
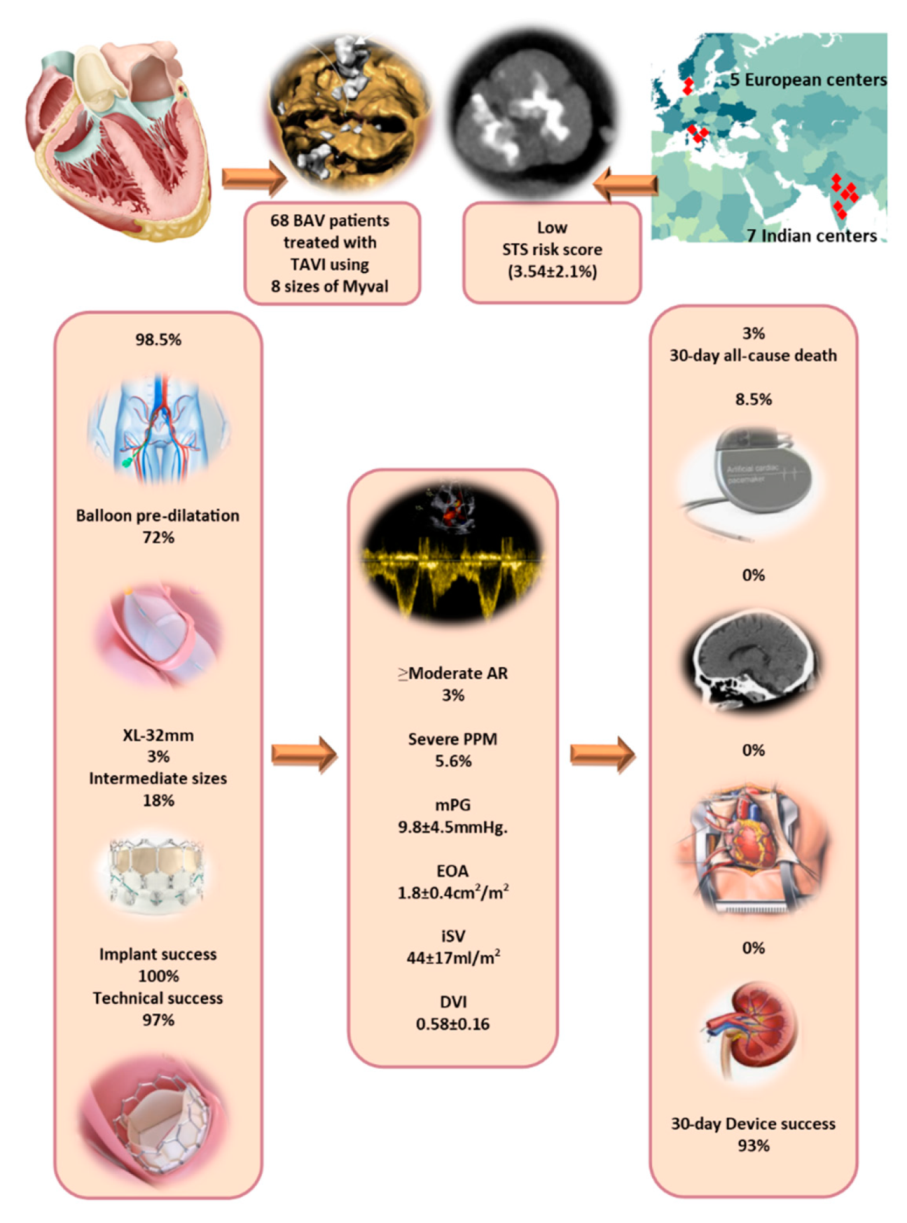
Safety and Efficacy of Myval Implantation in Patients with Severe Bicuspid Aortic Valve Stenosis—A Multicenter Real-World Experience

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
- 1.
- Endpoints and definitions
- 2.
