
Effects of Hyperglycemia and Diabetes Mellitus on Coagulation and Hemostasis

 , , and
, , and
Abstract
:1. Introduction
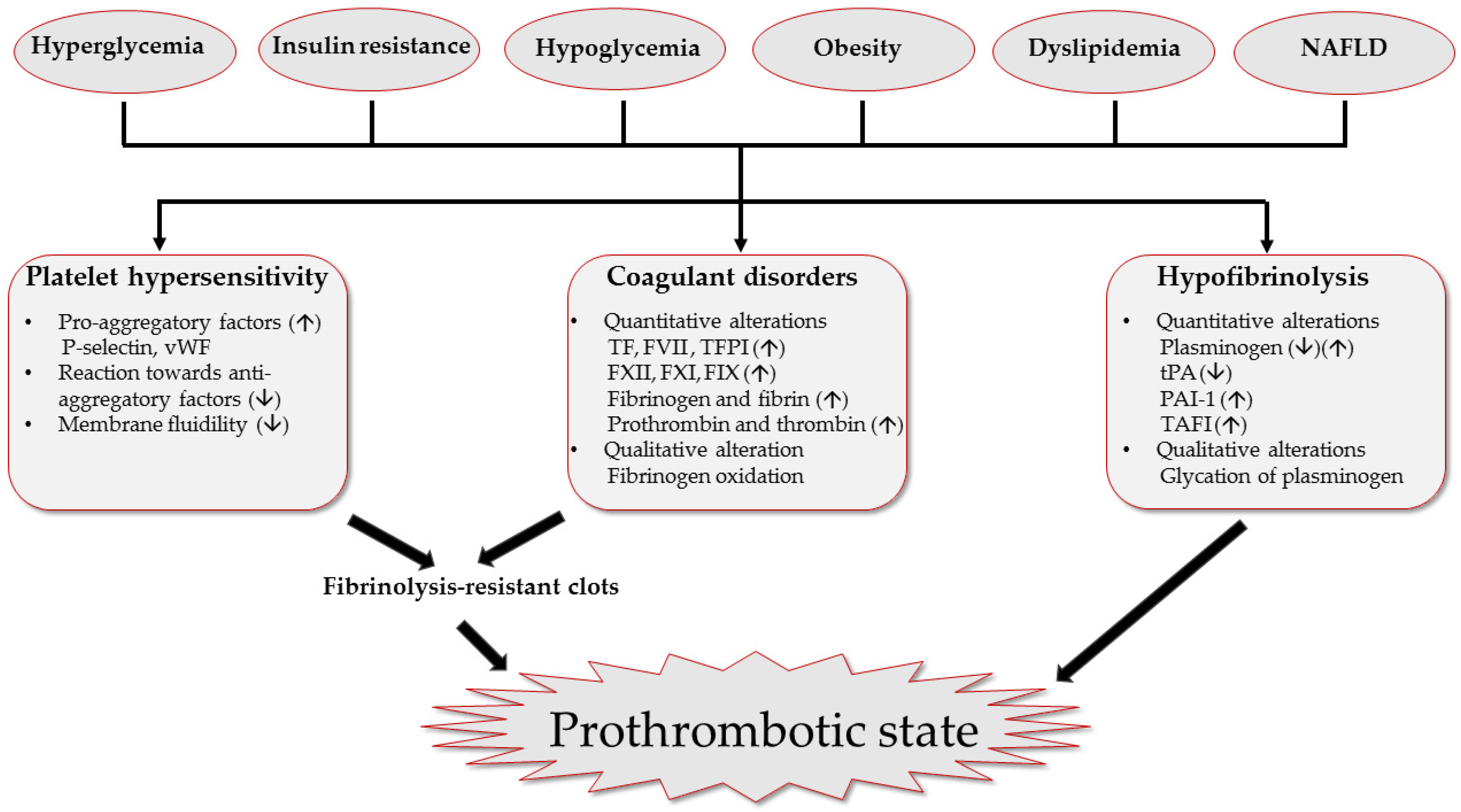
2. Prothrombotic State Associated with Diabetes Mellitus
2.1. Platelet Hypersensitivity
2.1.1. Hyperglycemia
2.1.2. Insulin Resistance
2.2. Quantitative and Qualitative Alterations of Coagulation Factors
2.3. Hypofibrinolysis
3. Prothrombotic Effects of Coexisting Metabolic Disorders
3.1. Hypoglycemia
3.2. Obesity
3.3. Dyslipidemia
3.4. Nonachoholic Fatty Liver Disease (NAFLD)
4. Management of Pro-Thrombotic State in DM
4.1. Antiplatelet Medications
4.2. Anticoagulation Medications
4.3. Metabolism Optimization
4.3.1. Glucose Control
4.3.2. Weight Loss
4.3.3. Lipid-Lowering Therapy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Hulst, A.H.; Visscher, M.J.; Cherpanath, T.G.V.; van de Wouw, L.; Godfried, M.B.; Thiel, B.; Gerritse, B.M.; Scohy, T.V.; Bouwman, R.A.; Willemsen, M.G.; et al. Effects of Liraglutide on Myocardial Function After Cardiac Surgery: A Secondary Analysis of the Randomised Controlled GLOBE Trial. J. Clin. Med. 2020, 9, 0673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szekely, A.; Levin, J.; Miao, Y.; Tudor, I.C.; Vuylsteke, A.; Ofner, P.; Mangano, D.T. Investigators of the Multicenter Study of Perioperative Ischemia Research Group. Impact of hyperglycemia on perioperative mortality after coronary artery bypass graft surgery. J. Thorac. Cardiovasc. Surg. 2011, 142, 430–437e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versteeg, H.H.; Heemskerk, J.W.; Levi, M.; Reitsma, P.H. New fundamentals in hemostasis. Physiol. Rev. 2013, 93, 327–358. [Google Scholar] [CrossRef] [Green Version]
- Chapin, J.C.; Hajjar, K.A. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015, 29, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westein, E.; Hoefer, T.; Calkin, A.C. Thrombosis in diabetes: A shear flow effect? Clin. Sci. 2017, 131, 1245–1260. [Google Scholar] [CrossRef]
- Patti, G.; Cerchiara, E.; Bressi, E.; Giannetti, B.; Veneri, A.D.; Di Sciascio, G.; Avvisati, G.; De Caterina, R. Endothelial Dysfunction, Fibrinolytic Activity, and Coagulation Activity in Patients with Atrial Fibrillation According to Type II Diabetes Mellitus Status. Am. J. Cardiol. 2020, 125, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.N.; Deyell, J.S.; Sharma, S.N.; Barseghian, A. Role of and Recent Evidence for Antiplatelet Therapy in Prevention of Cardiovascular Disease in Diabetes. Curr. Cardiol. Rep. 2019, 21, 78. [Google Scholar] [CrossRef]
- Lemkes, B.A.; Hermanides, J.; Devries, J.H.; Holleman, F.; Meijers, J.C.; Hoekstra, J.B. Hyperglycemia: A prothrombotic factor? J. Thromb. Haemost. 2010, 8, 1663–1669. [Google Scholar] [CrossRef]
- Holinstat, M. Normal platelet function. Cancer Metastasis Rev. 2017, 36, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Manzo-Silberman, S.; Nicaise-Roland, P.; Neukirch, C.; Tubach, F.; Huisse, M.G.; Chollet-Martin, S.; Abergel, H.; Driss, F.; Alfaiate, T.; Ajzenberg, N.; et al. Effect of rapid desensitization on platelet inhibition and basophil activation in patients with aspirin hypersensitivity and coronary disease. Eur. Heart J. Cardiovasc. Pharmacother. 2017, 3, 77–81. [Google Scholar] [CrossRef]
- Santilli, F.; Simeone, P.; Liani, R.; Davi, G. Platelets and diabetes mellitus. Prostaglandins Other Lipid Mediat. 2015, 120, 28–39. [Google Scholar] [CrossRef]
- Saluja, M.; Swami, Y.K.; Meena, S.R. Study of Impact of Glycemic Status (HbA1c) on Platelet Activity measured by Mean Platelet Volume & Vascular Complications in Diabetics. J. Assoc. Physicians India 2019, 67, 26–29. [Google Scholar] [PubMed]
- Malachowska, B.; Tomasik, B.; Szadkowska, A.; Baranowska-Jazwiecka, A.; Wegner, O.; Mlynarski, W.; Fendler, W. Altered platelets’ morphological parameters in children with type 1 diabetes—A case-control study. BMC Endocr. Disord. 2015, 15, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesh, V.; Kumar, R.; Varma, D.K.; Bhatia, P.; Yadav, J.; Dayal, D. Changes in platelet morphology indices in relation to duration of disease and glycemic control in children with type 1 diabetes mellitus. J. Diabetes Complicat. 2018, 32, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Ozder, A.; Eker, H.H. Investigation of mean platelet volume in patients with type 2 diabetes mellitus and in subjects with impaired fasting glucose: A cost-effective tool in primary health care? Int. J. Clin. Exp. Med. 2014, 7, 2292–2297. [Google Scholar]
