
Improving the Assessment Process of Family Functioning in Adult Bipolar Disorders: A PRISMA Systematic Review

 ,
,
Abstract
:1. Introduction
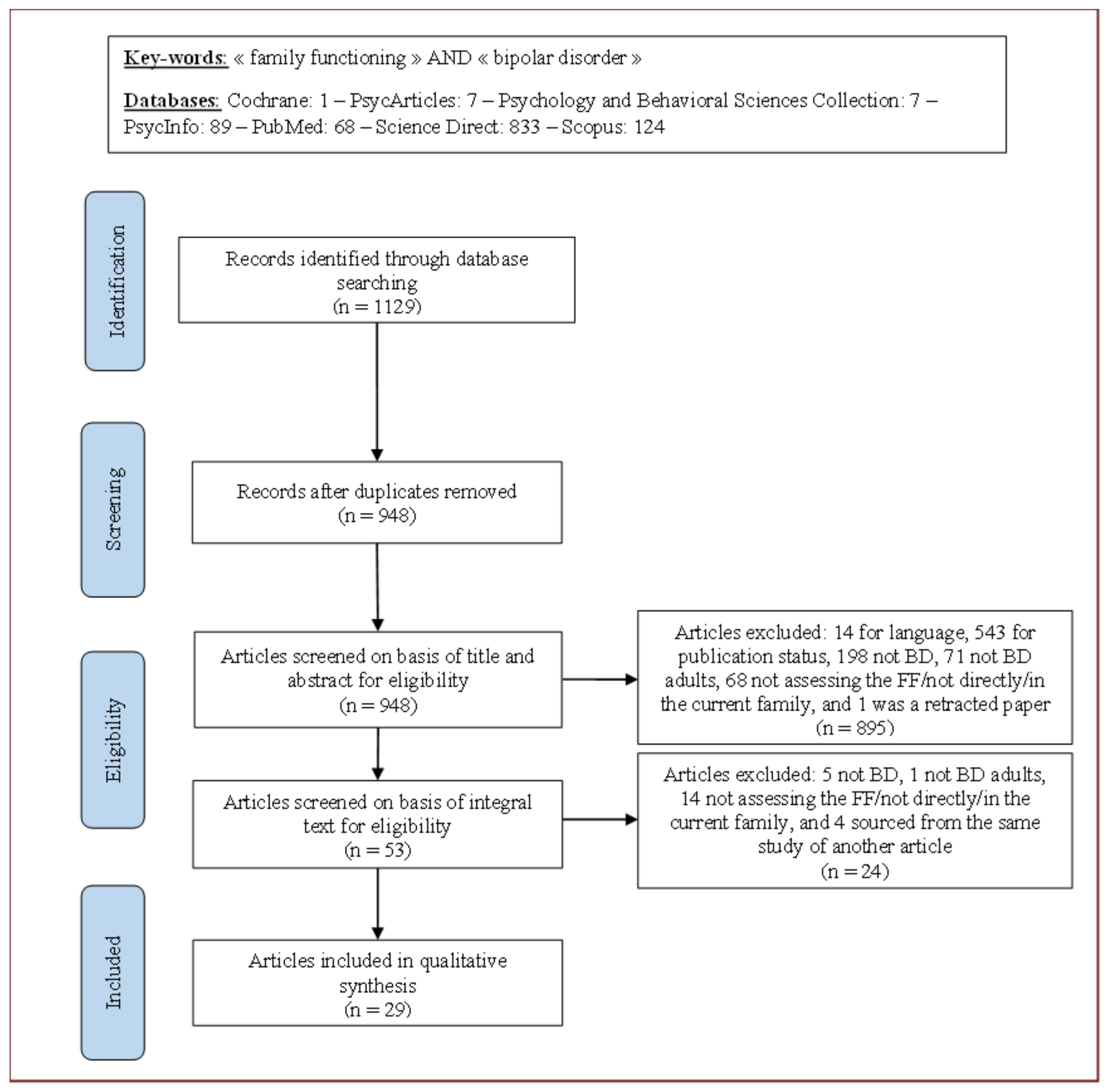
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Study Selection
2.4. Data Collection Process
3. Results
3.1. Instruments to Assess Family Functioning

{kind=link}
| Family Assessment Device (FAD) | Family Adaptability and Cohesion Evaluation Scale (FACES) | Family Environment Scale (FES) | Another Questionnaire | Semi-Structured Interview | |
|---|---|---|---|---|---|
| Dimensions of Family Functioning | Problem-Solving, Communication, Roles, Affective Responsiveness, Affective Involvement, Behavior Control, and General Functioning | Cohesion and Adaptability | Relationships, Personal Growth, and System Maintenance | No Standardization | No Standardization |
| [22] Cohen et al. (2013) | x † | ||||
| [23] Du Rocher Schudlich et al. (2008) | x † | ||||
| [24] Robinson (1996) | x † | ||||
| [25] Sheets et al. (2010) | x † | McMaster Clinical Rating Scale | |||
| [26] Uebelacker et al. (2006) | x † | McMaster Clinical Rating Scale | |||
| [27] Weinstock and Miller (2010) | x † | ||||
| [28] Friedmann et al. (1997) | x | ||||
| [29] Heru and Ryan (2004) | x | ||||
| [30] Miller et al. (1986) | x | ||||
| [31] Weinstock et al. (2006) | x | McMaster Clinical Rating Scale | |||
| [35] Koutra et al. (2016) | x ‡ | Family Questionnaire, Family Burden Scale, and General Health Questionnaire–28-item version | |||
| [36] Shalev et al. (2019) | x | Conflict Behavior Questionnaire | |||
| [37] Freed et al. (2015) | x | ||||
| [38] Reinares et al. (2016) | x | ||||
| [39] Mueser et al. (2009) | Brief Symptom Inventory, and Family Attitude Scale | Family Experiences Interview Schedule | |||
| [40] Suresky et al. (2014) | Overall Caregiver Burden Scale | ||||
| [41] Sveinbjarnardottir et al. (2013) | ICE Expressive Family Functioning Questionnaire | ||||
| [42] Fitzhenry et al. (2015) | Systemic Clinical Outcome and Routine Evaluation | ||||
| [43] Jones et al. (2017) | Confusion, Hubbub and Order Scale | ||||
| [44] Clarkin et al. (1990) | Family Attitude Inventory | ||||
| [45] Weintraub (1987) | Family Evaluation Form | ||||
| [46] Wang and Henning (2012) | x | ||||
| [48] Lau et al. (2018) | x † | ||||
| [49] MacPherson et al. (2018) | x | ||||
| [50] Berutti et al. (2016) | x | ||||
| [51] Koyama et al. (2004) | x | ||||
| [52] Müller et al. (2019) | x | ||||
| [53] Park et al. (2015) | x | ||||
| [54] Weinstock et al. (2013) | x | ||||
| TOTAL (% of use of the instrument among studies) | 51.7% | 13.8% | 6.9% | 27.6% | 20.7% |
3.2. Informant(s)
3.3. Family Characteristics
3.4. Family Functioning and Bipolar Disorders
3.5. Risk of Bias in the Assessment of Family Functioning
3.6. Risk of Bias in the Current Review
4. Discussion
4.1. Assessing Family Functioning as a Multidimensional Concept
4.2. Performing a Multi-Method Assessment of Family Functioning
4.3. Using Several Family Members as Informants
4.4. Characterizing the Family
4.5. Family Functioning as a Determinant of Remission: The Need for Assessment Guidelines
5. Conclusions: Toward Personalized Care, a Systemic Person-Oriented Approach
