
Left Ventricular Non-Compaction Cardiomyopathy-Still More Questions than Answers


 , , and
, , and
Abstract
:1. Introduction
2. Pathogenesis
3. Clinical Presentation
4. Diagnostic Methods
4.1. Echocardiography
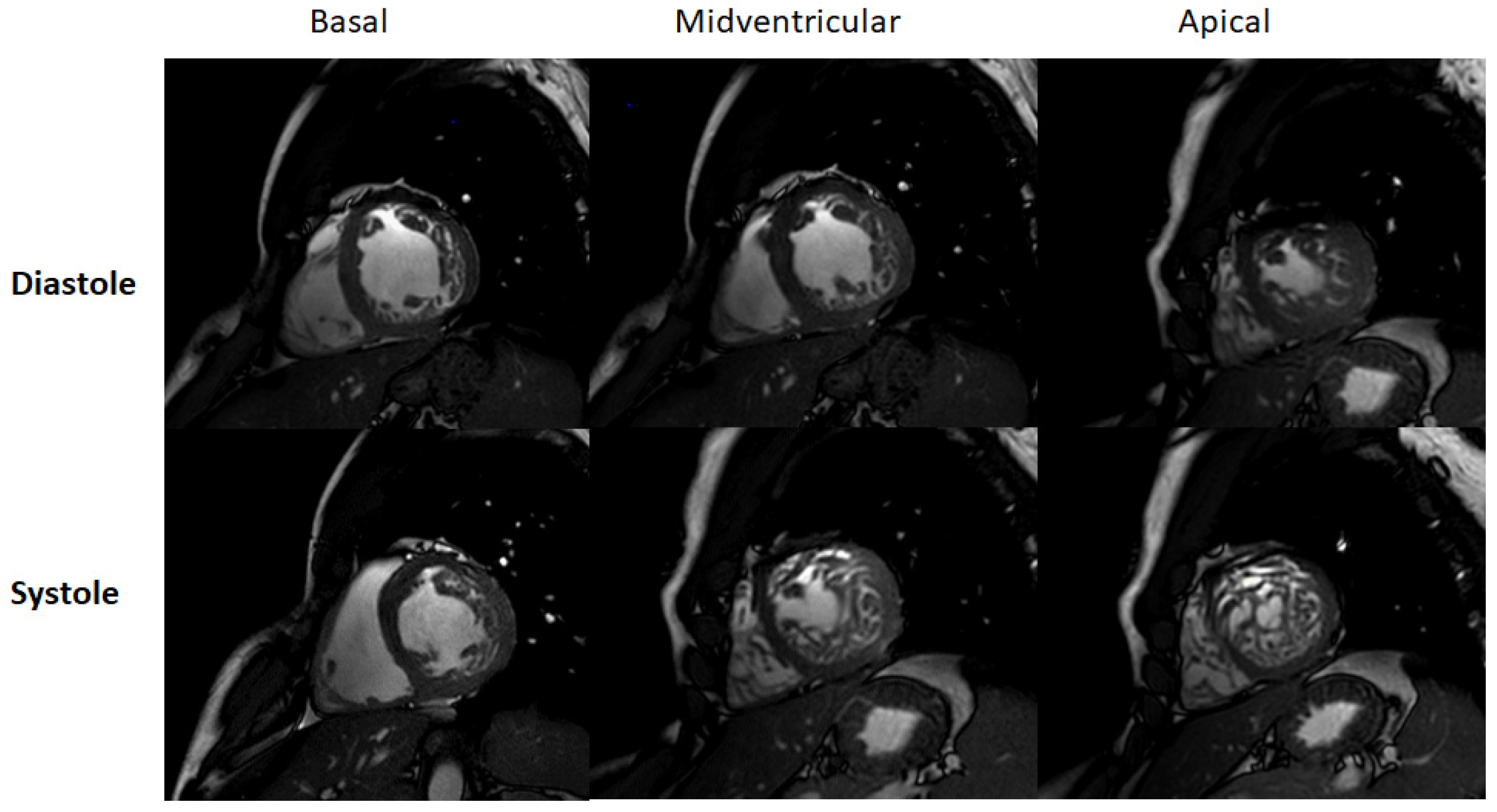
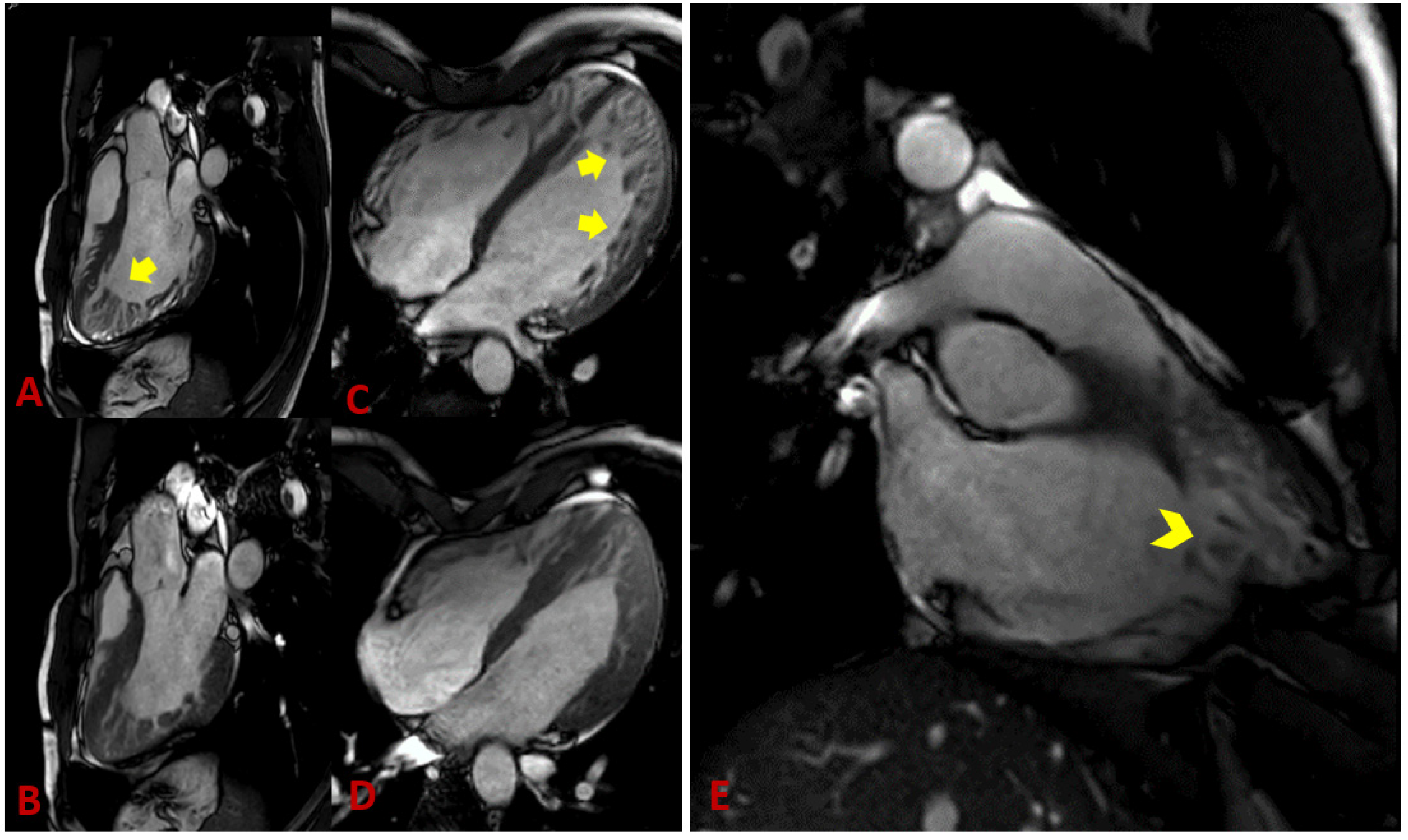
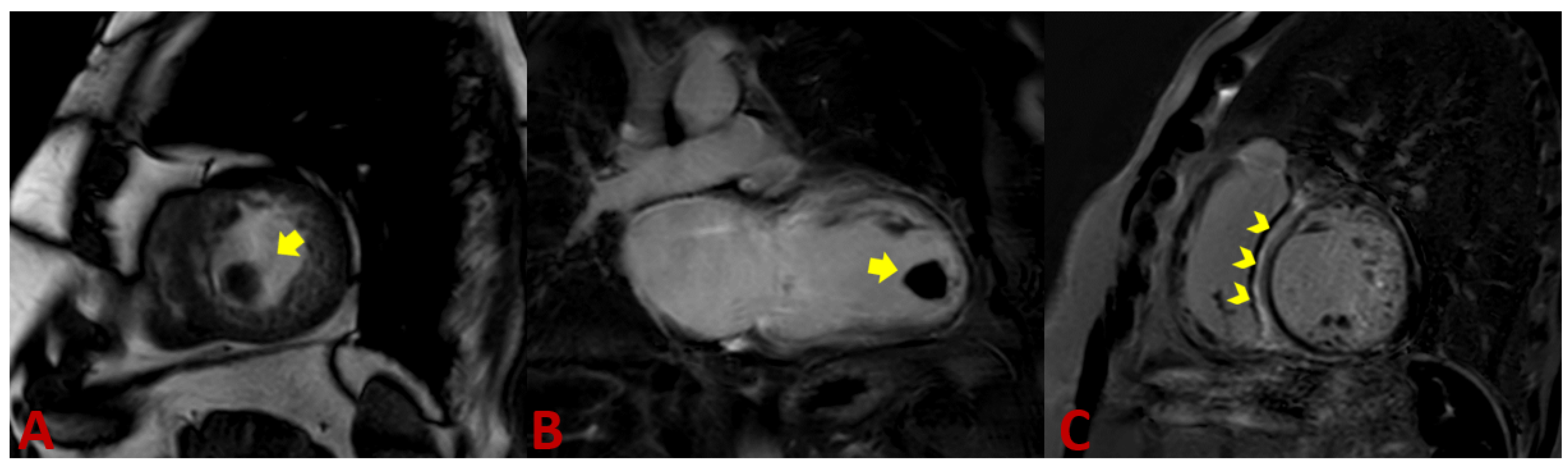
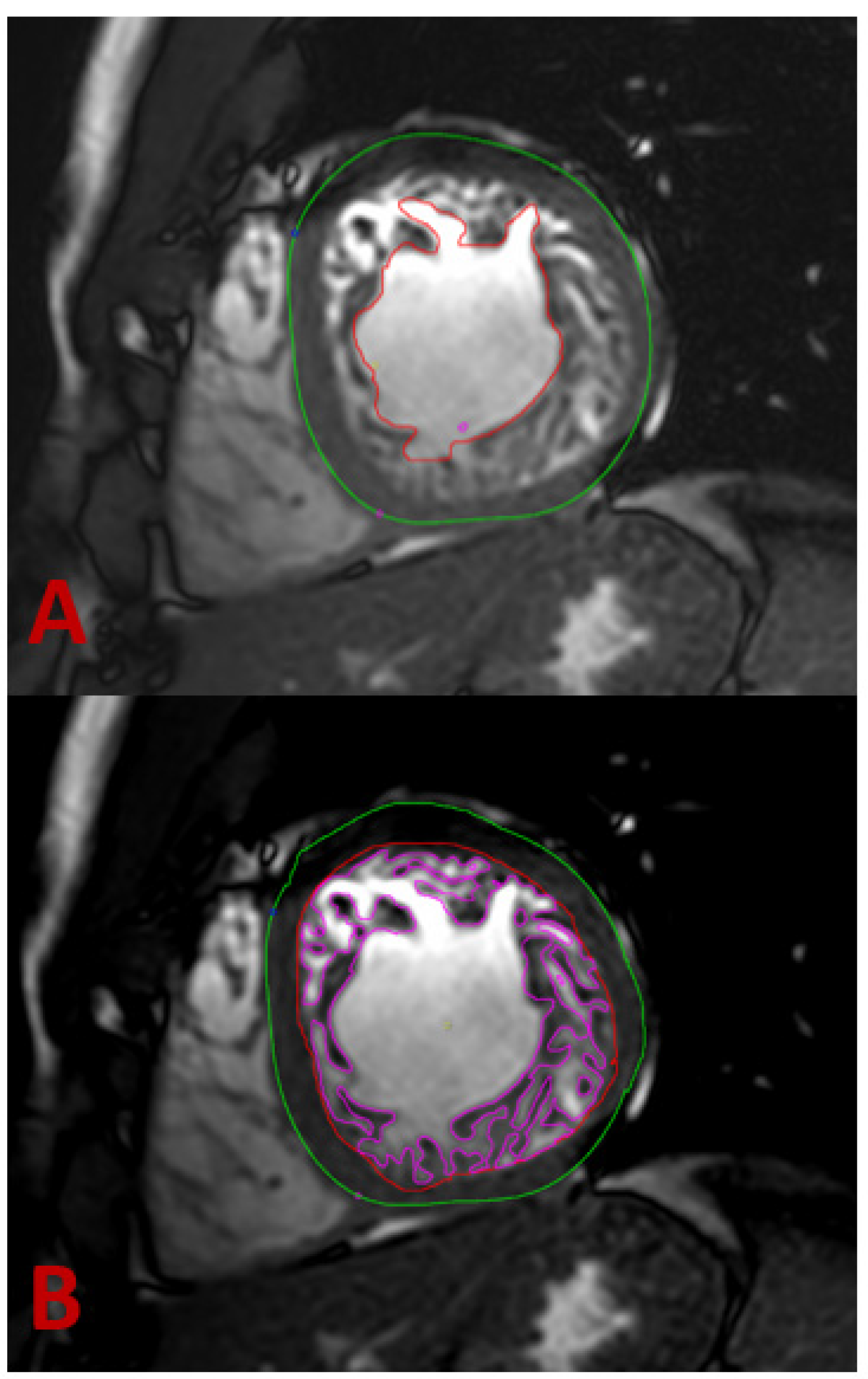
4.2. Magnet Resonance Imaging
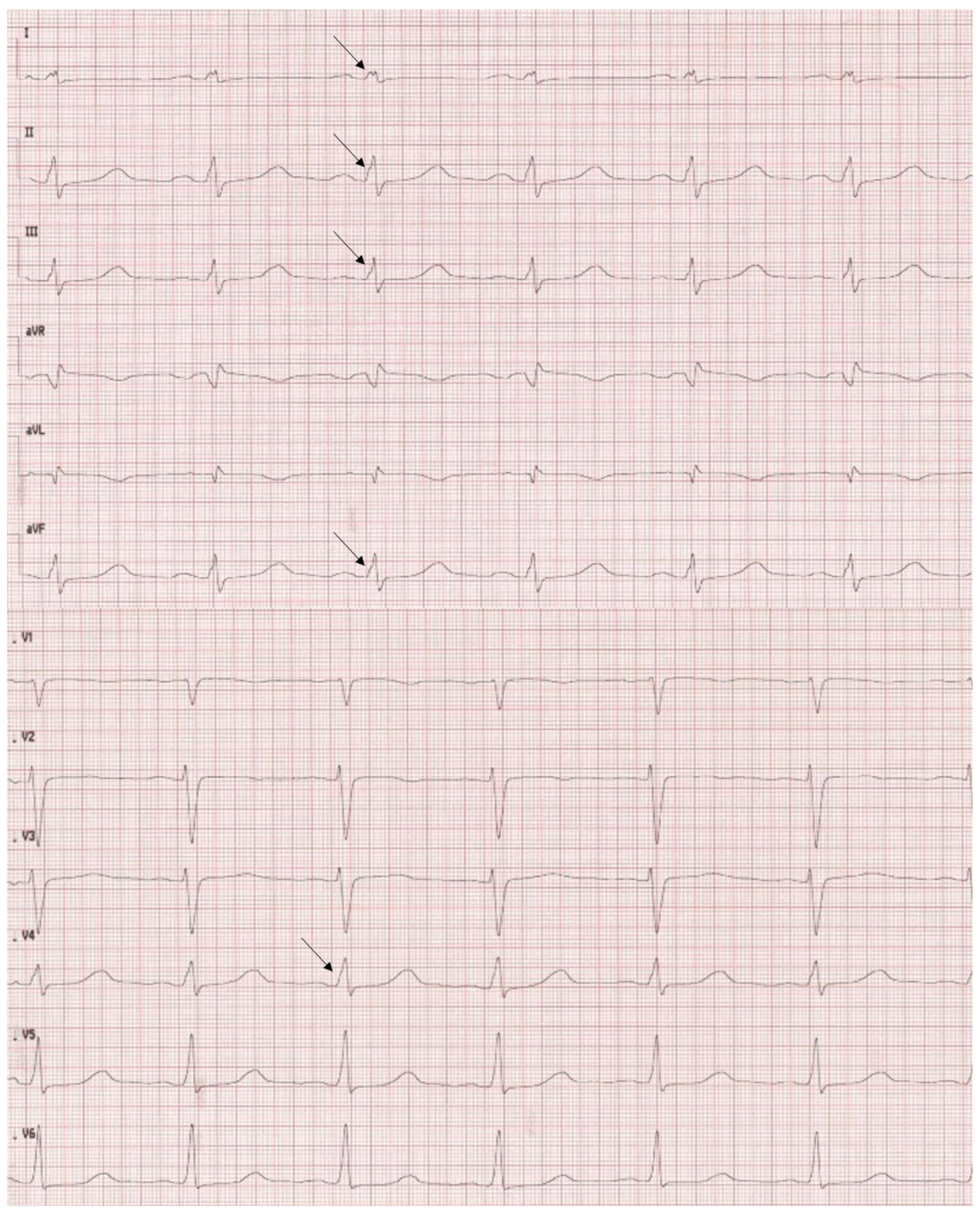
4.3. ECG
4.4. Computer Tomography
4.5. Endomyocardial Biopsy
5. Genetics
6. Differential Diagnosis
7. Treatment
8. Prognosis
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grant, R.T. An unusual anomaly of the coronary vessels in the malformed heart of a child. Heart 1926, 1, 273–283. [Google Scholar]
- Engberding, R.; Bender, F. Identification of a rare congenital anomaly of the myocardium by two-dimensional echocardiography: Persistence of isolated myocardial sinusoids. Am. J. Cardiol. 1984, 53, 1733–1734. [Google Scholar] [CrossRef]
- Chin, T.K.; Perloff, J.K.; Williams, R.G.; Jue, K.; Mohrmann, R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation 1990, 82, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerecke, B.J.; Engberding, R. Noncompaction Cardiomyopathy-History and Current Knowledge for Clinical Practice. J. Clin. Med. 2021, 10, 2457. [Google Scholar] [CrossRef]
- Protonotarios, A.; Elliott, P.M. Left ventricular non-compaction: Have we reached the limits of conventional imaging. Eur. Heart J. 2020, 41, 1437–1438. [Google Scholar] [CrossRef]
- D’Silva, A.; Jensen, B. Left ventricular non-compaction cardiomyopathy: How many needles in the haystack. Heart 2021, 107, 1344–1352. [Google Scholar] [CrossRef]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B.; American, H.A.; et al. Contemporary definitions and classification of the cardiomyopathies: An American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006, 113, 1807–1816. [Google Scholar]
- Arbustini, E.; Narula, N.; Dec, G.W.; Reddy, K.S.; Greenberg, B.; Kushwaha, S.; Marwick, T.; Pinney, S.; Bellazzi, R.; Favalli, V.; et al. The MOGE(S) classification for a phenotype-genotype nomenclature of cardiomyopathy: Endorsed by the World Heart Federation. J. Am. Coll. Cardiol. 2013, 62, 2046–2072. [Google Scholar] [CrossRef] [Green Version]
- Arbustini, E.; Favalli, V.; Narula, N.; Serio, A.; Grasso, M. Left Ventricular Noncompaction: A Distinct Genetic Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 68, 949–966. [Google Scholar] [CrossRef]
- Van Waning, J.I.; Moesker, J.; Heijsman, D.; Boersma, E.; Majoor-Krakauer, D. Systematic Review of Genotype-Phenotype Correlations in Noncompaction Cardiomyopathy. J. Am. Heart Assoc. 2019, 8, e012993. [Google Scholar] [CrossRef] [PubMed]
