
Prognostic Value of Pulmonary Artery Pulsatility Index in Right Ventricle Failure-Related Mortality in Inoperable Chronic Thromboembolic Pulmonary Hypertension

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Right Heart Catheterization and Pulmonary Angiography
2.3. Echocardiography
2.4. Risk Stratification
2.5. Statistical Analysis
3. Results
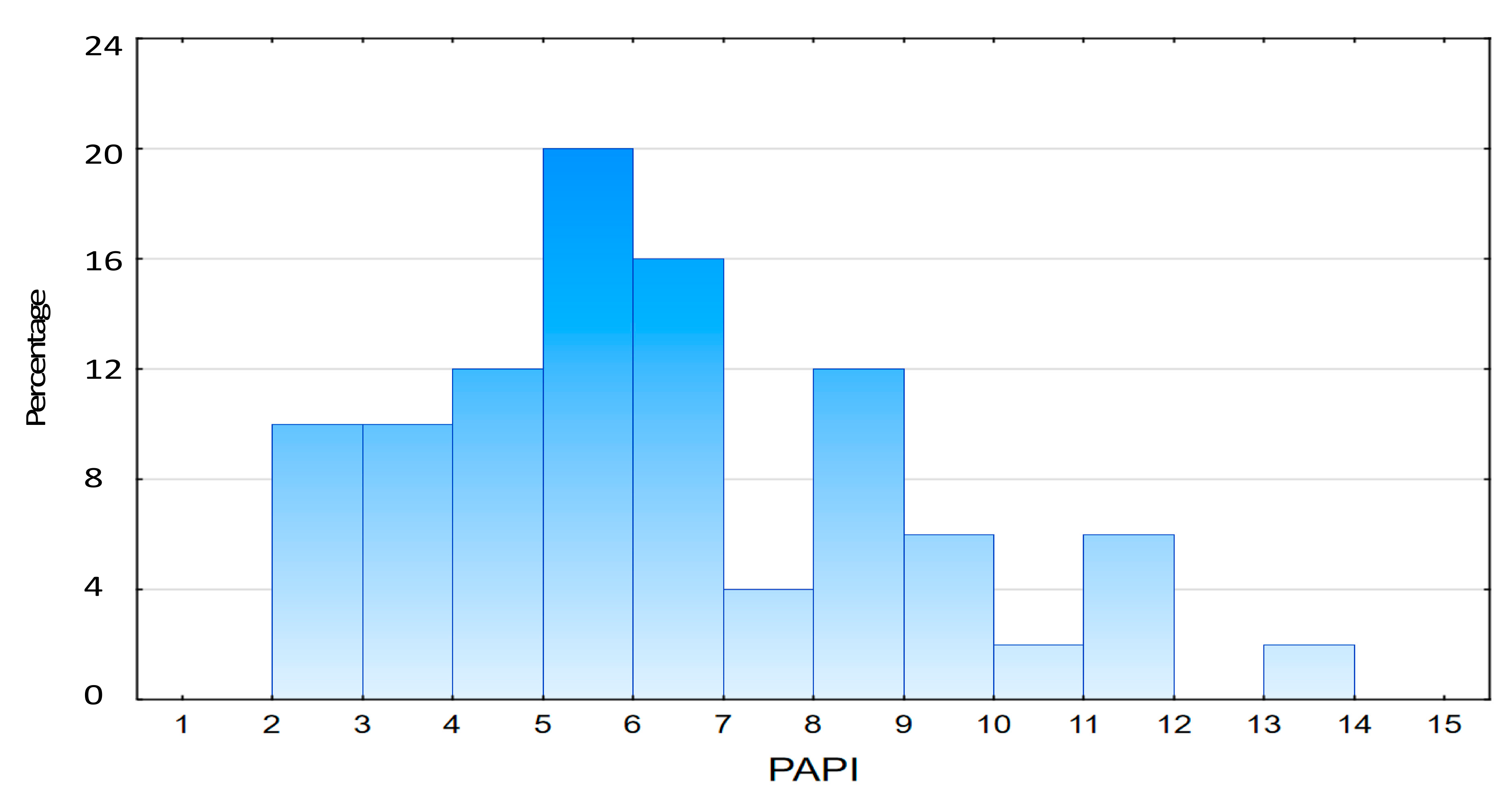
3.1. Study Population
3.2. Risk Categorization Based on Pulmonary Artery Pulsatility Index
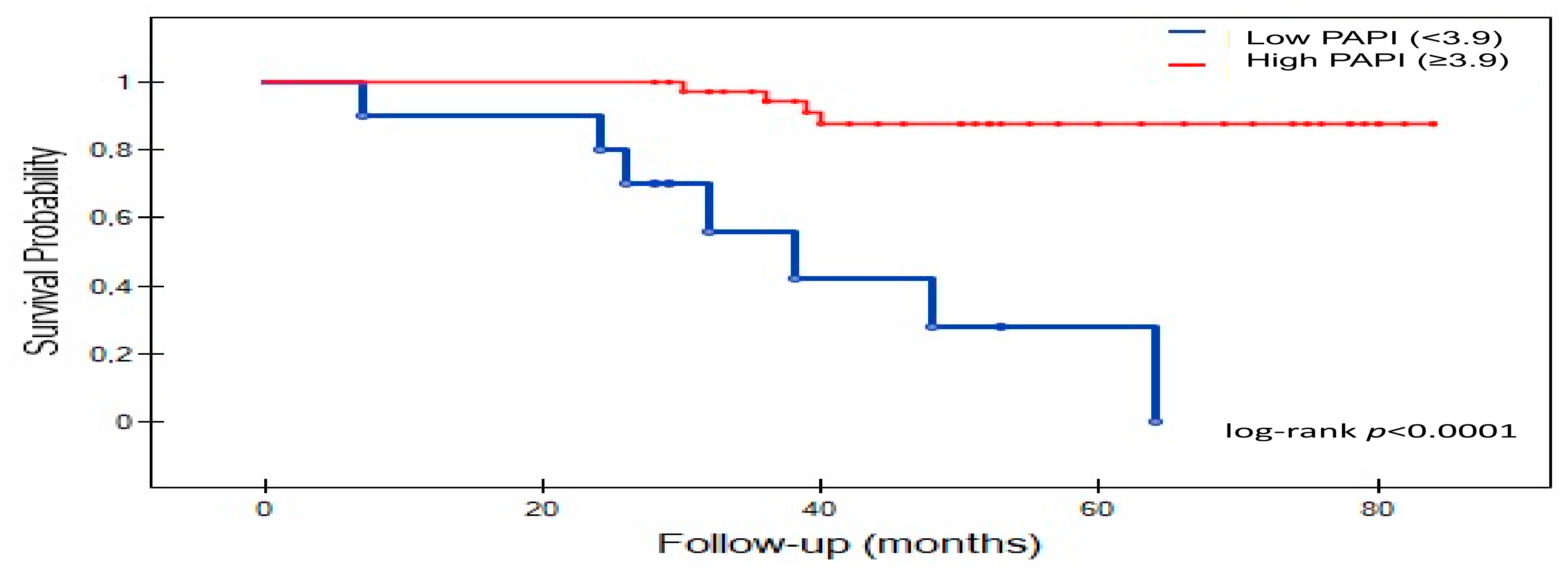
3.3. Survival Analysis
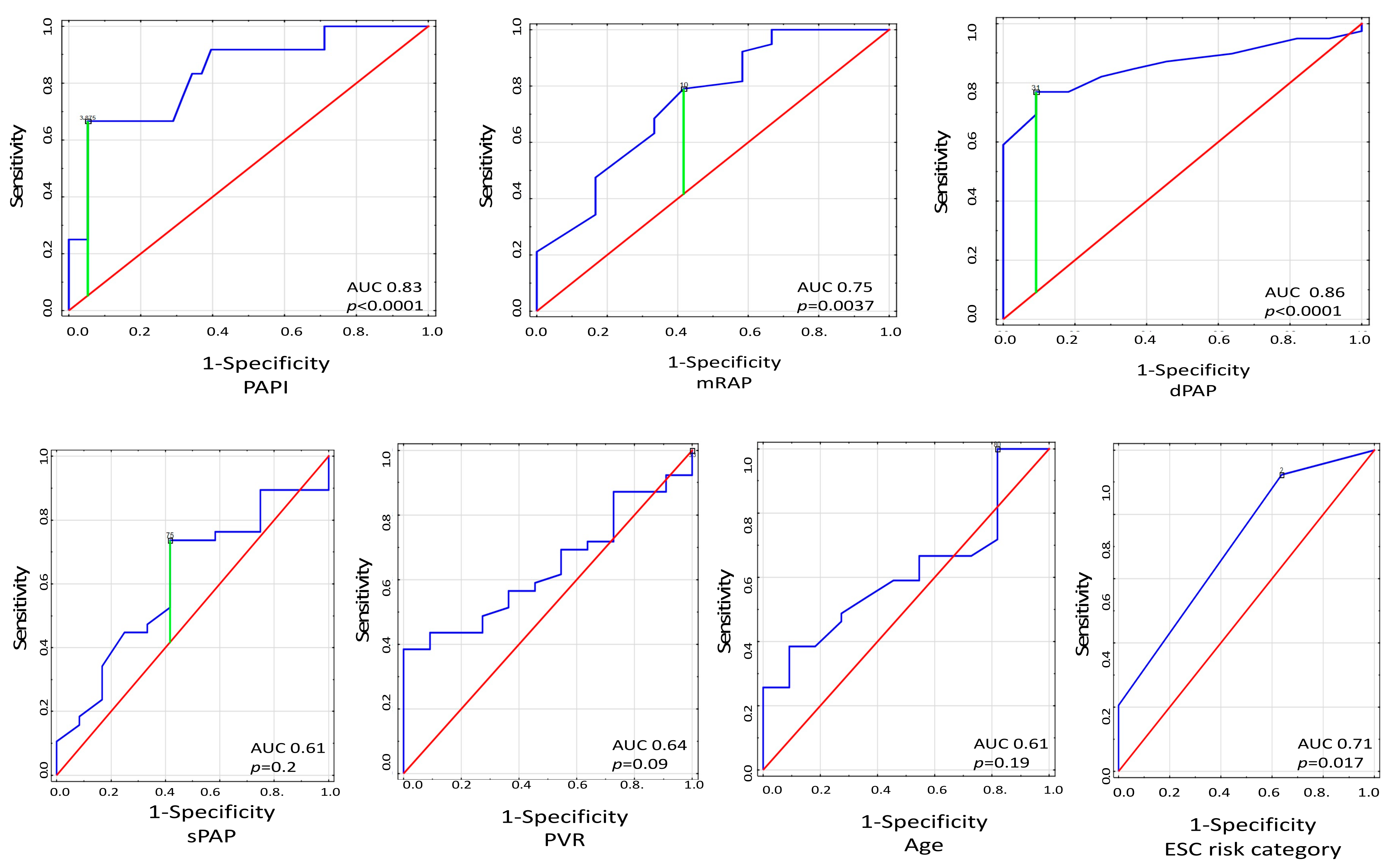
3.4. Mortality Risk Assessment
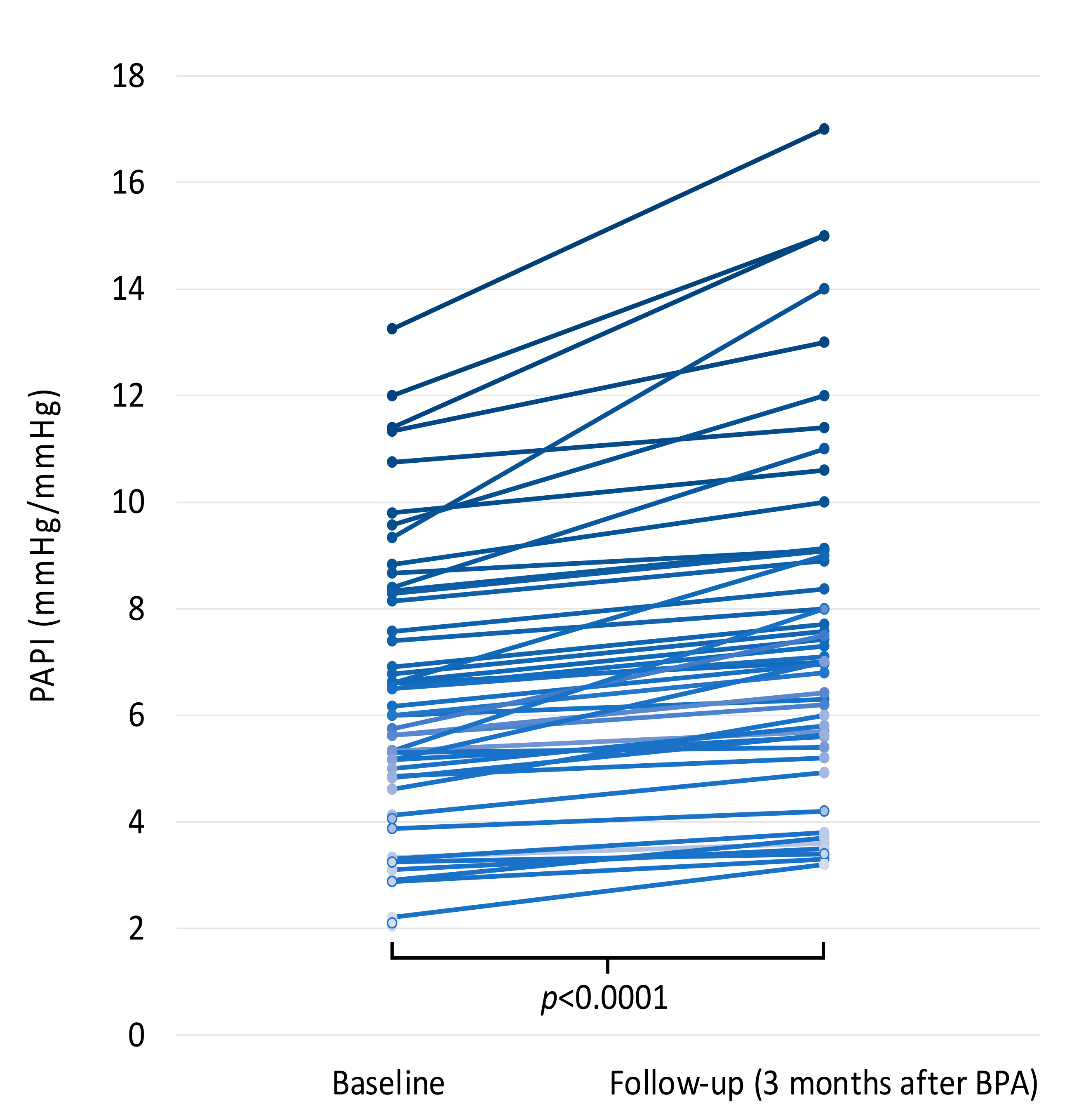
3.5. Change in PAPI Values after Interventional Treatment of CTEPH
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruaro, B.; Baratella, E.; Caforio, G.; Confalonieri, P.; Wade, B.; Marrocchio, C.; Geri, P.; Pozzan, R.; Andrisano, A.G.; Assunta Cova, M.; et al. Chronic Thromboembolic Pulmonary Hypertension: An Update. Diagnostics 2022, 12, 235. [Google Scholar] [CrossRef]
- Pepke-Zaba, J.; Delcroix, M.; Lang, I.; Mayer, E.; Jansa, P.; Ambroz, D.; Treacy, C.; D’Armini, A.M.; Morsolini, M.; Snijder, R.; et al. Chronic thromboembolic pulmonary hypertension (CTEPH): Results from an international prospective registry. Circulation 2011, 124, 1973–1981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopeć, G.; Dzikowska-Diduch, O.; Mroczek, E.; Mularek-Kubzdela, T.; Chrzanowski, Ł.; Skoczylas, I.; Tomaszewski, M.; Peregud-Pogorzelska, M.; Karasek, D.; Lewicka, E.; et al. Characteristics and outcomes of patients with chronic thromboembolic pulmonary hypertension in the era of modern therapeutic approaches: Data from the Polish multicenter registry (BNP-PL). Adv. Chronic. Dis. 2021, 12, 20406223211002961. [Google Scholar] [CrossRef] [PubMed]
- Jansa, P.; Heller, S.; Svoboda, M.; Pad’our, M.; Ambrož, D.; Dytrych, V.; Širanec, M.; Kovárník, T.; Felšőci, M.; Hutyra, M.; et al. Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension: Impact on Clinical and Hemodynamic Parameters, Quality of Life and Risk Profile. J. Clin. Med. 2020, 9, 3608. [Google Scholar] [CrossRef]