- Zaccardi, F.; Rocca, B.; Rizzi, A.; Ciminello, A.; Teofili, L.; Ghirlanda, G.; De Stefano, V.; Pitocco, D. Platelet indices and glucose control in type 1 and type 2 diabetes mellitus: A case-control study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Kaur, M.; Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 2018, 17, 121. [Google Scholar] [CrossRef]
- Ghoshal, K.; Bhattacharyya, M. Overview of platelet physiology: Its hemostatic and nonhemostatic role in disease pathogenesis. Sci. World J. 2014, 2014, 781857. [Google Scholar] [CrossRef] [Green Version]
- Giannella, A.; Ceolotto, G.; Radu, C.M.; Cattelan, A.; Iori, E.; Benetti, A.; Fabris, F.; Simioni, P.; Avogaro, A.; Vigili de Kreutzenberg, S. PAR-4/Ca(2+)-calpain pathway activation stimulates platelet-derived microparticles in hyperglycemic type 2 diabetes. Cardiovasc. Diabetol. 2021, 20, 77. [Google Scholar] [CrossRef] [PubMed]
- Rusak, T.; Misztal, T.; Rusak, M.; Branska-Januszewska, J.; Tomasiak, M. Involvement of hyperglycemia in the development of platelet procoagulant response: The role of aldose reductase and platelet swelling. Blood Coagul. Fibrinolysis 2017, 28, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Kito, K.; Tanabe, K.; Sakata, K.; Fukuoka, N.; Nagase, K.; Iida, M.; Iida, H. Endothelium-dependent vasodilation in the cerebral arterioles of rats deteriorates during acute hyperglycemia and then is restored by reducing the glucose level. J. Anesth. 2018, 32, 531–538. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. Standards of medical care in diabetes-2015 abridged for primary care providers. Clin. Diabetes 2015, 33, 97–111. [Google Scholar] [CrossRef] [Green Version]
- Baldane, S.; Ipekci, S.H.; Kebapcilar, A. Relationship Between Insulin Resistance and Mean Platelet Volume in Gestational Diabetes Mellitus. J. Lab. Physicians 2015, 7, 112–115. [Google Scholar] [CrossRef]
- Voigt, M.; Gebert, M.; Haug, U.; Hulko, M.; Storr, M.; Boschetti-de-Fierro, A.; Beck, W.; Krause, B. Retention of beneficial molecules and coagulation factors during haemodialysis and haemodiafiltration. Sci. Rep. 2019, 9, 6370. [Google Scholar] [CrossRef] [Green Version]
- Esteghamat, F.; Broughton, J.S.; Smith, E.; Cardone, R.; Tyagi, T.; Guerra, M.; Szabo, A.; Ugwu, N.; Mani, M.V.; Azari, B.; et al. CELA2A mutations predispose to early-onset atherosclerosis and metabolic syndrome and affect plasma insulin and platelet activation. Nat. Genet. 2019, 51, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.C.; Liao, M.T.; Hsieh, P.S. The Dualistic Effect of COX-2-Mediated Signaling in Obesity and Insulin Resistance. Int. J. Mol. Sci. 2019, 20, 3115. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Tremaroli, V.; Schmidt, C.; Lundqvist, A.; Olsson, L.M.; Kramer, M.; Gummesson, A.; Perkins, R.; Bergstrom, G.; Backhed, F. The Gut Microbiota in Prediabetes and Diabetes: A Population-Based Cross-Sectional Study. Cell Metab. 2020, 32, 379–390e3. [Google Scholar] [CrossRef]
- Witkowski, M.; Weeks, T.L.; Hazen, S.L. Gut Microbiota and Cardiovascular Disease. Circ. Res. 2020, 127, 553–570. [Google Scholar] [CrossRef]
- Zhu, W.; Gregory, J.C.; Org, E.; Buffa, J.A.; Gupta, N.; Wang, Z.; Li, L.; Fu, X.; Wu, Y.; Mehrabian, M.; et al. Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell 2016, 165, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Nemet, I.; Saha, P.P.; Gupta, N.; Zhu, W.; Romano, K.A.; Skye, S.M.; Cajka, T.; Mohan, M.L.; Li, L.; Wu, Y.; et al. A Cardiovascular Disease-Linked Gut Microbial Metabolite Acts via Adrenergic Receptors. Cell 2020, 180, 862–877e22. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Esteve, E.; Tremaroli, V.; Khan, M.T.; Caesar, R.; Manneras-Holm, L.; Stahlman, M.; Olsson, L.M.; Serino, M.; Planas-Felix, M.; et al. Metformin alters the gut microbiome of individuals with treatment-naive type 2 diabetes, contributing to the therapeutic effects of the drug. Nat. Med. 2017, 23, 850–858. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Lippi, G. Understanding the extent of the diagnostic potential of coagulation factors. Expert Rev. Mol. Diagn 2020, 20, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Dayer, M.R.; Mard-Soltani, M.; Dayer, M.S.; Alavi, S.M. Causality relationships between coagulation factors in type 2 diabetes mellitus: Path analysis approach. Med. J. Islam Repub. Iran 2014, 28, 59. [Google Scholar] [PubMed]