- Statistical analysis
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Procedural Characteristics
3.3. Clinical Outcomes
3.4. Echocardiographic Outcome
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masri, A.; Svensson, L.G.; Griffin, B.P.; Desai, M.Y. Contemporary natural history of bicuspid aortic valve disease: A systematic review. Heart 2017, 103, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.C.; Ko, J.M. Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation 2005, 111, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Vincent, F.; Ternacle, J.; Denimal, T.; Shen, M.; Redfors, B.; Delhaye, C.; Simonato, M.; Debry, N.; Verdier, B.; Shahim, B.; et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation 2021, 143, 1043–1061. [Google Scholar] [CrossRef]
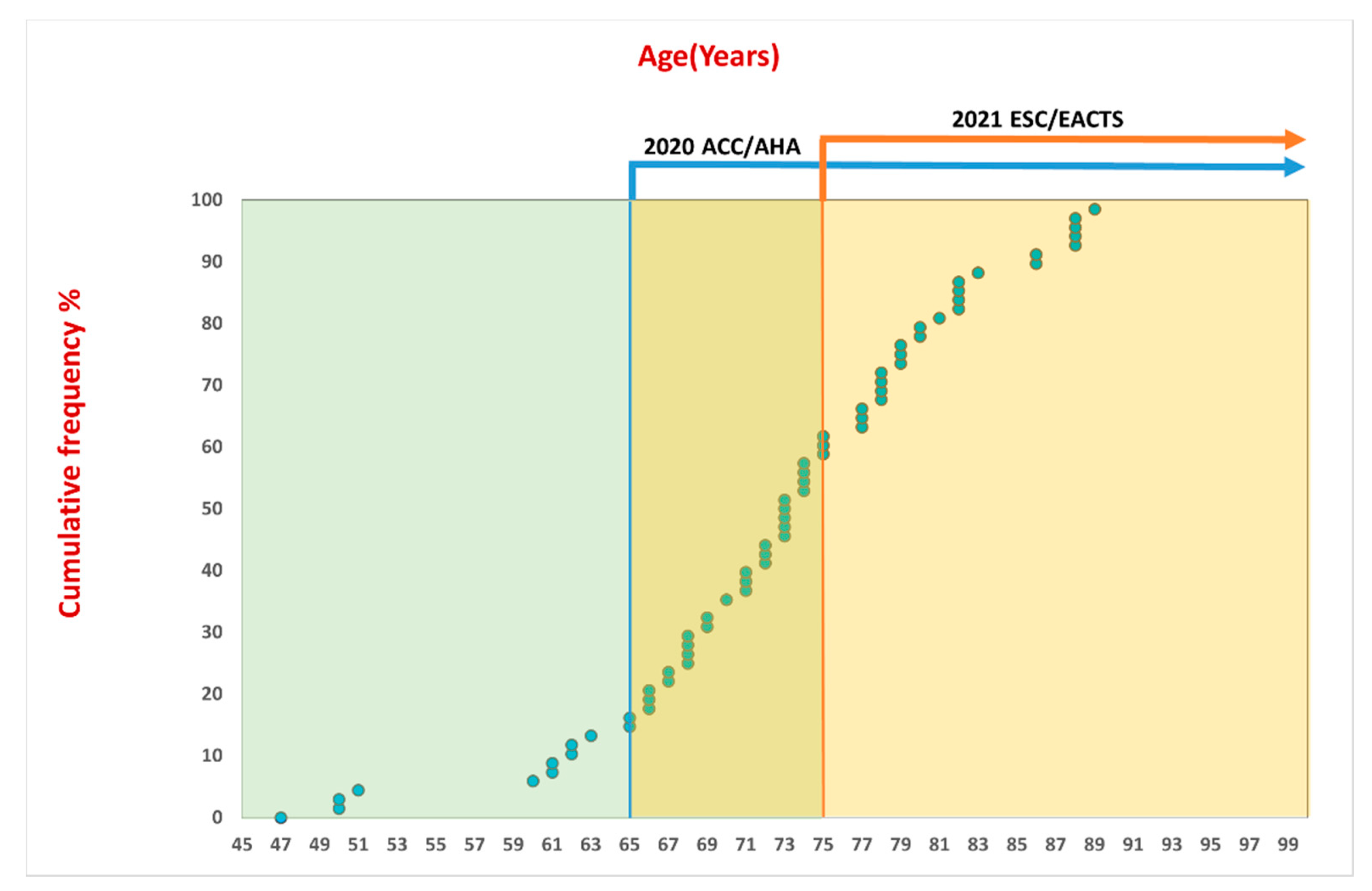
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, ehab395. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2021, 77, e25–e197. [Google Scholar] [CrossRef] [PubMed]
- Michelena, H.I.; Della Corte, A.; Evangelista, A.; Maleszewski, J.J.; Edwards, W.D.; Roman, M.J.; Devereux, R.B.; Fernandez, B.; Asch, F.M.; Barker, A.J.; et al. International Consensus Statement on Nomenclature and Classification of the Congenital Bicuspid Aortic Valve and Its Aortopathy, for Clinical, Surgical, Interventional and Research Purposes. Ann. Thorac. Surg. 2021, 112, e203–e235. [Google Scholar] [CrossRef] [PubMed]
- Sievers, H.H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Michelena, H.I.; Della Corte, A.; Evangelista, A.; Maleszewski, J.J.; Edwards, W.D.; Roman, M.J.; Devereux, R.B.; Fernandez, B.; Asch, F.M.; Barker, A.J.; et al. International consensus statement on nomenclature and classification of the congenital bicuspid aortic valve and its aortopathy, for clinical, surgical, interventional and research purposes. Eur. J. Cardio-Thorac. Surg. 2021, 60, 448–476. [Google Scholar] [CrossRef]
- Kawashima, H.; Serruys, P.W.; Mylotte, D.; Rosseel, L.; Amat-Santos, I.J.; Rao, R.S.; Onuma, Y.; Wijns, W.; Abdel-Wahab, M.; Baumbach, A.; et al. Operator preference and determinants of size selection when additional intermediate-size aortic transcatheter heart valves are made available. Int. J. Cardiol. 2021, 338, 168–173. [Google Scholar] [CrossRef]