- Kataoka, M.; Inami, T.; Kawakami, T.; Fukuda, K.; Satoh, T. Balloon Pulmonary Angioplasty (Percutaneous Transluminal Pulmonary Angioplasty) for Chronic Thromboembolic Pulmonary Hypertension: A Japanese Perspective. JACC Cardiovasc. Interv. 2019, 12, 1382–1388. [Google Scholar] [CrossRef]
- Araszkiewicz, A.; Darocha, S.; Pietrasik, A.; Pietura, R.; Jankiewicz, S.; Banaszkiewicz, M.; Sławek-Szmyt, S.; Biederman, A.; Mularek-Kubzdelaa, T.; Lesiak, M.; et al. Balloon pulmonary angioplasty for the treatment of residual or recurrent pulmonary hypertension after pulmonary endarterectomy. Int. J. Cardiol. 2019, 278, 232–237. [Google Scholar] [CrossRef]
- Darocha, S.; Roik, M.; Kopeć, G.; Araszkiewicz, A.; Furdal, M.; Lewandowski, M.; Jacheć, W.; Grabka, M.; Banaszkiewicz, M.; Pietrasik, A.; et al. Balloon Pulmonary Angioplasty in Chronic Thromboembolic Pulmonary Hypertension: A Multicenter Registry. EuroIntervention 2022, 17, 1104–1111. [Google Scholar] [CrossRef]
- Darocha, S.; Araszkiewicz, A.; Kurzyna, M.; Banaszkiewicz, M.; Jankiewicz, S.; Dobosiewicz, A.; Sławek-Szmyt, S.; Janus, M.; Grymuza, M.; Pietrasik, A.; et al. Balloon Pulmonary Angioplasty in Technically Operable and Technically Inoperable Chronic Thromboembolic Pulmonary Hypertension. J. Clin. Med. 2021, 10, 1038. [Google Scholar] [CrossRef]
- Mizoguchi, H.; Ogawa, A.; Munemasa, M.; Mikouchi, H.; Ito, H.; Matsubara, H. Refined balloon pulmonary angioplasty for inoperable patients with chronic thromboembolic pulmonary hypertension. Circ. Cardiovasc. Interv. 2012, 5, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Ghofrani, H.A.; D’Armini, A.M.; Grimminger, F.; Hoeper, M.M.; Jansa, P.; Kim, N.H.; Mayer, E.; Simonneau, G.; Wilkins, M.R.; Fritsch, A.; et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N. Engl. J. Med. 2013, 369, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Simonneau, G.; D’Armini, A.M.; Ghofrani, H.A.; Grimminger, F.; Hoeper, M.M.; Jansa, P.; Kim, N.H.; Wang, C.; Wilkins, M.R.; Fritschet, A.; et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension: A long-term extension study (CHEST-2). Eur. Respir. J. 2015, 45, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Siennicka, A.; Darocha, S.; Banaszkiewicz, M.; Kędzierski, P.; Dobosiewicz, A.; Błaszczak, P.; Peregud-Pogorzelska, M.; Kasprzak, J.D.; Tomaszewski, M.; Mroczek, E.; et al. Treatment of chronic thromboembolic pulmonary hypertension in a multidisciplinary team. Adv. Respir. Dis. 2019, 13, 1753466619891529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galieè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, S.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The joint task force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [PubMed]
- Delcroix, M.; Staehler, G.; Gall, H.; Grünig, E.; Held, M.; Halank, M.; Klose, H.; Vonk-Noordegraaf, A.; Rosenkranz, S.; Pepke-Zaba, J.; et al. Risk assessment in medically treated chronic thromboembolic pulmonary hypertension patients. Eur. Respir. J. 2018, 52, 1800248. [Google Scholar] [CrossRef] [PubMed]
- Sandqvist, A.; Kylhammar, D.; Bartfay, S.E.; Hesselstrand, R.; Hjalmarsson, C.; Kavianipour, M.; Nisell, M.; Rådegran, G.; Wikström, G.; Kjellström, B.; et al. Risk stratification in chronic thromboembolic pulmonary hypertension predicts survival. Scand. Cardiovasc. J. 2021, 55, 43–49. [Google Scholar] [CrossRef]
- Simonneau, G.; D’Armini, A.M.; Ghofrani, H.A.; Grimminger, F.; Jansa, P.; Kim, N.H.; Mayer, E.; Pulido, T.; Wang, C.; Colorado, P.; et al. Predictors of long-term outcomes in patients treated with riociguat for chronic thromboembolic pulmonary hypertension: Data from the CHEST-2 open-label, randomised, long-term extension trial. Lancet Respir. Med. 2016, 4, 372–380. [Google Scholar] [CrossRef]