- Kasthuri, R.S.; Glover, S.L.; Boles, J.; Mackman, N. Tissue factor and tissue factor pathway inhibitor as key regulators of global hemostasis: Measurement of their levels in coagulation assays. Semin. Thromb. Hemost. 2010, 36, 764–771. [Google Scholar] [CrossRef] [Green Version]
- Boden, G.; Rao, A.K. Effects of hyperglycemia and hyperinsulinemia on the tissue factor pathway of blood coagulation. Curr. Diab. Rep. 2007, 7, 223–227. [Google Scholar] [CrossRef]
- Soma, P.; Swanepoel, A.C.; Bester, J.; Pretorius, E. Tissue factor levels in type 2 diabetes mellitus. Inflamm. Res. 2017, 66, 365–368. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, S.; Mrosewski, I.; Silawal, S.; Schulze-Tanzil, G. The interrelation of osteoarthritis and diabetes mellitus: Considering the potential role of interleukin-10 and in vitro models for further analysis. Inflamm. Res. 2018, 67, 285–300. [Google Scholar] [CrossRef] [PubMed]
- Meerarani, P.; Moreno, P.R.; Cimmino, G.; Badimon, J.J. Atherothrombosis: Role of tissue factor; link between diabetes, obesity and inflammation. Indian J. Exp. Biol. 2007, 45, 103–110. [Google Scholar] [PubMed]
- Chaudhuri, J.; Bains, Y.; Guha, S.; Kahn, A.; Hall, D.; Bose, N.; Gugliucci, A.; Kapahi, P. The Role of Advanced Glycation End Products in Aging and Metabolic Diseases: Bridging Association and Causality. Cell Metab. 2018, 28, 337–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabro, P.; Cirillo, P.; Limongelli, G.; Maddaloni, V.; Riegler, L.; Palmieri, R.; Pacileo, G.; De Rosa, S.; Pacileo, M.; De Palma, R.; et al. Tissue factor is induced by resistin in human coronary artery endothelial cells by the NF-kB-dependent pathway. J. Vasc. Res. 2011, 48, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, M.; Weithauser, A.; Tabaraie, T.; Steffens, D.; Krankel, N.; Witkowski, M.; Stratmann, B.; Tschoepe, D.; Landmesser, U.; Rauch-Kroehnert, U. Micro-RNA-126 Reduces the Blood Thrombogenicity in Diabetes Mellitus via Targeting of Tissue Factor. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1263–1271. [Google Scholar] [CrossRef] [Green Version]
- Witkowski, M.; Tabaraie, T.; Steffens, D.; Friebel, J.; Dorner, A.; Skurk, C.; Witkowski, M.; Stratmann, B.; Tschoepe, D.; Landmesser, U.; et al. MicroRNA-19a contributes to the epigenetic regulation of tissue factor in diabetes. Cardiovasc. Diabetol. 2018, 17, 34. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, M.; Witkowski, M.; Saffarzadeh, M.; Friebel, J.; Tabaraie, T.; Ta Bao, L.; Chakraborty, A.; Dorner, A.; Stratmann, B.; Tschoepe, D.; et al. Vascular miR-181b controls tissue factor-dependent thrombogenicity and inflammation in type 2 diabetes. Cardiovasc. Diabetol. 2020, 19, 20. [Google Scholar] [CrossRef]
- Fu, G.; Yan, Y.; Chen, L.; Zhang, M.; Ming, L. Shortened Activated Partial Thromboplastin Time and Increased Superoxide Dismutase Levels Are Associated with Type 2 Diabetes Mellitus. Ann. Clin. Lab. Sci 2018, 48, 469–477. [Google Scholar] [PubMed]
- van der Toorn, F.A.; de Mutsert, R.; Lijfering, W.M.; Rosendaal, F.R.; van Hylckama Vlieg, A. Glucose metabolism affects coagulation factors: The NEO study. J. Thromb. Haemost. 2019. [Google Scholar] [CrossRef]
