
Relationship between Metabolic Syndrome and Clinical Outcome in Patients Treated with Drug-Eluting Stenting after Rotational Atherectomy for Complex Calcified Coronary Lesions

Abstract
:1. Introduction
2. Methods
2.1. Patient Data
2.2. Definition of MS
2.3. Study Endpoint
2.4. Statistical Analysis
3. Results
3.1. Study Design and Patients
3.2. Baseline Characteristics
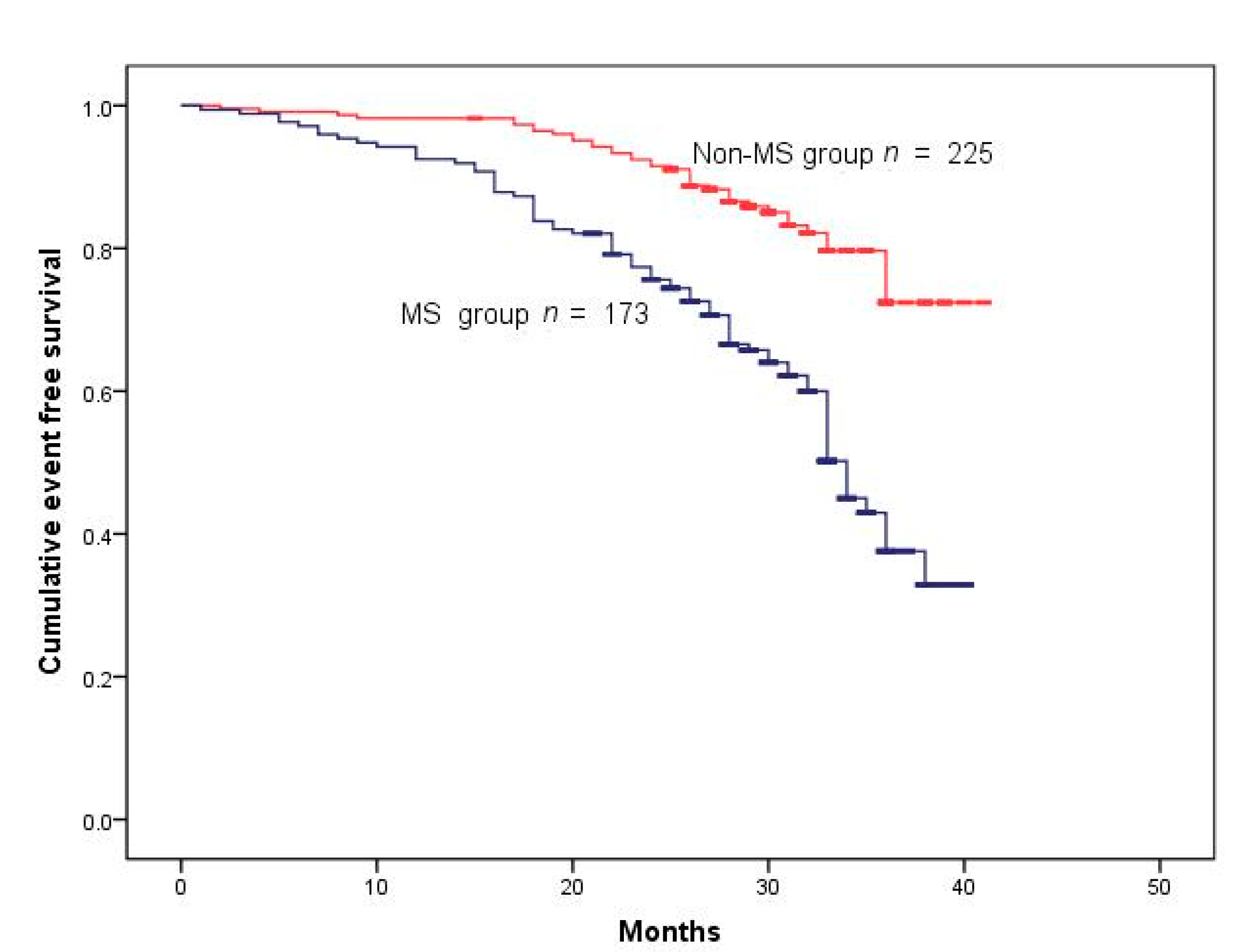
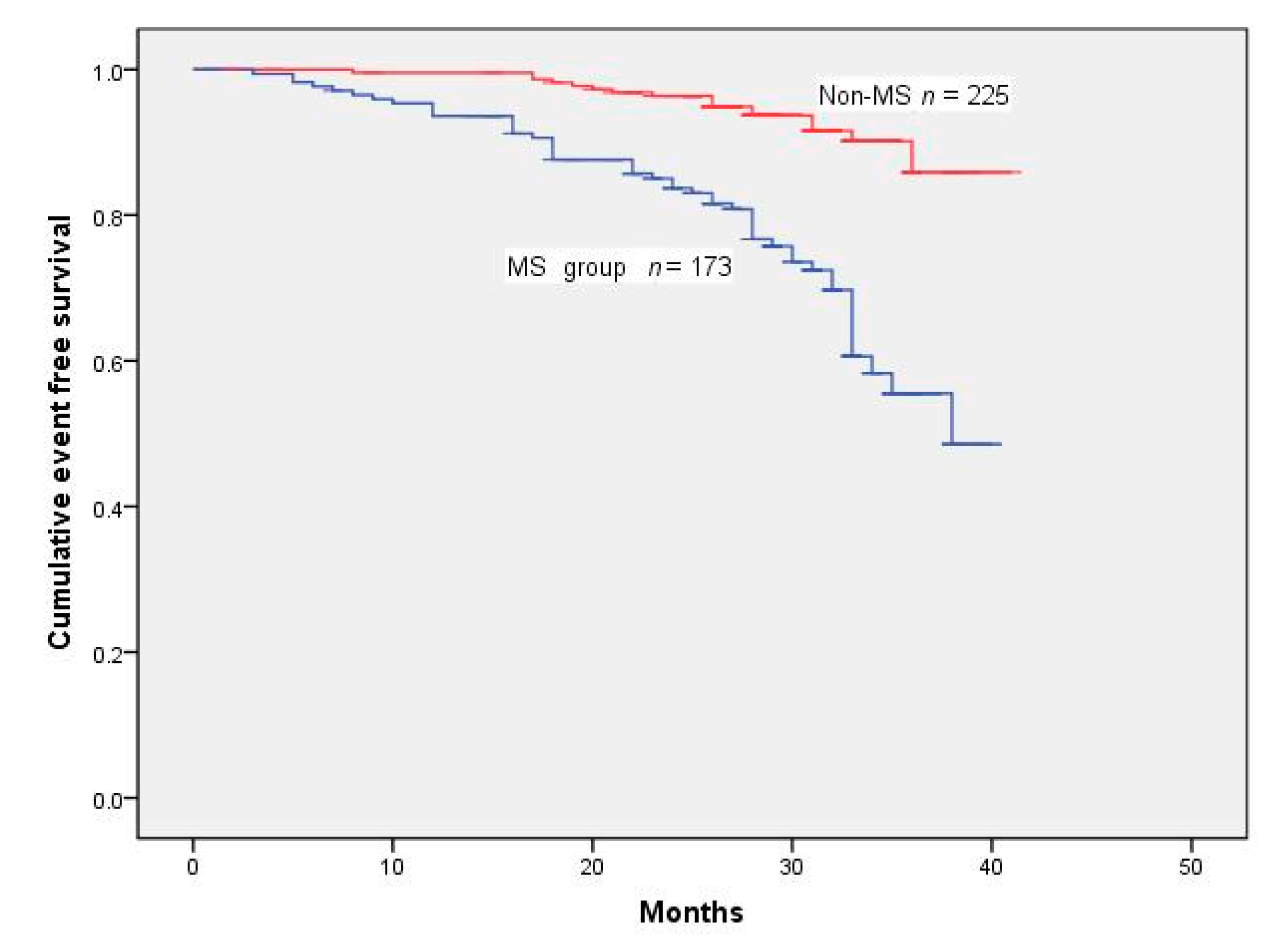
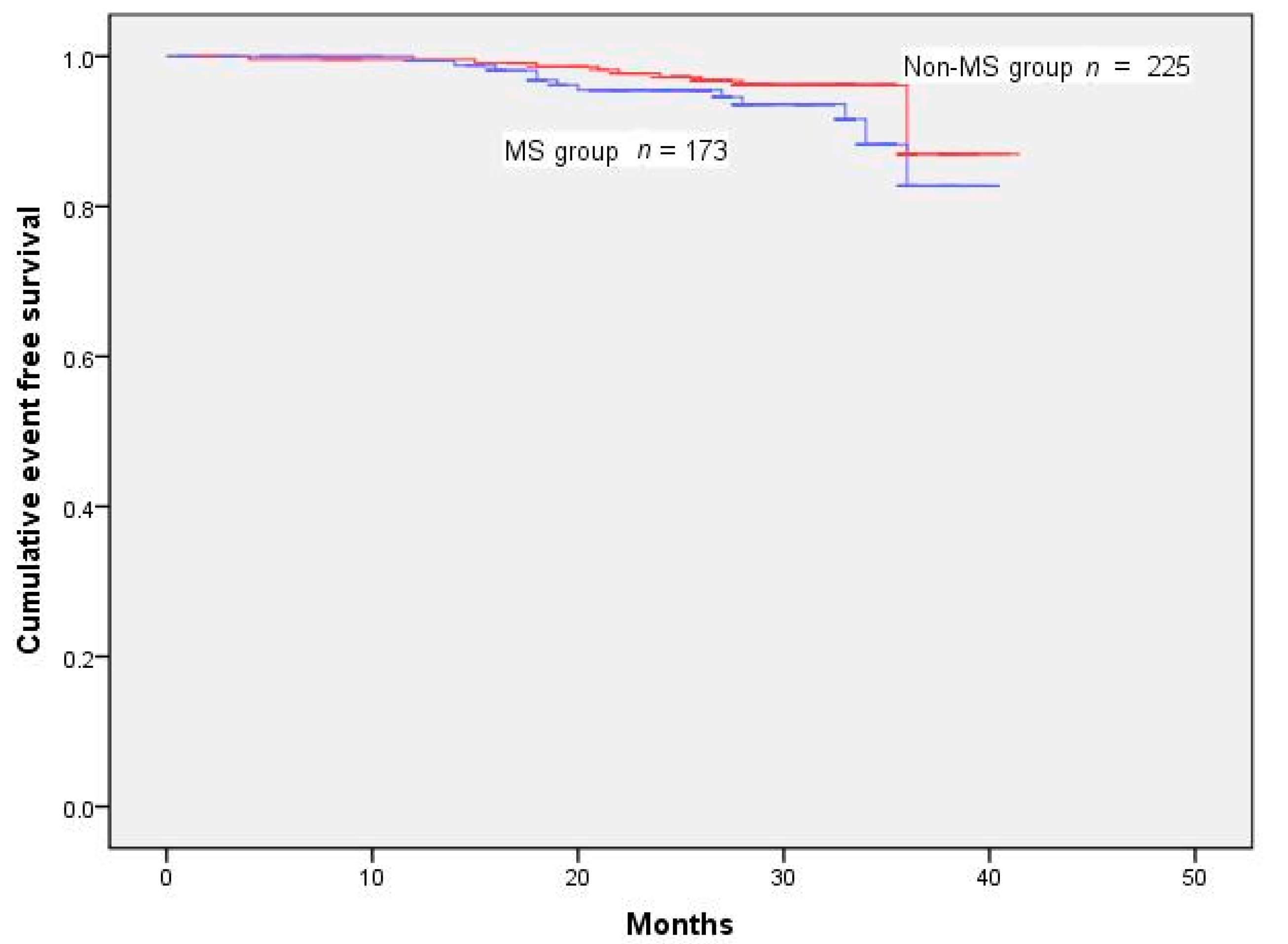
3.3. Analysis of Mortality and MACE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Madhavan, M.V.; Tarigopula, M.; Mintz, G.S.; Maehara, A.; Stone, G.W.; Généreux, P. Coronary artery calcification: Pathogenesis and prognostic implications. J. Am. Coll. Cardiol. 2014, 63, 1703–1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, J.W.; Blaha, M.J.; Defilippis, A.P.; Budoff, M.J.; Nasir, K.; Blumenthal, R.S.; Jones, S.R. Coronary artery calcium progression: An important clinical measurement? A review of published reports. J. Am. Coll. Cardiol. 2010, 56, 1613–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakahara, T.; Dweck, M.R.; Narula, N.; Pisapia, D.; Narula, J.; Strauss, H.W. Coronary Artery Calcification: From Mechanism to Molecular Imaging. JACC Cardiovasc. Imaging 2017, 10, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Keshawarz, A.; Pyle, L.; Alman, A.; Sassano, C.; Westfeldt, E.; Sippl, R.; Snell-Bergeon, J. Type 1 Diabetes Accelerates Progression of Coronary Artery Calcium Over the Menopausal Transition: The CACTI Study. Diabetes Care 2019, 42, 2315–2321. [Google Scholar] [CrossRef] [Green Version]
- Wong, N.D.; Nelson, J.C.; Granston, T.; Bertoni, A.G.; Blumenthal, R.S.; Carr, J.J.; Guerci, A.; Jacobs, D.R., Jr.; Kronmal, R.; Liu, K.; et al. Metabolic syndrome, diabetes, and incidence and progression of coronary calcium: The Multiethnic Study of Atherosclerosis study. JACC Cardiovasc. Imaging 2012, 5, 358–366. [Google Scholar] [CrossRef] [Green Version]
