
A Prognostic Merit of Statins in Patients with Chronic Hemodialysis after Percutaneous Coronary Intervention—A 10-Year Follow-Up Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Follow-Up Duration
2.1.1. Participants
2.1.2. Follow-Up
2.1.3. Endpoints
2.2. Statistical Analysis
3. Results
3.1. Baseline Demographics and Procedural Characteristics
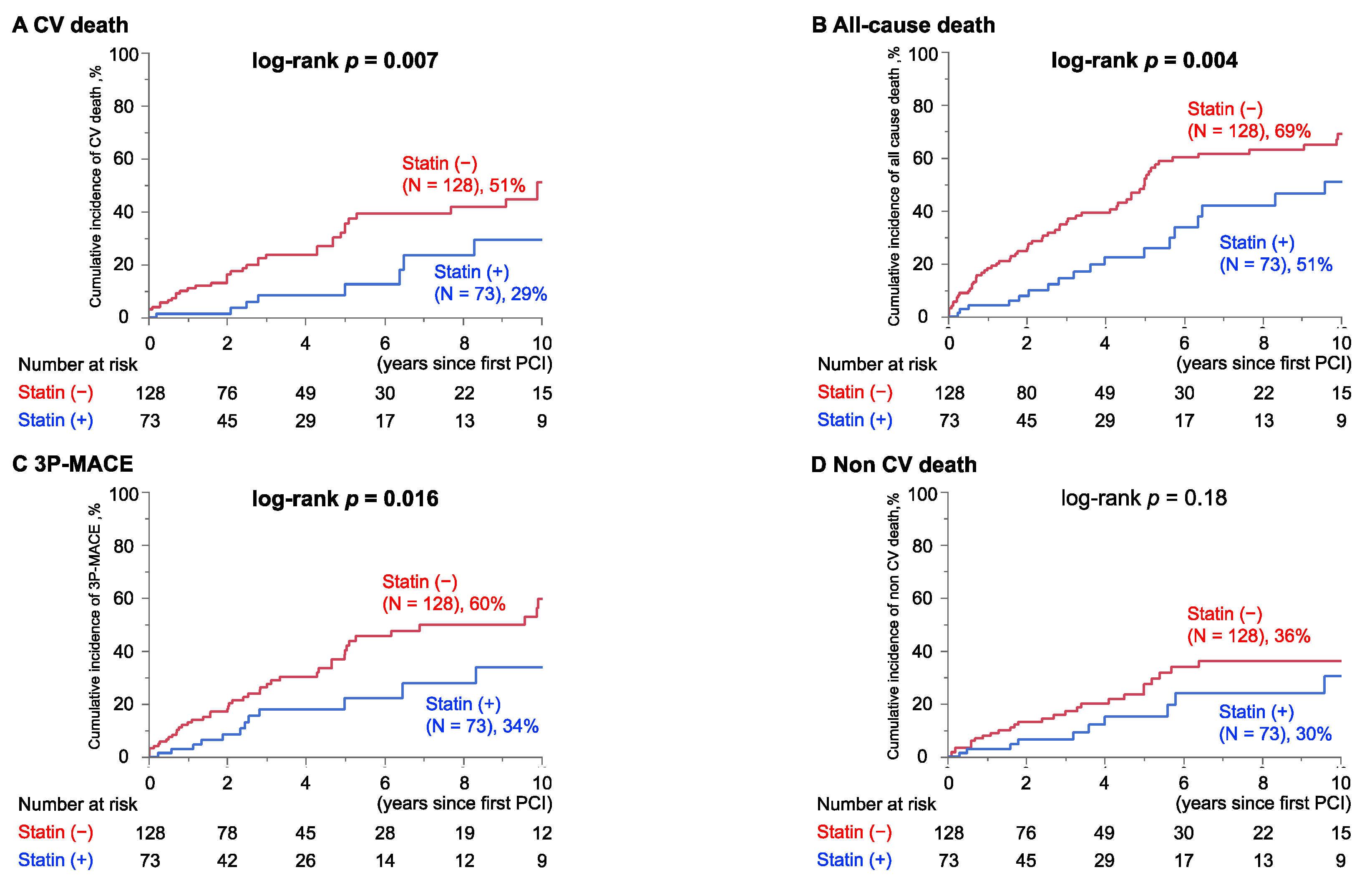
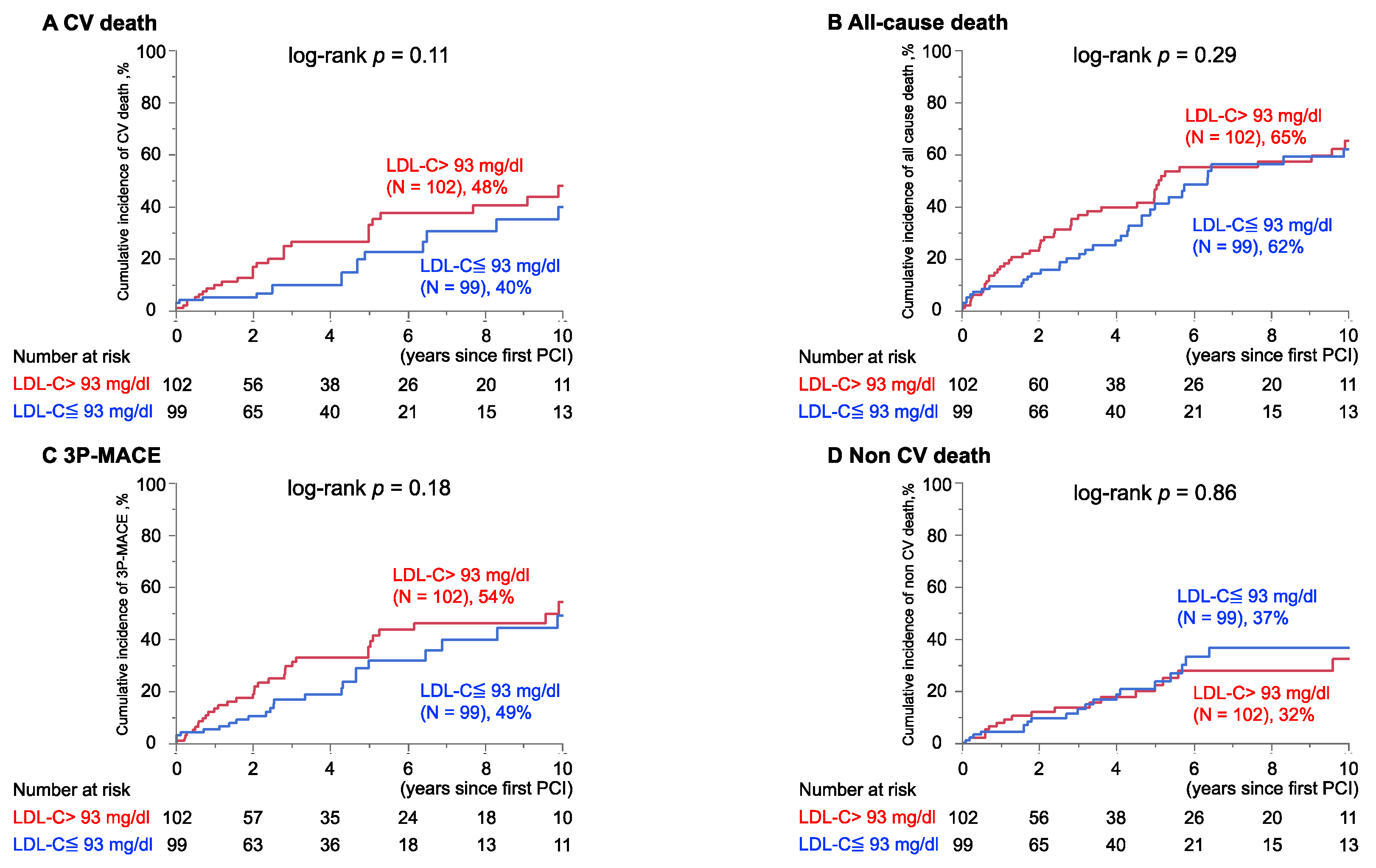
3.2. Reduced Rates of Adverse Events Following PCI in Patients Receiving Statins, While There Was No Difference in Groups Divided by Preprocedural LDL-C Level
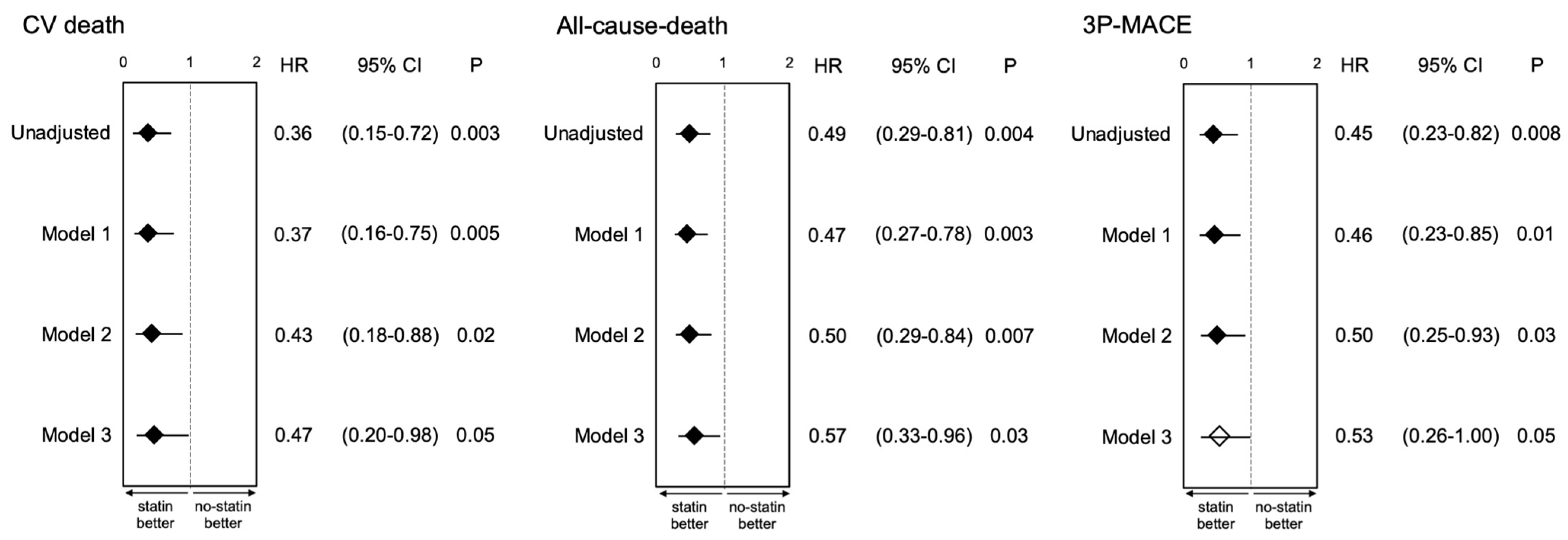
3.3. Adjusted Prognostic Impact of Statin Use for Outcomes Following PCI in Patients with Maintenance Hemodialysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Saran, R.; Robinson, B.; Abbott, K.C.; Bragg-Gresham, J.; Chen, X.; Gipson, D.; Gu, H.; Hirth, R.A.; Hutton, D.; Jin, Y.; et al. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2020, 75, A6–A7. [Google Scholar] [CrossRef]
- Kramer, A.; Boenink, R.; Noordzij, M.; Bosdriesz, J.R.; Stel, V.S.; Beltran, P.; Ruiz, J.C.; Seyahi, N.; Comas Farnes, J.; Stendahl, M.; et al. The ERA-EDTA Registry Annual Report 2017: A summary. Clin. Kidney J. 2020, 13, 693–709. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Stirnadel-Farrant, H.A.; Karaboyas, A.; Cizman, B.; Bieber, B.A.; Kler, L.; Jones, D.; Cobitz, A.R.; Robinson, B.M. Cardiovascular Event Rates among Hemodialysis Patients Across Geographical Regions-A Snapshot From The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. Rep. 2019, 4, 864–872. [Google Scholar] [CrossRef] [Green Version]
- Joki, N.; Hase, H.; Nakamura, R.; Yamaguchi, T. Onset of coronary artery disease prior to initiation of haemodialysis in patients with end-stage renal disease. Nephrol. Dial. Transplant. 1997, 12, 718–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otsuka, Y.; Ishiwata, S.; Inada, T.; Kanno, H.; Kyo, E.; Hayashi, Y.; Fujita, H.; Michishita, I. Comparison of haemodialysis patients and non-haemodialysis patients with respect to clinical characteristics and 3-year clinical outcomes after sirolimus-eluting stent implantation: Insights from the Japan multi-centre post-marketing surveillance registry. Eur. Heart J. 2011, 32, 829–837. [Google Scholar] [CrossRef] [Green Version]
- Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of LDL-lowering therapy among men and women: Meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet 2015, 385, 1397–1405. [Google Scholar] [CrossRef]
- Wanner, C.; Krane, V.; März, W.; Olschewski, M.; Mann, J.F.; Ruf, G.; Ritz, E. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N. Engl. J. Med. 2005, 353, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Fellström, B.C.; Jardine, A.G.; Schmieder, R.E.; Holdaas, H.; Bannister, K.; Beutler, J. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N. Engl. J. Med. 2009, 360, 1395–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo-controlled trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Tonelli, M. KDIGO Clinical Practice Guideline for Lipid Management in CKD: Summary of recommendation statements and clinical approach to the patient. Kidney Int. 2014, 85, 1303–1309. [Google Scholar] [CrossRef] [Green Version]
- Hick, K.A.; Mahaffey, K.W.; Mehran, R.; Nissen, S.E.; Wiviott, S.D.; Dunn, B.; Solomon, S.D.; Marler, J.R.; Teerlink, J.R.; Farb, A.; et al. 2017 Cardiovascular and Stroke Endpoint Definitions for Clinical Trials. Circulation 2018, 137, 961–972. [Google Scholar] [CrossRef]
- Eknoyan, G.; Beck, G.J.; Cheung, A.K.; Daugirdas, J.T.; Greene, T.; Kusek, J.W.; Dwyer, J.T. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N. Engl. J. Med. 2002, 347, 2010–2019. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Jardine, A.G.; Schneider, M.P.; Holdaas, H.; Holme, I.; Fellstroem, B.C.; Zannad, F.; Schmieder, R.E.; AURORA Study Group. Determinants of cardiovascular risk in haemodialysis patients: Post hoc analyses of the AURORA study. Am. J. Nephrol. 2013, 37, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Nitta, K.; Goto, S.; Masakane, I.; Hanafusa, N.; Taniguchi, M.; Hasegawa, T.; Nakai, S.; Wada, A.; Hamano, T.; Hoshino, J.; et al. Annual dialysis data report for 2018, JSDT Renal Data Registry: Survey methods, facility data, incidence, prevalence, and mortality. Ren. Replace. Ther. 2020, 6, 41. [Google Scholar] [CrossRef]