- Luijkx, T.; Cramer, M.J.; Zaidi, A.; Rienks, R.; Senden, P.J.; Sharma, S.; van Hellemondt, F.J.; Buckens, C.F.; Mali, W.P.; Velthuis, B.K. Ethnic differences in ventricular hypertrabeculation on cardiac MRI in elite football players. Neth. Heart J. 2012, 20, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Kawel-Boehm, N.; McClelland, R.L.; Zemrak, F.; Captur, G.; Hundley, W.G.; Liu, C.Y.; Moon, J.C.; Petersen, S.E.; Ambale-Venkatesh, B.; Lima, J.A.C.; et al. Hypertrabeculated Left Ventricular Myocardium in Relationship to Myocardial Function and Fibrosis: The Multi-Ethnic Study of Atherosclerosis. Radiology 2017, 284, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Weir-McCall, J.R.; Yeap, P.M.; Papagiorcopulo, C.; Fitzgerald, K.; Gandy, S.J.; Lambert, M.; Belch, J.J.; Cavin, I.; Littleford, R.; Macfarlane, J.A.; et al. Left Ventricular Noncompaction: Anatomical Phenotype or Distinct Cardiomyopathy. J. Am. Coll. Cardiol. 2016, 68, 2157–2165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, S.B.; Jones, K.; Blanch, B.; Puranik, R.; McGeechan, K.; Barratt, A.; Semsarian, C. A systematic review and meta-analysis of the prevalence of left ventricular non-compaction in adults. Eur. Heart J. 2020, 41, 1428–1436. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, A.; Dabiesingh, D.S.; Bhumireddy, G.P.; Mohamed, A.; Asfour, A.; Briggs, W.M.; Ho, J.; Khan, S.A.; Grossman, A.; Klem, I.; et al. Prevalence and Prognostic Significance of Left Ventricular Noncompaction in Patients Referred for Cardiac Magnetic Resonance Imaging. Circ. Cardiovasc. Imaging 2017, 10, e006174. [Google Scholar] [CrossRef] [Green Version]
- Towbin, J.A.; Jefferies, J.L. Cardiomyopathies Due to Left Ventricular Noncompaction, Mitochondrial and Storage Diseases, and Inborn Errors of Metabolism. Circ. Res. 2017, 121, 838–854. [Google Scholar] [CrossRef] [Green Version]
- Sedmera, D.; Pexieder, T.; Vuillemin, M.; Thompson, R.P.; Anderson, R.H. Developmental patterning of the myocardium. Anat. Rec. 2000, 258, 319–337. [Google Scholar] [CrossRef]
- Blausen, B.E.; Johannes, R.S.; Hutchins, G.M. Computer-based reconstructions of the cardiac ventricles of human embryos. Am. J. Cardiovasc. Pathol. 1990, 3, 37–43. [Google Scholar]
- Faber, J.W.; D’Silva, A.; Christoffels, V.M.; Jensen, B. Lack of morphometric evidence for ventricular compaction in humans. J. Cardiol. 2021, 78, 397–405. [Google Scholar] [CrossRef]
- Luxán, G.; Casanova, J.C.; Martínez-Poveda, B.; Prados, B.; D’Amato, G.; MacGrogan, D.; Gonzalez-Rajal, A.; Dobarro, D.; Torroja, C.; Martinez, F.; et al. Mutations in the NOTCH pathway regulator MIB1 cause left ventricular noncompaction cardiomyopathy. Nat. Med. 2013, 19, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Jensen, B.; van der Wal, A.C.; Moorman, A.F.M.; Christoffels, V.M. Excessive trabeculations in noncompaction do not have the embryonic identity. Int. J. Cardiol. 2017, 227, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stöllberger, C.; Wegner, C.; Finsterer, J. CHADS2- and CHA2DS2VASc scores and embolic risk in left ventricular hypertrabeculation/noncompaction. J. Stroke Cerebrovasc. Dis. 2013, 22, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Engberding, R.; Stöllberger, C.; Schneider, B.; Nothnagel, D.; Fehske, W.; Gerecke, B.J. Abstract 14769: Heart Failure in Noncompaction Cardiomyopathy - Data from the German Noncompaction Registry (ALKK). Circulation 2012, 126, A14769. [Google Scholar]
- Howard, T.S.; Valdes, S.O.; Hope, K.D.; Morris, S.A.; Landstrom, A.P.; Schneider, A.E.; Miyake, C.Y.; Denfield, S.W.; Pignatelli, R.H.; Wang, Y.; et al. Association of Wolff-Parkinson-White With Left Ventricular Noncompaction Cardiomyopathy in Children. J. Card. Fail. 2019, 25, 1004–1008. [Google Scholar] [CrossRef]