- Lallukka, S.; Luukkonen, P.K.; Zhou, Y.; Isokuortti, E.; Leivonen, M.; Juuti, A.; Hakkarainen, A.; Orho-Melander, M.; Lundbom, N.; Olkkonen, V.M.; et al. Obesity/insulin resistance rather than liver fat increases coagulation factor activities and expression in humans. Thromb. Haemost. 2017, 117, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neergaard-Petersen, S.; Hvas, A.M.; Kristensen, S.D.; Grove, E.L.; Larsen, S.B.; Phoenix, F.; Kurdee, Z.; Grant, P.J.; Ajjan, R.A. The influence of type 2 diabetes on fibrin clot properties in patients with coronary artery disease. Thromb. Haemost. 2014, 112, 1142–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul Razak, M.K.; Sultan, A.A. The importance of measurement of plasma fibrinogen level among patients with type- 2 diabetes mellitus. Diabetes Metab. Syndr. 2019, 13, 1151–1158. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Kimura, H.; Yokota, S.; Yamamoto, Y.; Hashimoto, T.; Nakagawa, M.; Ito, M.; Ogura, T. Effect of IL-6 elevation in malignant pleural effusion on hyperfibrinogenemia in lung cancer patients. Jpn. J. Clin. Oncol. 2000, 30, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Pieters, M.; van Zyl, D.G.; Rheeder, P.; Jerling, J.C.; Loots du, T.; van der Westhuizen, F.H.; Gottsche, L.T.; Weisel, J.W. Glycation of fibrinogen in uncontrolled diabetic patients and the effects of glycaemic control on fibrinogen glycation. Thromb. Res. 2007, 120, 439–446. [Google Scholar] [CrossRef] [Green Version]
- White, N.J.; Wang, Y.; Fu, X.; Cardenas, J.C.; Martin, E.J.; Brophy, D.F.; Wade, C.E.; Wang, X.; St John, A.E.; Lim, E.B.; et al. Post-translational oxidative modification of fibrinogen is associated with coagulopathy after traumatic injury. Free Radic. Biol. Med. 2016, 96, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Park, H.S.; Gu, J.Y.; Yoo, H.J.; Han, S.E.; Park, C.H.; Kim, Y.I.; Nam-Goong, I.S.; Kim, E.S.; Kim, H.K. Thrombin Generation Assay Detects Moderate-Intensity Statin-Induced Reduction of Hypercoagulability in Diabetes. Clin. Appl. Thromb. Hemost. 2018, 24, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Chitongo, P.B.; Roberts, L.N.; Yang, L.; Patel, R.K.; Lyall, R.; Luxton, R.; Aylwin, S.J.B.; Arya, R. Visceral Adiposity Is an Independent Determinant of Hypercoagulability as Measured by Thrombin Generation in Morbid Obesity. TH Open 2017, 1, e146–e154. [Google Scholar] [CrossRef] [Green Version]
- Salvagno, G.L.; Favaloro, E.J.; Demonte, D.; Gelati, M.; Poli, G.; Targher, G.; Lippi, G. Influence of hypertriglyceridemia, hyperbilirubinemia and hemolysis on thrombin generation in human plasma. Clin. Chem. Lab. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kearney, K.; Tomlinson, D.; Smith, K.; Ajjan, R. Hypofibrinolysis in diabetes: A therapeutic target for the reduction of cardiovascular risk. Cardiovasc. Diabetol. 2017, 16, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draxler, D.F.; Medcalf, R.L. The fibrinolytic system-more than fibrinolysis? Transfus. Med. Rev. 2015, 29, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Ajjan, R.A.; Gamlen, T.; Standeven, K.F.; Mughal, S.; Hess, K.; Smith, K.A.; Dunn, E.J.; Anwar, M.M.; Rabbani, N.; Thornalley, P.J.; et al. Diabetes is associated with posttranslational modifications in plasminogen resulting in reduced plasmin generation and enzyme-specific activity. Blood 2013, 122, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Canecki-Varzic, S.; Prpic-Krizevac, I.; Bilic-Curcic, I. Plasminogen activator inhibitor-1 concentrations and bone mineral density in postmenopausal women with type 2 diabetes mellitus. BMC Endocr. Disord. 2016, 16, 14. [Google Scholar] [CrossRef] [Green Version]
- Bryk, A.H.; Prior, S.M.; Plens, K.; Konieczynska, M.; Hohendorff, J.; Malecki, M.T.; Butenas, S.; Undas, A. Predictors of neutrophil extracellular traps markers in type 2 diabetes mellitus: Associations with a prothrombotic state and hypofibrinolysis. Cardiovasc. Diabetol. 2019, 18, 49. [Google Scholar] [CrossRef]
- Freeland, B. Hypoglycemia in Diabetes Mellitus. Home Healthc. Now 2017, 35, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Damle, N.A.; Passah, A.; Sharma, R.; Goyal, H.; Arunraj, S.T.; Gupta, P.; Jana, M. Tracer Accumulation in Relation to Venous Thrombus on (18)F-DOPA PET/CT in a Case of Persistent Hyperinsulinemic Hypoglycemia of Infancy. Nucl. Med. Mol. Imaging 2019, 53, 148–151. [Google Scholar] [CrossRef]