- McClelland, R.L.; Jorgensen, N.W.; Budoff, M.; Blaha, M.J.; Post, W.S.; Kronmal, R.A.; Bild, D.E.; Shea, S.; Liu, K.; Watson, K.E.; et al. 10-Year Coronary Heart Disease Risk Prediction Using Coronary Artery Calcium and Traditional Risk Factors: Derivation in the MESA (Multi-Ethnic Study of Atherosclerosis) with Validation in the HNR (Heinz Nixdorf Recall) Study and the DHS (Dallas Heart Study). J. Am. Coll. Cardiol. 2015, 66, 1643–1653. [Google Scholar] [CrossRef] [Green Version]
- Cardarelli, R.; Hall, A.; Rankin, W. Coronary Artery Calcium Progression Is Associated with Cardiovascular Events Among Asymptomatic Individuals: From the North Texas Primary Care Practice-based Research Network (NorTex-PBRN). J. Am. Board. Fam. Med. 2017, 30, 592–600. [Google Scholar] [CrossRef] [Green Version]
- Généreux, P.; Redfors, B.; Witzenbichler, B.; Arsenault, M.P.; Weisz, G.; Stuckey, T.D.; Rinaldi, M.J.; Neumann, F.J.; Christopher Metzger, D.; Henry, T.D.; et al. Two-year outcomes after percutaneous coronary intervention of calcified lesions with drug-eluting stents. Int. J. Cardiol. 2017, 231, 61–67. [Google Scholar] [CrossRef]
- Sharma, S.K.; Tomey, M.I.; Teirstein, P.S.; Kini, A.S.; Reitman, A.B.; Lee, A.C.; Généreux, P.; Chambers, J.W.; Grines, C.L.; Himmelstein, S.I.; et al. North American Expert Review of Rotational Atherectomy. Circ. Cardiovasc. Interv. 2019, 12, e007448. [Google Scholar] [CrossRef]
- Kammerlander, A.A.; Mayrhofer, T.; Ferencik, M.; Pagidipati, N.J.; Karady, J.; Ginsburg, G.S.; Lu, M.T.; Bittner, D.O.; Puchner, S.B.; Bihlmeyer, N.A.; et al. Association of Metabolic Phenotypes With Coronary Artery Disease and Cardiovascular Events in Patients With Stable Chest Pain. Diabetes Care 2021, 44, 1038–1045. [Google Scholar] [CrossRef]
- Bin, H.; Yujie, Z.; Yuyang, L.; Dongmei, S.; Yingxin, Z.; Dean, J.; Shiwei, Y.; Zhe, F.; Bin, N. Impact of metabolic syndrome on clinical outcomes after drug-eluting stent implantation in patients with coronary artery disease. Angiology 2011, 62, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Jia, S.D.; Liu, Y.; Xu, J.J.; Gao, Z.; Song, Y.; Tang, X.F.; Jiang, P.; Zhao, X.Y.; Song, L.; et al. The impact of metabolic syndrome and its individual components on long-term prognosis of patients undergoing percutaneous coronary intervention. Zhonghua Yi Xue Za Zhi 2020, 100, 1623–1628. [Google Scholar] [CrossRef] [PubMed]
