; et al. COLOR III: A multicentre randomised clinical trial comparing transanal TME versus laparoscopic TME for mid and low rectal cancer. Surg. Endosc. 2016, 30, 3210–3215. [Google Scholar] [CrossRef] [Green Version]
- Lelong, B.; de Chaisemartin, C.; Meillat, H.; Cournier, S.; Boher, J.M.; Genre, D.; Karoui, M.; Tuech, J.J.; Delpero, J.R.; French Research Group of Rectal Cancer Surgery (GRECCAR). A multicentre randomised controlled trial to evaluate the efficacy, morbidity and functional outcome of endoscopic transanal proctectomy versus laparoscopic proctectomy for low-lying rectal cancer (ETAP-GRECCAR 11 TRIAL): Rationale and design. BMC Cancer 2017, 17, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simillis, C.; Lal, N.; Thoukididou, S.N.; Kontovounisios, C.; Smith, J.J.; Hompes, R.; Adamina, M.; Tekkis, P.P. Open Versus Laparoscopic Versus Robotic Versus Transanal Mesorectal Excision for Rectal Cancer. Ann. Surg. 2019, 270, 59–68. [Google Scholar] [CrossRef]
- Kang, L.; Chen, Y.-G.; Zhang, H.; Zhang, H.-Y.; Lin, G.-L.; Yang, Y.-C.; Chen, W.-H.; Luo, S.-L.; Chen, N.; Tong, W.-D.; et al. Transanal total mesorectal excision for rectal cancer: A multicentric cohort study. Gastroenterol. Rep. 2020, 8, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Oostendorp, S.E.; Belgers, H.J.; Bootsma, B.T.; Hol, J.C.; Belt, E.J.T.H.; Bleeker, W.; Den Boer, F.C.; Demirkiran, A.; Dunker, M.S.; Fabry, H.F.J.; et al. Locoregional recurrences after transanal total mesorectal excision of rectal cancer during implementation. Br. J. Surg. 2020, 107, 1211–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simo, V.; Tejedor, P.; Jimenez, L.M.; Hernan, C.; Zorilla, J.; Arrredondo, J. Oncological safety of transanal total mesorectal excision (TaTME) for rectal cancer: Mid-term results of a prospective multicentre study. Surg. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fleshman, J.; Branda, M.E.; Sargent, D.J.; Boller, A.M.; George, V.V.; Abbas, M.A.; Peters, W.R.; Maun, D.C.; Chang, G.J.; Herline, A.; et al. Disease-free Survival and Local Recurrence for Laparoscopic Resection Compared With Open Resection of Stage II to III Rectal Cancer. Ann. Surg. 2019, 269, 589–595. [Google Scholar] [CrossRef] [PubMed]
- TaTME. Available online: https://tatme.medicaldata.eu (accessed on 30 November 2020).
- Adamina, M.; Buchs, N.C.; Penna, M.; Hompes, R. St. Gallen consensus on safe implementation of transanal total mesorectal excision. Surg. Endosc. 2018, 32, 1091–1103. [Google Scholar] [CrossRef] [Green Version]
- Francis, N.; Penna, M.; Mackenzie, H.; Carter, F.; Hompes, R. Consensus on structured training curriculum for transanal total mesorectal excision (TaTME). Surg. Endosc. 2017, 31, 2711–2719. [Google Scholar] [CrossRef]
- Hompes, R.; Adamina, M.; Aigner, F.; Araujo, S.; Arezzo, A.; Ashamalla, S.; de-Beche Adams, T.; Bell, S.; Bemelman, W.; Brown, C.; et al. International expert consensus guidance on indications, implementation and quality measures for transanal total mesorectal excision. Colorectal Dis. 2020, 22, 749–755. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (y); mean ± SD | 60.6 ± 12.4 |
| Sex; n (%) | |
| Male | 117 (74.5) |
| Female | 40 (25.5) |
| BMI (kg/m2); mean ± SD | 26.2 ± 5.0 |
| ASA classification; n (%) | |
| ASA 1 | 14 (8.9) |
| ASA 2 | 104 (66.2) |
| ASA 3 | 35 (22.3) |
| ASA 4 | 4 (2.5) |
| Tumor height AV (cm); mean ± SD | 6.1 ± 2.3 |
| Tumor height AV; n (%) | |
| >6cm | 64 (40.8) |
| ≤6cm | 93 (59.2) |
| Neoadjuvant treatment; n (%) | |
| Yes | 114 (72.6) |
| No | 43 (27.4) |
| Preoperative T stage; n (%) | |
| mrT0 | 1 (0.6) |
| mrT1 | 5 (3.2) |
| mrT2 | 36 (22.9) |
| mrT3 | 100 (63.6) |
| mrT4 | 7 (4.5) |
| mrTx | 8 (5.1) |
| Preoperative N stage; n (%) | |
| mrN- | 42 (26.8) |
| mrN+ | 104 (66.3) |
| mrNx | 11 (7.0) |
| Preoperative M stage; n (%) | |
| M0 | 137 (87.3) |
| M1 | 20 (12.7) |
| Preoperative mrCRM+ *; n (%) | 54 (34.2) |
| Operative time (min); mean ± SD | 306.6 ± 108.5 |
| Two-team approach; n (%) | 134 (85.4) |
| Abdominal dissection; n (%) | |
