
Usefulness of Respiratory Mechanics and Laboratory Parameter Trends as Markers of Early Treatment Success in Mechanically Ventilated Severe Coronavirus Disease: A Single-Center Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statements
2.2. Study Design, Setting, and Population
2.3. Management of Coronavirus Disease
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Outcomes
3.2. Ventilatory and Laboratory Parameters and Liberation from Mechanical Ventilation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda, A.; Suzuki, K.; Endo, M.; et al. Clinical epidemiology of hospitalized patients with COVID-19 in Japan: Report of the COVID-19 Registry Japan. Clin. Infect. Dis. 2020, ciaa1470. [Google Scholar] [CrossRef] [PubMed]
- Miike, S.; Sakamoto, N.; Washino, T.; Kosaka, A.; Kuwahara, Y.; Ishida, T.; Hikone, M.; Oyabu, T.; Kojima, H.; Iwabuchi, S.; et al. Critically ill patients with COVID-19 in Tokyo, Japan: A single-center case series. J. Infect. Chemother. 2020, 27, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Japan ECMOnet for COVID-19; Shime, N. Save the ICU and save lives during the COVID-19 pandemic. J. Intensive Care 2020, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Piroth, L.; Cottenet, J.; Mariet, A.S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: A nationwide, population-based retrospective cohort study. Lancet Respir. Med. 2020, 9, 251–259. [Google Scholar] [CrossRef]
- Alicandro, G.; Remuzzi, G.; La Vecchia, C. Italy’s first wave of the COVID-19 pandemic has ended: No excess mortality in May, 2020. Lancet 2020, 396, e27–e28. [Google Scholar] [CrossRef]
- Vanhorebeek, I.; Latronico, N.; Van den Berghe, G. ICU-acquired weakness. Intensive Care Med. 2020, 46, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, C.; Suarez-Sipmann, F.; Mellado-Artigas, R.; Hernández, M.; Gea, A.; Arruti, E.; Aldecoa, S.; Martinez-Palli, G.; Marintez-Gonzalez, M.A.; Slutsky, A.S.; et al. Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. 2020, 46, 2200–2211. [Google Scholar] [CrossRef]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Beenen, L.F.M.; Bos, L.D.; Scheerder, M.J.; Lobé, N.H.J.; Muller, M.C.A.; Schultz, M.J.; van den Aardweg, J.G.; Goorhuis, A.; Bonta, P.I.; Middledorp, S.; et al. Extensive pulmonary perfusion defects compatible with microthrombosis and thromboembolic disease in severe Covid-19 pneumonia. Thromb. Res. 2020, 196, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Gamberini, L.; Tonetti, T.; Spadaro, S.; Zani, G.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Bacchi Reggiani, M.L.; Bertellini, E.; Castelli, A.; et al. Factors influencing liberation from mechanical ventilation in coronavirus disease 2019: Multicenter observational study in fifteen Italian ICUs. J. Intensive Care 2020, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578, Erratum in 2020, 395, 1694. [Google Scholar] [CrossRef]
- Sato, R.; Ishikane, M.; Kinoshita, N.; Suzuki, T.; Nakamoto, T.; Hayakawa, K.; Bekki, N.; Hara, H.; Ohmagari, N. A new challenge of unfractionated heparin anticoagulation treatment for moderate to severe COVID-19 in Japan. Glob. Health Med. 2020, 2, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Nishio, N.; Hiramatsu, M.; Goto, Y.; Shindo, Y.; Yamamoto, T.; Jingushi, N.; Wakahara, K.; Sone, M. Surgical strategy and optimal timing of tracheostomy in patients with COVID-19: Early experiences in Japan. Auris Nasus Larynx 2020, 48, 518–524. [Google Scholar] [CrossRef]
- Iida, Y.; Iwata, K.; Uchiyama, Y.; Utsunomiya, A.; Endo, S.; Kasai, F.; Kato, M.; Kubo, T.; Kojima, N.; Sasanuma, N.; et al. Q&A on Rehabilitation Medicine for COVID-19 Patients in ICU. The Japanese Society of Intensive Care Medicine. Available online: https://www.jsicm.org/news/upload/COVID-19_rehab_qa_v1.pdf (accessed on 10 January 2021).
