
Employing the Multivariate Edmonton Scale in the Assessment of Frailty Syndrome in Heart Failure

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
- patient’s lack of consent to participate in the study
- LVEF > 40%
- other diagnosis significantly burdening the prognosis within one year (e.g., active neoplastic disease, acute coronary syndrome, stroke up to 3 months, pulmonary hypertension)
- depression diagnosis on the Geriatric depression scale according to Yesavage (GDS) [13].
- diagnosis of cognitive dysfunction with dementia—assessment based on the Mini-Mental State Examination (MMSE) questionnaire [14].
2.2. The Course of the Study
- interview (demographic, sociodemographic, and clinical data were obtained, i.e., New York Heart Association (NYHA) functional class, etiology of the heart failure, presence of comorbidities, reason for planned hospitalization, and the course of hospitalization). The obtained information was verified based on the current medical documentation. Information on the ejection fraction (EF) was obtained from the echocardiography
- assessment of severity of the frailty syndrome—Edmonton Frailty Scale questionnaire.
- evaluation of the occurrence of depression using the Geriatric depression scale according to Yesavage
- assessment of cognitive functions—MMSE Mini-Mental State Examination questionnaire.
- Information on hospital readmissions after 6 and 12 months was obtained from telephone interviews conducted with study participants.
2.3. Research Tools
- 0–4 points—no frailty
- 5–6 points—particularly sensitive people predisposed to presenting frailty
- 7–8 points—mild frailty
- 9–10 points—moderate frailty
- 11 points or more—serious weakness.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- Assessment and monitoring of the state of increased sensitivity to the development of frailty or FS in patients with HF should influence the differentiation of clinical management. Our results confirm that patients in the pre-frail group, and the presence of frailty itself, may be associated with higher rates of complications during hospitalization.
- There is a need to standardize the research in terms of the research tools used in the described group of patients.
- The Edmonton Questionnaire may be a helpful tool for the assessment of frailty in hospitalized patients with HF. There is a need for further research involving larger groups of study subjects.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Vitale, C.; Uchmanowicz, I. Frailty in patients with heart failure. Eur. Heart J. Suppl. 2019, 21, L12–L16. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Howlett, S.E. Fifteen years of progress in understanding frailty and health in aging. BMC Med. 2018, 16, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Ellahham, S.; Ibrahim, H.S. Frailty in Heart Failure: A Coalesce of International Guidelines. J. Clin. Exp. Cardiol. 2019, 10, 2. [Google Scholar]
- Vitale, C.; Jankowska, E.; Hill, L.; Piepoli, M.; Doehner, W.; Anker, S.D.; Lainscak, M.; Jaarsma, T.; Ponikowski, P.; Giuseppe, M.C.R.; et al. Heart Failure Association/European Society of Cardiology position paper on frailty in patients with heart failure. Eur. J. Heart Fail. 2019, 21, 1299–1305. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/ejhf.1611 (accessed on 14 February 2020). [CrossRef]
- Sobczyńska, M.; Główczyńska, R.; Opolski, G. Zwiększanie przez zespół kruchości częstości występowania powikłań u pacjentów poddawanych zabiegom kardiologii inwazyjnej i operacjom kardiochirurgicznym. Folia Cardiol. 2017, 12, 557–564. [Google Scholar] [CrossRef]
- Goldwater, D.; Altman, N. Frailty and heart failure. Am. Coll. Cardiol. 2016. Available online: https://www.acc.org/latest-in-cardiology/articles/2016/08/05/08/40/frailty-and-heart-failure (accessed on 15 January 2019).