- Younis, A.; Younis, A.; Tzur, B.; Peled, Y.; Shlomo, N.; Goldenberg, I.; Fisman, E.Z.; Tenenbaum, A.; Klempfner, R. Metabolic syndrome is independently associated with increased 20-year mortality in patients with stable coronary artery disease. Cardiovasc. Diabetol. 2016, 15, 149. [Google Scholar] [CrossRef] [Green Version]
- Lopes, N.H.; Paulitsch, F.S.; Pereira, A.C.; Góis, A.F.; Gagliardi, A.; Garzillo, C.L.; Ferreira, J.F.; Stolf, N.A.; Hueb, W. Impact of metabolic syndrome on the outcome of patients with stable coronary artery disease: 2-year follow-up of the MASS II study. Coron. Artery Dis. 2008, 19, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Levantesi, G.; Macchia, A.; Marfisi, R.; Franzosi, M.G.; Maggioni, A.P.; Nicolosi, G.L.; Schweiger, C.; Tavazzi, L.; Tognoni, G.; Valagussa, F.; et al. Metabolic syndrome and risk of cardiovascular events after myocardial infarction. J. Am. Coll. Cardiol. 2005, 46, 277–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Shiode, N.; Kozuma, K.; Aoki, J.; Awata, M.; Nanasato, M.; Tanabe, K.; Yamaguchi, J.; Kusano, H.; Nie, H.; Kimura, T. The impact of coronary calcification on angiographic and 3-year clinical outcomes of everolimus-eluting stents: Results of a XIENCE V/PROMUS post-marketing surveillance study. Cardiovasc. Interv. Ther. 2018, 33, 313–320. [Google Scholar] [CrossRef]
- Gupta, T.; Weinreich, M.; Greenberg, M.; Colombo, A.; Latib, A. Rotational Atherectomy: A Contemporary Appraisal. Interv. Cardiol. 2019, 14, 182–189. [Google Scholar] [CrossRef]
- Dill, T.; Dietz, U.; Hamm, C.W.; Küchler, R.; Rupprecht, H.J.; Haude, M.; Cyran, J.; Ozbek, C.; Kuck, K.H.; Berger, J.; et al. A randomized comparison of balloon angioplasty versus rotational atherectomy in complex coronary lesions (COBRA study). Eur. Heart J. 2000, 21, 1759–1766. [Google Scholar] [CrossRef]
- Reifart, N.; Vandormael, M.; Krajcar, M.; Göhring, S.; Preusler, W.; Schwarz, F.; Störger, H.; Hofmann, M.; Klöpper, J.; Müller, S.; et al. Randomized comparison of angioplasty of complex coronary lesions at a single center. Excimer Laser, Rotational Atherectomy, and Balloon Angioplasty Comparison (ERBAC) Study. Circulation 1997, 96, 91–98. [Google Scholar] [CrossRef]
