
White Matter Integrity of the Corpus Callosum and Psychopathological Dimensions in Deficit and Non-Deficit Schizophrenia Patients

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessments
2.3. Image Acquisition
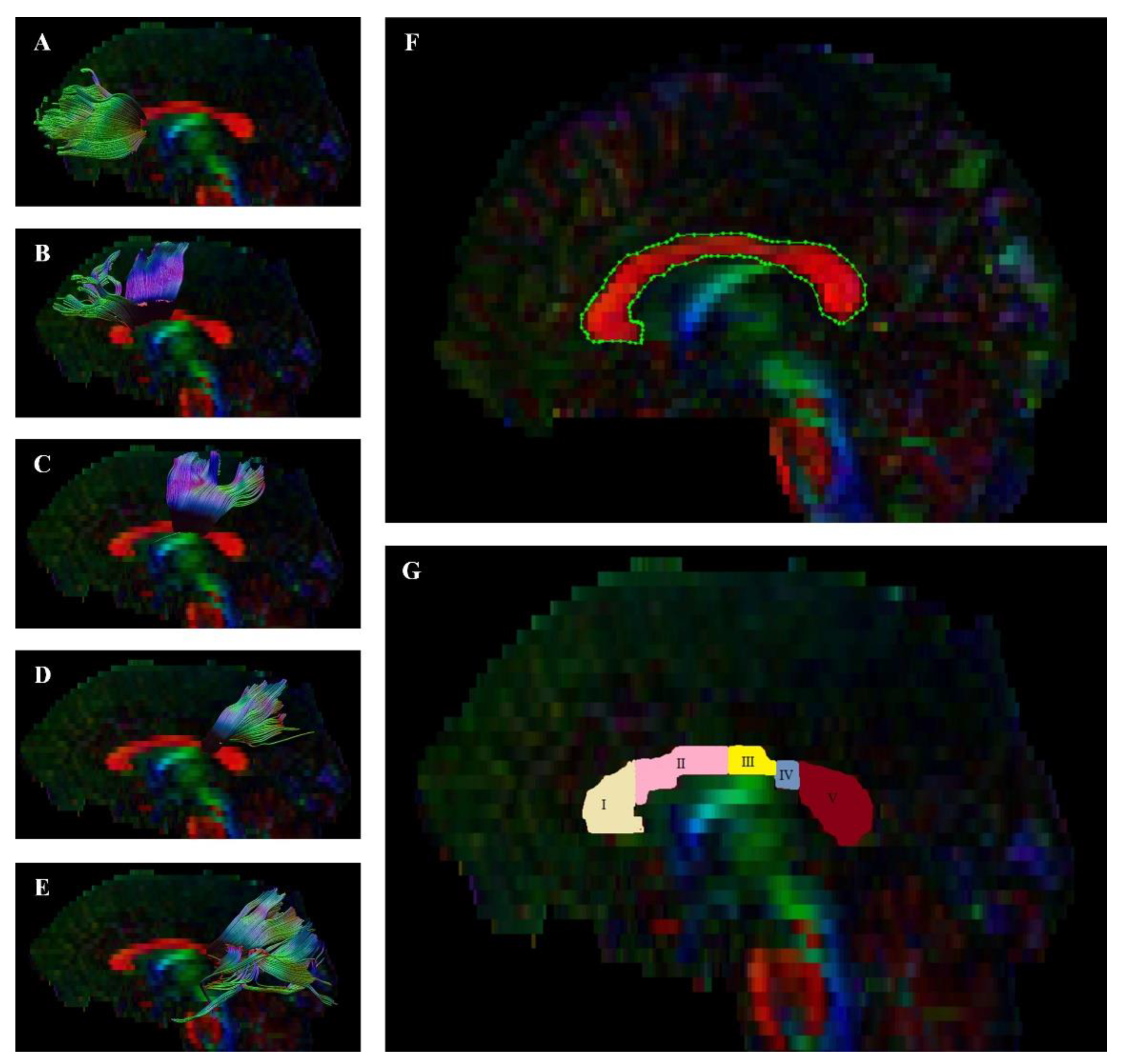
2.4. Image Processing and Quality
2.5. Procedure
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participants
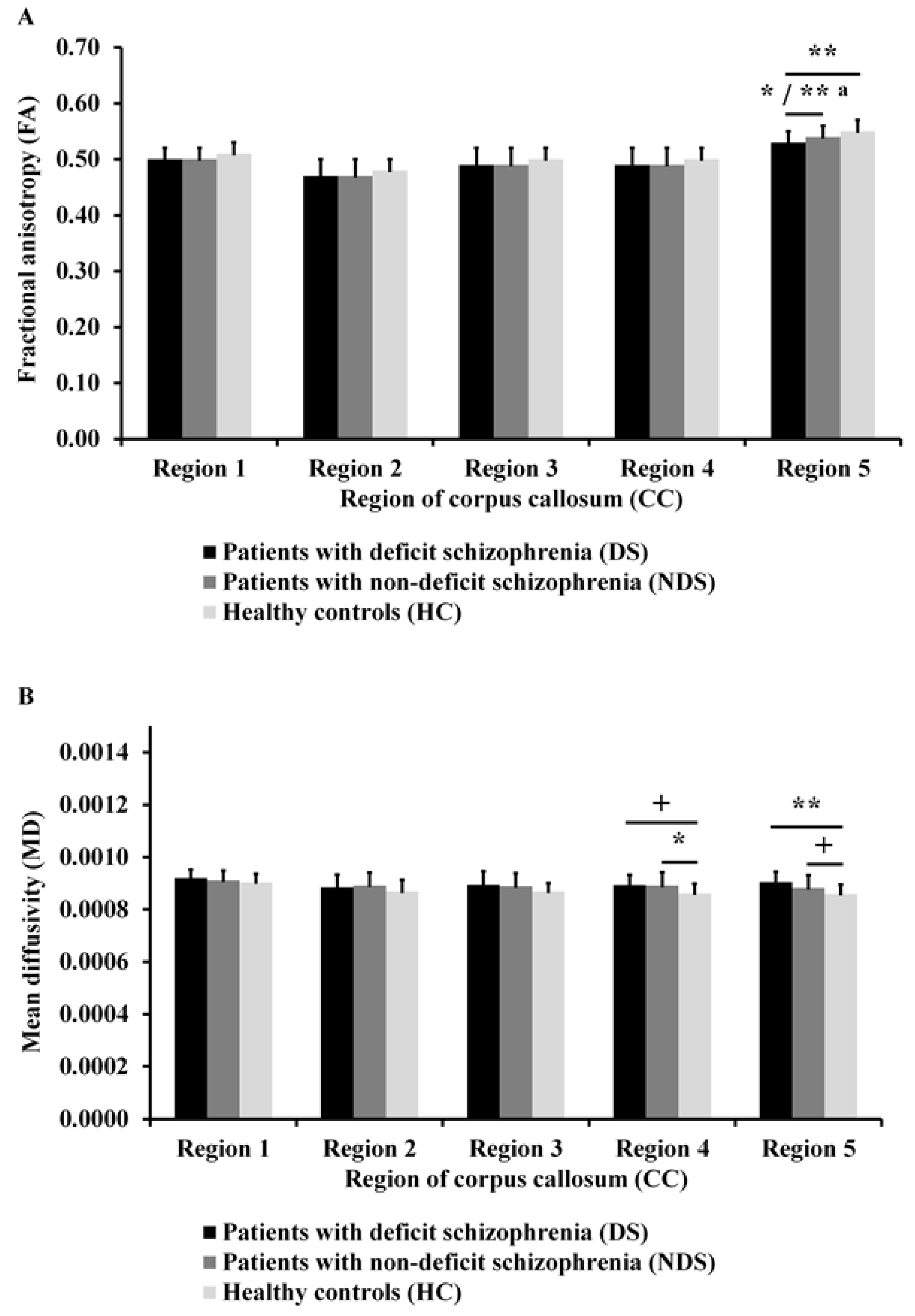
3.2. Differences in DTI Measures
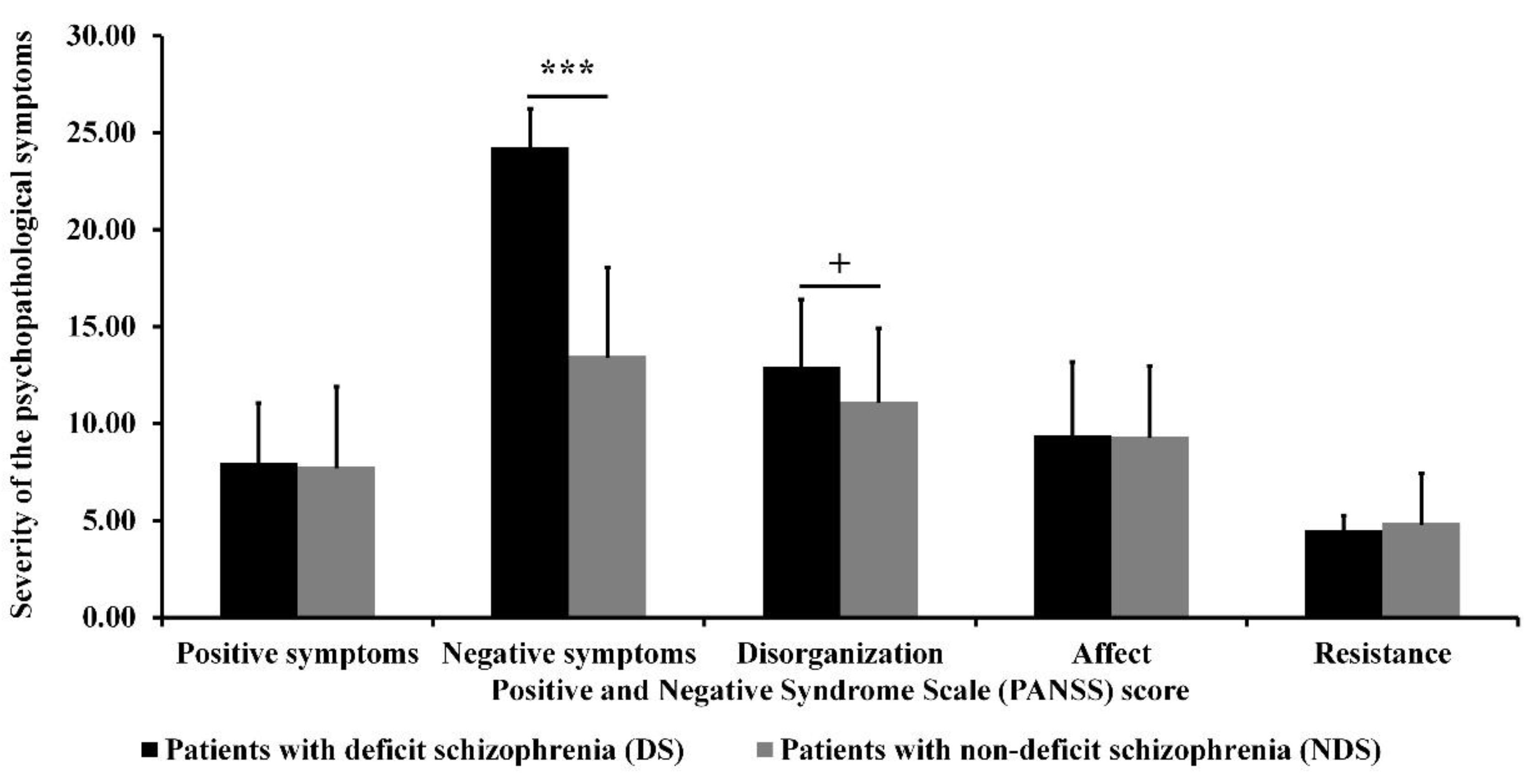
3.3. Differences in Psychopathological Dimensions
3.4. Relationship between DTI Measures and Psychopathological Dimensions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANCOVA | Analysis of covariance |
| ANOVA | Analysis of variance |
| BNSS | Brief Negative Symptom Scale |
| CC | Corpus callosum |
| DS | Deficit syndrome |
| DSM-IV | Diagnostic and Statistical Manual of Mental Disorders Fourth Edition |
| DTI | Diffusion tensor imaging |
| FA | Fractional anisotropy |
| GAF | Global Assessment of Functioning |
| HC | Healthy controls |
| ICD-10 | International Statistical Classification of Diseases and Related Health Problems Tenth Edition |
| M | Means |
| MD | Mean diffusivity |
| MINI | Mini-International Neuropsychiatric Interview |
| MRI | Magnetic resonance imaging |
| NDS | Non-deficit schizophrenia |
| PANSS | Positive and Negative Syndrome Scale |
| ROI | Region of interest |
| SD | Standard deviations |
| SNS | Self-evaluation of Negative Symptoms |
| TRS | Treatment-resistant schizophrenia |
| WM | White matter |
References
- McGrath, J.; Saha, S.; Chant, D.; Welham, J. Schizophrenia: A Concise Overview of Incidence, Prevalence, and Mortality. Epidemiol. Rev. 2008, 30, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentini, M.; Biondi, M.; Pasquini, M.; Picardi, A. Dimensional psychopathology of schizophrenia: SVARAD dimensional profiles in an acute inpatient sample. Riv. Psichiatr. 2018, 53, 40–48. [Google Scholar] [PubMed]
- Samochowiec, J.; Tyburski, E.; Misiak, B. Schizophrenia in Men; Medical Education Publishing: Warsaw, Poland, 2020. [Google Scholar]
- Charlson, F.J.; Ferrari, A.J.; Santomauro, D.F.; Diminic, S.; Stockings, E.; Scott, J.G.; McGrath, J.; A Whiteford, H. Global Epidemiology and Burden of Schizophrenia: Findings From the Global Burden of Disease Study 2016. Schizophr. Bull. 2018, 44, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Galderisi, S.; DeLisi, L.E.; Borgwardt, S. Neuroimaging of Schizophrenia and other Primary Psychotic Disorders: Achievements and Perspectives; Springer: Berlin/Heidelberg, Germany, 2019; pp. 1–345. [Google Scholar]
- Carpenter, W.T.; Heinrichs, D.W.; Wagman, A.M. Deficit and nondeficit forms of schizophrenia: The concept. Am. J. Psychiatry 1988, 145, 578–583. [Google Scholar] [CrossRef]
