
Efficacy of Empiric Antibiotic Coverage in Community-Acquired Pneumonia Associated with Each Atypical Bacteria: A Meta-Analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection Criteria
2.2. Outcomes, Data Analysis, and Risk of Bias
3. Results
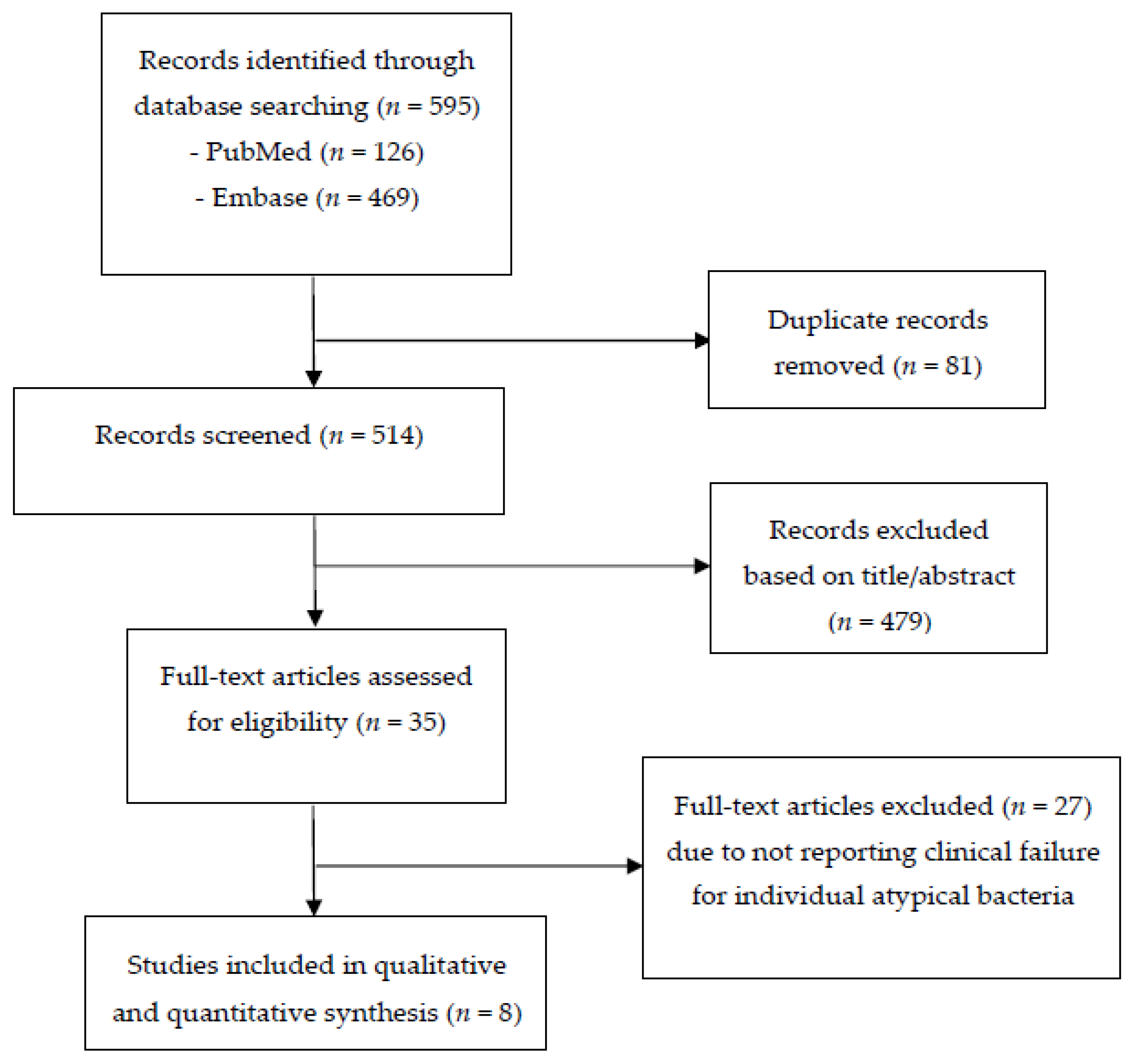
3.1. Search Results and Study Characteristics
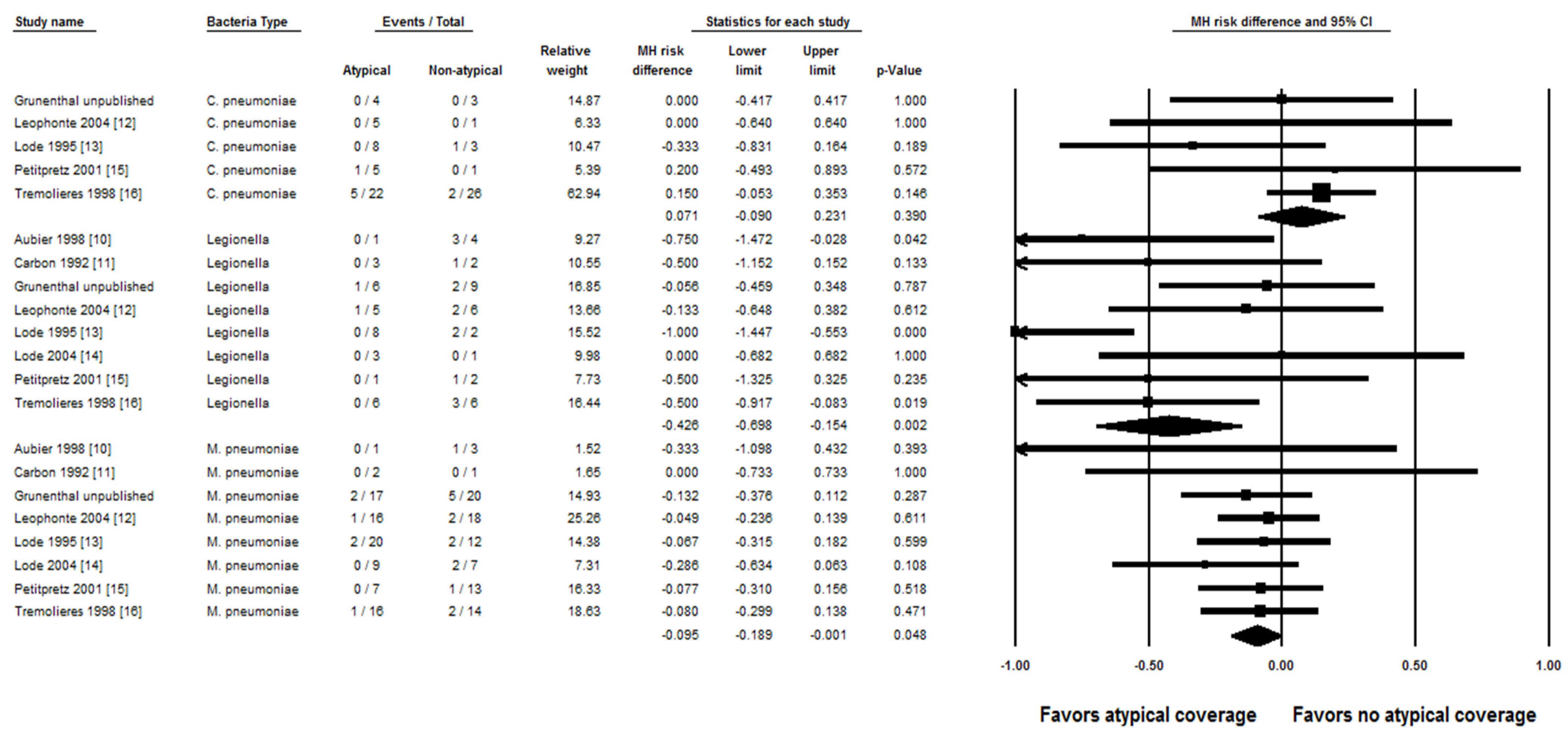
3.2. Study Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Database/Search Dates | Search Strategy |
|---|---|
| PubMed/MEDLINE, National Library of Medicine (Searched until 21 March 2021) | #1-“Macrolides”[Mesh] OR “Fluoroquinolones”[Mesh] OR |
| “Doxycycline”[Mesh] | |
| #2-“beta-Lactams”[Mesh] | |
| #3-pneumonia[Mesh] | |
| #4-#1 AND #2 AND #3 AND “randomized controlled trial”[Publication Type] | |
| Embase, Elsevier (Searched until 21 March 2021) | #1-‘macrolide’/exp OR ‘quinoline derived antiinfective agent’/exp OR |
| ‘doxycycline’/exp | |
| #2-‘beta lactam antibiotic’/exp | |
| #3-‘pneumonia’/exp | |
| #4-#1 AND #2 AND #3 AND [randomized controlled trial]/lim |
References
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Pneumonia in Adults: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/cg191 (accessed on 23 July 2019).