- Vitale, C.; Spoletini, I.; Rosano, G.M. Frailty in Heart Failure: Implications for Management. Card. Fail. Rev. 2018, 4, 104. [Google Scholar] [CrossRef]
- Testa, G.; Curcio, F.; Liguori, I.; Basile, C.; Papillo, M.; Tocchetti, C.G.; Galizia, G.; Della-Morte, D.; Gargiulo, G.; Cacciatore, F.; et al. Physical vs. multidimensional frailty in older adults with and without heart failure. ESC Heart Fail. 2020, 7, 1371–1380. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/ehf2.12688 (accessed on 12 August 2021). [CrossRef] [PubMed] [Green Version]
- McDonagh, J.; Martin, L.; Ferguson, C.; Jha, S.R.; Macdonald, P.S.; Davidson, P.M.; Newton, P.J. Frailty assessment instruments in heart failure: A systematic review. Eur. J. Cardiovasc. Nurs. 2018, 17, 23–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albiński, R.; Kleszczewska-Albińska, A.; Bedyńska, S. Validity and reliability of different versions of the scale—Review. Psychiatr. Pol. 2011, 45, 555–562. [Google Scholar]
- Mitchell, A.J. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 2009, 43, 411–431. Available online: https://pubmed.ncbi.nlm.nih.gov/18579155/ (accessed on 27 December 2021). [CrossRef] [PubMed]
- Rolfson, D.B.; Majumdar, S.R.; Tsuyuki, R.T.; Tahir, A.; Rockwood, K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006, 35, 526–529. Available online: https://0-academic-oup-com.brum.beds.ac.uk/ageing/article/35/5/526/9782 (accessed on 14 February 2020). [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 20 December 2021).
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S, 4th ed.; Springer: New York, NY, USA, 2002; ISBN 0-387-95457-0. [Google Scholar]