- Galderisi, S.; Maj, M.; Mucci, A.; Cassano, G.B.; Invernizzi, G.; Rossi, A.; Vita, A.; Dell’Osso, L.; Daneluzzo, E.; Pini, S. Historical, Psychopathological, Neurological, and Neuropsychological Aspects of Deficit Schizophrenia: A Multicenter Study. Am. J. Psychiatry 2002, 159, 983–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, B.; Galderisi, S. Deficit schizophrenia: An update. World Psychiatry 2008, 7, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Galderisi, S.; Quarantelli, M.; Volpe, U.; Mucci, A.; Cassano, G.B.; Invernizzi, G.; Rossi, A.; Vita, A.; Pini, S.; Cassano, P.; et al. Patterns of Structural MRI Abnormalities in Deficit and Nondeficit Schizophrenia. Schizophr. Bull. 2008, 34, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Emsley, R.; Rabinowitz, J.; Torreman, M. The factor structure for the Positive and Negative Syndrome Scale (PANSS) in recent-onset psychosis. Schizophr. Res. 2003, 61, 47–57. [Google Scholar] [CrossRef]
- Crow, T.J. The Two-syndrome Concept: Origins and Current Status. Schizophr. Bull. 1985, 11, 471–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, B.; Strauss, G.P.; Nguyen, L.; Fischer, B.A.; Daniel, D.G.; Cienfuegos, A.; Marder, S.R. The Brief Negative Symptom Scale: Psychometric Properties. Schizophr. Bull. 2011, 37, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Shafer, A.; Dazzi, F. Meta-analysis of the positive and Negative Syndrome Scale (PANSS) factor structure. J. Psychiatr. Res. 2019, 115, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, S.H.; Folsom, T.D. The Neurodevelopmental Hypothesis of Schizophrenia, Revisited. Schizophr. Bull. 2009, 35, 528–548. [Google Scholar] [CrossRef]
- Barron, H.; Hafizi, S.; Andreazza, A.C.; Mizrahi, R. Neuroinflammation and Oxidative Stress in Psychosis and Psychosis Risk. Int. J. Mol. Sci. 2017, 18, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najjar, S.; Pearlman, D.M. Neuroinflammation and white matter pathology in schizophrenia: Systematic review. Schizophr. Res. 2015, 161, 102–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friston, K.; Brown, H.R.; Siemerkus, J.; Stephan, K.E. The dysconnection hypothesis. Schizophr. Res. 2016, 176, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Fan, L.; Qiu, C.; Jiang, T. Prefrontal cortex and the dysconnectivity hypothesis of schizophrenia. Neurosci. Bull. 2015, 31, 207–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoonover, K.E.; Farmer, C.B.; Cash, A.E.; Roberts, R.C. Pathology of white matter integrity in three major white matter fasciculi: A post-mortem study of schizophrenia and treatment status. Br. J. Pharmacol. 2019, 176, 1143–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soares, J.M.; Marques, P.; Alves, V.; Sousa, N. A hitchhiker’s guide to diffusion tensor imaging. Front. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, S.; Jahanshad, N.; Zalesky, A.; Kochunov, P.; Agartz, I.; Alloza, C.; A Andreassen, O.; Arango, C.; Banaj, N.; Bouix, S.; et al. Widespread white matter microstructural differences in schizophrenia across 4322 individuals: Results from the ENIGMA Schizophrenia DTI Working Group. Mol. Psychiatry 2018, 23, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, P. X linked recessive inheritance of agenesis of the corpus callosum. J. Med. Genet. 1983, 20, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Schutter, D.J.; Harmon-Jones, E. The corpus callosum: A commissural road to anger and aggression. Neurosci. Biobehav. Rev. 2013, 37, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.; Walterfang, M.; Petralli, C.; Velakoulis, D. First-Episode ‘Coenesthetic’ Schizophrenia Presenting with Alien Hand Syndrome and Partial Agenesis of the Corpus Callosum. Neuropsychobiology 2008, 58, 118–122. [Google Scholar] [CrossRef]