- Garcia-Gomez, M.; Delgado-Arana, J.R.; Halim, J.; De Marco, F.; Trani, C.; Martin, P.; Won-Keun, K.; Montorfano, M.; den Heijer, P.; Bedogni, F.; et al. Next-generation balloon-expandable Myval transcatheter heart valve in low-risk aortic stenosis patients. Catheter. Cardiovasc. Interv. 2021. [Google Scholar] [CrossRef]
- Delgado-Arana, J.R.; Gordillo-Monge, M.X.; Halim, J.; De Marco, F.; Trani, C.; Martin, P.; Infusino, F.; Ancona, M.; den Heijer, P.; Bedogni, F.; et al. Early clinical and haemodynamic matched comparison of balloon-expandable valves. Heart 2021. [Google Scholar] [CrossRef]
- Sharma, S.K.; Rao, R.S.; Chandra, P.; Goel, P.K.; Bharadwaj, P.; Joseph, G.; Jose, J.; Mahajan, A.U.; Mehrotra, S.; Sengottovelu, G.; et al. First-in-human evaluation of a novel balloon-expandable transcatheter heart valve in patients with severe symptomatic native aortic stenosis: The MyVal-1 study. EuroIntervention 2020, 16, 421–429. [Google Scholar] [CrossRef]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef] [Green Version]
- Varc-3 Writing, C.; Genereux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve Academic Research Consortium 3: Updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document (VARC-2). Eur. J. Cardio-Thorac. Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef]
- Lancellotti, P.; Pibarot, P.; Chambers, J.; Edvardsen, T.; Delgado, V.; Dulgheru, R.; Pepi, M.; Cosyns, B.; Dweck, M.R.; Garbi, M.; et al. Recommendations for the imaging assessment of prosthetic heart valves: A report from the European Association of Cardiovascular Imaging endorsed by the Chinese Society of Echocardiography, the Inter-American Society of Echocardiography, and the Brazilian Department of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 589–590. [Google Scholar] [CrossRef] [Green Version]
- Zamorano, J.L.; Badano, L.P.; Bruce, C.; Chan, K.L.; Goncalves, A.; Hahn, R.T.; Keane, M.G.; La Canna, G.; Monaghan, M.J.; Nihoyannopoulos, P.; et al. EAE/ASE recommendations for the use of echocardiography in new transcatheter interventions for valvular heart disease. Eur. Heart J. 2011, 32, 2189–2214. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Asch, F.M.; Bruce, C.; Gillam, L.D.; Grayburn, P.A.; Hahn, R.T.; Inglessis, I.; Islam, A.M.; Lerakis, S.; Little, S.H.; et al. Guidelines for the Evaluation of Valvular Regurgitation After Percutaneous Valve Repair or Replacement: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2019, 32, 431–475. [Google Scholar] [CrossRef]