- Liu, X.; Liu, X.; Xu, Y.; Xu, Z.; Huang, Y.; Chen, S.; Li, S.; Liu, D.; Lin, Z.; Li, Y. Ventilatory Ratio in Hypercapnic Mechanically Ventilated Patients with COVID-19-associated Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 201, 1297–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, P.; Singh, S.; Hardman, J.G.; Bersten, A.D.; Soni, N.; Australia and New Zealand Intensive Care Society Clinical Trials Group. Evaluation of the physiological properties of ventilatory ratio in a computational cardiopulmonary model and its clinical application in an acute respiratory distress syndrome population. Br. J. Anaesth. 2014, 112, 96–101. [Google Scholar] [CrossRef] [Green Version]
- Doiron, K.A.; Hoffmann, T.C.; Beller, E.M. Early intervention (mobilization or active exercise) for critically ill adults in the intensive care unit. Cochrane Database Syst. Rev. 2018, 3, CD010754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Saez de Asteasu, M.L.; Lucia, A.; Galbete, A.; Garcia-Baztan, A.; Alonso-Remedo, J.; Gonzalez-Glaria, B.; Gonzalo-Lozaro, M.; et al. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients During Acute Hospitalization: A Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 28–36, Erratum in 2019, 179, 127. [Google Scholar] [CrossRef]
- Davis, S.D.; Rosenfeld, M.; Lee, H.S.; Ferkol, T.W.; Sagel, S.D.; Dell, S.D.; Milla, C.; Pittman, J.E.; Shapiro, A.J.; Sullivan, K.M.; et al. Primary Ciliary Dyskinesia: Longitudinal Study of Lung Disease by Ultrastructure Defect and Genotype. Am. J. Respir. Crit. Care Med. 2019, 199, 190–198. [Google Scholar] [CrossRef]
- Yang, T.; Li, Z.; Jiang, L.; Wang, Y.; Xi, X. Risk factors for intensive care unit-acquired weakness: A systematic review and meta-analysis. Acta Neurol. Scand. 2018, 138, 104–114. [Google Scholar] [CrossRef]
- Martini, K.; Blüthgen, C.; Walter, J.E.; Nguyen-Kim, T.D.L.; Thienemann, F.; Frauenfelder, T. Patterns of organizing pneumonia and microinfarcts as surrogate for endothelial disruption and microangiopathic thromboembolic events in patients with coronavirus disease 2019. PLoS ONE 2020, 15, e0240078. [Google Scholar] [CrossRef]