- Gazzaniga, M.S. Cerebral specialization and interhemispheric communication: Does the corpus callosum enable the human condition? Brain 2000, 123, 1293–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodruff, P.W.; McManus, I.C.; David, A.S. Meta-analysis of corpus callosum size in schizophrenia. J. Neurol. Neurosurg. Psychiatry 1995, 58, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Arnone, D.; McIntosh, A.; Tan, G.; Ebmeier, K. Meta-analysis of magnetic resonance imaging studies of the corpus callosum in schizophrenia. Schizophr. Res. 2008, 101, 124–132. [Google Scholar] [CrossRef]
- Johnson, S.L.M.; Greenstein, D.; Clasen, L.; Miller, R.; LaLonde, F.; Rapoport, J.; Gogtay, N. Absence of anatomic corpus callosal abnormalities in childhood-onset schizophrenia patients and healthy siblings. Psychiatry Res. Neuroimaging 2013, 211, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, D.; Wang, Y.; Chang, X.; Jiang, Y.; Klugah-Brown, B.; Luo, C.; Yao, D. Shared abnormality of white matter integrity in schizophrenia and bipolar disorder: A comparative voxel-based meta-analysis. Schizophr. Res. 2017, 185, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Koshiyama, D.; Fukunaga, M.; Okada, N.; Morita, K.; Nemoto, K.; Usui, K.; Yamamori, H.; Yasuda, Y.; Fujimoto, M.; Kudo, N.; et al. White matter microstructural alterations across four major psychiatric disorders: Mega-analysis study in 2937 individuals. Mol. Psychiatry 2020, 25, 883–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Re, E.C.; Bouix, S.; Fitzsimmons, J.; Blokland, G.A.; Mesholam-Gately, R.; Wojcik, J.; Kikinis, Z.; Kubicki, M.; Petryshen, T.; Pasternak, O.; et al. Diffusion abnormalities in the corpus callosum in first episode schizophrenia: Associated with enlarged lateral ventricles and symptomatology. Psychiatry Res. 2019, 277, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Madigand, J.; Tréhout, M.; Delcroix, N.; Dollfus, S.; Leroux, E. Corpus callosum microstructural and macrostructural abnormalities in schizophrenia according to the stage of disease. Psychiatry Res. Neuroimaging 2019, 291, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Del Re, E.C.; Konishi, J.; Bouix, S.; Blokland, G.A.M.; Mesholam-Gately, R.I.; Goldstein, J.M.; Kubicki, M.; Wojcik, J.; Pasternak, O.; Seidman, L.J.; et al. Enlarged lateral ventricles inversely correlate with reduced corpus callosum central volume in first episode schizophrenia: Association with functional measures. Brain Imaging Behav. 2016, 10, 1264–1273. [Google Scholar] [CrossRef] [Green Version]
- Rowland, L.M.; A Spieker, E.; Francis, A.; Barker, P.B.; Carpenter, W.T.; Buchanan, R.W. White Matter Alterations in Deficit Schizophrenia. Neuropsychopharmacology 2009, 34, 1514–1522. [Google Scholar] [CrossRef] [PubMed]