- Kawashima, H.; Wang, R.; Mylotte, D.; Jagielak, D.; De Marco, F.; Ielasi, A.; Onuma, Y.; den Heijer, P.; Terkelsen, C.J.; Wijns, W.; et al. Quantitative Angiographic Assessment of Aortic Regurgitation after Transcatheter Aortic Valve Implantation among Three Balloon-Expandable Valves. Glob. Heart 2021, 16, 20. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Newby, D.E. Transcatheter Valve Replacement for Bicuspid Aortic Stenosis. JAMA 2021, 326, 1009–1010. [Google Scholar] [CrossRef] [PubMed]
- Gorla, R.; Casenghi, M.; Finotello, A.; De Marco, F.; Morganti, S.; Regazzoli, D.; Bianchi, G.; Acerbi, E.; Popolo Rubbio, A.; Brambilla, N.; et al. Outcome of transcatheter aortic valve replacement in bicuspid aortic valve stenosis with new-generation devices. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 20–28. [Google Scholar] [CrossRef]
- Iannopollo, G.; Romano, V.; Buzzatti, N.; Ancona, M.; Ferri, L.; Russo, F.; Bellini, B.; Granada, J.F.; Chieffo, A.; Montorfano, M. Supra-annular sizing of transcatheter aortic valve prostheses in raphe-type bicuspid aortic valve disease: The LIRA method. Int. J. Cardiol. 2020, 317, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Kim, W.K.; Dhoble, A.; Milhorini Pio, S.; Babaliaros, V.; Jilaihawi, H.; Pilgrim, T.; De Backer, O.; Bleiziffer, S.; Vincent, F.; et al. Bicuspid Aortic Valve Morphology and Outcomes After Transcatheter Aortic Valve Replacement. J. Am. Coll Cardiol. 2020, 76, 1018–1030. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Yoon, S.H.; Chakravarty, T.; Kapadia, S.R.; Krishnaswamy, A.; Shah, P.B.; Kaneko, T.; Skipper, E.R.; Rinaldi, M.; Babaliaros, V.; et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke Among Patients at Low Surgical Risk. JAMA 2021, 326, 1034–1044. [Google Scholar] [CrossRef] [PubMed]
- Ielasi, A.; Moscarella, E.; Mangieri, A.; Giannini, F.; Tchetche, D.; Kim, W.K.; Sinning, J.M.; Landes, U.; Kornowski, R.; De Backer, O.; et al. Procedural and clinical outcomes of type 0 versus type 1 bicuspid aortic valve stenosis undergoing trans-catheter valve replacement with new generation devices: Insight from the BEAT international collaborative registry. Int. J. Cardiol. 2021, 325, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Weir-McCall, J.R.; Attinger-Toller, A.; Blanke, P.; Perlman, G.Y.; Sellers, S.L.; Wood, D.; Webb, J.G.; Leipsic, J. Annular versus supra-annular sizing for transcatheter aortic valve replacement in bicuspid aortic valve disease. J. Cardiovasc. Comput. Tomogr. 