- Ichida, F. Left ventricular noncompaction. Circ. J. 2009, 73, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Towbin, J.A.; Lorts, A.; Jefferies, J.L. Left ventricular non-compaction cardiomyopathy. Lancet 2015, 386, 813–825. [Google Scholar] [CrossRef]
- Bhaskaran, A.; Campbell, T.; Virk, S.; Bennett, R.G.; Kizana, E.; Kumar, S. Electrophysiologic and electroanatomic characterization of ventricular arrhythmias in non-compaction cardiomyopathy: A systematic review. J. Cardiovasc. Electrophysiol. 2021, 32, 1421–1429. [Google Scholar] [CrossRef]
- Stöllberger, C.; Blazek, G.; Gessner, M.; Bichler, K.; Wegner, C.; Finsterer, J. Neuromuscular comorbidity, heart failure, and atrial fibrillation as prognostic factors in left ventricular hypertrabeculation/noncompaction. Herz 2015, 40, 906–911. [Google Scholar] [CrossRef]
- Dhawan, R.; Kadir, S.; Barton, D.E.; Stone, J.R.; Chatzizisis, Y.S. Myocardial infarction secondary to coronary embolus in a patient with left ventricular non-compaction cardiomyopathy: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab077. [Google Scholar] [CrossRef]
- Salati, M.; Di Mauro, A.; Bregasi, A.; Mattioli, R. Coronary artery bypass graft and mitral valvuloplasty in a patient with isolated ventricular non-compaction. Interact. Cardiovasc. Thorac. Surg. 2010, 11, 354–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stöllberger, C.; Finsterer, J.; Blazek, G. Isolated left ventricular abnormal trabeculation: Follow-up and association with neuromuscular disorders. Can. J. Cardiol. 2001, 17, 163–168. [Google Scholar] [PubMed]
- Jenni, R.; Oechslin, E.N.; van der Loo, B. Isolated ventricular non-compaction of the myocardium in adults. Heart 2007, 93, 11–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joong, A.; Hayes, D.A.; Anderson, B.R.; Zuckerman, W.A.; Carroll, S.J.; Lai, W.W. Comparison of Echocardiographic Diagnostic Criteria of Left Ventricular Noncompaction in a Pediatric Population. Pediatr. Cardiol. 2017, 38, 1493–1504. [Google Scholar] [CrossRef]
- Van Dalen, B.M.; Caliskan, K.; Soliman, O.I.; Nemes, A.; Vletter, W.B.; Ten Cate, F.J.; Geleijnse, M.L. Left ventricular solid body rotation in non-compaction cardiomyopathy: A potential new objective and quantitative functional diagnostic criterion. Eur. J. Heart Fail. 2008, 10, 1088–1093. [Google Scholar] [CrossRef] [Green Version]
- Yubbu, P.; Nawaytou, H.M.; Calderon-Anyosa, R.; Banerjee, A. Diagnostic value of myocardial deformation pattern in children with noncompaction cardiomyopathy. Int. J. Cardiovasc. Imaging 2018, 34, 1529–1539. [Google Scholar] [CrossRef]
- Sparrow, P.; Merchant, N.; Provost, Y.; Doyle, D.; Nguyen, E.; Paul, N. Cardiac MRI and CT features of inheritable and congenital conditions associated with sudden cardiac death. Eur. Radiol. 2009, 19, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Ichida, F.; Hamamichi, Y.; Miyawaki, T.; Ono, Y.; Kamiya, T.; Akagi, T.; Hamada, H.; Hirose, O.; Isobe, T.; Yamada, K.; et al. Clinical features of isolated noncompaction of the ventricular myocardium: Long-term clinical course, hemodynamic properties, and genetic background. J. Am. Coll. Cardiol. 1999, 34, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Grothoff, M.; Pachowsky, M.; Hoffmann, J.; Posch, M.; Klaassen, S.; Lehmkuhl, L.; Gutberlet, M. Value of cardiovascular MR in diagnosing left ventricular non-compaction cardiomyopathy and in discriminating between other cardiomyopathies. Eur. Radiol. 2012, 22, 2699–2709. [Google Scholar] [CrossRef] [Green Version]