- Moussa, I.; Di Mario, C.; Moses, J.; Reimers, B.; Di Francesco, L.; Martini, G.; Tobis, J.; Colombo, A. Coronary stenting after rotational atherectomy in calcified and complex lesions. Angiographic and clinical follow-up results. Circulation 1997, 96, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Lhermusier, T.; Minha, S.; Waksman, R. Rational use of rotational atherectomy in calcified lesions in the drug-eluting stent era: Review of the evidence and current practice. Cardiovasc. Revasc. Med. 2015, 16, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Liistro, F.; Porto, I.; Angioli, P.; Grotti, S.; Ducci, K.; Falsini, G.; Bolognese, L. Elutax paclitaxel-eluting balloon followed by bare-metal stent compared with Xience V drug-eluting stent in the treatment of de novo coronary stenosis: A randomized trial. Am. Heart J. 2013, 166, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Tamura, H.; Miyauchi, K.; Dohi, T.; Tsuboi, S.; Ogita, M.; Kasai, T.; Okai, I.; Katoh, Y.; Miyazaki, T.; Naito, R.; et al. Comparison of Clinical and Angiographic Outcomes after Bare Metal Stents and Drug-Eluting Stents Following Rotational Atherectomy. Int. Heart J. 2016, 57, 150–157. [Google Scholar] [CrossRef] [Green Version]
- Hachinohe, D.; Kashima, Y.; Kanno, D.; Kobayashi, K.; Sugie, T.; Kaneko, U.; Tadano, Y.; Watanabe, T.; Shitan, H.; Fujita, T. Rotational atherectomy and new-generation drug-eluting stent implantation. Catheter. Cardiovasc. Interv. 2018, 91, 1026–1034. [Google Scholar] [CrossRef]
- Abdel-Wahab, M.; Baev, R.; Dieker, P.; Kassner, G.; Khattab, A.A.; Toelg, R.; Sulimov, D.; Geist, V.; Richardt, G. Long-term clinical outcome of rotational atherectomy followed by drug-eluting stent implantation in complex calcified coronary lesions. Catheter. Cardiovasc. Interv. 2013, 81, 285–291. [Google Scholar] [CrossRef]
- Grundy, S.M. Metabolic syndrome pandemic. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Song, F.; Wang, X.; Wang, L.; Wang, D.; Yin, X.; Cao, S.; Gong, Y.; Yue, W.; Yan, F.; et al. Prevalence of metabolic syndrome among middle-aged and elderly adults in China: Current status and temporal trends. Ann. Med. 2018, 50, 345–353. [Google Scholar] [CrossRef]