- Christensen, R.H.B. Ordinal—Regression Models for Ordinal Data. R Package Version 2019.12-10. 2019. Available online: https://cran.r-project.org/package=ordinal (accessed on 20 December 2021).
- Sun, C. erer: Empirical Research in Economics with R. R Package Version 3.0. 2020. Available online: https://cran.r-project.org/package=erer (accessed on 20 December 2021).
- Kohl, M. MKpower: Power Analysis and Sample Size Calculation. R Package Version 0.5. 2020. Available online: http://www.stamats.de (accessed on 2 February 2020).
- Friendly, M. vcdExtra: ‘Vcd’ Extensions and Additions. R Package Version 0.7-1. 2017. Available online: https://cran.r-project.org/package=vcdExtra (accessed on 2 February 2020).
- Marengoni, A.; Zucchelli, A.; Vetrano, D.L.; Aloisi, G.; Brandi, V.; Ciutan, M.; Panait, C.L.; Bernabei, R.; Onder, G.; Palmer, K. Heart failure, frailty, and pre-frailty: A systematic review and meta-analysis of observational studies. Int. J. Cardiol. 2020, 316, 161–171. [Google Scholar] [CrossRef]
- Denfeld, Q.E.; Winters-Stone, K.; Mudd, J.O.; Gelow, J.M.; Kurdi, S.; Lee, C.S. The prevalence of frailty in heart failure: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 236, 283–289. [Google Scholar] [CrossRef]
- McDonagh, J.; Ferguson, C.; Newton, P.J. Frailty Assessment in Heart Failure: An Overview of the Multi-domain Approach. Curr. Heart Fail. Rep. 2018, 15, 17–23. [Google Scholar] [CrossRef]