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; et al. Guidelines for the management of adult lower respiratory tract infections—Summary. Clin. Microbiol. Infect. 2011, 17 (Suppl. 6), 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, F.W.; Summersgill, J.T.; Ramirez, J.A. Role of Atypical Pathogens in the Etiology of Community-Acquired Pneumonia. Semin. Respir. Crit. Care Med. 2016, 37, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.L.; Hu, B.J.; He, L.X.; Wei, L.; Xie, H.M.; Wang, B.Q.; Li, H.Y.; Chen, X.H.; Zhou, C.M.; Deng, W.W. Etiology and antimicrobial resistance of community-acquired pneumonia in adult patients in China. Chin. Med. J. 2012, 125, 2967–2972. [Google Scholar] [PubMed]
- Eljaaly, K.; Alshehri, S.; Aljabri, A.; Abraham, I.; Al Mohajer, M.; Kalil, A.C.; Nix, D.E. Clinical failure with and without empiric atypical bacteria coverage in hospitalized adults with community-acquired pneumonia: A systematic review and meta-analysis. BMC Infect. Dis. 2017, 17, 385. [Google Scholar] [CrossRef] [Green Version]
- Thabit, A.K.; Crandon, J.L.; Nicolau, D.P. Antimicrobial resistance: Impact on clinical and economic outcomes and the need for new antimicrobials. Expert Opin. Pharmacother. 2015, 16, 159–177. [Google Scholar] [CrossRef]
- Eljaaly, K.; Botaish, A.; Bahobail, F.; Almehmadi, M.; Assabban, Z.; Thabit, A.K.; Alraddadi, B.; Aljabri, A.; Alqahtani, N.; Aseeri, M.A.; et al. Systematic review and meta-analysis of the safety of erythromycin compared to clarithromycin in adults and adolescents with pneumonia. J. Chemother. 2020, 32, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Eljaaly, K.; Alshehri, S.; Bhattacharjee, S.; Al-Tawfiq, J.A.; Patanwala, A.E. Contraindicated drug-drug interactions associated with oral antimicrobial agents prescribed in the ambulatory care setting in the United States. Clin. Microbiol. Infect. 2019, 25, 620–622. [Google Scholar] [CrossRef] [Green Version]
- Aubier, M.; Verster, R.; Regamey, C.; Geslin, P.; Vercken, J.B. Once-daily sparfloxacin versus high-dosage amoxicillin in the treatment of community-acquired, suspected pneumococcal pneumonia in adults. Clin. Infect. Dis. 1998, 26, 1312–1320. [Google Scholar] [CrossRef] [Green Version]
- Carbon, C.; Léophonte, P.; Petitpretz, P.; Chauvin, J.P.; Hazebroucq, J. Efficacy and safety of temafloxacin versus those of amoxicillin in hospitalized adults with community-acquired pneumonia. Antimicrob. Agents Chemother. 1992, 36, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Léophonte, P.; File, T.; Feldman, C. Gemifloxacin once daily for 7 days compared to amoxicillin/clavulanic acid thrice daily for 10 days for the treatment of community-acquired pneumonia of suspected pneumococcal origin. Respir. Med. 2004, 98, 708–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lode, H.; Garau, J.; Grassi, C.; Hosie, J.; Huchon, G.; Legakis, N.; Segev, S.; Wijnands, G. Treatment of community-acquired pneumonia: A randomized comparison of sparfloxacin, amoxycillin-clavulanic acid and erythromycin. Eur. Respir. J. 1995, 8, 1999–2007. [Google Scholar] [CrossRef] [PubMed]