- Kitis, O.; Ozalay, O.; Zengin, E.B.; Haznedaroglu, D.; Eker, M.C.; Yalvac, D.; Oğuz, K.; Coburn, K.; Gonul, A.S. Reduced left uncinate fasciculus fractional anisotropy in deficit schizophrenia but not in non-deficit schizophrenia. Psychiatry Clin. Neurosci. 2012, 66, 34–43. [Google Scholar] [CrossRef]
- Voineskos, A.N.; Foussias, G.; Lerch, J.; Felsky, D.; Remington, G.; Rajji, T.K.; Lobaugh, N.; Pollock, B.G.; Mulsant, B.H. Neuroimaging Evidence for the Deficit Subtype of Schizophrenia. JAMA Psychiatry 2013, 70, 472–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, W.; Li, N.; Deng, W.; Li, M.; Huang, C.; Ma, X.; Wang, Q.; Guo, W.; Li, Y.; Jiang, L.; et al. White matter alterations in first episode treatment-naïve patients with deficit schizophrenia: A combined VBM and DTI study. Sci. Rep. 2015, 5, 12994. [Google Scholar] [CrossRef]
- Tan, A.S.; Chew, Q.H.; Sim, K. Cerebral white matter changes in deficit and non-deficit subtypes of schizophrenia. J. Neural Transm. 2020, 127, 1073–1079. [Google Scholar] [CrossRef]
- Spalletta, G.; De Rossi, P.; Piras, F.; Iorio, M.; Dacquino, C.; Scanu, F.; Girardi, P.; Caltagirone, C.; Kirkpatrick, B.; Chiapponi, C. Brain white matter microstructure in deficit and non-deficit subtypes of schizophrenia. Psychiatry Res. Neuroimaging 2015, 231, 252–261. [Google Scholar] [CrossRef]
- Lang, X.-E.; Zhu, D.; Zhang, G.; Du, X.; Jia, Q.; Yin, G.; Chen, D.; Xiu, M.; Cao, B.; Wang, L.; et al. Sex difference in association of symptoms and white matter deficits in first-episode and drug-naive schizophrenia. Transl. Psychiatry 2018, 8, 281. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gastiasoro, A.; Zubiaurre-Elorza, L.; Peña, J.; Ibarretxe-Bilbao, N.; Rilo, O.; Schretlen, D.J.; Ojeda, N. Altered frontal white matter asymmetry and its implications for cognition in schizophrenia: A tractography study. NeuroImage Clin. 2019, 22, 101781. [Google Scholar] [CrossRef] [PubMed]
- Koshiyama, D.; Fukunaga, M.; Okada, N.; Morita, K.; Nemoto, K.; Yamashita, F.; Yamamori, H.; Yasuda, Y.; Fujimoto, M.; Kelly, S.; et al. Role of frontal white matter and corpus callosum on social function in schizophrenia. Schizophr. Res. 2018, 202, 180–187. [Google Scholar] [CrossRef] [PubMed]
- De Assunção-Leme, I.B.; Zugman, A.; De Moura, L.M.; Sato, J.R.; Higuchi, C.; Ortiz, B.B.; Noto, C.; Ota, V.K.; Belangero, S.I.; Bressan, R.A.; et al. Is treatment-resistant schizophrenia associated with distinct neurobiological callosal connectivity abnormalities? CNS Spectr. 2020, 1–5. [Google Scholar] [CrossRef]
- Kapur, S. Looking for a “biological test” to diagnose “schizophrenia”: Are we chasing red herrings? World Psychiatry 2011, 10, 32. [Google Scholar] [CrossRef] [Green Version]
- Harms, M.P.; Akhter, K.D.; Csernansky, J.G.; Mori, S.; Barch, D.M. Fractional anisotropy in individuals with schizophrenia and their nonpsychotic siblings. Psychiatry Res. Neuroimaging 2015, 231, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitford, T.J.; Kubicki, M.; Schneiderman, J.S.; O’Donnell, L.J.; King, R.; Alvarado, J.L.; Khan, U.; Markant, D.; Nestor, P.G.; Niznikiewicz, M.; et al. Corpus Callosum Abnormalities and Their Association with Psychotic Symptoms in Patients with Schizophrenia. Biol. Psychiatry 2010, 68, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Hofer, S.; Frahm, J. Topography of the human corpus callosum revisited—Comprehensive fiber tractography using diffusion tensor magnetic resonance imaging. Neuroimage 2006, 32, 989–994. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Kirkpatrick, B.; Buchanan, R.W.; Breier, A.; Carpenter, W.T. Case identification and stability of the deficit syndrome of schizophrenia. Psychiatry Res. 1993, 47, 47–56. [Google Scholar] [CrossRef]
- Goetz, R.R.; Corcoran, C.; Yale, S.; Stanford, A.D.; Kimhy, D.; Amador, X.; Malaspina, D. Validity of a ‘proxy’ for the deficit syndrome derived from the Positive And Negative Syndrome Scale (PANSS). Schizophr. Res. 2007, 93, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Dollfus, S.; Mach, C.; Morello, R. Self-evaluation of negative symptoms. Schizophr. Bull. 2016, 42, 571–578. [Google Scholar] [CrossRef] [Green Version]
- Hall, R.C. Global Assessment of Functioning: A Modified Scale. J. Psychosom. Res. 1995, 36, 267–275. [Google Scholar] [CrossRef]
- Leemans, A.; Jeurissen, B.; Sijbers, J.; Jones, D.K. ExploreDTI: A graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc. Int. Soc. Magn. Reson. Med. 2009, 17, 3537. [Google Scholar]
- Hair, J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Educational International: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Wendt, H.W. Dealing with a common problem in Social science: A simplified rank-biserial coefficient of correlation based on the U statistic. Eur. J. Soc. Psychol. 1972, 2, 463–465. [Google Scholar] [CrossRef]
- Ohoshi, Y.; Takahashi, S.; Yamada, S.; Ishida, T.; Tsuda, K.; Tsuji, T.; Terada, M.; Shinosaki, K.; Ukai, S. Microstructural abnormalities in callosal fibers and their relationship with cognitive function in schizophrenia: A tract-specific analysis study. Brain Behav. 2019, 9, e01357. [Google Scholar] [CrossRef] [PubMed]
- Thiese, M.S.; Ronna, B.; Ott, U. P value interpretations and considerations. J. Thorac. Dis. 2016, 8, E928–E931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparotti, R.; Valsecchi, P.; Carletti, F.; Galluzzo, A.; Liserre, R.; Cesana, B.; Sacchetti, E. Reduced fractional anisotropy of corpus callosum in first-contact, antipsychotic drug-naive patients with schizophrenia. Schizophr. Res. 2009, 108, 41–48. [Google Scholar] [CrossRef]
- Podwalski, P.; Szczygieł, K.; Tyburski, E.; Sagan, L.; Misiak, B.; Samochowiec, J. Magnetic resonance diffusion tensor imaging in psychiatry: A narrative review of its potential role in diagnosis. Pharmacol. Rep. 2020, 73, 43–56. [Google Scholar] [CrossRef]
- Köşger, F.; Yiğitaslan, S.; Eşsizoğlu, A.; Güleç, G.; Dağ Karataş, R.; Sevil Değirmenci, S. Inflammation and oxidative stress in deficit schizophrenia. Noropsikiyatri Ars. 2020, 57, 303–307. [Google Scholar]
- Garcia-Rizo, C.; Fernandez-Egea, E.; Oliveira, C.; Justicia, A.; Bernardo, M.; Kirkpatrick, B. Inflammatory markers in antipsychotic-naïve patients with nonaffective psychosis and deficit vs. nondeficit features. Psychiatry Res. 2012, 198, 212–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogel, B.O.; Lett, T.A.; Erk, S.; Mohnke, S.; Wackerhagen, C.; Brandl, E.J.; Romanczuk-Seiferth, N.; Otto, K.; Schweiger, J.I.; Tost, H.; et al. The influence of MIR137 on white matter fractional anisotropy and cortical surface area in individuals with familial risk for psychosis. Schizophr. Res. 2018, 195, 190–196. [Google Scholar] [CrossRef]