- Hasan, S.S.; Radford, S.; Know, C.S.; Zaidi, S.T.R. Venous thromboembolism in critically ill COVID-19 patients receiving prophylactic or therapeutic anticoagulation: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2020, 50, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Risitano, A.M.; Mastellos, D.C.; Huber-Lang, M.; Yancopoulou, D.; Garlanda, C.; Ciceri, F.; Lambris, J.D. Complement as a target in COVID-19? Nat. Rev. Immunol. 2020, 20, 343–344, Erratum in 2020, 20, 448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skendros, P.; Mitsios, A.; Chrysanthopoulou, A.; Mastellos, D.C.; Metallidis, S.; Rafailidis, P.; Nitinopoulou, M.; Sertaridou, E.; Tsironidou, V.; Tsigalou, C.; et al. Complement and tissue factor-enriched neutrophil extracellular traps are key drivers in COVID-19 immunothrombosis. J. Clin. Investig. 2020, 130, 6151–6157. [Google Scholar] [CrossRef] [PubMed]
- d’Alessandro, M.; Cameli, P.; Refini, R.M.; Bergantini, L.; Alonzi, V.; Lanzarone, N.; Bennett, D.; Rana, G.D.; Montagnani, F.; Scolletta, S.; et al. Serum KL-6 concentrations as a novel biomarker of severe COVID-19. J. Med. Virol. 2020, 92, 2216–2220. [Google Scholar] [CrossRef]
- Kory, P.; Kanne, J.P. SARS-CoV-2 organising pneumonia: ‘Has there been a widespread failure to identify and treat this prevalent condition in COVID-19?’. BMJ Open Respir. Res. 2020, 7, e000724. [Google Scholar] [CrossRef] [PubMed]
- Copin, M.C.; Parmentier, E.; Duburcq, T.; Poissy, J.; Mathieu, D.; Lille COVID-19 ICU and Anatomopathology Group. Time to consider histologic pattern of lung injury to treat critically ill patients with COVID-19 infection. Intensive Care Med. 2020, 46, 1124–1126. [Google Scholar] [CrossRef] [Green Version]
- Flikweert, A.W.; Grootenboers, M.J.J.H.; Yick, D.C.Y.; du Mée, A.W.F.; van der Meer, N.J.M.; Rettig, T.C.D.; Kant, M.K.M. Late histopathologic characteristics of critically ill COVID-19 patients: Different phenotypes without evidence of invasive aspergillosis, a case series. J. Crit. Care 2020, 59, 149–155. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef]
- Avilés-Jurado, F.X.; Prieto-Alhambra, D.; González-Sánchez, N.; de Ossó, J.; Arancibia, C.; Rojas-Lechuga, M.J.; Ruiz-Sevilla, L.; Remacha, R.; Sanchez, I.; Lehrer-Coriat, E.; et al. Timing, Complications, and Safety of Tracheotomy in Critically Ill Patients With COVID-19. JAMA Otolaryngol. Head Neck Surg. 2020, 147, 1–8. [Google Scholar] [CrossRef]