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Alonso, J.; Petukhova, M.; Vilagut, G.; Chatterji, S.; Heeringa, S.; Üstün, T.B.; Al-Hamzawi, A.; Viana, M.C.; Angermeyer, M.; Bromet, E.; et al. Days out of role due to common physical and mental conditions: Results from the WHO World Mental Health surveys. Mol. Psychiatry 2011, 16, 1234–1246. [Google Scholar] [CrossRef]
- Chatterton, M.L.; Ke, X.; Lewis, B.E.; Rajagopalan, K.; Lazarus, A. Impact of bipolar disorder on the family: Utilization and cost of health care resources. Pharm. Ther. 2008, 33, 14–34. [Google Scholar]
- Dore, G.; Romans, S. Impact of bipolar affective disorder on family and partners. J. Affect. Disord. 2001, 67, 147–158. [Google Scholar] [CrossRef]
- Pompili, M.; Harnic, D.; Gonda, X.; Forte, A.; Dominici, G.; Innamorati, M.; Fountoulakis, K.N.; Serafini, G.; Sher, L.; Janiri, L.; et al. Impact of living with bipolar patients: Making sense of caregivers’ burden. World J. Psychiatry 2014, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Steele, A.; Maruyama, N.; Galynker, I. Psychiatric symptoms in caregivers of patients with bipolar disorder: A review. J. Affect. Disord. 2010, 121, 10–21. [Google Scholar] [CrossRef]
- Reinares, M.; Bonnín, C.D.M.; Hidalgo-Mazzei, D.; Sanchez-Moreno, J.; Colom, F.; Vieta, E. The role of family interventions in bipolar disorder: A systematic review. Clin. Psychol. Rev. 2016, 43, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Granek, L.; Danan, D.; Bersudsky, Y.; Osher, Y. Living with bipolar disorder: The impact on patients, spouses, and their marital relationship. Bipolar Disord. 2016, 18, 192–199. [Google Scholar] [CrossRef]
- Grover, S.; Nehra, R.; Thakur, A. Bipolar affective disorder and its impact on various aspects of marital relationship. Ind. Psychiatry J. 2017, 26, 114–120. [Google Scholar] [CrossRef]
- Aneshensel, C.S.; Phelan, J.C.; Bierman, A. (Eds.) Handbook of the Sociology of Mental Health; Springer: Dordrecht, The Netherlands, 2013; ISBN 978-94-007-4275-8. [Google Scholar]
- Miklowitz, D.J. Family factors and the course of bipolar affective disorder. Arch. Gen. Psychiatry 1988, 45, 225–231. [Google Scholar] [CrossRef]
- Miklowitz, D.J.; Wisniewski, S.; Miyahara, S.; Otto, M.; Sachs, G.S. Perceived criticism from family members as a predictor of the one-year course of bipolar disorder. Psychiatry Res. 2005, 136, 101–111. [Google Scholar] [CrossRef]
- Perlick, D.A.; Rosenheck, R.A.; Clarkin, J.F.; Maciejewski, P.K.; Sirey, J.; Struening, E.; Link, B.G. Impact of family burden and affective response on clinical outcome among patients with bipolar disorder. Psychiatr. Serv. 2004, 55, 1029–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morin, E. Introduction à La Pensée Complexe; Points: Paris, France, 2014. [Google Scholar]
- Minuchin, S.; Montalvo, B.; Guerney, B.; Rosman, B.; Schumer, F. Families of the Slums; Basic Books: New York, NY, USA, 1967. [Google Scholar]
- Goodwin, G.; Haddad, P.; Ferrier, I.; Aronson, J.; Barnes, T.; Cipriani, A.; Coghill, D.R.; Fazel, S.; Geddes, J.; Grunze, H.; et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology. J. Psychopharmacol. 2016, 30, 495–553. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence Bipolar Disorder. The Assessment and Managementof Bipolar Disorder in Adults, Children and Young People in Primary and Secondary Care; Updated Edition—NICE Guideline No. 185; The British Psychological Society; The Royal College of Psychiatrists: London, UK, 2014. [Google Scholar]