- Hanafusa, N.; Nakai, S.; Iseki, K.; Tsubakihara, Y. Japanese society for dialysis therapy renal data registry-a window through which we can view the details of Japanese dialysis population. Kidney Int. Suppl. 2015, 5, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Foster, B.J.; Mitsnefes, M.M.; Dahhou, M.; Zhang, X.; Laskin, B.L. Changes in Excess Mortality from End Stage Renal Disease in the United States from 1995 to 2013. Clin. J. Am. Soc. Nephrol. 2018, 13, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R. Blood pressure and mortality among hemodialysis patients. Hypertension 2010, 55, 762–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricks, J.; Molnar, M.Z.; Kovesdy, C.P.; Shah, A.; Nissenson, A.R.; Williams, M.; Kalantar-Zadeh, K. Glycemic control and cardiovascular mortality in hemodialysis patients with diabetes: A 6-year cohort study. Diabetes 2012, 61, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Collins, R. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, S.C.; Craig, J.C.; Navaneethan, S.D.; Tonelli, M.; Pellegrini, F.; Strippoli, G.F. Benefits and harms of statin therapy for persons with chronic kidney disease: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 263–275. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Wanner, C. Lipid management in chronic kidney disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2013 clinical practice guideline. Ann. Intern. Med. 2014, 160, 182–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyauchi, K.; Kimura, T.; Shimokawa, H.; Daida, H.; Iimuro, S.; Iwata, H.; Ozaki, Y.; Sakuma, I.; Nakagawa, Y.; Hibi, K.; et al. Rationale and Design of Randomized Evaluation of Aggressive or Moderate Lipid Lowering Therapy with Pitavastatin in Coronary Artery Disease (REAL-CAD) Trial. Int. Heart J. 