- Thuny, F.; Jacquier, A.; Jop, B.; Giorgi, R.; Gaubert, J.Y.; Bartoli, J.M.; Moulin, G.; Habib, G. Assessment of left ventricular non-compaction in adults: Side-by-side comparison of cardiac magnetic resonance imaging with echocardiography. Arch. Cardiovasc. Dis. 2010, 103, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Saremi, F.; Grizzard, J.D.; Kim, R.J. Optimizing cardiac MR imaging: Practical remedies for artifacts. Radiographics 2008, 28, 1161–1187. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Selvanayagam, J.B.; Wiesmann, F.; Robson, M.D.; Francis, J.M.; Anderson, R.H.; Watkins, H.; Neubauer, S. Left ventricular non-compaction: Insights from cardiovascular magnetic resonance imaging. J. Am. Coll. Cardiol. 2005, 46, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Stacey, R.B.; Andersen, M.M.; St Clair, M.; Hundley, W.G.; Thohan, V. Comparison of systolic and diastolic criteria for isolated LV noncompaction in CMR. JACC Cardiovasc. Imaging 2013, 6, 931–940. [Google Scholar] [CrossRef] [Green Version]
- Jacquier, A.; Thuny, F.; Jop, B.; Giorgi, R.; Cohen, F.; Gaubert, J.Y.; Vidal, V.; Bartoli, J.M.; Habib, G.; Moulin, G. Measurement of trabeculated left ventricular mass using cardiac magnetic resonance imaging in the diagnosis of left ventricular non-compaction. Eur. Heart J. 2010, 31, 1098–1104. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; Kim, S.M.; Lee, S.C.; Chang, S.A.; Jang, S.Y.; Choe, Y.H. Quantification of left ventricular trabeculae using cardiovascular magnetic resonance for the diagnosis of left ventricular non-compaction: Evaluation of trabecular volume and refined semi-quantitative criteria. J. Cardiovasc. Magn. Reson. 2016, 18, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Captur, G.; Muthurangu, V.; Cook, C.; Flett, A.S.; Wilson, R.; Barison, A.; Sado, D.M.; Anderson, S.; McKenna, W.J.; Mohun, T.J.; et al. Quantification of left ventricular trabeculae using fractal analysis. J. Cardiovasc. Magn. Reson. 2013, 15, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stöllberger, C.; Finsterer, J.; Blazek, G. Isolated left ventricular abnormal trabeculation is a cardiac manifestation of neuromuscular disorders. Cardiology 2000, 94, 72–76. [Google Scholar] [CrossRef]
- Melendez-Ramirez, G.; Castillo-Castellon, F.; Espinola-Zavaleta, N.; Meave, A.; Kimura-Hayama, E.T. Left ventricular noncompaction: A proposal of new diagnostic criteria by multidetector computed tomography. J. Cardiovasc. Comput. Tomogr. 2012, 6, 346–354. [Google Scholar] [CrossRef]
- Macaione, F.; Meloni, A.; Positano, V.; Pistoia, L.; Barison, A.; Di Lisi, D.; Spasiano, A.; Campisi, S.; Spiga, A.; Righi, R.; et al. The planimetric Grothoff’s criteria by cardiac magnetic resonance can improve the specificity of left ventricular non-compaction diagnosis in thalassemia intermedia. Int. J. Cardiovasc. Imaging 2020, 36, 1105–1112. [Google Scholar] [CrossRef]
