
Pre-Interventional 3D-Printing-Assisted Planning of Flow Disrupter Implantation for the Treatment of an Intracranial Aneurysm

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
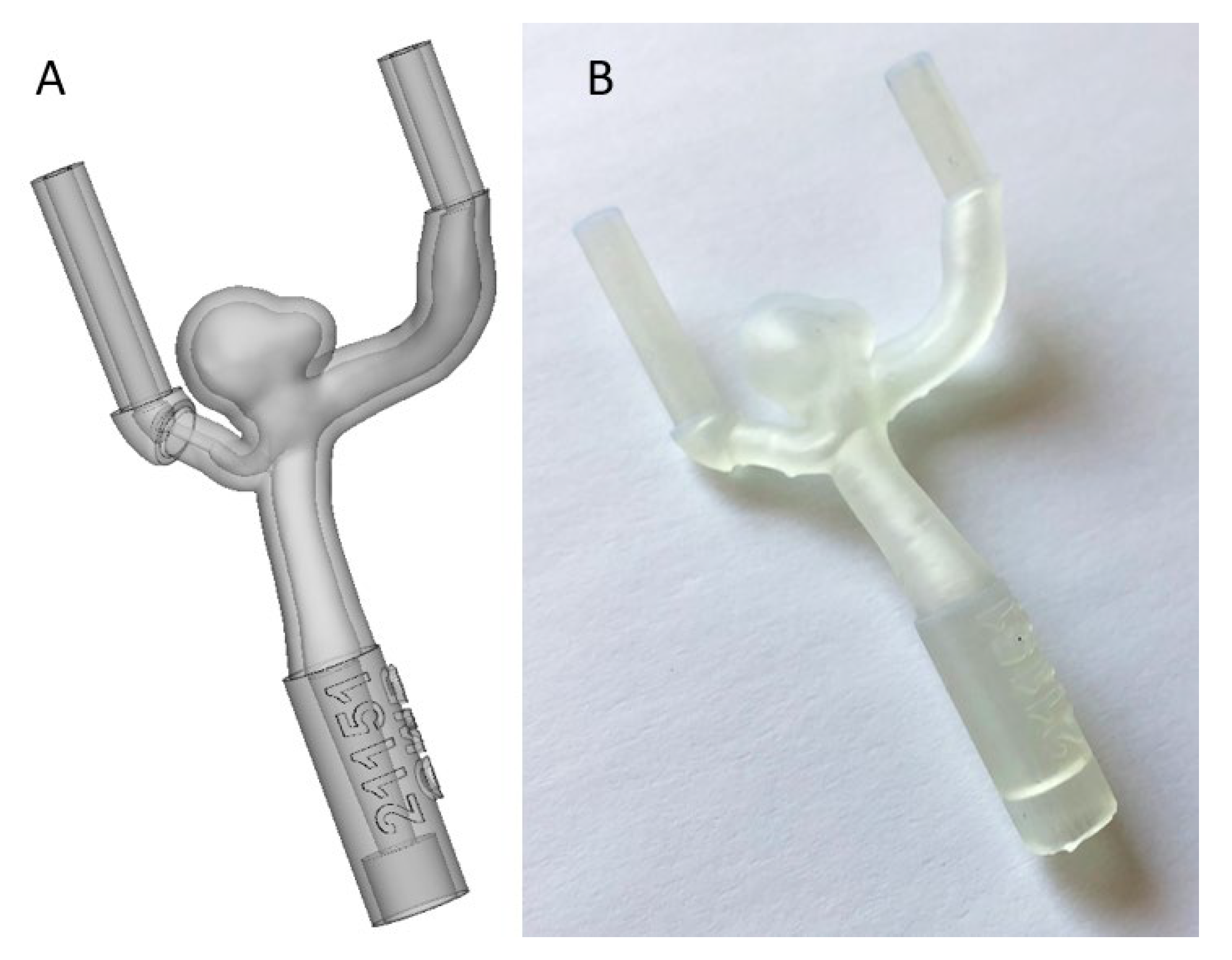
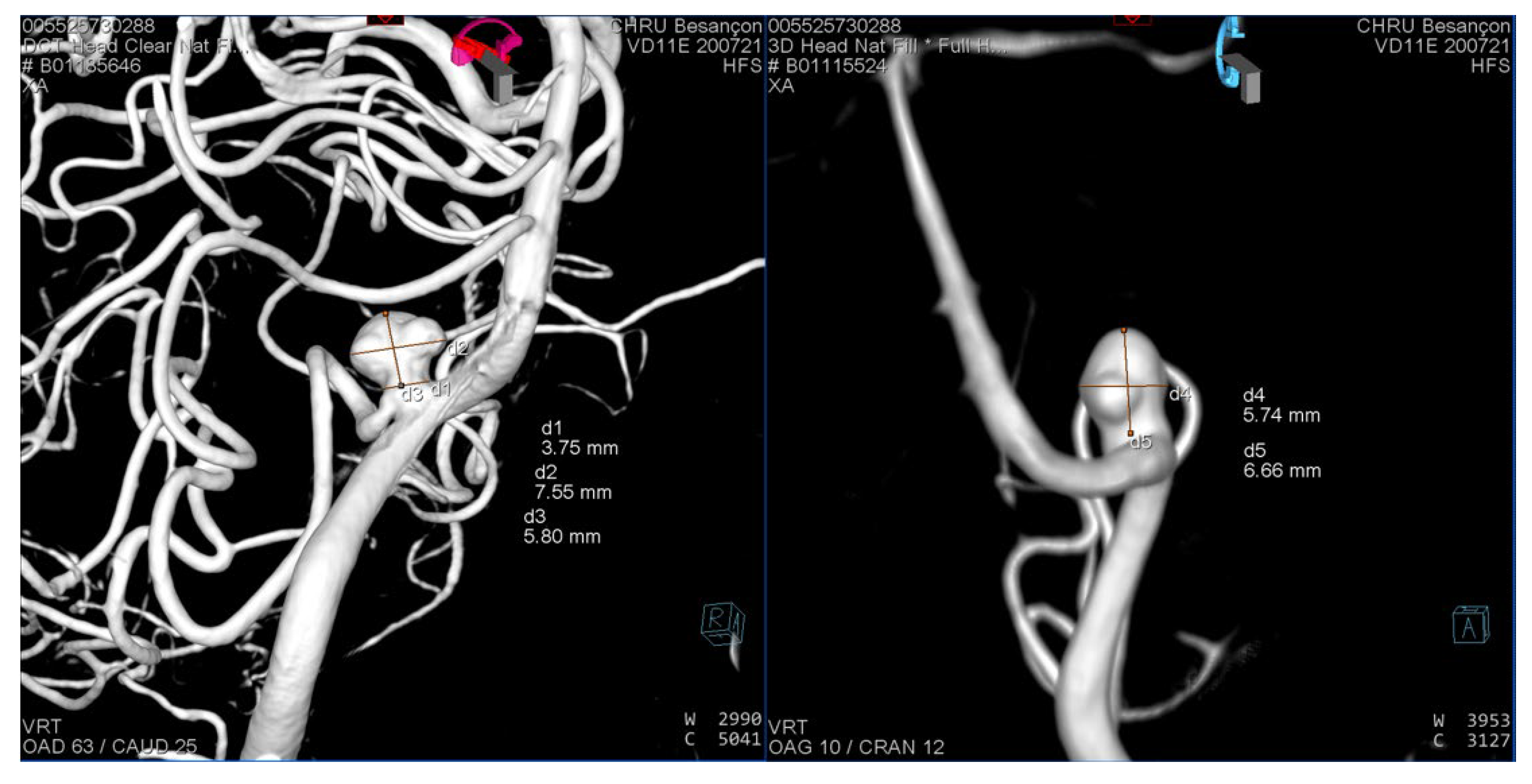
2.1. Segmentation of the 3D Model
2.2. Production of the 3D Model
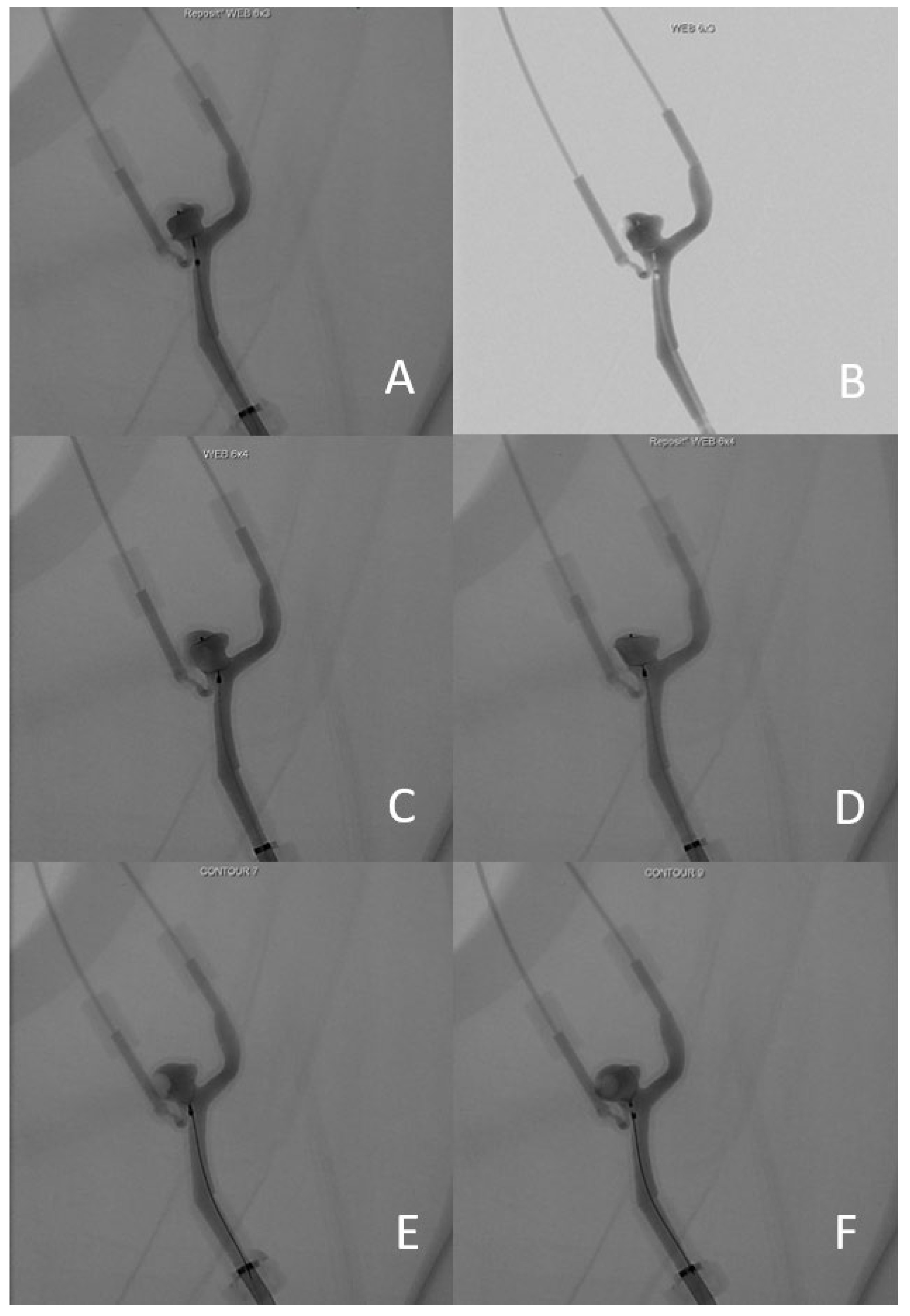
2.3. Testing the 3D Model
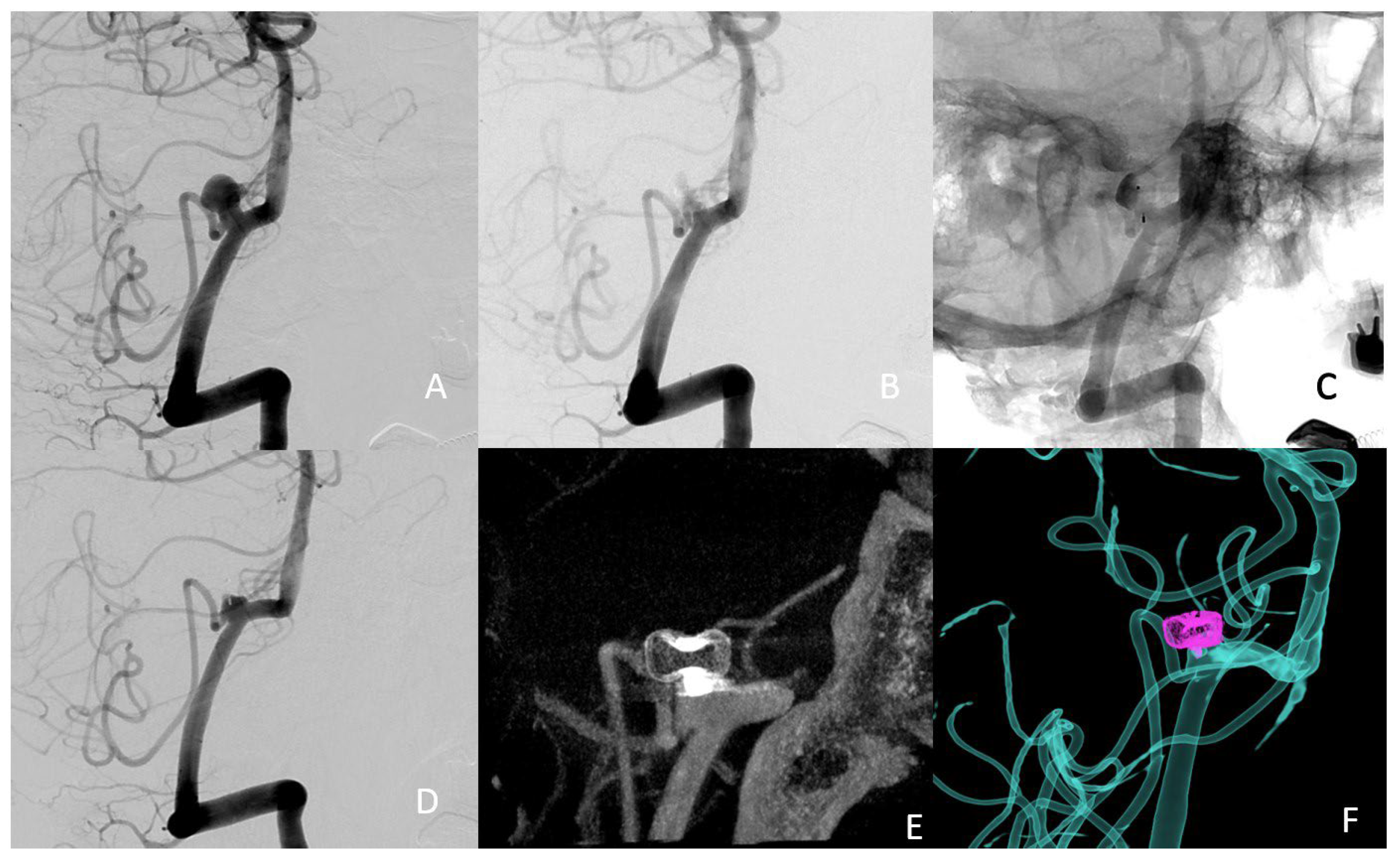
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piotin, M.; Biondi, A.; Sourour, N.; Mounayer, C.; Jaworski, M.; Mangiafico, S.; Andersson, T.; Söderman, M.; Goffette, P.; Anxionnat, R.; et al. The LUNA Aneurysm Embolization System for Intracranial Aneurysm Treatment: Short-Term, Mid-Term and Long-Term Clinical and Angiographic Results. J. Neurointerv. Surg. 2018, 10, e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klisch, J.; Sychra, V.; Strasilla, C.; Liebig, T.; Fiorella, D. The Woven EndoBridge Cerebral Aneurysm Embolization Device (WEB II): Initial Clinical Experience. Neuroradiology 2011, 53, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Bhogal, P.; Lylyk, I.; Chudyk, J.; Perez, N.; Bleise, C.; Lylyk, P. The Contour-Early Human Experience of a Novel Aneurysm Occlusion Device. Clin. Neuroradiol. 