2020, 14, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Petronio, A.S.; Angelillis, M.; De Backer, O.; Giannini, C.; Costa, G.; Fiorina, C.; Castriota, F.; Bedogni, F.; Laborde, J.C.; Sondergaard, L. Bicuspid aortic valve sizing for transcatheter aortic valve implantation: Development and validation of an algorithm based on multi-slice computed tomography. J. Cardiovasc. Comput. Tomogr. 2020, 14, 452–461. [Google Scholar] [CrossRef]
- Kim, W.K.; Renker, M.; Rolf, A.; Fischer-Rasokat, U.; Wiedemeyer, J.; Doss, M.; Mollmann, H.; Walther, T.; Nef, H.; Hamm, C.W.; et al. Annular versus supra-annular sizing for TAVI in bicuspid aortic valve stenosis. EuroIntervention 2019, 15, e231–e238. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | |
|---|---|
| Age (Range) | 72.6 ± 9.4 (47–80) |
| Men | 49 (72%) |
| Women | 19 (28%) |
| BSA m2 | 1.75 ± 0.24 |
| BMI kg/m2 | 26.8 ± 6.5 |
| BMI < 30 kg/cm2 | 47 (69%) |
| BMI ≥ 30 kg/cm2 | 21 (31%) |
| BAV Phenotype (Sievers’ classification) | 62 (91%) |
| Sievers’ type 0 | 12 (19%) |
| Sievers’ type 1 | 46 (74%) |
| Sievers’ type 2 | 4 (7%) |
| Clinical characteristics | |
| STS risk score% | 3.54 ± 2.1 |
| NYHA class III/IV | 46 (68%) |
| NYHA class I/II | 22 (32%) |
| Prior atrial fibrillation | 12 (18%) |
| Peripheral vascular disease | 9 (13%) |
| Characteristic | n (%) |
|---|---|
| Access site | |
| Transfemoral | 67 (98.5%) |
| Other | 1 (1.5%) |
| Local anaesthesia and moderate sedation | 68 (100%) |
| Balloon predilatation | 49 (72%) |
| Balloon postdilatation | 8 (12%) |
| Implanted Myval THV size | |
| 20 mm | 7 (10%) |
| 21.5 mm | 2 (3%) |
| 23 mm | 20 (29.4%) |
| 24.5 mm | 5 (7.4%) |
| 26 mm | 14 (20.6) |
| 27.5 mm | 5 (7.4%) |
| 29 mm | 13 (19%) |
| 32 mm | 2 (3%) |
| Python 14-F introducer sheath | 67 (98.5%) |
| Another introducer sheath (22-F) | 1 (1.5%) |
| Navigator THV delivery system | 68 (100%) |
| Outcome | n (%) |
|---|---|
| Procedural death | 0 |
| Failed delivery | 0 |
| Major vascular complications | 1 (1.5%) |
| Life-threatening bleeding | 1 (1.5%) |
| Conversion to surgery | 0 |
| Device migration or embolization | 0 |
| Aortic root injury | 0 |
| Coronary obstruction | 0 |
| Successful positioning and implantation | 68 (100%) |
| Outcome | n (%) |
|---|---|
| Transvalvular maximum velocity >3 m/s | 1 (1.5%) |