- Yun, H.; Zeng, M.S.; Jin, H.; Yang, S. Isolated noncompaction of ventricular myocardium: A magnetic resonance imaging study of 11 patients. Korean J. Radiol. 2011, 12, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Vogel-Claussen, J.; Rochitte, C.E.; Wu, K.C.; Kamel, I.R.; Foo, T.K.; Lima, J.A.; Bluemke, D.A. Delayed enhancement MR imaging: Utility in myocardial assessment. Radiographics 2006, 26, 795–810. [Google Scholar] [CrossRef] [PubMed]
- Jassal, D.S.; Nomura, C.H.; Neilan, T.G.; Holmvang, G.; Fatima, U.; Januzzi, J.; Brady, T.J.; Cury, R.C. Delayed enhancement cardiac MR imaging in noncompaction of left ventricular myocardium. J. Cardiovasc. Magn. Reson. 2006, 8, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Jenni, R.; Wyss, C.A.; Oechslin, E.N.; Kaufmann, P.A. Isolated ventricular noncompaction is associated with coronary microcirculatory dysfunction. J. Am. Coll. Cardiol. 2002, 39, 450–454. [Google Scholar] [CrossRef] [Green Version]
- Dodd, J.D.; Holmvang, G.; Hoffmann, U.; Ferencik, M.; Abbara, S.; Brady, T.J.; Cury, R.C. Quantification of left ventricular noncompaction and trabecular delayed hyperenhancement with cardiac MRI: Correlation with clinical severity. AJR Am. J. Roentgenol. 2007, 189, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Mavrogeni, S.I.; Markousis-Mavrogenis, G.; Vartela, V.; Manolopoulou, D.; Abate, E.; Hamadanchi, A.; Rigopoulos, A.G.; Kolovou, G.; Noutsias, M. The pivotal role of cardiovascular imaging in the identification and risk stratification of non-compaction cardiomyopathy patients. Heart Fail Rev. 2020, 25, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Haukilahti, M.A.; Eranti, A.; Kenttä, T.; Huikuri, H.V. QRS Fragmentation Patterns Representing Myocardial Scar Need to Be Separated from Benign Normal Variants: Hypotheses and Proposal for Morphology based Classification. Front. Physiol. 2016, 7, 653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, M.K.; Maskoun, W.; Shen, C.; Michael, M.A.; Suradi, H.; Desai, M.; Subbarao, R.; Bhakta, D. Fragmented QRS on twelve-lead electrocardiogram predicts arrhythmic events in patients with ischemic and nonischemic cardiomyopathy. Heart Rhythm. 2010, 7, 74–80. [Google Scholar] [CrossRef]
- Steffel, J.; Kobza, R.; Oechslin, E.; Jenni, R.; Duru, F. Electrocardiographic characteristics at initial diagnosis in patients with isolated left ventricular noncompaction. Am. J. Cardiol. 2009, 104, 984–989. [Google Scholar] [CrossRef] [Green Version]
- Gati, S.; Rajani, R.; Carr-White, G.S.; Chambers, J.B. Adult left ventricular noncompaction: Reappraisal of current diagnostic imaging modalities. JACC Cardiovasc. Imaging 2014, 7, 1266–1275. [Google Scholar] [CrossRef] [Green Version]
- Udeoji, D.U.; Philip, K.J.; Morrissey, R.P.; Phan, A.; Schwarz, E.R. Left ventricular noncompaction cardiomyopathy: Updated review. Ther. Adv. Cardiovasc. Dis. 2013, 7, 260–273. [Google Scholar] [CrossRef]