2018, 59, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.G.; Oliver, M.F.; Ezekowitz, M.D.; Ganz, P.; Waters, D.; Kane, J.P.; Olsson, A.G. Rationale and design of the Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering (MIRACL) study that evaluates atorvastatin in unstable angina pectoris and in non–Q-wave acute myocardial infarction. Am. J. Cardiol. 1998, 81, 578–581. [Google Scholar] [CrossRef]
- De Vriese, A.S. Should Statins Be Banned from Dialysis? J. Am. Soc. Nephrol. 2017, 28, 1675–1676. [Google Scholar] [CrossRef]
- Puri, R.; Nicholls, S.J.; Shao, M.; Kataoka, Y.; Uno, K.; Kapadia, S.R.; Tuzcu, E.M.; Nissen, S.E. Impact of statins on serial coronary calcification during atheroma progression and regression. J. Am. Coll. Cardiol. 2015, 65, 1273–1282. [Google Scholar] [CrossRef]
- Streja, E.; Gosmanova, E.O.; Molnar, M.Z.; Soohoo, M.; Moradi, H.; Potukuchi, P.K.; Kalantar-Zadeh, K.; Kovesdy, C.P. Association of Continuation of Statin Therapy Initiated Before Transition to Chronic Dialysis Therapy With Mortality After Dialysis Initiation. JAMA Netw. Open 2018, 1, e182311. [Google Scholar] [CrossRef] [Green Version]
- Soohoo, M.; Moradi, H.; Obi, Y.; Rhee, C.M.; Gosmanova, E.O.; Molnar, M.Z.; Kashyap, M.L.; Gillen, D.L.; Kovesdy, C.P.; Kalantar-Zadeh, K.; et al. Statin Therapy Before Transition to End-Stage Renal Disease With Posttransition Outcomes. J. Am. Heart Assoc. 2019, 8, e011869. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.M.; Lin, M.S.; Chang, C.H.; Cheng, H.W.; Chang, S.T.; Wang, P.C.; Chang, H.Y.; Lin, Y.S. Moderate to high intensity statin in dialysis patients after acute myocardial infarction: A national cohort study in Asia. Atherosclerosis 2017, 267, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Jeong, H.Y.; Yang, D.H.; Kim, J.; Lee, S.Y. Beneficial effect of statins in patients receiving chronic hemodialysis following percutaneous coronary intervention: A nationwide retrospective cohort study. Sci. Rep. 2018, 8, 9692. [Google Scholar] [CrossRef] [PubMed]