- Korabathina, R.; Heffernan, K.S.; Paruchuri, V.; Patel, A.R.; Mudd, J.O.; Prutkin, J.M.; Orr, N.M.; Weintraub, A.; Kimmelstiel, C.D.; Kapur, N.K.; et al. The pulmonary artery pulsatility index identifies severe right ventricular dysfunction in acute inferior myocardial infarction. Catheter. Cardiovasc. Interv. 2012, 80, 593–600. [Google Scholar] [CrossRef]
- Kang, G.; Ha, R.; Banerjee, D. Pulmonary artery pulsatility index predicts right ventricular failure after left ventricular assist device implantation. J. Heart Lung Transpl. 2016, 35, 67–73. [Google Scholar] [CrossRef]
- Lim, Y.; Low, T.T.; Chan, S.P.; Lin, W.; Teo, T.W.; Jang, J.J.; Kuntjoro, I.; Tay, E.L.-W.; Yip, J.W.-L. Does pulmonary artery pulsatility index predict mortality in pulmonary arterial hypertension? ESC Heart Fail. 2021, 8, 3835–3844. [Google Scholar] [CrossRef]
- Kurzyna, M.; Araszkiewicz, A.; Błaszczak, P.; Grabka, M.; Hawranek, M.; Kopeć, G.; Mroczek, E.; Zembala, M.; Torbicki, A.; Ochała, A. Summary of recommendations for the haemodynamic and angiographic assessment of the pulmonary circulation. Joint statement of the Polish Cardiac Society’s Working Group on Pulmonary Circulation and Association of Cardiovascular Interventions. Kardiol. Pol. 2015, 73, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Sławek-Szmyt, S.; Araszkiewicz, A.; Jankiewicz, S.; Smukowska-Gorynia, A.; Grygier, M.; Janus, M.; Lesiak, M.; Mularek-Kubzdela, T. Association of Electrocardiographic Signs of Right Ventricular Hypertrophy and Clot Localization in Chronic Thromboembolic Pulmonary Hypertension. J. Clin. Med. 2022, 11, 625. [Google Scholar] [CrossRef] [PubMed]
- Thistlethwaite, P.A.; Mo, M.; Madani, M.M.; Deutsch, R.; Blanchard, D.; Kapelanski, D.P.; Jamieson, S.W. Operative classification of thromboembolic disease determines outcome after pulmonary endarterectomy. J. Thorac. Cardiovasc. Surg. 2002, 124, 1203–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kass, G.V. An exploratory technique for investigating large quantities of categorical data. Appl. Stat. 1980, 29, 119–127. [Google Scholar] [CrossRef]