- Zhang, Y.; Yuan, M.; Gong, M.; Tse, G.; Li, G.; Liu, T. Frailty and Clinical Outcomes in Heart Failure: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 1003–1008.e1. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Zhang, J.; Weston, J.; Clark, A.L. Identification of Frailty in Chronic Heart Failure. JACC Heart Fail. 2019, 7, 291–302. [Google Scholar] [CrossRef]
- Fabrício-Wehbe, S.C.C.; Cruz, I.R.; Haas, V.J.; Diniz, M.A.; Dantas, R.A.S.; Rodrigues, R.A.P. Reproducibility of the Brazilian version of the Edmonton Frail Scale for elderly living in the community. Rev. Lat. Am. Enfermagem. 2013, 21, 1330–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankowska-Polańska, B.; Uchmanowicz, B.; Kujawska-Danecka, H.; Nowicka-Sauer, K.; Chudiak, A.; Dudek, K.; Rosińczuk, J. Assessment of frailty syndrome using Edmonton frailty scale in Polish elderly sample. Aging Male 2019, 22, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Kuśnierz, M.; Wleklik, M.; Jankowska-Polańska, B.; Jaroch, J.; Łoboz-Grudzień, K. Frailty syndrome and rehospitalizations in elderly heart failure patients. Aging Clin. Exp. Res. 2018, 30, 617–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, D.; Aladio, M.; Girado, C.A.; Pérez de la Hoz, R.; Sara Berensztein, C. Frailty is independently associated with 1-year mortality after hospitalization for acute heart failure. Int. J. Cardiol. Heart Vasc. 2018, 21, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.-P.; Chen, L.-Y.; Zhu, J.-J.; Liu, W.-X.; Ma, C.-S. Association of frailty with in-hospital outcomes in elderly patients with heart failure. World J. Clin. Cases 2021, 9, 11208–11219. [Google Scholar] [CrossRef]