- Sutt, A.L.; Tronstad, O.; Barnett, A.G.; Kitchenman, S.; Fraser, J.F. Earlier tracheostomy is associated with an earlier return to walking, talking, and eating. Aust. Crit. Care 2020, 33, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, V.; Siempos, I.; Magira, E.; Kokkoris, S.; Zakynthinos, G.E.; Zakynthinos, S. PEEP levels in COVID-19 pneumonia. Crit. Care 2020, 24, 303. [Google Scholar] [CrossRef]
- Roesthuis, L.; van den Berg, M.; van der Hoeven, H. Advanced respiratory monitoring in COVID-19 patients: Use less PEEP! Crit. Care 2020, 24, 230. [Google Scholar] [CrossRef] [PubMed]
- Beloncle, F.M.; Pavlovsky, B.; Desprez, C.; Fage, N.; Olivier, P.Y.; Asfar, P.; Richard, J.C.; Mercat, A. Recruitability and effect of PEEP in SARS-Cov-2-associated acute respiratory distress syndrome. Ann. Intensive Care 2020, 10, 55. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Patients (31) | Early Liberation from MV | p Value | |
|---|---|---|---|---|
| Success (20) | Failure (11) | |||
| Age, years, median (IQR) | 71 (64–76) | 71 (64–77) | 70 (56–73) | 0.535 |
| Male sex, n (%) | 25 (81) | 17 (85) | 8(73) | 0.546 |
| BMI (kg/m2), median (IQR) | 24.5 (21.8–28.5) | 25.2 (21.5–28.5) | 23.2 (22.4– 30.2) | 0.67 |
| Comorbidities, n, median (IQR) | 1 (1–2) | 1 (1–2) | 2 (1–2) | 0.118 |
| HT, n (%) | 11 (35) | 6 (30) | 5 (45) | 0.452 |
| DM, n (%) | 18 (58) | 10 (50) | 8 (73) | 0.275 |
| Chronic heart failure, n (%) | 3 (9.6) | 1 (5) | 2 (18) | 0.281 |
| End-stage renal disease, n (%) | 5 (16) | 2 (10) | 3 (27) | 0.317 |
| Cancer, n (%) | 2 (6.4) | 1 (5) | 1 (9.1) | >0.99 |
| Chronic pulmonary disease, n (%) | 2 (6.4) | 1 (5) | 1 (9.1) | >0.99 |
| Dementia, n (%) | 3 (9.6) | 3 (15) | 0 (0) | 0.535 |
| 4C mortality score, median (IQR) | 12 (11–14) | 12 (11–13) | 12 (11–14) | 0.707 |
| SOFA score, median (IQR) | 7 (6–10) | 7 (5–10) | 7 (6–10) | 0.802 |
| APACHE II score, median (IQR) | 13 (11–19) | 13 (11–19) | 15 (11–19) | 0.521 |
| Parameters at the time of MV | ||||
| PaO2/FiO2 ratio | 96 (82–114) | 85 (81–114) | 101 (89–113) | 0.47 |
| Static compliance, mL/cmH2O, median (IQR) | 38 (33–42) | 38 (34–43) | 38 (33–39) | 0.614 |
| Ventilatory ratio, median (IQR) | 1.26 (1.17–1.41) | 1.24 (1.17–1.32) | 1.38 (1.18–1.58) | 0.119 |