- Chen, Q.; Zhang, Y.; Ding, D.; Li, D.; Xia, M.; Li, X.; Yang, Y.; Li, Q.; Hu, G.; Ling, W. Metabolic syndrome and its individual components with mortality among patients with coronary heart disease. Int. J. Cardiol. 2016, 224, 8–14. [Google Scholar] [CrossRef]
- Cavallari, I.; Cannon, C.P.; Braunwald, E.; Goodrich, E.L.; Im, K.; Lukas, M.A.; O’Donoghue, M.L. Metabolic syndrome and the risk of adverse cardiovascular events after an acute coronary syndrome. Eur. J. Prev. Cardiol. 2018, 25, 830–838. [Google Scholar] [CrossRef]
- Lovic, M.B.; Djordjevic, D.B.; Tasic, I.S.; Nedeljkovic, I.P. Impact of metabolic syndrome on clinical severity and long-term prognosis in patients with myocardial infarction with ST-segment elevation. Hellenic. J. Cardiol. 2018, 59, 226–231. [Google Scholar] [CrossRef]
- Echahidi, N.; Pibarot, P.; Després, J.P.; Daigle, J.M.; Mohty, D.; Voisine, P.; Baillot, R.; Mathieu, P. Metabolic syndrome increases operative mortality in patients undergoing coronary artery bypass grafting surgery. J Am Coll Cardiol 2007, 50, 843–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almalla, M.; Schröder, J.; Deserno, V.; Vogt, F.; Koos, R.; Koch, K.C.; Marx, N.; Hoffmann, R. Long-term clinical outcome of sirolimus-eluting stent implantation in metabolic syndrome and diabetes. J. Invasive Cardiol. 2010, 22, 317–321. [Google Scholar] [PubMed]
- Won, K.B.; Kim, B.K.; Chang, H.J.; Shin, D.H.; Kim, J.S.; Ko, Y.G.; Choi, D.; Ha, J.W.; Hong, M.K.; Jang, Y. Metabolic syndrome does not impact long-term survival in patients with acute myocardial infarction after successful percutaneous coronary intervention with drug-eluting stents. Catheter. Cardiovasc. Interv. 2014, 83, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhai, Y.; Zhao, J.; He, H.; Li, Y.; Liu, Y.; Feng, A.; Li, L.; Huang, T.; Xu, A.; et al. Impact of Metabolic Syndrome and It’s Components on Prognosis in Patients With Cardiovascular Diseases: A Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 704145. [Google Scholar] [CrossRef]