- Kwok, C.S.; Zieroth, S.; Van Spall, H.G.C.; Helliwell, T.; Clarson, L.; Mohamed, M.; Mallen, C.; Duckett, S.; Mamas, M.A. The Hospital Frailty Risk Score and its association with in-hospital mortality, cost, length of stay and discharge location in patients with heart failure short running title: Frailty and outcomes in heart failure. Int. J. Cardiol. 2020, 300, 184–190. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Zhang, J.; Weston, J.; Squire, I.B.; Clark, A.L. Effect of frailty on treatment, hospitalisation and death in patients with chronic heart failure. Clin. Res. Cardiol. 2021, 110, 1249–1258. [Google Scholar] [CrossRef]
- Pandey, A.; Kitzman, D.; Whellan, D.J.; Duncan, P.W.; Mentz, R.J.; Pastva, A.M.; Nelson, M.B.; Upadhya, B.; Chen, H.; Reeves, G.R. Frailty among Older Decompensated Heart Failure Patients: Prevalence, Association with Patient-Centered Outcomes, and Efficient Detection Methods. JACC Heart Fail. 2019, 7, 1079–1088. [Google Scholar] [CrossRef]
- Kleipool, E.E.F.; Hoogendijk, E.O.; Trappenburg, M.C.; Handoko, M.L.; Huisman, M.; Peters, M.J.L.; Muller, M. Frailty in older adults with cardiovascular disease: Cause, effect or both? Aging Dis. 2018, 9, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Dewan, P.; Jackson, A.; Jhund, P.S.; Shen, L.; Ferreira, J.P.; Petrie, M.C.; Abraham, W.T.; Desai, A.S.; Dickstein, K.; Køber, L.; et al. The prevalence and importance of frailty in heart failure with reduced ejection fraction—An analysis of PARADIGM-HF and ATMOSPHERE. Eur. J. Heart Fail. 2020, 22, 2123–2133. [Google Scholar] [CrossRef]