- Seyler, C.; Meder, B.; Weis, T.; Schwaneberg, T.; Weitmann, K.; Hoffmann, W.; Katus, H.A.; Dösch, A. TranslatiOnal Registry for CardiomyopatHies (TORCH)-rationale and first results. ESC Heart Fail. 2017, 4, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Waning, J.I.; Caliskan, K.; Hoedemaekers, Y.M.; van Spaendonck-Zwarts, K.Y.; Baas, A.F.; Boekholdt, S.M.; van Melle, J.P.; Teske, A.J.; Asselbergs, F.W.; Backx, A.P.C.M.; et al. Genetics, Clinical Features, and Long-Term Outcome of Noncompaction Cardiomyopathy. J. Am. Coll. Cardiol. 2018, 71, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Van Waning, J.I.; Caliskan, K.; Michels, M.; Schinkel, A.F.L.; Hirsch, A.; Dalinghaus, M.; Hoedemaekers, Y.M.; Wessels, M.W.; IJpma, A.S.; Hofstra, R.M.W.; et al. Cardiac Phenotypes, Genetics, and Risks in Familial Noncompaction Cardiomyopathy. J. Am. Coll. Cardiol. 2019, 73, 1601–1611. [Google Scholar] [CrossRef] [PubMed]
- Adabifirouzjaei, F.; Igata, S.; DeMaria, A.N. Hypertrabeculation; a phenotype with Heterogeneous etiology. Prog. Cardiovasc. Dis. 2021, 68, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Musunuru, K.; Hershberger, R.E.; Day, S.M.; Klinedinst, N.J.; Landstrom, A.P.; Parikh, V.N.; Prakash, S.; Semsarian, C.; Sturm, A.C.; American Heart Association Council on Genomic and Precision Medicine. Genetic Testing for Inherited Cardiovascular Diseases: A Scientific Statement from the American Heart Association. Circ. Genom. Precis Med. 2020, 13, e000067. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC SDG. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Takamatsu, M.; Kamohara, K.; Sato, M.; Koga, Y. Effect of Noncompacted Myocardial Resection on Isolated Left Ventricular Noncompaction. Ann. Thorac. Surg. 2020, 110, e387–e389. [Google Scholar] [CrossRef]
- Bertini, M.; Ziacchi, M.; Biffi, M.; Biagini, E.; Rocchi, G.; Martignani, C.; Ferlito, M.; Pasquale, F.; Cervi, E.; Branzi, A.; et al. Effects of cardiac resynchronisation therapy on dilated cardiomyopathy with isolated ventricular non-compaction. Heart 2011, 97, 295–300. [Google Scholar] [CrossRef]
- Oginosawa, Y.; Nogami, A.; Soejima, K.; Aonuma, K.; Kubota, S.; Sato, T.; Sugiyasu, A.; Yoshida, K.; Kowase, S. Effect of cardiac resynchronization therapy in isolated ventricular noncompaction in adults: Follow-up of four cases. J. Cardiovasc. Electrophysiol. 2008, 19, 935–938. [Google Scholar] [CrossRef]
- Muser, D.; Nucifora, G.; Gianfagna, E.; Pavoni, D.; Rebellato, L.; Facchin, D.; Daleffe, E.; Proclemer, A. Clinical spectrum of isolated left ventricular noncompaction: Thromboembolic events, malignant left ventricular arrhythmias, and refractory heart failure. J. Am. Coll. Cardiol. 2014, 63, e39. [Google Scholar] [CrossRef] [Green Version]
- Sohns, C.; Ouyang, F.; Volkmer, M.; Metzner, A.; Nürnberg, J.H.; Ventura, R.; Gerecke, B.; Jansen, H.; Reinhardt, A.; Kuck, K.H.; et al. Therapy of ventricular arrhythmias in patients suffering from isolated left ventricular non-compaction cardiomyopathy. Europace 2019, 21, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, C.; Lavalle, C.; Magnocavallo, M.; Alfarano, M.; Mariani, M.V.; Bernardini, F.; Della Rocca, D.G.; Galardo, G.; Severino, P.; Di Lullo, L.; et al. A proposed strategy for anticoagulation therapy in noncompaction cardiomyopathy. ESC Heart Fail. 2022, 9, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Pöyhönen, P.; Kuusisto, J.; Järvinen, V.; Pirinen, J.; Räty, H.; Lehmonen, L.; Paakkanen, R.; Martinez-Majander, N.; Putaala, J.; Sinisalo, J. Left ventricular non-compaction as a potential source for cryptogenic ischemic stroke in the young: A case-control study. PLoS ONE 2020, 15, e0237228. [Google Scholar] [CrossRef] [PubMed]