- Kasai, T.; Miyauchi, K.; Kurata, T.; Okazaki, S.; Kajimoto, K.; Kubota, N.; Daida, H. Impact of metabolic syndrome among patients with and without diabetes mellitus on long-term outcomes after percutaneous coronary intervention. Hypertens Res. 2008, 31, 235–241. [Google Scholar] [CrossRef]
- Lovic, M.B.; Savic, L.; Matic, D.; Djordjevic, D.; Nedeljkovic, I.; Tasic, I. Predictive value of metabolic syndrome definitions in patients with myocardial infarction with ST segment elevation—Are they all the same? Acta Cardiol. 2018, 73, 574–582. [Google Scholar] [CrossRef]
- Deo, S.V.; Sundaram, V.; Wilson, B.; Sahadevan, J.; Madan Mohan, S.K.; Rubelowsky, J.; Elgudin, Y.; Cmolik, B. Adverse events after coronary artery bypass grafting in patients with preoperative metabolic syndrome: A 10-year follow-up of the Veterans Affairs Database. J. Thorac. Cardiovasc. Surg. 2022, 163, 2096–2103.e3. [Google Scholar] [CrossRef]
- Xu, D.; Guo, Y.; Wang, H.; Gu, B.; Liu, G.; Zhou, C.; Wu, X.; Wang, J.; Cao, K. The angiographic and clinical outcomes after coronary stenting in patients with metabolic syndrome. Atherosclerosis 2012, 221, 416–421. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, C.; Zhou, P.; Li, J.; Chen, R.; Wang, Y.; Zhao, X.; Zhao, H.; Song, L.; Yan, H. Prevalence and impact of metabolic syndrome in patients with multivessel coronary artery disease and acute coronary syndrome. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2693–2699. [Google Scholar] [CrossRef]
- Patsa, C.; Toutouzas, K.; Tsiamis, E.; Tsioufis, C.; Spanos, A.; Karanasos, A.; Michelongona, A.; Tousoulis, D.; Stefanadis, C. Impact of metabolic syndrome on clinical outcomes after new generation drug-eluting stent implantation: The ‘obesity paradox’ phenomenon is still apparent. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Hachinohe, D.; Nie, Z.; Kashima, Y.; Luo, J.; Haraguchi, T.; Shitan, H.; Watanabe, T.; Tadano, Y.; Kaneko, U.; et al. Comparison of Drug-Eluting Stent and Plain Old Balloon Angioplasty After Rotational Atherectomy in Severe Calcified and Large Coronary. Int. Heart J. 2021, 62, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Bouisset, F.; Barbato, E.; Reczuch, K.; Dobrzycki, S.; Meyer-Gessner, M.; Bressollette, E.; Cayla, G.; Lhermusier, T.; Zajdel, W.; Palazuelos Molinero, J.; et al. Clinical outcomes of PCI with rotational atherectomy: The European multicentre Euro4C registry. EuroIntervention 2020, 16, e305–e312. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Chen, Y.; Yang, H.; Yao, K.; Ge, J. Outcomes of rotational atherectomy for severely calcified coronary lesions: A single center 5-year experience. Catheter. Cardiovasc. Interv. 2021, 98, E254–E261. [Google Scholar] [CrossRef]
- Dong, H.; Hachinohe, D.; Nie, Z.; Kashima, Y.; Li, G.; Haraguchi, T.; Shitan, H.; Watanabe, T.; Tadano, Y.; Kaneko, U.; et al. Predictors of clinical outcome after rotational atherectomy-facilitated percutaneous coronary intervention in hemodialysis patients. Ann. Palliat. Med. 2021, 10, 11308–11321. [Google Scholar] [CrossRef]
- Lu, Y.H.; Lu, J.M.; Wang, S.Y.; Li, C.L.; Liu, L.S.; Zheng, R.P.; Tian, H.; Wang, X.L.; Yang, L.J.; Zhang, Y.Q.; et al. Comparison of the diagnostic criteria of metabolic syndrome by International Diabetes Federation and that by Chinese Medical Association Diabetes Branch. Zhonghua Yi Xue Za Zhi 2006, 86, 386–389. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MS (n = 173) | No MS (n = 225) | p | |
|---|---|---|---|
| Age (years) * | 65.65 ± 8.664 | 65.27 ± 8.314 | 0.772 |
| Male, n (%) | 119 (68.79%) | 149 (66.22%) | 0.333 |
| BMI (kg/m2) * | 26.33 ± 1.75 | 24.59 ± 1.966 | <0.001 |
| DM, n (%) | 119 (68.79%) | 39 (17.33%) | <0.001 |
| Hypertension, n (%) | 154 (89.01%) | 137 (60.89%) | <0.001 |
| TG (mmol/L) * | 2.292 ± 2.070 | 1.605 ± 1.042 | <0.001 |
| LDL-C (mmol /L) * | 1.085 ± 0.297 | 1.206 ± 0.315 | <0.001 |
| HDL-C (mmol /L) * | 2.99 ± 0.942 | 2.46 ± 0.729 | <0.001 |
| Current Smoking, n (%) | 101 (58.38%) | 153 (57.78%) | 0.493 |
| Family history of CAD, n (%) | 22 (12.72%) | 30 (13.33%) | 0.490 |
| Prior MI, n (%) | 23 (13.29%) | 26 (11.56%) | 0.346 |
| Stroke | 33 (19.08%) | 26 (11.56%) | 0.026 |
| Chronic Kidney failure, n (%) | 46 (26.59%) | 36 (16.00%) | 0.007 |