- Herzog, C.A.; Ma, J.Z.; Collins, A.J. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N. Engl. J. Med. 1998, 339, 799–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shroff, G.R.; Solid, C.A.; Herzog, C.A. Long-term survival and repeat coronary revascularization in dialysis patients after surgical and percutaneous coronary revascularization with drug-eluting and bare metal stents in the United States. Circulation 2013, 127, 1861–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, T.I.; Montez-Rath, M.E.; Tsai, T.T.; Hlatky, M.A.; Winkelmayer, W.C. Drug-Eluting Versus Bare-Metal Stents During PCI in Patients With End-Stage Renal Disease on Dialysis. J. Am. Coll. Cardiol. 2016, 67, 1459–1469. [Google Scholar] [CrossRef]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., 3rd; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Beddhu, S.; Pappas, L.M.; Ramkumar, N.; Samore, M.H. Malnutrition and atherosclerosis in dialysis patients. J. Am. Soc. Nephrol. 2004, 15, 733–742. [Google Scholar] [CrossRef]
- Qureshi, A.R.; Alvestrand, A.; Divino-Filho, J.C.; Gutierrez, A.; Heimbürger, O.; Lindholm, B.; Bergström, J. Inflammation, malnutrition, and cardiac disease as predictors of mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2002, 13, S28–S36. [Google Scholar] [CrossRef] [PubMed]
- den Elzen, W.P.; van Manen, J.G.; Boeschoten, E.W.; Krediet, R.T.; Dekker, F.W. The effect of single and repeatedly high concentrations of C-reactive protein on cardiovascular and non-cardiovascular mortality in patients starting with dialysis. Nephrol. Dial. Transplant. 2006, 21, 1588–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 201) | Statin (n = 73) | Non-Statin (n = 128) | p-Value | |
|---|---|---|---|---|
| BMI 1, kg/m2 | 22.4 ± 3.9 | 22.6 ± 4.3 | 22.3 ± 3.6 | 0.67 |
| Age, years | 66.0 ± 10.3 | 65.2 ± 11.9 | 66.6 ± 9.3 | 0.35 |
| Male, n (%) | 168 (83.6) | 56 (76.7) | 112 (87.5) | 0.047 |
| Hypertension, n (%) | 174 (86.6) | 60 (82.2) | 114 (89.1) | 0.17 |
| Dyslipidemia, n (%) | 156 (77.6) | 73 (100) | 83 (64.8) | <0.001 |
| Diabetic nephropathy, n (%) | 123 (61.2) | 44 (60.3) | 79 (61.7) | 0.84 |