- Mazimba, S.; Ginn, G.; Mwansa, H.; Laja, O.; Jeukeng, C.; Elumogo, C.; Patterson, B.; Kennedy, J.L.W.; Mehta, N.; Hossack, J.A.; et al. Pulmonary Artery Proportional Pulse Pressure (PAPP) Index Identifies Patients With Improved Survival From the CardioMEMS Implantable Pulmonary Artery Pressure Monitor. Heart Lung Circ. 2021, 30, 1389–1396. [Google Scholar] [CrossRef]
- Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Paruchuri, V.; Denofrio, D.; Kapur, N.K. Pulmonary Artery Pulsatility Index Is Associated With Right Ventricular Failure After Left Ventricular Assist Device Surgery. J. Card. Fail. 2016, 22, 110–116. [Google Scholar] [CrossRef]
- Kochav, S.M.; Flores, R.J.; Truby, L.K.; Topkara, V.K. Prognostic Impact of Pulmonary Artery Pulsatility Index (PAPi) in Patients With Advanced Heart Failure: Insights From the ESCAPE Trial. J Card. Fail. 2018, 24, 453–459. [Google Scholar] [CrossRef]
- Raymer, D.S.; Moreno, J.D.; Sintek, M.A.; Nassif, M.E.; Sparrow, C.T.; Adamo, L.; Novak, E.L.; LaRue, S.J.; Vader, J.M. The Combination of Tricuspid Annular Plane Systolic Excursion and HeartMate Risk Score Predicts Right Ventricular Failure After Left Ventricular Assist Device Implantation. ASAIO J. 2019, 65, 247–251. [Google Scholar] [CrossRef]
- Lim, Y.; Low, T.T.; Chan, S.P.; Teo, T.W.; Jang, J.J.; Yip, N.; Kuntjoro, I.; Tay, E.L.; Yip, J.W. Pulmonary arterial hypertension in a multi-ethnic Asian population: Charac- teristics, survival and mortality predic- tors from a 14-year follow-up study. Respirology 2019, 24, 162–170. [Google Scholar] [CrossRef]
- Saouti, N.; de Man, F.; Westerhof, N.; Boonstra, A.; Twisk, J.; Postmus, P.E.; Vonk Noordegraaf, A. Predictors of mortality in inoperable chronic thromboembolic pulmonary hypertension. Respir Med. 2009, 103, 1013–1019. [Google Scholar] [CrossRef] [Green Version]
- Miwa, H.; Tanabe, N.; Jujo, T.; Kato, F.; Anazawa, R.; Yamamoto, K.; Naito, A.; Kasai, H.; Nishimura, R.; Suda, R.; et al. Long-Term Outcome of Chronic Thromboembolic Pulmonary Hypertension at a Single Japanese Pulmonary Endarterectomy Center. Circ. J. 2018, 82, 1428–1436. [Google Scholar] [CrossRef] [Green Version]