- Lode, H.; Magyar, P.; Muir, J.F.; Loos, U.; Kleutgens, K.; International Gatifloxacin Study Group. Once-daily oral gatifloxacin vs three-times-daily co-amoxiclav in the treatment of patients with community-acquired pneumonia. Clin. Microbiol. Infect. 2004, 10, 512–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petitpretz, P.; Arvis, P.; Marel, M.; Moita, J.; Urueta, J.; CAP5 Moxifloxacin Study Group. Oral moxifloxacin vs high-dosage amoxicillin in the treatment of mild-to-moderate, community-acquired, suspected pneumococcal pneumonia in adults. Chest 2001, 119, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Trémolières, F.; de Kock, F.; Pluck, N.; Daniel, R. Trovafloxacin versus high-dose amoxicillin (1 g three times daily) in the treatment of community-acquired bacterial pneumonia. Eur. J. Clin. Microbiol. Infect. Dis. 1998, 17, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Postma, D.F.; van Werkhoven, C.H.; van Elden, L.J.; Thijsen, S.F.; Hoepelman, A.I.; Kluytmans, J.A.; Boersma, W.G.; Compaijen, C.J.; van der Wall, E.; Prins, J.M.; et al. Antibiotic treatment strategies for community-acquired pneumonia in adults. N. Engl. J. Med. 2015, 372, 1312–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farnham, A.; Alleyne, L.; Cimini, D.; Balter, S. Legionnaires’ disease incidence and risk factors, New York, New York, USA, 2002–2011. Emerg. Infect. Dis. 2014, 20, 1795–1802. [Google Scholar] [CrossRef]
- CDC. Centres for Disease Control and Prevention: Mycoplasma Pneumoniae Infections. Available online: https://www.cdc.gov/pneumonia/atypical/mycoplasma/about/people-at-risk.html (accessed on 11 January 2021).
- Sharma, L.; Losier, A.; Tolbert, T.; Dela Cruz, C.S.; Marion, C.R. Atypical Pneumonia: Updates on Legionella, Chlamydophila, and Mycoplasma Pneumonia. Clin. Chest Med. 2017, 38, 45–58. [Google Scholar] [CrossRef] [Green Version]
- McCracken, G.H., Jr. Current status of antibiotic treatment for Mycoplasma pneumoniae infections. Pediatr. Infect. Dis. 1986, 5, 167–171. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M.; Musher, D.M., Jr.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef] [PubMed]


| Study | Study Period | Design | Location | Funding Source (Manufactured Drug) | Legionella spp. | M. Pneumoniae | C. Pneumoniae | Characteristics of Community-Acquired Pneumonia | Atypical vs. Non-Atypical Regimen | Duration of Therapy (Days) |
|---|---|---|---|---|---|---|---|---|---|---|
| Aubier 1998 [10] | 1991–1992 | Superiority, double-blind, RCT | 55 sites in 3 countries (Europe, South Africa) | Non-industry | 1 vs. 4 | 1 vs. 3 | NA | Hospitalized, mild–moderate | Sparfloxacin PO 400 mg q24h, then 200 mg q24h vs. amoxicillin 1 g PO q24h | 10–14 |
| Carbon 1992 [11] | 1989–1990 | Superiority, double-blind, RCT | 27 sites in France | Industry (temafloxacin) | 3 vs. 2 | 2 vs. 1 | NA | Hospitalized, mild–moderate | Temafloxacin 600 mg PO q12h vs. amoxicillin 500 mg PO q8h | 10 |
| Leophonte 2004 [12] | 1998–1999 | Superiority, double-blind, RCT | 102 sites in 3 countries (Europe, South Africa) | Industry (gemifloxacin) | 5 vs. 6 | 16 vs. 18 | 5 vs. 1 | >90% hospitalized, suspected pneumococcal mild–moderate | Gemifloxacin 320 mg PO q24h vs. amoxicillin/clav 1.2 g PO q8h | 7 vs. 10 |