| Duration of hemodialysis (years) | 5.2 (1.6–10.0) | 4.0 (1.2–8.9) | 5.4 (1.9–10.9) | 0.20 |
| History of smoking, n (%) | 118 (58.7) | 39 (53.4) | 79 (61.7) | 0.25 |
| Family history, n (%) | 46 (22.9) | 15 (20.6) | 31 (24.2) | 0.55 |
| Atrial fibrillation, n (%) | 26 (12.9) | 8 (11.0) | 18 (14.1) | 0.53 |
| Prior PCI 2, n (%) | 39 (19.5) | 14 (19.2) | 25 (19.7) | 0.93 |
| Prior myocardial infarction, n (%) | 44 (21.9) | 17 (23.3) | 27 (21.1) | 0.72 |
| Prior CABG 3, n (%) | 38 (18.9) | 12 (16.4) | 26 (20.3) | 0.50 |
| Peripheral arterial disease, n (%) | 55 (27.4) | 21 (28.8) | 34 (26.6) | 0.74 |
| Prior cerebrovascular disease, n (%) | 34 (16.9) | 11 (15.1) | 23 (18.0) | 0.60 |
| ACS 4, n (%) | 36 (17.9) | 12 (16.4) | 24 (18.8) | 0.68 |
| Number of vessels | 2.1 ± 0.8 | 2.0 ± 0.8 | 2.1 ± 0.8 | 0.49 |
| RCA 5, n (%) | 74 (36.8) | 27 (37.0) | 47 (36.7) | 0.97 |
| LAD 6, n (%) | 80 (39.8) | 28 (38.4) | 52 (40.6) | 0.75 |
| LCX 7, n (%) | 38 (18.9) | 15 (20.6) | 23 (18.0) | 0.65 |
| LMT 8, n (%) | 7 (3.5) | 2 (2.7) | 5 (3.9) | 1.00 |
| SVG 9, n (%) | 2 (1.0) | 1 (1.4) | 1 (0.8) | 1.00 |
| Stent diameter, mm | 3.0 ± 0.4 | 2.9 ± 0.4 | 3.0 ± 0.4 | 0.15 |
| Total stent length, mm | 23 (15–32) | 24 (15–33) | 20 (15–32) | 0.25 |
| Medications | ||||
| Beta blocker, n (%) | 96 (47.8) | 39 (53.4) | 57 (44.5) | 0.22 |
| CCB 10, n (%) | 105 (52.2) | 34 (46.6) | 71 (55.5) | 0.22 |
| ACEI/ARB 11, n (%) | 106 (52.7) | 33 (45.2) | 73 (57.0) | 0.11 |
| Statin type | <0.001 | |||
| Low-intensity statin, n (%) | 51 (25.4) | 51 (69.9) | 0 (0) | |
| Moderate-intensity statin, n (%) | 22 (11.0) | 22 (30.1) | 0 (0) | |
| High-intensity statin, n (%) | 0 (0) | 0 (0) | 0 (0) | |
| Labolatory findings | ||||
| TC 12, mg/dL | 163.3 ± 35.5 | 158.9 ± 34.7 | 165.8 ± 35.8 | 0.18 |
| LDL-C 13, mg/dL | 96.9 ± 30.3 | 89.6 ± 27.3 | 101.0 ± 31.3 | 0.01 |
| HDL-C 14, mg/dL | 42.6 ± 14.0 | 44.3 ± 13.4 | 41.6 ± 14.2 | 0.18 |
| TG 15, mg/dL | 106.0 (79.0–146.0) | 107.0 (82.5–154.0) | 105.5 (78.0–142.5) | 0.68 |
| Non-FBG 16, mg/dL | 110.3 ± 41.1 | 104.5 ± 27.5 | 113.6 ± 46.8 | 0.13 |