- Patel, S.; Mahon, K.; Wellington, R.; Zhang, J.; Chaplin, W.; Szeszko, P.R. A meta-analysis of diffusion tensor imaging studies of the corpus callosum in schizophrenia. Schizophr. Res. 2011, 129, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Tohid, H.; Faizan, M.; Faizan, U. Alterations of the occipital lobe in schizophrenia. Neurosciences 2015, 20, 213–224. [Google Scholar] [CrossRef] [Green Version]
- Miyata, J.; Yamada, M.; Namiki, C.; Hirao, K.; Saze, T.; Fujiwara, H.; Shimizu, M.; Kawada, R.; Fukuyama, H.; Sawamoto, N.; et al. Reduced white matter integrity as a neural correlate of social cognition deficits in schizophrenia. Schizophr. Res. 2010, 119, 232–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantrowitz, J.T.; Butler, P.D.; Schecter, I.; Silipo, G.; Javitt, D.C. Seeing the World Dimly: The Impact of Early Visual Deficits on Visual Experience in Schizophrenia. Schizophr. Bull. 2009, 35, 1085–1094. [Google Scholar] [CrossRef] [Green Version]
- Foong, J.; Symms, M.R.; Barker, G.J.; Maier, M.; Woermann, F.G.; Miller, D.H.; Ron, M.A. Neuropathological abnormalities in schizophrenia: Evidence from magnetization transfer imaging. Brain 2001, 124, 882–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujino, J.; Takahashi, H.; Miyata, J.; Sugihara, G.; Kubota, M.; Sasamoto, A.; Fujiwara, H.; Aso, T.; Fukuyama, H.; Murai, T. Impaired empathic abilities and reduced white matter integrity in schizophrenia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 48, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Yao, S.; Kirkpatrick, B.; Shi, C.; Yi, J. Psychopathology and neuropsychological impairments in deficit and nondeficit schizophrenia of Chinese origin. Psychiatry Res. 2008, 158, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Tiryaki, A.; Yazıcı, M.K.; Anil, A.E.; Kabakci, E.; Karaagaoglu, E.; Göğüş, A. Reexamination of the characteristics of the deficit schizophrenia patients. Eur. Arch. Psychiatry Clin. Neurosci. 2003, 253, 221–227. [Google Scholar] [CrossRef]
- Tyburski, E.; Pełka-Wysiecka, J.; Mak, M.; Samochowiec, A.; Bieńkowski, P.; Samochowiec, J. Neuropsychological Profile of Specific Executive Dysfunctions in Patients with Deficit and Non-deficit Schizophrenia. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.S.; Brown, L.A.; Minor, K.S. The psychiatric symptomatology of deficit schizophrenia: A meta-analysis. Schizophr. Res. 2010, 118, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kawasaki, Y.; Takahashi, T.; Furuichi, A.; Noguchi, K.; Seto, H.; Suzuki, M. Reduced white matter fractional anisotropy and clinical symptoms in schizophrenia: A voxel-based diffusion tensor imaging study. Psychiatry Res. Neuroimaging 2012, 202, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Minami, T.; Nobuhara, K.; Okugawa, G.; Takase, K.; Yoshida, T.; Sawada, S.; Ha-Kawa, S.; Ikeda, K.; Kinoshita, T. Diffusion Tensor Magnetic Resonance Imaging of Disruption of Regional White Matter in Schizophrenia. Neuropsychobiology 2003, 47, 141–145. [Google Scholar] [CrossRef]