| Prior PCI | 34 (19.65%) | 37 (16.44%) | 0.242 |
| Previous CABG, n (%) | 4 (2.31%) | 5 (2.22%) | 0.604 |
| LVEF < 50% | 7 (4.05%) | 9 (4.00%) | 0.588 |
| Medication, n (%) | |||
| Aspirin | 171 (98.84) | 222 (98.67%) | 0.622 |
| ACE inhibitors | 144 (83.23%) | 128 (56.89%) | <0.001 |
| β-blockers | 139 (80.35%) | 173 (76.89%) | 0.240 |
| Statins | 170 (98.27%) | 222 (98.67%) | 0.278 |
| Nitrates | 106 (61.27%) | 154 (68.44%) | 0.083 |
| Hypoglycemic drug | 109 (63.01%) | 40 (17.78%) | <0.001 |
| MS (n = 173) | Non-MS (n = 225) | p-Value | |
|---|---|---|---|
| MACE | 78 (45.09%) | 38 (16.89%) | <0.001 |
| All-cause death | 19 (10.98%) | 15 (6.67%) | 0.090 |
| MI | 12 (6.94%) | 10 (4.44%) | 0.195 |
| TVR | 51 (29.48%) | 17 (7.56%) | <0.001 |
| HR | 95% CI | p-Value | |
|---|---|---|---|
| MACE | 1.775 | 1.117–2.822 | 0.015 |
| All-cause death | 1.557 | 0.478–5.069 | 0.462 |
| MI | 0.810 | 0.168–4.075 | 0.798 |
| TVR | 2.658 | 1.390–5.080 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, B.; Xiao, C.; Wang, Z.; Jia, D.; Yang, S.; Jia, S.; Zhai, G.; Han, H.; Xu, X.; Shi, D.; et al. Relationship between Metabolic Syndrome and Clinical Outcome in Patients Treated with Drug-Eluting Stenting after Rotational Atherectomy for Complex Calcified Coronary Lesions. J. Clin. Med. 2022, 11, 4192. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144192
Hu B, Xiao C, Wang Z, Jia D, Yang S, Jia S, Zhai G, Han H, Xu X, Shi D, et al. Relationship between Metabolic Syndrome and Clinical Outcome in Patients Treated with Drug-Eluting Stenting after Rotational Atherectomy for Complex Calcified Coronary Lesions. Journal of Clinical Medicine. 2022; 11(14):4192. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144192
Chicago/Turabian StyleHu, Bin, Changbo Xiao, Zhijian Wang, Dean Jia, Shiwei Yang, Shuo Jia, Guangyao Zhai, Hongya Han, Xiaohan Xu, Dongmei Shi, and et al. 2022. "Relationship between Metabolic Syndrome and Clinical Outcome in Patients Treated with Drug-Eluting Stenting after Rotational Atherectomy for Complex Calcified Coronary Lesions" Journal of Clinical Medicine 11, no. 14: 4192. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11144192