- Pandey, A.; Kitzman, D.; Reeves, G. Frailty Is Intertwined with Heart Failure: Mechanisms, Prevalence, Prognosis, Assessment, and Management. JACC Heart Fail. 2019, 7, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Młynarska, A.; Lisiak, M.; Kałużna-Oleksy, M.; Wleklik, M.; Chudiak, A.; Dudek, M.; Migaj, J.; Hinterbuchner, L.; Gobbens, R. Heart Failure and Problems with Frailty Syndrome: Why it is Time to Care About Frailty Syndrome in Heart Failure. Card. Fail. Rev. 2019, 5, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchmanowicz, I.; Nessler, J.; Gobbens, R.; Gackowski, A.; Kurpas, D.; Straburzynska-Migaj, E.; Kałuzna-Oleksy, M.; Jankowska, E.A. Coexisting Frailty with Heart Failure. Front. Physiol. 2019, 10, 791. [Google Scholar] [CrossRef] [Green Version]
- Butts, B.; Gary, R. Coexisting frailty, cognitive impairment, and heart failure: Implications for clinical care. J. Clin. Outcomes Manag. 2015, 22, 38–46. [Google Scholar]
- Kałużna-Oleksy, M.; Kukfisz, A.; Migaj, J.; Dudek, M.; Krysztofiak, H.; Sawczak, F.; Szczechla, M.; Przytarska, K.; Straburzyńska-Migaj, E.; Wleklik, M.; et al. A Simple Risk Score Based on Routine Clinical Parameters Can Predict Frailty in Hospitalized Heart Failure Patients. J. Clin. Med. 2021, 10, 5963. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, J.; Alexander, K.P.; Mack, M.J.; Maurer, M.S.; Green, P.; Allen, L.A.; Popma, J.J.; Ferrucci, L.; Forman, D.E. Frailty Assessment in the Cardiovascular Care of Older Adults. J. Am. Coll. Cardiol. 2014, 63, 747–762. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Quantitative Variables | All Patients (n = 106) Mean ± Standard Deviation or Median (First Quartile; Third Quartile) |
|---|---|
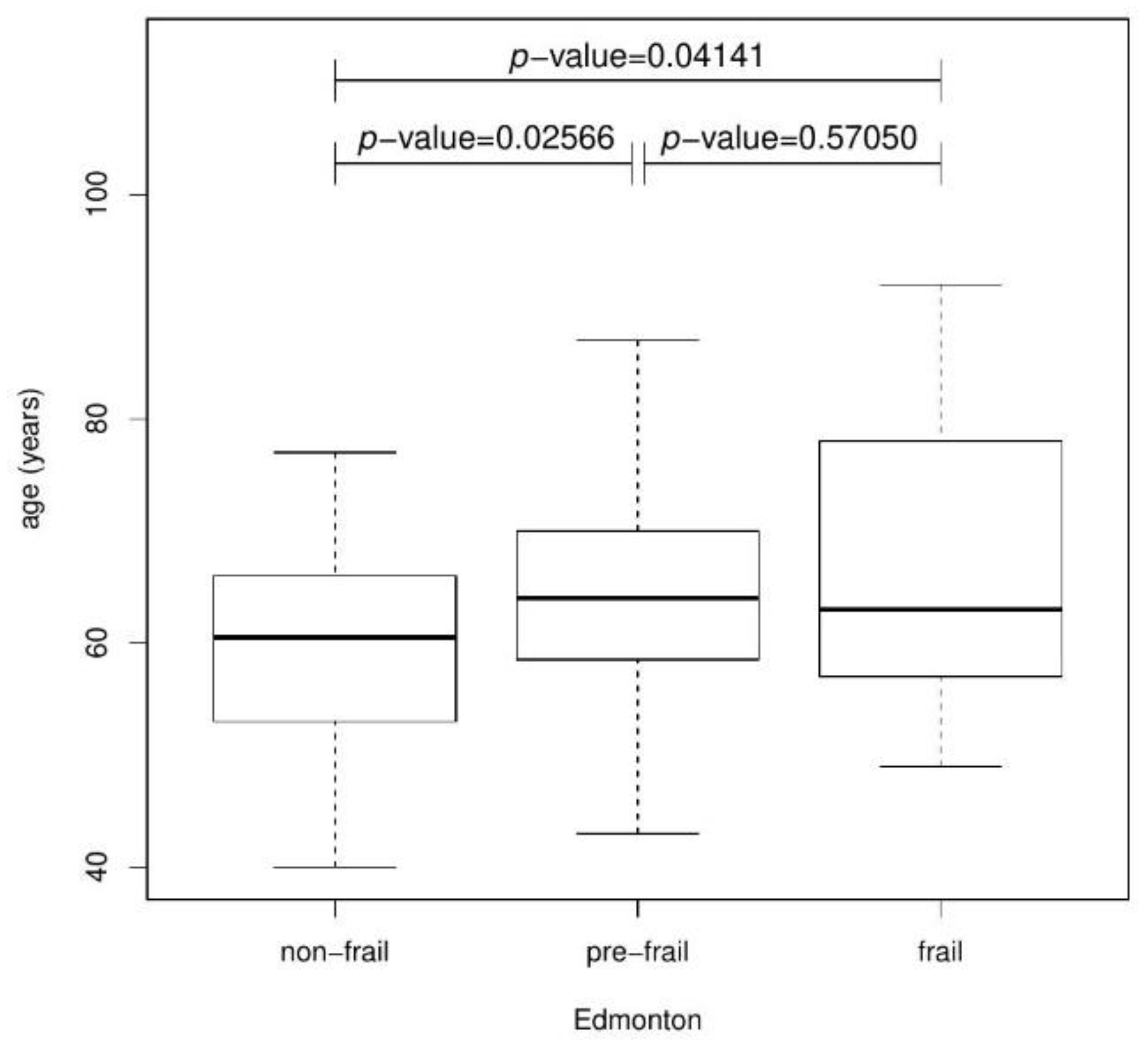
| Age (years) | 62.6 ± 9.7 |