- Homma, S.; Thompson, J.L.; Pullicino, P.M.; Levin, B.; Freudenberger, R.S.; Teerlink, J.R.; Ammon, S.E.; Graham, S.; Sacco, R.L.; Mann, D.L.; et al. Warfarin and aspirin in patients with heart failure and sinus rhythm. N. Engl. J. Med. 2012, 366, 1859–1869. [Google Scholar] [CrossRef] [Green Version]
- Pullicino, P.M.; Qian, M.; Sacco, R.L.; Freudenberger, R.; Graham, S.; Teerlink, J.R.; Mann, D.; Di Tullio, M.R.; Ponikowski, P.; Lok, D.J.; et al. Recurrent stroke in the warfarin versus aspirin in reduced cardiac ejection fraction (WARCEF) trial. Cerebrovasc. Dis. 2014, 38, 176–181. [Google Scholar] [CrossRef] [Green Version]
- Pelliccia, A.; Solberg, E.E.; Papadakis, M.; Adami, P.E.; Biffi, A.; Caselli, S.; La Gerche, A.; Niebauer, J.; Pressler, A.; Schmied, C.M.; et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: Position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2019, 40, 19–33. [Google Scholar] [CrossRef]
- Aung, N.; Doimo, S.; Ricci, F.; Sanghvi, M.M.; Pedrosa, C.; Woodbridge, S.P.; Al-Balah, A.; Zemrak, F.; Khanji, M.Y.; Munroe, P.B.; et al. Prognostic Significance of Left Ventricular Noncompaction: Systematic Review and Meta-Analysis of Observational Studies. Circ. Cardiovasc. Imaging 2020, 13, e009712. [Google Scholar] [CrossRef]
- Zemrak, F.; Ahlman, M.A.; Captur, G.; Mohiddin, S.A.; Kawel-Boehm, N.; Prince, M.R.; Moon, J.C.; Hundley, W.G.; Lima, J.A.; Bluemke, D.A.; et al. The relationship of left ventricular trabeculation to ventricular function and structure over a 9.5-year follow-up: The MESA study. J. Am. Coll. Cardiol. 2014, 64, 1971–1980. [Google Scholar] [CrossRef] [Green Version]
- Murphy, R.T.; Thaman, R.; Blanes, J.G.; Ward, D.; Sevdalis, E.; Papra, E.; Kiotsekoglou, A.; Kiotsekolglou, A.; Tome, M.T.; Pellerin, D.; et al. Natural history and familial characteristics of isolated left ventricular non-compaction. Eur. Heart J. 2005, 26, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, V.R.; Lyle, M.; Miranda, W.R.; Farwati, M.; Isath, A.; Patlolla, S.H.; Hodge, D.O.; Asirvatham, S.J.; Kapa, S.; Deshmukh, A.J.; et al. Long-Term Survival of Patients With Left Ventricular Noncompaction. J. Am. Heart Assoc. 2021, 10, e015563. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. iLVNC. NC morphology in left ventricles with normal systolic and diastolic function, size, and wall thickness; |
| 2. LVNC with LV dilation and dysfunction at onset, such as in the paradigmatic infantile CMP of Barth syndrome |
| 3. LVNC in hearts fulfilling the diagnostic criteria for DCM, HCM, RCM, or ARVC; |
| 4. LVNC associated with congenital heart disease; |
| 5. Syndromes with LVNC, either sporadic or familial, in which the noncompaction morphology is one of the cardiac traits associated with both monogenic defects and chromosomal anomalies, i.e., complex syndromes with several multiorgan defects; |