2021, 31, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Cagnazzo, F.; Marnat, G.; Ferreira, I.; Daube, P.; Derraz, I.; Dargazanli, C.; Lefevre, P.-H.; Gascou, G.; Riquelme, C.; Morganti, R.; et al. Comparison of Woven EndoBridge Device Sizing with Conventional Measurements and Virtual Simulation Using the Sim&Size Software: A Multicenter Experience. J. NeuroInterv. Surg. 2021, 13, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Nagassa, R.G.; McMenamin, P.G.; Adams, J.W.; Quayle, M.R.; Rosenfeld, J.V. Advanced 3D Printed Model of Middle Cerebral Artery Aneurysms for Neurosurgery Simulation. 3D Print. Med. 2019, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-L.; Yuan, Z.-G.; Qian, G.-L.; Bao, W.-Q.; Jin, G.-L. 3D Printing of Intracranial Aneurysm Based on Intracranial Digital Subtraction Angiography and Its Clinical Application. Medicine 2018, 97, e11103. [Google Scholar] [CrossRef] [PubMed]
- Waqas, M.; Mokin, M.; Lim, J.; Vakharia, K.; Springer, M.E.; Meess, K.M.; Ducharme, R.W.; Ionita, C.N.; Nagesh, S.V.S.; Gutierrez, L.C.; et al. Design and Physical Properties of 3-Dimensional Printed Models Used for Neurointervention: A Systematic Review of the Literature. Neurosurgery 2020, 87, E445–E453. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, P.; Prabhu, S.P.; Flynn, K.; Orbach, D.B.; Smith, E. Optimizing Cerebrovascular Surgical and Endovascular Procedures in Children via Personalized 3D Printing. J. Neurosurg. Pediatr. 2015, 16, 584–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arthur, A.; Hoit, D.; Coon, A.; Delgado Almandoz, J.E.; Elijovich, L.; Cekirge, S.; Fiorella, D.; WEB-IT Study Investigators. Physician Training Protocol within the WEB Intrasaccular Therapy (WEB-IT) Study. J. Neurointerv. Surg. 2018, 10, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Szary, J.; Luis, M.S.; Mikulski, S.; Patel, A.; Schulz, F.; Tretiakow, D.; Fercho, J.; Jaguszewska, K.; Frankiewicz, M.; Pawłowska, E.; et al. The Role of 3D Printing in Planning Complex Medical Procedures and Training of Medical Professionals—Cross-Sectional Multispecialty Review. Int. J. Environ. Res. Public Health 2022, 19, 3331. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Narayanan, M.D.K.; Umana, G.E.; Montemurro, N.; Chaurasia, B.; Deora, H. Virtual Reality in Neurosurgery: Beyond Neurosurgical Planning. Int. J. Environ. Res. Public Health 2022, 19, 1719. [Google Scholar] [CrossRef] [PubMed]