- Naeije, R.; Vachiery, J.L.; Yerly, P.; Vanderpool, R. The transpulmonary pressure gradient for the diagnosis of pulmonary vascular disease. Eur. Respir. J. 2013, 41, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Gerges, C.; Gerges, M.; Lang, M.B.; Zhang, Y.; Jakowitsch, J.; Probst, P.; Maurer, G.; Lang, I.M. Diastolic pulmonary vascular pressure gradient: A predictor of prognosis in “out-of-proportion: Pulmonary hypertension. Chest 2013, 143, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Apitz, C.; Berger, R.M.F.; Ivy, D.D.; Humpl, T.; Bonnet, D.; Beghetti, M.; Schranz, D.; Latus, H. Hemodynamic and prognostic impact of the diastolic pulmonary arterial pressure in children with pulmonary arterial hypertension-a registry-based analysis. Cardiovasc. Diagn. Ther. 2021, 11, 1037–1047. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All N = 50, (%) | Low PAPI (<3.9) N = 10 (%) | High PAPI (≥3.9) N = 40 (%) | p-Value |
|---|---|---|---|---|
| Age (years), mean (SD) | 64 (12.2) | 63.4 (7.0) | 64.3 (13.3) | 0.78 |
| Sex | 0.72 | |||
| female | 30 (60) | 6 (60) | 24 (60) | |
| male | 20 (40) | 4 (40) | 16 (40) | |
| BMI (kg/m2) | 29.3 (7.0) | 33.8 (5.3) | 28.2 (7.1) | 0.0066 |
| WHO FC | 0.0017 | |||
| I | - | - | - | |
| II | 9 (18) | - | 9 (22.5) | |
| III | 28 (56) | 3 (30) | 25 (62.5) | |
| IV | 12 (24) | 7 (70) | 5 (12.5) | |
| Previous pulmonary embolism | 0.14 | |||
| yes | 34 (68) | 9 (90) | 25 (62.5) | |
| no | 16 (32) | 1 (10) | 15 (37.5) | |
| Coronary artery disease | 10 (20) | 3 (30) | 7 (17.5) | 0.41 |
| Chronic obstructive pulmonary disease | 7 (14) | 2 (20) | 5 (12.5) | 0.62 |
| Diabetes mellitus | 11 (22) | 4 (40) | 7 (17.5) | 0.2 |
| Systemic arterial hypertension | 35 (70) | 8 (80) | 27 (67.5) | 0.7 |
| Known thrombophilia | 2 (4) | - | 2 (5) | 0.77 |
| Chronic renal insufficiency | 11 (22) | 5 (50) | 6 (15) | 0.03 |
| Anticoagulation therapy | ||||
| DOAC | 33 (66) | 6 (60) | 27 (67.5) | 0.72 |
| VKA | 17 (34) | 4 (40) | 13 (32.5) | 0.72 |