| PEEP, cmH2O | 11 (10–14) | 10 (10–12) | 14 (10–15) | |
| NMB, n (%) | 5 (16) | 4 (20) | 1 (9.1) | |
| Prone positioning, n (%) | 13 (42) | 7 (35) | 6 (55) | 0.477 |
| D-dimer level, μg/mL, median (IQR) | 2.31 (1.52–4.54) | 1.63 (1.09–4.18) | 3.36 (2.35–10.1) | 0.132 |
| Treatment | ||||
| Anti-viral, n (%) | ||||
| Favipiravir | 15 (48) | 8 (40) | 7 (64) | |
| Remdesivir | 16 (52) | 13 (65) | 3 (27) | |
| Steroid, n (%) | 26 (84) | 19 (95) | 7 (64) | 0.0416 |
| Initial antibacterial drug, n (%) | 21 (68) | 14 (70) | 7 (64) | >0.99 |
| Tracheostomy, n (%) | 7 (23) | 0 (0) | 7 (64) | <0.001 |
| Duration of mechanical ventilation (days), median (IQR) | 10 (5–20) | 6 (4–9) | 24 (20–30) | <0.001 |
| ICU stay, median (IQR) | 12 (10–20) | 11 (8–12) | 27 (21–36) | <0.001 |
| In-hospital mortality, n (%) | 2 (6.5) | 1 (5) | 1 (9.1) | >0.99 |
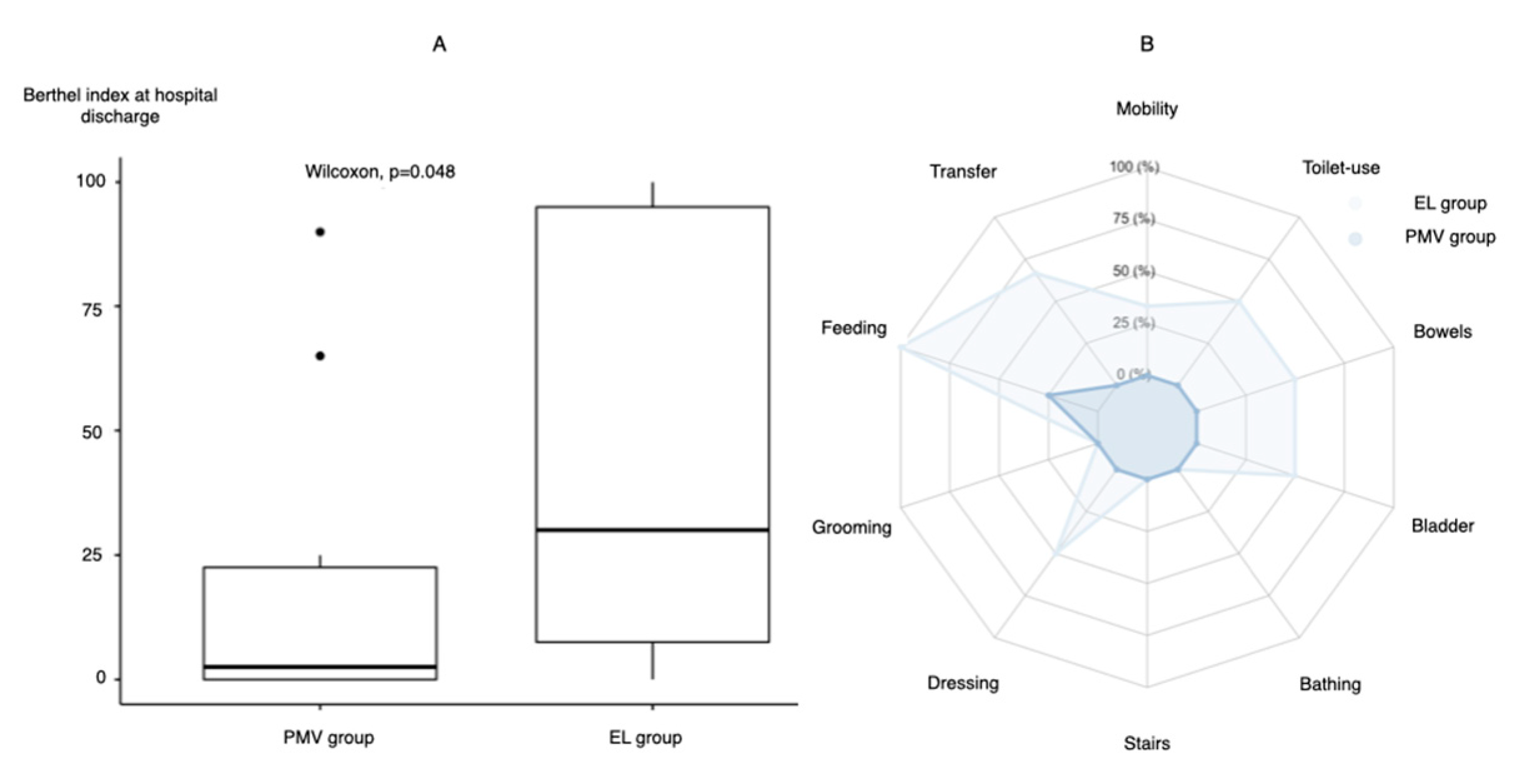
| Barthel index at discharge, median (IQR) | 20 (0–65) | 30 (7.5–95) | 2.5 (0–22.5) | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasugai, D.; Ozaki, M.; Nishida, K.; Hiraiwa, H.; Jingushi, N.; Numaguchi, A.; Omote, N.; Shindo, Y.; Goto, Y. Usefulness of Respiratory Mechanics and Laboratory Parameter Trends as Markers of Early Treatment Success in Mechanically Ventilated Severe Coronavirus Disease: A Single-Center Pilot Study. J. Clin. Med. 2021, 10, 2513. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112513
Kasugai D, Ozaki M, Nishida K, Hiraiwa H, Jingushi N, Numaguchi A, Omote N, Shindo Y, Goto Y. Usefulness of Respiratory Mechanics and Laboratory Parameter Trends as Markers of Early Treatment Success in Mechanically Ventilated Severe Coronavirus Disease: A Single-Center Pilot Study. Journal of Clinical Medicine. 2021; 10(11):2513. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112513
Chicago/Turabian StyleKasugai, Daisuke, Masayuki Ozaki, Kazuki Nishida, Hiroaki Hiraiwa, Naruhiro Jingushi, Atsushi Numaguchi, Norihito Omote, Yuichiro Shindo, and Yukari Goto. 2021. "Usefulness of Respiratory Mechanics and Laboratory Parameter Trends as Markers of Early Treatment Success in Mechanically Ventilated Severe Coronavirus Disease: A Single-Center Pilot Study" Journal of Clinical Medicine 10, no. 11: 2513. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112513