- Gestel, F.V.; Frantz, T.; Vannerom, C.; Verhellen, A.; Gallagher, A.G.; Elprama, S.A.; Jacobs, A.; Buyl, R.; Bruneau, M.; Jansen, B.; et al. The Effect of Augmented Reality on the Accuracy and Learning Curve of External Ventricular Drain Placement. Neurosurg. Focus 2021, 51, E8. [Google Scholar] [CrossRef] [PubMed]
- Panesar, S.S.; Magnetta, M.; Mukherjee, D.; Abhinav, K.; Branstetter, B.F.; Gardner, P.A.; Iv, M.; Fernandez-Miranda, J.C. Patient-Specific 3-Dimensionally Printed Models for Neurosurgical Planning and Education. Neurosurg. Focus 2019, 47, E12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Zhang, Y.; Ding, C.; Ting, K.; Yoon, S.; Sahak, H.; Hope, A.; McLachlin, S.; Crawford, E.; Hardisty, M.; et al. Virtual Reality as a Learning Tool in Spinal Anatomy and Surgical Techniques. N. Am. Spine Soc. J. (NASSJ) 2021, 6, 100063. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Condino, S.; Cattari, N.; D’Amato, R.; Ferrari, V.; Cutolo, F. Augmented Reality-Assisted Craniotomy for Parasagittal and Convexity En Plaque Meningiomas and Custom-Made Cranio-Plasty: A Preliminary Laboratory Report. Int. J. Environ. Res. Public Health 2021, 18, 9955. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charbonnier, G.; Primikiris, P.; Billottet, B.; Louvrier, A.; Vancheri, S.; Ferhat, S.; Biondi, A. Pre-Interventional 3D-Printing-Assisted Planning of Flow Disrupter Implantation for the Treatment of an Intracranial Aneurysm. J. Clin. Med. 2022, 11, 2950. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112950
Charbonnier G, Primikiris P, Billottet B, Louvrier A, Vancheri S, Ferhat S, Biondi A. Pre-Interventional 3D-Printing-Assisted Planning of Flow Disrupter Implantation for the Treatment of an Intracranial Aneurysm. Journal of Clinical Medicine. 2022; 11(11):2950. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112950
Chicago/Turabian StyleCharbonnier, Guillaume, Panagiotis Primikiris, Benjamin Billottet, Aurélien Louvrier, Sergio Vancheri, Serine Ferhat, and Alessandra Biondi. 2022. "Pre-Interventional 3D-Printing-Assisted Planning of Flow Disrupter Implantation for the Treatment of an Intracranial Aneurysm" Journal of Clinical Medicine 11, no. 11: 2950. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112950