| 6MWD (m), mean (SD) | 308.2 (120) | 236.2 (108.5) | 328.2 (116.3) | 0.03 |
| NT-proBNP (pg/mL), mean (SD) | 2296.4 (2939) | 1566.8 (794.8) | 2483.4 (3254.2) | 0.51 |
| ESC 2015 risk category | 0.1 | |||
| low (1) | 8 (16) | - | 8 (20) | |
| intermediate (2) | 35 (70) | 7 (70) | 28 (70) | |
| high (3) | 7 (14) | 3 (30) | 4 (10) |
| Parameter Mean (SD) | All N = 50 | Low PAPI (<3.9) N = 10 | High PAPI (≥3.9) N = 40 | p-Value |
|---|---|---|---|---|
| Hemodynamic data | ||||
| sSAP (mmHg) | 143.8 (26) | 139.5 (26.8) | 144.9 (26.1) | 0.57 |
| dSAP (mmHg) | 85 (17.6) | 77.6 (31.5) | 87.5 (11.7) | 0.22 |
| mRAP (mmHg) | 9.2 (4.6) | 14.9 (4.4) | 7.8 (2.8) | 0.0001 |
| sRVP (mmHg) | 78 (17.3) | 71.2 (18.5) | 79.7 (16.8) | 0.17 |
| dRVP (mmHg) | 6.0 (5.6) | 9.2 (4.9) | 5.2 (4.1) | 0.018 |
| edRVP (mmHg) | 12.3 (5.1) | 16.5 (4.6) | 11.2 (4.7) | 0.004 |
| sPAP (mmHg) | 79.7 (15.3) | 79.1 (12.4) | 79.9 (16.4) | 0.089 |
| dPAP (mmHg) | 29.3 (7.4) | 35.8 (5.3) | 27.7 (7.0) | 0.0012 |
| mPAP (mmHg) | 48.1 (9.2) | 50.9 (8.5) | 47.5 (9.4) | 0.30 |
| PAWP (mmHg) | 10.1 (2.9) | 11.2 (2.8) | 9.9 (2.9) | 0.066 |
| PAPI (mmHg/mmHg) | 6.4 (2.7) | 3.0 (0.8) | 7.2 (2.3) | < 0.0001 |
| PVR (Wood units) | 7.2 (3.2) | 6.12 (2.5) | 7.5 (3.3) | 0.31 |
| SVR (Wood units) | 18 (7.0) | 15 (6.2) | 18.8 (7.1) | 0.67 |
| CO (L/min) | 5.8 (1.6) | 5.6 (1.5) | 6.5 (1.7) | 0.10 |
| CI (L/min/m2) | 3.1 (0.75) | 3.0 (0.75) | 3.3 (0.78) | 0.36 |
| SV (mL) | 76.6 (24.5) | 70.7 (33.1) | 78 (22.1) | 0.4 |
| SvO2 (%) | 67.6 (6.3) | 66.5 (5.6) | 67.9 (6.5) | 0.55 |
| SaO2 (%) | 91.6 (3.6) | 90.7 (4.12) | 91.8 (3.4) | 0.5 |
| Echocardiographic data | ||||
| RAA (cm2) | 27.4 (9.5) | 34.3 (11.1) | 25.7 (8.3) | 0.026 |
| RV free wall thickness (mm) | 5.4 (0.9) | 6 (0.7) | 4.8 (1.1) | 0.1 |
| RV end-diastolic diameter (4 ch) (mm) | 48.6 (9.6) | 52.2 (10.1) | 47.7 (9.4) | 0.21 |
| TAPSE (mm) | 19 (4.9) | 16.4 (4.0) | 19.6 (8.5) | 0.57 |
| TRV max (m/s) | 4.4 (0.6) | 4.12 (0.43) | 4.46 (0.61) | 0.1 |
| TVPG (mmHg) | 82 (20.5) | 71 (16.5) | 85 (20.7) | 0.21 |