- Foong, J.; Maier, M.; A Clark, C.; Barker, G.J.; Miller, D.H.; A Ron, M. Neuropathological abnormalities of the corpus callosum in schizophrenia: A diffusion tensor imaging study. J. Neurol. Neurosurg. Psychiatry 2000, 68, 242–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijanki, K.R.; Hodis, B.; Magnotta, V.A.; Zeien, E.; Andreasen, N.C. Effects of age on white matter integrity and negative symptoms in schizophrenia. Schizophr. Res. 2015, 161, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Kanaan, R.; Barker, G.; Brammer, M.; Giampietro, V.; Shergill, S.; Woolley, J.; Picchioni, M.; Toulopoulou, T.; McGuire, P. White matter microstructure in schizophrenia: Effects of disorder, duration and medication. Br. J. Psychiatry 2009, 194, 236–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Cao, D.; Liang, X.; Zhao, J. Schizophrenia symptomatic associations with diffusion tensor imaging measured fractional anisotropy of brain: A meta-analysis. Neuroradiology 2017, 59, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.Y.; Fan, F.-M.; Chen, D.-C.; Tan, Y.-L.; Tan, S.-P.; Hu, K.; Salas, R.; Kosten, T.R.; Zunta-Soares, G.; Soares, J.C. Extensive White Matter Abnormalities and Clinical Symptoms in Drug-Naive Patients With First-Episode Schizophrenia: A Voxel-Based Diffusion Tensor Imaging Study. J. Clin. Psychiatry 2016, 77, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Kubicki, M.; Styner, M.; Bouix, S.; Gerig, G.; Markant, D.; Smith, K.; Kikinis, R.; McCarley, R.; Shenton, M. Reduced interhemispheric connectivity in schizophrenia-tractography based segmentation of the corpus callosum. Schizophr. Res. 2008, 106, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, C.; Zhang, Y.; Wei, F.; Cheng, Y.; Cao, Y.; Hou, H. Magnetic resonance imaging DTI-FT study on schizophrenic patients with typical negative first symptoms. Exp. Ther. Med. 2016, 12, 1450–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Edmiston, E.K.; Chen, K.; Tang, Y.; Ouyang, X.; Jiang, Y.; Fan, G.; Ren, L.; Liu, J.; Zhou, Y.; et al. A comparative diffusion tensor imaging study of corpus callosum subregion integrity in bipolar disorder and schizophrenia. Psychiatry Res. Neuroimaging 2014, 221, 58–62. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| At least two of the following six negative symptoms must be present: |
| a. Restricted affect |
| b. Diminished emotional range |
| c. Poverty of speech |
| d. Curbing of interests |
| e. Diminished sense of purpose |
| f. Diminished social drive |
| Some combination of two or more of the negative symptoms listed above has been present for the preceding 12 months and always was present during periods of clinical stability (including chronic psychotic states). These symptoms may or may not be detectable during transient episodes of acute psychotic disorganization or decompensation. |
| The negative symptoms above are primary (i.e., not secondary to factors other than the disease process). Such factors include: |