- King, R.; Ajjan, R. Hypoglycaemia, thrombosis and vascular events in diabetes. Expert Rev. Cardiovasc. Ther. 2016, 14, 1099–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, K.; Ito, T.; Nagasato, T.; Shinnakasu, A.; Kurano, M.; Arimura, A.; Arimura, H.; Hashiguchi, H.; Deguchi, T.; Maruyama, I.; et al. Effects of glycemic control and hypoglycemia on Thrombus formation assessed using automated microchip flow chamber system: An exploratory observational study. Thromb. J. 2019, 17, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joy, N.G.; Mikeladze, M.; Younk, L.M.; Tate, D.B.; Davis, S.N. Effects of equivalent sympathetic activation during hypoglycemia on endothelial function and pro-atherothrombotic balance in healthy individuals and obese standard treated type 2 diabetes. Metabolism 2016, 65, 1695–1705. [Google Scholar] [CrossRef] [Green Version]
- Chow, E.; Iqbal, A.; Walkinshaw, E.; Phoenix, F.; Macdonald, I.A.; Storey, R.F.; Ajjan, R.; Heller, S.R. Prolonged Prothrombotic Effects of Antecedent Hypoglycemia in Individuals with Type 2 Diabetes. Diabetes Care 2018, 41, 2625–2633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglay, K.; Hannachi, H.; Joseph Howie, P.; Xu, J.; Li, X.; Engel, S.S.; Moore, L.M.; Rajpathak, S. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr. Med. Res. Opin. 2016, 32, 1243–1252. [Google Scholar] [CrossRef]
- Klovaite, J.; Benn, M.; Nordestgaard, B.G. Obesity as a causal risk factor for deep venous thrombosis: A Mendelian randomization study. J. Intern. Med. 2015, 277, 573–584. [Google Scholar] [CrossRef]
- Christiansen, S.C.; Lijfering, W.M.; Naess, I.A.; Hammerstrom, J.; van Hylckama Vlieg, A.; Rosendaal, F.R.; Cannegieter, S.C. The relationship between body mass index, activated protein C resistance and risk of venous thrombosis. J. Thromb. Haemost. 2012, 10, 1761–1767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, C.W.; Kopp, H.P.; Steiner, S.; Kriwanek, S.; Krzyzanowska, K.; Bartok, A.; Roka, R.; Minar, E.; Schernthaner, G. Weight loss reduces tissue factor in morbidly obese patients. Obes. Res. 2003, 11, 950–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perego, F.; Davi, G. Beyond hyperglycemia in diabetes: Role of statin treatment on thrombogenesis triggered by inflammation: Editorial to: “Impact of statins on the coagulation status of type 2 diabetes patients evaluated by a novel thrombin-generations assay” by Ferroni, P. Cardiovasc. Drugs Ther. 2012, 26, 281–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.A.; Kim, J.E.; Song, S.H.; Kim, H.K. Influence of blood lipids on global coagulation test results. Ann. Lab. Med. 2015, 35, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Krysiak, R.; Handzlik, G.; Okopien, B. Hemostatic effects of fenofibrate in patients with mixed dyslipidemia and impaired fasting glucose. Pharmacol. Rep. 2010, 62, 1099–1107. [Google Scholar] [CrossRef]
- Verbree-Willemsen, L.; Zhang, Y.N.; Gijsberts, C.M.; Schoneveld, A.H.; Wang, J.W.; Lam, C.S.P.; Vernooij, F.; Bots, M.L.; Peelen, L.M.; Grobbee, D.E.; et al. LDL extracellular vesicle coagulation protein levels change after initiation of statin therapy. Findings from the METEOR trial. Int. J. Cardiol. 2018, 271, 247–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Kotronen, A.; Joutsi-Korhonen, L.; Sevastianova, K.; Bergholm, R.; Hakkarainen, A.; Pietilainen, K.H.; Lundbom, N.; Rissanen, A.; Lassila, R.; Yki-Jarvinen, H. Increased coagulation factor VIII, IX, XI and XII activities in non-alcoholic fatty liver disease. Liver Int. 2011, 31, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Verrijken, A.; Francque, S.; Mertens, I.; Prawitt, J.; Caron, S.; Hubens, G.; Van Marck, E.; Staels, B.; Michielsen, P.; Van Gaal, L. Prothrombotic factors in histologically proven nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology 2014, 59, 121–129. [Google Scholar] [CrossRef]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.L.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [Green Version]
- ASCEND Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar] [CrossRef]
- Alzahrani, S.H.; Ajjan, R.A. Coagulation and fibrinolysis in diabetes. Diab. Vasc. Dis. Res. 2010, 7, 260–273. [Google Scholar] [CrossRef]