| Open | 3 (1.9) |
| Laparoscopic | 154 (98.1) |
| Conversion; n (%) | |
| Abdominal | 9 (5.7) |
| Perineal | 0 (0.0) |
| Defunctioning stoma; n (%) | |
| None | 16 (10.2) |
| Ileostomy | 135 (86.0) |
| Colostomy | 6 (3.8) |
| Anastomotic technique; n (%) | |
| None | 7 (4.5) |
| Hand-sewn | 54 (34.4) |
| Stapled (circular) | 96 (61.1) |
| Anastomotic distance from AV (cm); mean ± SD | 3.5 ± 1.5 |
| Urinary tract trauma; n (%) | 0 (0.0) |
| Pursestring failure; n (%) | 10 (6.4) |
| Complications; n (%) | 49 (31.2) |
| Anastomotic leak | 11 (7.0) |
| Colon ischemia | 5 (3.2) |
| Compartment syndrome | 1 (0.6) |
| Haemorrhage | 2 (1.3) |
| Internal hernia | 1 (0.6) |
| Obstruction | 2 (1.3) |
| Perforation | 1 (0.6) |
| Stoma complication | 5 (3.2) |
| Wound breakdown | 14 (8.9) |
| Cardiovascular complication | 3 (1.9) |
| DVT | 1 (0.6) |
| PE | 2 (1.3) |
| Pulmonary complication | 4 (2.5) |
| Renal Failure | 7 (4.5) |
| Urinary tract infection | 3 (1.9) |
| Others | 3 (1.9) |
| Re-operation | 21 (13.4) |
| Early anastomotic leak *; n (%) | 11 (7.0) |
| Endoscopic therapy | 9 (81.8) |
| Re-operation | 7 (63.6) |
| Definitive stoma after leakage | 3 (27.3) |
| Length of stay (days); mean ±SD | 11.4 ± 9.2 |
| Surgical morbidity (Clavien–Dindo III-V) **; n (%) | 30 (19.1) |
| Postoperative death | 3 (1.9) |
| Tumor size (mm); mean ± SD | 27.5 ± 17.4 |
| Distal margin (mm); mean ± SD | 21.0 ± 22.0 |
| Circumferential margin (mm); mean ± SD | 14.5 ± 11.4 |
| Positive circumferential margin *; n (%) | 12 (7.6) |
| Positive circumferential margin; n (%) | |
| Tumor height from AV >6cm, (n = 65) | 5 (7.7) |
| Tumor height from AV ≤6cm, (n = 92) | 7 (7.6) |
| No. lymph nodes harvested; mean ± SD | 16.2 ± 6.3 |
| pTMNT; n (%) | |
| T0 | 26 (16.6) |
| T1 | 17 (10.8) |
| T2 | 55 (35.0) |
| T3 | 52 (33.1) |
| T4 | 6 (3.8) |
| Tx | 1 (0.6) |
| pTMNN; n (%) | |
| N0 | 112 (71.3) |
| N1 | 30 (19.1) |
| N2 | 15 (9.6) |
| Quality of mesorectal specimen (Mercury grade); n (%) | |
| I (complete) | 137 (87.3) |
| II (nearly complete) | 12 (7.6) |
| III (incomplete) | 3 (1.9) |
| Missing | 5 (3.2) |
| Resection margin R1; n (%) | 7 (4.5) |
| Follow-up (mo); mean ± SD (range) | 19.5 ± 13.5 (0.1–52.3) |
| Local recurrence, n (%) | 6 (3.8) |
| Local recurrence only | 3 (1.9) |
| Simultaneous local/systemic recurrence | 3 (1.9) |
| Tumor recurrence (systemic), n (%) | 13 (8.3) |
| Death, n (%) | 22 (14.0) |
| Cancer | 10 (45.5) |
| Not cancer related | 4 (18.2) |
| 30-day mortality | 3 (13.6) |
| Unknown | 5 (22.7) |
| 3-year follow up * (n = 58) | |
| Local recurrence, n (%) | 2 (3.4) |
| Local recurrence only | 0 (0.0) |
| Simultaneous local/systemic recurrence | 2 (3.4) |
| Tumor recurrence (systemic), n (%) | 7 (12.1) |
| Death, n (%) | 12 (20.3) |
| Cancer | 7 (58.3) |
| Not cancer related | 2 (16.7) |
| 30-day mortalityUnknown | 1 (8.3)2 (16.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dittrich, L.; Biebl, M.; Schmuck, R.; Gül, S.; Weiss, S.; Haase, O.; Knoop, M.; Alkatout, I.; Pratschke, J.; Aigner, F. Initial Experience with the Safe Implementation of Transanal Total Mesorectal Excision (TaTME) as a Standardized Procedure for Low Rectal Cancer. J. Clin. Med. 2021, 10, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010072
Dittrich L, Biebl M, Schmuck R, Gül S, Weiss S, Haase O, Knoop M, Alkatout I, Pratschke J, Aigner F. Initial Experience with the Safe Implementation of Transanal Total Mesorectal Excision (TaTME) as a Standardized Procedure for Low Rectal Cancer. Journal of Clinical Medicine. 2021; 10(1):72. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010072
Chicago/Turabian StyleDittrich, Luca, Matthias Biebl, Rosa Schmuck, Safak Gül, Sascha Weiss, Oliver Haase, Michael Knoop, Ibrahim Alkatout, Johann Pratschke, and Felix Aigner. 2021. "Initial Experience with the Safe Implementation of Transanal Total Mesorectal Excision (TaTME) as a Standardized Procedure for Low Rectal Cancer" Journal of Clinical Medicine 10, no. 1: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10010072