| Lode 1995 [13] | 1990–1992 | Superiority, double-blind, RCT | 124 sites in 9 countries (Europe, Israel) | Industry (sparfloxacin) | 8 vs. 2 | 20 vs. 12 | 8 vs. 3 | Hospitalized and outpatients, mild–moderate | Sparfloxacin PO 400 mg once, then 200 mg q24h or erythromycin 1 g PO q12h vs. amoxicillin/clav 625 mg PO q8h | 7–14 |
| Lode 2004 [14] | 1997–1998 | Superiority, double-blind, RCT | 73 sites in 16 countries (mostly Europe) | Industry (gatifloxacin) | 3 vs. 1 | 9 vs. 7 | NA | Hospitalized, mild–moderate | Gatifloxacin 400 mg PO q24h vs. amoxicillin/clav 625 mg PO q8h | 5–10 |
| Petitpretz 2001 [15] | 1997–1998 | Superiority, double-blind, RCT | 82 sites in 20 countries (Europe, South America, Australia, Africa) | Industry (moxifloxacin) | 1 vs. 2 | 7 vs. 13 | 5 vs. 1 | 79% hospitalized, mild–moderate | Moxifloxacin 400 mg PO q24h vs. amoxicillin 1 g PO q8h | 10 |
| Tremolieres 1998 [16] | 1995–1996 | Superiority, double-blind, RCT | 44 sites in Europe, South Africa, Costa Rica | Industry (trovafloxacin) | 6 vs. 6 | 16 vs. 14 | 22 vs. 26 | 75% hospitalized, any severity | Trovafloxacin 200 mg PO q24h vs. amoxicillin 1 g PO q8h | 7–10 |
| Grunenthal 2000 (unpublished; KF5501/16) | 1999–2000 | Superiority, double-blind, RCT | 132 sites, multinational | Industry (gatifloxacin) | 6 vs. 9 | 17 vs. 20 | 4 vs. 3 | Hospitalized, any severity | Gatifloxacin 400 mg PO q24h vs. amoxicillin 1 g PO q8h | 7–10 |
| Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | ||
|---|---|---|---|---|---|---|---|
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
| Aubier 1998 [10] | ? | ? | + | + | − | + | + |
| Carbon 1992 [11] | ? | ? | + | + | − | + | − |
| Leophonte 2004 [12] | ? | ? | + | + | − | − | ? |
| Lode 1995 [13] | ? | ? | + | + | + | + | ? |
| Lode 2004 [14] | + | + | + | + | + | + | ? |
| Petitpretz 2001 [15] | + | + | + | + | − | + | ? |
| Tremolieres 1998 [16] | ? | ? | + | + | + | + | ? |
| Grunenthal 2000 (unpublished; KF5501/16) | ? | ? | + | + | + | + | ? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eljaaly, K.; Aljabri, A.; Rabaan, A.A.; Aljuhani, O.; Thabit, A.K.; Alshibani, M.; Almangour, T.A. Efficacy of Empiric Antibiotic Coverage in Community-Acquired Pneumonia Associated with Each Atypical Bacteria: A Meta-Analysis. J. Clin. Med. 2021, 10, 4321. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194321
Eljaaly K, Aljabri A, Rabaan AA, Aljuhani O, Thabit AK, Alshibani M, Almangour TA. Efficacy of Empiric Antibiotic Coverage in Community-Acquired Pneumonia Associated with Each Atypical Bacteria: A Meta-Analysis. Journal of Clinical Medicine. 2021; 10(19):4321. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194321
Chicago/Turabian StyleEljaaly, Khalid, Ahmed Aljabri, Ali A. Rabaan, Ohoud Aljuhani, Abrar K. Thabit, Mohannad Alshibani, and Thamer A. Almangour. 2021. "Efficacy of Empiric Antibiotic Coverage in Community-Acquired Pneumonia Associated with Each Atypical Bacteria: A Meta-Analysis" Journal of Clinical Medicine 10, no. 19: 4321. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194321