| 6. Acquired and potentially reversible LVNC, which has been reported in athletes; it has also been reported in sickle cell anemia, pregnancy, myopathies, and chronic renal failure; |
| 7. Right ventricular noncompaction, concomitant with that of the left ventricle, or present as a unique anatomic area of NC. |
| Author | Method | Diagnostic Criteria | Cardiac Phase | Cut-Off |
|---|---|---|---|---|
| Petersen [42] | CMR | Ratio of compacted epicardium and non-compacted endocardium | End diastole | NC/C ≥ 2.3 |
| Stacey [43] | CMR | Ratio of compacted epicardium and non-compacted endocardium | Short axis, end-systole | NC/C ratio of ≥ 2.0 |
| Jacquier [44] | CMR | A value of trabeculated LV mass above 20% of the global mass of the LV | End diastole | LV trabeculated mass > 20% |
| Grothoff [39] | CMR | Ratio of total LV trabeculated mass to global myocardial mass | End systole | Trabeculated ventricular mass greater than 25% of the global left ventricular mass; noncompacted mass greater than 15 g/m2 |
| Choi [45] | CMR | A percentage of trabeculated myocardial volume of the total myocardial volume of the LV | End-diastole, long-axis | LV trabeculated volume > 35% |
| Captur [46] | CMR | Maximal fractal dimension | End diastole | Global fractal dimension > 1.26; apical fractal dimension > 1.3 |
| Chin [3] | ECHO | The ratio of the distance from the deepest trabecular recess to the epicardial surface (X) and the distance from the tip of the trabeculation to the epicardial surface (Y) | Long axis, end diastole | X/Y ≤ 0.5 |
| Stöllberger [47] | ECHO | Ratio of compacted and non-compacted endocardium. Presence of at least 3 trabeculations protruding in the left ventricle apically from papillary muscle, presence of the blood flow between trabeculations. | Four chamber, end diastole | NC/C > 2 |
| Jenni [33] | ECHO | Ratio of compacted and non-compacted endocardium. Absence of coexisting cardiac abnormalities, the presence of deep trabeculations, which are filled with blood | Short axis, end systole | NC/C ≥ 2 |
| Melendez-Ramirez [48] | MDCT | Ratio of compacted and non-compacted endocardium in at least 2 or more segments | All 17 segments, end diastole | NC/C ratio > 2.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paluszkiewicz, J.; Milting, H.; Kałużna-Oleksy, M.; Pyda, M.; Janus, M.; Körperich, H.; Piran, M. Left Ventricular Non-Compaction Cardiomyopathy-Still More Questions than Answers. J. Clin. Med. 2022, 11, 4135. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144135
Paluszkiewicz J, Milting H, Kałużna-Oleksy M, Pyda M, Janus M, Körperich H, Piran M. Left Ventricular Non-Compaction Cardiomyopathy-Still More Questions than Answers. Journal of Clinical Medicine. 2022; 11(14):4135. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144135
Chicago/Turabian StylePaluszkiewicz, Jerzy, Hendrik Milting, Marta Kałużna-Oleksy, Małgorzata Pyda, Magdalena Janus, Hermann Körperich, and Misagh Piran. 2022. "Left Ventricular Non-Compaction Cardiomyopathy-Still More Questions than Answers" Journal of Clinical Medicine 11, no. 14: 4135. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144135