- Ma, N.; Yang, Y.; Liu, X.; Li, S.; Qin, Z.; Li, J. Plasma metabonomics and proteomics studies on the anti-thrombosis mechanism of aspirin eugenol ester in rat tail thrombosis model. J. Proteom. 2020, 215, 103631. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes, A. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42 (Suppl. S1), S103–S123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antithrombotic Trialists, C.; Baigent, C.; Blackwell, L.; Collins, R.; Emberson, J.; Godwin, J.; Peto, R.; Buring, J.; Hennekens, C.; Kearney, P.; et al. Aspirin in the primary and secondary prevention of vascular disease: Collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009, 373, 1849–1860. [Google Scholar] [CrossRef] [Green Version]
- Capodanno, A.D. Antithrombotic therapy for atherosclerotic cardiovascular disease risk mitigation in patients with coronary artery disease and diabetes mellitus. Circulation 2020, 142, 17. [Google Scholar] [CrossRef]
- Morel, O.; El Ghannudi, S.; Hess, S.; Reydel, A.; Crimizade, U.; Jesel, L.; Radulescu, B.; Wiesel, M.L.; Gachet, C.; Ohlmann, P. The extent of P2Y12 inhibition by clopidogrel in diabetes mellitus patients with acute coronary syndrome is not related to glycaemic control: Roles of white blood cell count and body weight. Thromb. Haemost. 2012, 108, 338–348. [Google Scholar] [CrossRef]
- Lee, S.W.; Park, S.W.; Yun, S.C.; Kim, Y.H.; Park, D.W.; Kim, W.J.; Lee, J.Y.; Lee, C.W.; Hong, M.K.; Kim, J.J.; et al. Triple antiplatelet therapy reduces ischemic events after drug-eluting stent implantation: Drug-Eluting stenting followed by Cilostazol treatment REduces Adverse Serious cardiac Events (DECREASE registry). Am. Heart J. 2010, 159, 284–291e1. [Google Scholar] [CrossRef]
- Gresele, P.; Migliacci, R. Picotamide versus aspirin in diabetic patients with peripheral arterial disease: Has David defeated Goliath? Eur. Heart J. 2004, 25, 1769–1771. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, W.R.; Money, S.R.; Brass, E.P. Long-term safety of cilostazol in patients with peripheral artery disease: The CASTLE study (Cilostazol: A Study in Long-term Effects). J. Vasc. Surg. 2008, 47, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rishavy, M.A.; Hallgren, K.W.; Wilson, L.; Singh, S.; Runge, K.W.; Berkner, K.L. Warfarin alters vitamin K metabolism: A surprising mechanism of VKORC1 uncoupling necessitates an additional reductase. Blood 2018, 131, 2826–2835. [Google Scholar] [CrossRef]
- Makani, A.; Saba, S.; Jain, S.K.; Bhonsale, A.; Sharbaugh, M.S.; Thoma, F.; Wang, Y.; Marroquin, O.C.; Lee, J.S.; Estes, N.A.M.; et al. Safety and Efficacy of Direct Oral Anticoagulants Versus Warfarin in Patients with Chronic Kidney Disease and Atrial Fibrillation. Am. J. Cardiol. 2020, 125, 210–214. [Google Scholar] [CrossRef]
- Bansilal, S.; Bloomgarden, Z.; Halperin, J.L.; Hellkamp, A.S.; Lokhnygina, Y.; Patel, M.R.; Becker, R.C.; Breithardt, G.; Hacke, W.; Hankey, G.J.; et al. Efficacy and safety of rivaroxaban in patients with diabetes and nonvalvular atrial fibrillation: The Rivaroxaban Once-daily, Oral, Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF Trial). Am. Heart J. 2015, 170, 675–682e8. [Google Scholar] [CrossRef]
- Baker, W.L.; Beyer-Westendorf, J.; Bunz, T.J.; Eriksson, D.; Meinecke, A.K.; Sood, N.A.; Coleman, C.I. Effectiveness and safety of rivaroxaban and warfarin for prevention of major adverse cardiovascular or limb events in patients with non-valvular atrial fibrillation and type 2 diabetes. Diabetes Obes. Metab. 2019, 21, 2107–2114. [Google Scholar] [CrossRef] [PubMed]
- Rocha, B.M.L.; da Cunha, G.J.L.; Aguiar, C.M.T. A narrative review of low-dose rivaroxaban in patients with atherothrombotic cardiovascular disease: Vascular protection beyond anticoagulation. Cardiovasc. Diagn. Ther. 2021, 11, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Hylek, E.M.; Held, C.; Alexander, J.H.; Lopes, R.D.; De Caterina, R.; Wojdyla, D.M.; Huber, K.; Jansky, P.; Steg, P.G.; Hanna, M.; et al. Major bleeding in patients with atrial fibrillation receiving apixaban or warfarin: The ARISTOTLE Trial (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation): Predictors, Characteristics, and Clinical Outcomes. J. Am. Coll. Cardiol. 2014, 63, 2141–2147. [Google Scholar] [CrossRef] [Green Version]