| Edmonton | 5 (3; 6) |
| Qualitative variables | All patients (n = 106) n (%) |
| Cause of hospitalization | |
| planned | 53 (50%) |
| worsening of heart failure | 53 (50%) |
| Etiology of heart failure | |
| coronary | 70 (66%) |
| non-coronary | 36 (34%) |
| Comorbidities | |
| yes | 100 (94.3%) |
| no | 6 (5.7%) |
| Diabetes | |
| yes | 43 (40.6%) |
| no | 63 (59.4%) |
| Hypertension | |
| yes | 78 (73.6%) |
| no | 28 (26.4%) |
| Chronic kidney disease | |
| yes | 30 (28.3%) |
| no | 76 (71.7%) |
| Hypothyroidism | |
| yes | 12 (11.3%) |
| no | 94 (88.7%) |
| Hyperthyroidism | |
| yes | 3 (2.8%) |
| no | 103 (97.2%) |
| Stroke | |
| yes | 13 (12.3%) |
| no | 93 (87.7%) |
| Chronic obstructive pulmonary disease | |
| yes | 17 (16%) |
| no | 89 (84%) |
| Lower limb atherosclerosis | |
| yes | 15 (14.2%) |
| no | 91 (85.8%) |
| Implantable cardioverter-defibrillator (ICD) | |
| yes | 52 (49%) |
| no | 54 (51%) |
| Cardiac resynchronization therapy with defibrillator function (CRT-D) | |
| yes | 17(16%) |
| no | 89 (84%) |
| NYHA_b- beginning of hospitalization | |
| II | 42 (39.6%) |
| II/III | 5 (4.7%) |
| III | 47 (44.3%) |
| III/IV | 12 (11.3%) |
| NYHA_e- end of hospitalization | |
| II | 58 (55.8%) |
| II/III | 28 (26.9%) |
| III | 18 (17.3%) |
| Complications hospitalization | |
| no | 83 (78.3%) |
| yes | 23 (21.7%) |
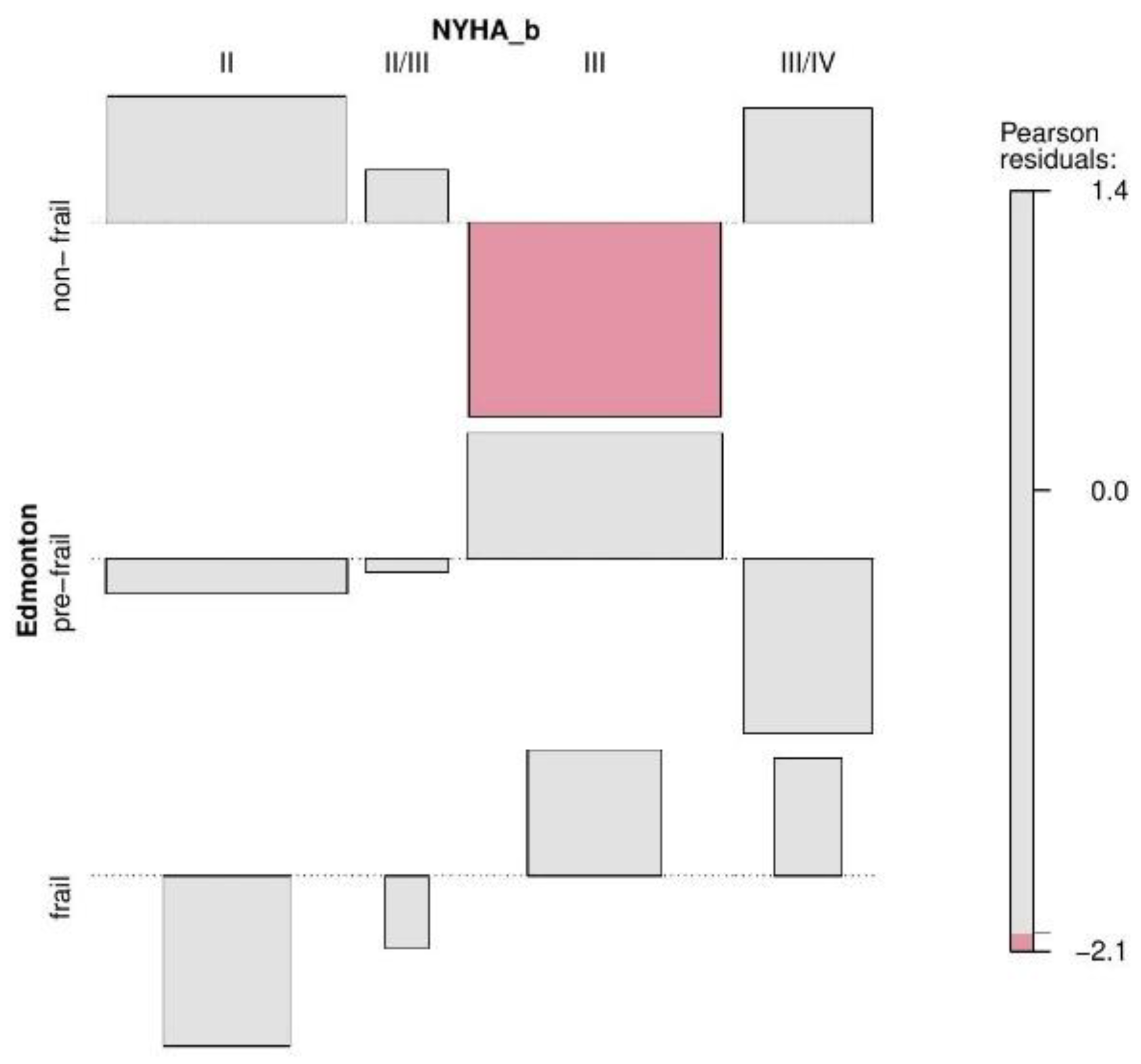
| NYHA_b | Edmonton | p-Value Fisher’s Exact Test for Count Data | ||
|---|---|---|---|---|
| Non-Frail | Pre-Frail | Frail | ||
| II | 24 | 17 | 1 | 0.00037 |
| II/III | 3 | 2 | 0 | |
| III | 11 | 27 | 9 | |
| III/IV | 8 | 1 | 3 | |