| Transvalvular mean pressure gradient ≥20 mmHg | 1 (1.5%) |
| Dimensionless velocity index <0.25 | 0 |
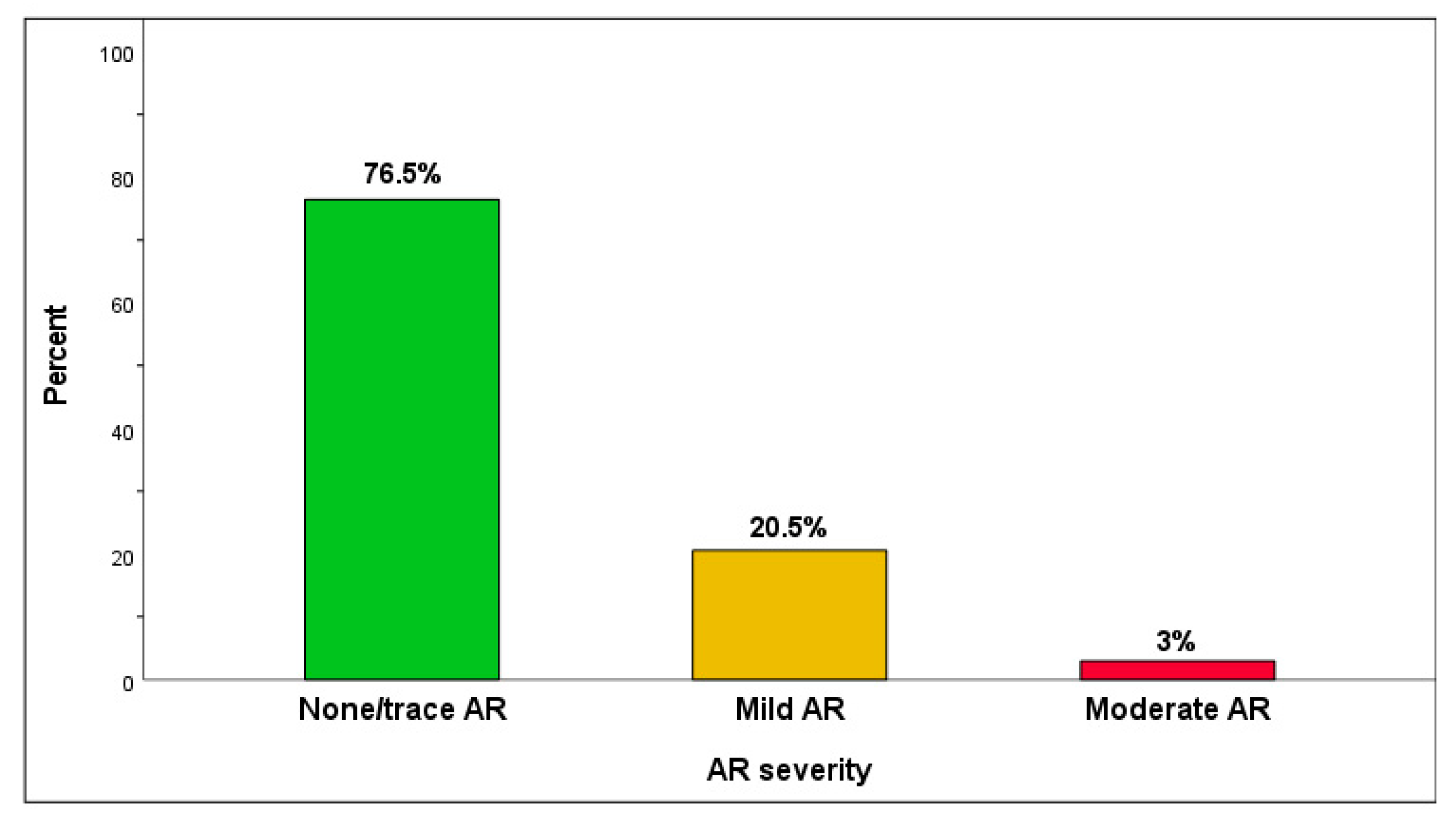
| Post-TAVI AR moderate or severe AR | 2 (3%) |
| Early safety (outcome) | |
| All-cause mortality | 2 (3%) |
| All stroke | 0 |
| Acute kidney injury (stage III-IV) | 0 |
| New permanent pacemaker implantation due to procedure related conduction abnormalities | 6 (8.5%) |
| Surgery or intervention related to the device | 0 |
| Parameter | |
|---|---|
| LV EF% | 56 ± 10 |
| Transvalvular maximum velocity m/s | 1.9 ± 0.5 |
| Transvalvular mean pressure gradient mmHg | 9.8 ± 4.5 |
| Effective orifice area cm2 | 1.8 ± 0.4 |
| Indexed effective orifice area cm2/m2 | 1.0 ± 0.27 |
| Indexed Stroke volume mL/m2 | 44 ± 17 |
| Dimensionless velocity index | 0.58 ± 0.16 |
| Post-TAVI AR | n (%) |
| None/trace | 52 (76.5%) |
| Mild | 14 (20.5%) |
| Moderate | 2 (3%) |
| Severe | 0 |
| Patient prosthesis mismatch (PPM) | n (%) |
| BMI < 30 kg/cm2 | |
| Moderate PPM (iEOA 0.66 and 0.85 cm2/m2) | 8 (14.8%) |
| Severe PPM (iEOA ≤ 0.65 cm2/m2) | 3 (5.6%) |
| BMI ≥ 30 kg/cm2 (n) | |
| Moderate PPM (iEOA 0.56 and 0.70 cm2/m2) | 2 (3.7%) |
| Severe PPM (iEOA ≤ 0.55 cm2/m2) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkoumy, A.; Jose, J.; Terkelsen, C.J.; Nissen, H.; Gunasekaran, S.; Abdelshafy, M.; Seth, A.; Elzomor, H.; Kumar, S.; Bedogni, F.; et al. Safety and Efficacy of Myval Implantation in Patients with Severe Bicuspid Aortic Valve Stenosis—A Multicenter Real-World Experience. J. Clin. Med. 2022, 11, 443. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020443
Elkoumy A, Jose J, Terkelsen CJ, Nissen H, Gunasekaran S, Abdelshafy M, Seth A, Elzomor H, Kumar S, Bedogni F, et al. Safety and Efficacy of Myval Implantation in Patients with Severe Bicuspid Aortic Valve Stenosis—A Multicenter Real-World Experience. Journal of Clinical Medicine. 2022; 11(2):443. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020443
Chicago/Turabian StyleElkoumy, Ahmed, John Jose, Christian J. Terkelsen, Henrik Nissen, Sengottuvelu Gunasekaran, Mahmoud Abdelshafy, Ashok Seth, Hesham Elzomor, Sreenivas Kumar, Francesco Bedogni, and et al. 2022. "Safety and Efficacy of Myval Implantation in Patients with Severe Bicuspid Aortic Valve Stenosis—A Multicenter Real-World Experience" Journal of Clinical Medicine 11, no. 2: 443. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020443