- Brambatti, M.; Darius, H.; Oldgren, J.; Clemens, A.; Noack, H.H.; Brueckmann, M.; Yusuf, S.; Wallentin, L.; Ezekowitz, M.D.; Connolly, S.J.; et al. Comparison of dabigatran versus warfarin in diabetic patients with atrial fibrillation: Results from the RE-LY trial. Int. J. Cardiol. 2015, 196, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Markowicz-Piasecka, M.; Huttunen, K.M.; Broncel, M.; Sikora, J. Sulfenamide and Sulfonamide Derivatives of Metformin—A New Option to Improve Endothelial Function and Plasma Haemostasis. Sci. Rep. 2019, 9, 6573. [Google Scholar] [CrossRef] [Green Version]
- Witkowski, M.; Friebel, J.; Tabaraie, T.; Grabitz, S.; Dorner, A.; Taghipour, L.; Jakobs, K.; Stratmann, B.; Tschoepe, D.; Landmesser, U.; et al. Metformin Is Associated with Reduced Tissue Factor Procoagulant Activity in Patients with Poorly Controlled Diabetes. Cardiovasc. Drugs Ther. 2020. [Google Scholar] [CrossRef] [PubMed]
- Khanolkar, M.P.; Morris, R.H.; Thomas, A.W.; Bolusani, H.; Roberts, A.W.; Geen, J.; Jackson, S.K.; Evans, L.M. Rosiglitazone produces a greater reduction in circulating platelet activity compared with gliclazide in patients with type 2 diabetes mellitus—An effect probably mediated by direct platelet PPARgamma activation. Atherosclerosis 2008, 197, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.B.; Temprosa, M.G.; Mather, K.J.; Orchard, T.J.; Kitabchi, A.E.; Watson, K.E.; Diabetes Prevention Program Research Group. Lifestyle and metformin interventions have a durable effect to lower CRP and tPA levels in the diabetes prevention program except in those who develop diabetes. Diabetes Care 2014, 37, 2253–2260. [Google Scholar] [CrossRef] [Green Version]
- Verdoia, M.; Pergolini, P.; Rolla, R.; Ceccon, C.; Caputo, M.; Aimaretti, G.; Suryapranata, H.; De Luca, G. Use of Metformin and Platelet Reactivity in Diabetic Patients Treated with Dual Antiplatelet Therapy. Exp. Clin. Endocrinol. Diabetes 2018. [Google Scholar] [CrossRef] [PubMed]
- Pal, P.; Kanaujiya, J.K.; Lochab, S.; Tripathi, S.B.; Sanyal, S.; Behre, G.; Trivedi, A.K. Proteomic analysis of rosiglitazone and guggulsterone treated 3T3-L1 preadipocytes. Mol. Cell Biochem. 2013, 376, 81–93. [Google Scholar] [CrossRef]
- Henriksson, C.E.; Hellum, M.; Haug, K.B.; Aass, H.C.; Joo, G.B.; Ovstebo, R.; Troseid, A.M.; Klingenberg, O.; Kierulf, P. Anticoagulant effects of an antidiabetic drug on monocytes in vitro. Thromb. Res. 2011, 128, e100–e106. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Kiwanuka, E.; Zanetti, M.; Cristini, M.; Vettore, M.; Tessari, P. Insulin acutely increases fibrinogen production in individuals with type 2 diabetes but not in individuals without diabetes. Diabetes 2003, 52, 1851–1856. [Google Scholar] [CrossRef] [Green Version]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barale, C.; Buracco, S.; Cavalot, F.; Frascaroli, C.; Guerrasio, A.; Russo, I. Glucagon-like peptide 1-related peptides increase nitric oxide effects to reduce platelet activation. Thromb. Haemost. 2017, 117, 1115–1128. [Google Scholar] [CrossRef] [Green Version]
- Simeone, P.; Liani, R.; Tripaldi, R.; Di Castelnuovo, A.; Guagnano, M.T.; Tartaro, A.; Bonadonna, R.C.; Federico, V.; Cipollone, F.; Consoli, A.; et al. Thromboxane-Dependent Platelet Activation in Obese Subjects with Prediabetes or Early Type 2 Diabetes: Effects of Liraglutide- or Lifestyle Changes-Induced Weight Loss. Nutrients 2018, 10, 1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Tanaka, A.; Shimabukuro, M.; Machii, N.; Teragawa, H.; Okada, Y.; Shima, K.R.; Takamura, T.; Taguchi, I.; Hisauchi, I.; Toyoda, S.; et al. Effect of Empagliflozin on Endothelial Function in Patients with Type 2 Diabetes and Cardiovascular Disease: Results from the Multicenter, Randomized, Placebo-Controlled, Double-Blind EMBLEM Trial. Diabetes Care 2019, 42, e159–e161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uthman, L.; Homayr, A.; Juni, R.P.; Spin, E.L.; Kerindongo, R.; Boomsma, M.; Hollmann, M.W.; Preckel, B.; Koolwijk, P.; van Hinsbergh, V.W.M.; et al. Empagliflozin and Dapagliflozin Reduce ROS Generation and Restore NO Bioavailability in Tumor Necrosis Factor alpha-Stimulated Human Coronary Arterial Endothelial Cells. Cell Physiol. Biochem. 2019, 53, 865–886. [Google Scholar] [CrossRef]