| a. Anxiety |
| b. Drug effect |
| c. Suspiciousness (and other psychotic symptoms) |
| d. Mental retardation |
| e. Depression |
| The patient meets ICD-10 criteria for schizophrenia. |
| Patients with Deficit Schizophrenia (DS) (n = 15) | Patients with Non-Deficit Schizophrenia (NDS) (n = 40) | Healthy Controls (HC) (n = 30) | F/H/χ2/t/Z | |
|---|---|---|---|---|
| Age: M (SD) | 39.80 (6.14) | 38.83 (7.24) | 37.30 (8.24) | 0.66 a |
| Years of education: M (SD) | 12.80 (2.60) | 13.40 (2.63) | 14.53 (2.60) | 4.85 b |
| Sex: female/male | 4/11 | 22/18 | 16/14 | 3.79 c |
| Antipsychotic medications: | ||||
| Atypical: n (%) | 11 (73.33) | 26 (65.00) | - | 1.24 c |
| Atypical and typical: n (%) | 4 (26.67) | 11 (27.50) | - | |
| Typical: n (%) | 0 (0.00) | 2 (5.00) | - | |
| No medications: n (%) | 0 (0.00) | 1 (2.50) | - | |
| Chlorpromazine equivalent (mg): M (SD) | 706.20 (323.36) | 622.00 (294.16) | - | 0.92 d |
| Duration of illness: M (SD) | 17.73 (5.80) | 13.60 (4.96) | - | −2.38 e |
| Exacerbation: M (SD) | 5.80 (2.54) | 6.23 (4.31) | - | −0.33 e |
| Treatment interruptions: M (SD) | 0.40 (0.57) | 1.08 (1.50) | - | −1.58 e |
| Global functioning in GAF: M (SD) | 55.33 (13.70) | 59.70 (13.82) | - | −1.05 d |
| Variable | Positive Symptoms in PANSS (r/rho) | Negative Symptoms in PANSS (r/rho) | Disorganization in PANSS (r/rho) | Affect in PANSS (r/rho) | Resistance in PANSS (r/rho) |
|---|---|---|---|---|---|
| Patients with deficit schizophrenia (DS) | |||||
| (n = 15) | |||||
| Fractional anisotropy (FA) | |||||
| Region 5 | 0.17 a | 0.16 a | 0.02 a | 0.18 a | −0.10 a |
| Mean diffusivity (MD) | |||||
| Region 5 | 0.01 a | −0.16 a | −0.08 a | −0.34 a | −0.13 a |
| Patients with non-deficit schizophrenia (NDS) | |||||
| (n = 40) | |||||
| Mean diffusivity (MD) | |||||
| Region 4 | 0.09 b | −0.17 b | 0.28 b | −0.17 b | 0.32 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podwalski, P.; Tyburski, E.; Szczygieł, K.; Waszczuk, K.; Rek-Owodziń, K.; Mak, M.; Plichta, P.; Bielecki, M.; Rudkowski, K.; Kucharska-Mazur, J.; et al. White Matter Integrity of the Corpus Callosum and Psychopathological Dimensions in Deficit and Non-Deficit Schizophrenia Patients. J. Clin. Med. 2021, 10, 2225. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112225
Podwalski P, Tyburski E, Szczygieł K, Waszczuk K, Rek-Owodziń K, Mak M, Plichta P, Bielecki M, Rudkowski K, Kucharska-Mazur J, et al. White Matter Integrity of the Corpus Callosum and Psychopathological Dimensions in Deficit and Non-Deficit Schizophrenia Patients. Journal of Clinical Medicine. 2021; 10(11):2225. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112225
Chicago/Turabian StylePodwalski, Piotr, Ernest Tyburski, Krzysztof Szczygieł, Katarzyna Waszczuk, Katarzyna Rek-Owodziń, Monika Mak, Piotr Plichta, Maksymilian Bielecki, Krzysztof Rudkowski, Jolanta Kucharska-Mazur, and et al. 2021. "White Matter Integrity of the Corpus Callosum and Psychopathological Dimensions in Deficit and Non-Deficit Schizophrenia Patients" Journal of Clinical Medicine 10, no. 11: 2225. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112225