| Tricuspid regurgitation severity n (%) | 0.9 | |||
| Mild | 5 (10) | - | 5 (12.5) | |
| Moderate | 40 (80) | 8 (80) | 32 (80) | |
| Severe | 5 (10) | 1 (10) | 4 (10) | |
| Pulmonary trunk diameter (mm) | 30.2 (5.7) | 34.3 (2.1) | 29.6 (5.8) | 0.026 |
| S’ wave (cm/s) | 12.02 (3.4) | 11.4 (4.3) | 12.2 (3.2) | 0.56 |
| Univariate Cox Proportional Analysis | Multivariable Cox Proportional Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value |
| PAPI (per 1 unit) | 0.48 | 0.32–0.72 | 0.0004 | 0.65 | 0.44–0.96 | 0.03 |
| 6MWD (per 1 m) | 0.99 | 0.98–0.99 | 0.002 | 0.99 | 0.98–0.99 | 0.018 |
| RAA (per 1 cm2) | 1.1 | 1.04–1.17 | 0.001 | 1.07 | 1.00–1.15 | 0.03 |
| mRAP (per 1 mmHg) | 1.2 | 1.1–1.4 | 0.001 | ns | ||
| TAPSE (per 1 mm) | 0.86 | 0.75–0.99 | 0.03 | ns | ||
| WHO FC (III/IV vs. I/II) | 1.4 | 0.54–2.75 | 0.006 | ns | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sławek-Szmyt, S.; Araszkiewicz, A.; Jankiewicz, S.; Grygier, M.; Mularek-Kubzdela, T.; Lesiak, M. Prognostic Value of Pulmonary Artery Pulsatility Index in Right Ventricle Failure-Related Mortality in Inoperable Chronic Thromboembolic Pulmonary Hypertension. J. Clin. Med. 2022, 11, 2735. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102735
Sławek-Szmyt S, Araszkiewicz A, Jankiewicz S, Grygier M, Mularek-Kubzdela T, Lesiak M. Prognostic Value of Pulmonary Artery Pulsatility Index in Right Ventricle Failure-Related Mortality in Inoperable Chronic Thromboembolic Pulmonary Hypertension. Journal of Clinical Medicine. 2022; 11(10):2735. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102735
Chicago/Turabian StyleSławek-Szmyt, Sylwia, Aleksander Araszkiewicz, Stanisław Jankiewicz, Marek Grygier, Tatiana Mularek-Kubzdela, and Maciej Lesiak. 2022. "Prognostic Value of Pulmonary Artery Pulsatility Index in Right Ventricle Failure-Related Mortality in Inoperable Chronic Thromboembolic Pulmonary Hypertension" Journal of Clinical Medicine 11, no. 10: 2735. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102735