- Sakurai, S.; Jojima, T.; Iijima, T.; Tomaru, T.; Usui, I.; Aso, Y. Empagliflozin decreases the plasma concentration of plasminogen activator inhibitor-1 (PAI-1) in patients with type 2 diabetes: Association with improvement of fibrinolysis. J. Diabetes Complicat. 2020, 34, 107703. [Google Scholar] [CrossRef]
- Bray, G.A.; Fruhbeck, G.; Ryan, D.H.; Wilding, J.P. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef] [Green Version]
- Stolberg, C.R.; Mundbjerg, L.H.; Funch-Jensen, P.; Gram, B.; Juhl, C.B.; Bladbjerg, E.M. Effects of gastric bypass followed by a randomized study of physical training on markers of coagulation activation, fibrin clot properties, and fibrinolysis. Surg. Obes. Relat. Dis. 2018, 14, 918–926. [Google Scholar] [CrossRef]
- Gram, A.S.; Petersen, M.B.; Quist, J.S.; Rosenkilde, M.; Stallknecht, B.; Bladbjerg, E.M. Effects of 6 Months of Active Commuting and Leisure-Time Exercise on Fibrin Turnover in Sedentary Individuals with Overweight and Obesity: A Randomised Controlled Trial. J. Obes. 2018, 2018, 7140754. [Google Scholar] [CrossRef]
- Teng, K.T.; Chang, L.F.; Vethakkan, S.R.; Nesaretnam, K.; Sanders, T.A.B. Effects of exchanging carbohydrate or monounsaturated fat with saturated fat on inflammatory and thrombogenic responses in subjects with abdominal obesity: A randomized controlled trial. Clin. Nutr. 2017, 36, 1250–1258. [Google Scholar] [CrossRef] [Green Version]
- Horber, S.; Lehmann, R.; Fritsche, L.; Machann, J.; Birkenfeld, A.L.; Haring, H.U.; Stefan, N.; Heni, M.; Fritsche, A.; Peter, A. Lifestyle intervention improves prothrombotic coagulation profile in individuals at high-risk for type 2 diabetes. J. Clin. Endocrinol. Metab. 2021. [Google Scholar] [CrossRef]
- Toso, A.; De Servi, S.; Leoncini, M.; Angiolillo, D.J.; Calabro, P.; Piscione, F.; Cattaneo, M.; Maffeo, D.; Bartorelli, A.; Palmieri, C.; et al. Effects of statin therapy on platelet reactivity after percutaneous coronary revascularization in patients with acute coronary syndrome. J. Thromb. Thrombolysis 2017, 44, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Undas, A.; Celiniska-Lowenhoff, M. Antiplatelet effects of micronized fenofibrate in subjects with dyslipidemia. Pol. Arch. Med. Wewn 2007, 117, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Mobarrez, F.; He, S.; Broijersen, A.; Wiklund, B.; Antovic, A.; Antovic, J.; Egberg, N.; Jorneskog, G.; Wallen, H. Atorvastatin reduces thrombin generation and expression of tissue factor, P-selectin and GPIIIa on platelet-derived microparticles in patients with peripheral arterial occlusive disease. Thromb. Haemost. 2011, 106, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Paciullo, F.; Momi, S.; Gresele, P. PCSK9 in Haemostasis and Thrombosis: Possible Pleiotropic Effects of PCSK9 Inhibitors in Cardiovascular Prevention. Thromb. Haemost. 2019, 119, 359–367. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Agent | Alterations in Coagulation-Fibrinolysis System |
|---|---|
| Metformin | tPA ↓[83]; platelet aggregation↓[84]; TF ↓[97] |
| Thiazolidinediones | fibrinogen↓; PAI-1↓[101] ; platelet aggregation↓[98] |
| Sulphonylureas | TF↓[102] |
| Insulin | platelet aggregation↓[18]; fibrinogen↑; PAI-1↑[103] |
| GLP-1RA | platelet aggregation↓[105]; NO↑[106] |
| SGLT-2i’s | NO↑[109]; PAI-1↓[110] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Weber, N.C.; Cohn, D.M.; Hollmann, M.W.; DeVries, J.H.; Hermanides, J.; Preckel, B. Effects of Hyperglycemia and Diabetes Mellitus on Coagulation and Hemostasis. J. Clin. Med. 2021, 10, 2419. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112419
Li X, Weber NC, Cohn DM, Hollmann MW, DeVries JH, Hermanides J, Preckel B. Effects of Hyperglycemia and Diabetes Mellitus on Coagulation and Hemostasis. Journal of Clinical Medicine. 2021; 10(11):2419. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112419
Chicago/Turabian StyleLi, Xiaoling, Nina C. Weber, Danny M. Cohn, Markus W. Hollmann, J. Hans DeVries, Jeroen Hermanides, and Benedikt Preckel. 2021. "Effects of Hyperglycemia and Diabetes Mellitus on Coagulation and Hemostasis" Journal of Clinical Medicine 10, no. 11: 2419. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112419