| Hemoglobin, g/dL | 10.6 ± 1.5 | 10.9 ± 1.5 | 10.5 ± 1.4 | 0.07 |
| HbA1c 17, % | 6.1 ± 1.1 | 6.1 ± 1.0 | 6.1 ±1.2 | 0.87 |
| Ca, mg/dL | 9.0 ± 0.9 | 9.0 ± 1.0 | 9.1 ± 0.8 | 0.83 |
| P, mg/dL | 5.2 ± 1.4 | 5.0 ± 1.4 | 5.3 ± 1.4 | 0.28 |
| hs-CRP 18, mg/L | 3.0 (1.0–12.1) | 2.1 (0.9–10.5) | 3.6 (1.2–12.3) | 0.13 |
| Albumin, mg/dL | 3.5 ± 0.5 | 3.6 ± 0.4 | 3.5 ± 0.5 | 0.18 |
| eGFR 19, mL/min/1.73 m2 | 6.0 ± 2.1 | 6.0 ± 2.1 | 6.0 ± 2.2 | 0.97 |
| Overall (n = 201) | Statin (n = 73) | Non-Statin (n = 128) | p-Value | |
|---|---|---|---|---|
| All-cause death, n (/1000 person-years) | 86 (107) | 19 (64.7) | 67 (131) | <0.001 |
| Cardiovascular death, n (/1000 person-years) | 47 (58.3) | 8 (27.2) | 39 (76.2) | 0.002 |
| Non-cardiovascular death, n (/1000 person-years) | 39 (48.4) | 11 (37.4) | 28 (54.7) | 0.24 |
| 3P-MACE 1, n (/1000 person-years) | 58 (77.0) | 12 (43.7) | 46 (96.1) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Funamizu, T.; Iwata, H.; Chikata, Y.; Doi, S.; Endo, H.; Wada, H.; Naito, R.; Ogita, M.; Kato, Y.; Okai, I.; et al. A Prognostic Merit of Statins in Patients with Chronic Hemodialysis after Percutaneous Coronary Intervention—A 10-Year Follow-Up Study. J. Clin. Med. 2022, 11, 390. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020390
Funamizu T, Iwata H, Chikata Y, Doi S, Endo H, Wada H, Naito R, Ogita M, Kato Y, Okai I, et al. A Prognostic Merit of Statins in Patients with Chronic Hemodialysis after Percutaneous Coronary Intervention—A 10-Year Follow-Up Study. Journal of Clinical Medicine. 2022; 11(2):390. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020390
Chicago/Turabian StyleFunamizu, Takehiro, Hiroshi Iwata, Yuichi Chikata, Shinichiro Doi, Hirohisa Endo, Hideki Wada, Ryo Naito, Manabu Ogita, Yoshiteru Kato, Iwao Okai, and et al. 2022. "A Prognostic Merit of Statins in Patients with Chronic Hemodialysis after Percutaneous Coronary Intervention—A 10-Year Follow-Up Study" Journal of Clinical Medicine 11, no. 2: 390. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020390