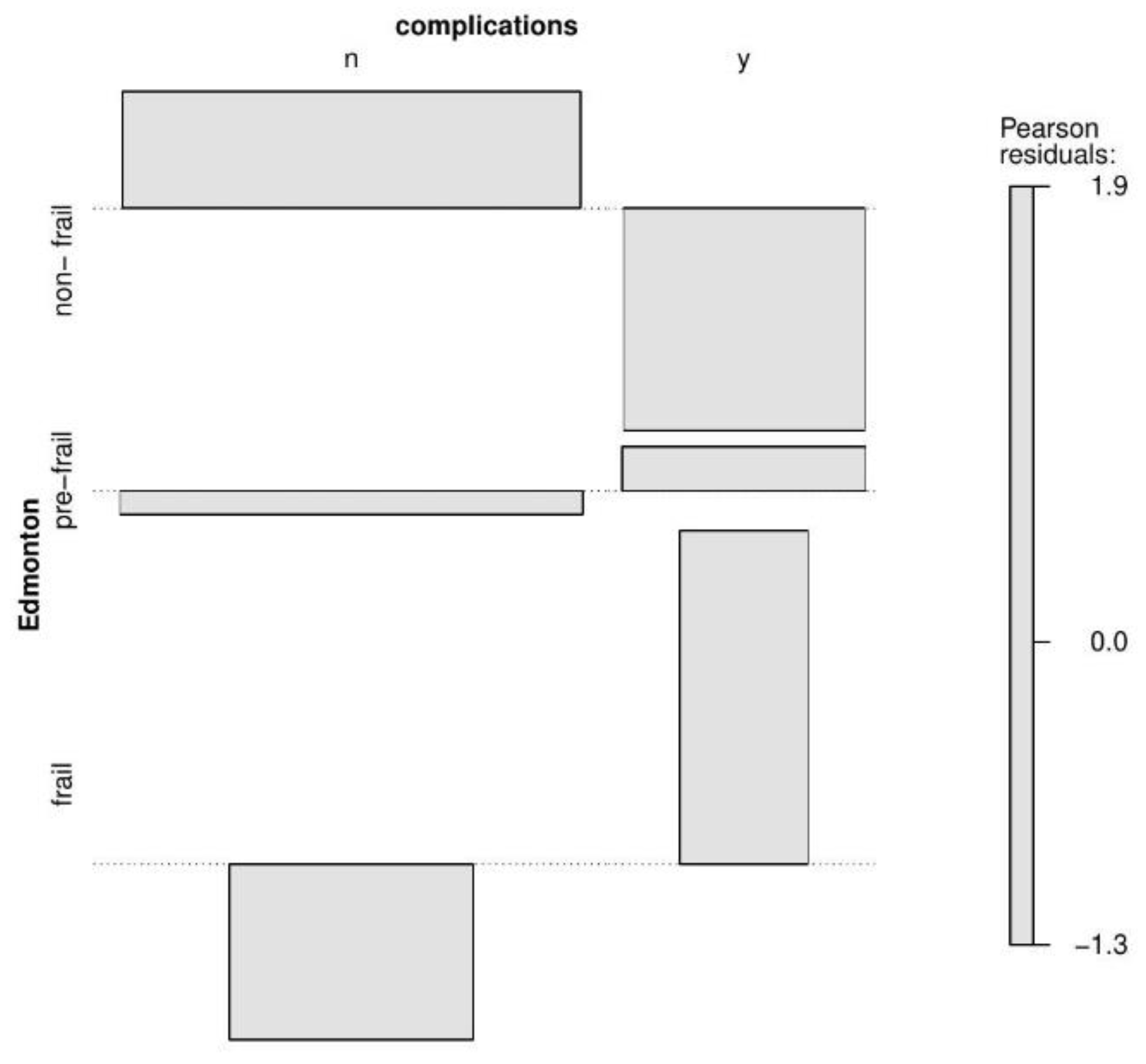
| Complications | Edmonton | p-Value Fisher’s Exact Test for Count Data | ||
|---|---|---|---|---|
| Non-Frail | Pre-Frail | Frail | ||
| No | 40 | 36 | 7 | 0.03875 |
| Yes | 6 | 11 | 6 | |
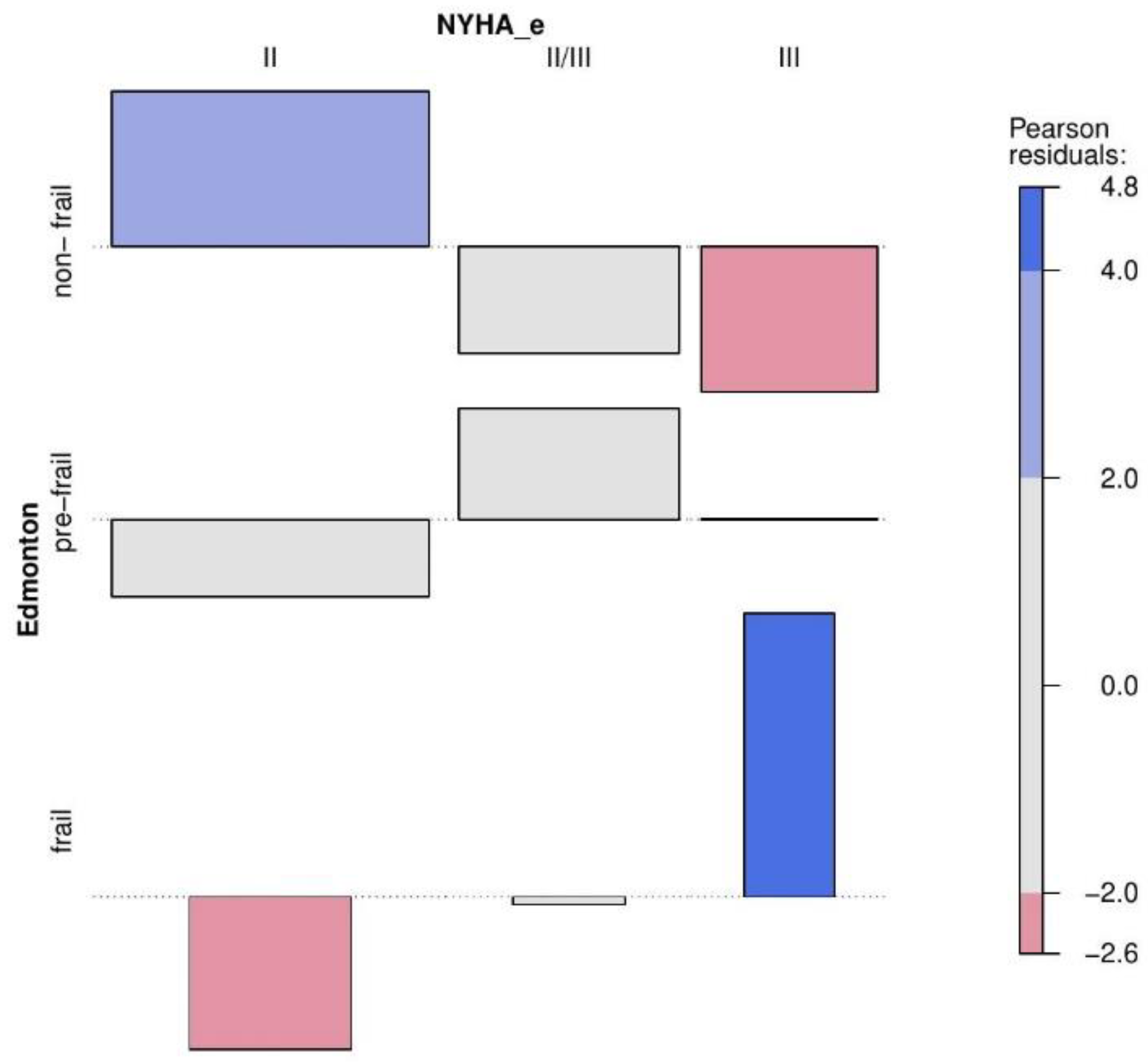
| NYHA_e | Edmonton | p-Value Fisher’s Exact Test for Count Data | ||
|---|---|---|---|---|
| Non-Frail | Pre-Frail | Frail | ||
| II | 39 | 19 | 0 | <0.00001 |
| II/III | 6 | 19 | 3 | |
| III | 1 | 8 | 9 | |
| Probability | |||
|---|---|---|---|
| Non-Frail | Pre-Frail | Frail | |
| Chronic kidney disease yes | 0.5482 | 0.3953 | 0.0565 |
| No | 0.8896 | 0.1015 | 0.0089 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Studzińska, K.; Wąż, P.; Frankiewicz, A.; Stopczyńska, I.; Studnicki, R.; Hansdorfer-Korzon, R. Employing the Multivariate Edmonton Scale in the Assessment of Frailty Syndrome in Heart Failure. J. Clin. Med. 2022, 11, 4022. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144022
Studzińska K, Wąż P, Frankiewicz A, Stopczyńska I, Studnicki R, Hansdorfer-Korzon R. Employing the Multivariate Edmonton Scale in the Assessment of Frailty Syndrome in Heart Failure. Journal of Clinical Medicine. 2022; 11(14):4022. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144022
Chicago/Turabian StyleStudzińska, Karolina, Piotr Wąż, Anna Frankiewicz, Iwona Stopczyńska, Rafał Studnicki, and Rita Hansdorfer-Korzon. 2022. "Employing the Multivariate Edmonton Scale in the Assessment of Frailty Syndrome in Heart Failure" Journal of Clinical Medicine 11, no. 14: 4022. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144022