- Yatham, L.N.; Kennedy, S.H.; Parikh, S.V.; Schaffer, A.; Bond, D.J.; Frey, B.N.; Sharma, V.; Goldstein, B.I.; Rej, S.; Beaulieu, S.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018, 20, 97–170. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Epstein, N.B.; Baldwin, L.M.; Bishop, D.S. The McMaster family assessment device*. J. Marital Fam. Ther. 1983, 9, 171–180. [Google Scholar] [CrossRef]
- Ryan, C.E.; Epstein, N.B.; Keitner, G.I.; Miller, I.W.; Bishop, D.S. Evaluating and Treating Families: The McMaster Approach; Taylor & Francis: New York, NY, USA, 2005. [Google Scholar]
- Cohen, A.N.; Drapalski, A.L.; Glynn, S.M.; Medoff, D.; Fang, L.J.; Dixon, L.B. Preferences for family involvement in care among consumers with serious mental illness. Psychiatr. Serv. 2013, 64, 257–263. [Google Scholar] [CrossRef]
- Schudlich, T.D.d.R.; Youngstrom, E.A.; Calabrese, J.R.; Findling, R.L. The Role of Family Functioning in Bipolar Disorder in Families. J. Abnorm. Child Psychol. 2008, 36, 849–863. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.A.R. Causal attributions about mental illness: Relationship to family functioning. Am. J. Orthopsychiatry 1996, 66, 282–295. [Google Scholar] [CrossRef]
- Sheets, E.S.; Miller, I.W. Predictors of relationship functioning for patients with bipolar disorder and their partners. J. Fam. Psychol. 2010, 24, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uebelacker, L.A.; Beevers, C.G.; Battle, C.L.; Strong, D.; Keitner, G.I.; Ryan, C.E.; Solomon, D.A.; Miller, I.W. Family functioning in bipolar I disorder. J. Fam. Psychol. 2006, 20, 701–704. [Google Scholar] [CrossRef]
- Weinstock, L.M.; Miller, I.W. Psychosocial predictors of mood symptoms 1 year after acute phase treatment of bipolar I disorder. Compr. Psychiatry 2010, 51, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Friedmann, M.S.; McDermut, W.H.; Solomon, D.A.; Ryan, C.E.; Keitner, G.I.; Miller, I.W. Family functioning and mental illness: A comparison of psychiatric and nonclinical families. Fam. Process 1997, 36, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Heru, A.M.; Ryan, C.E. Burden, reward and family functioning of caregivers for relatives with mood disorders: 1-year follow-up. J. Affect. Disord. 2004, 83, 221–225. [Google Scholar] [CrossRef]
- Miller, I.W.; Kabacoff, R.I.; Keitner, G.I.; Epstein, N.B.; Bishop, D.S. Family functioning in the families of psychiatric patients. Compr. Psychiatry 1986, 27, 302–312. [Google Scholar] [CrossRef]
- Weinstock, L.M.; Keitner, G.I.; Ryan, C.E.; Solomon, D.A.; Miller, I.W. Family functioning and mood disorders: A comparison between patients with major depressive disorder and bipolar I disorder. J. Consult. Clin. Psychol. 2006, 74, 1192–1202. [Google Scholar] [CrossRef]
- Olson, D.H.; Portner, J.; Bell, R. FACES II: Family Adaptability and Cohesion Evaluation Scales; Family Social Science; University of Minnesota: Minneapolis, MN, USA, 1982. [Google Scholar]
- Olson, D.H.; Sprenkle, D.H.; Russell, C. Circumplex model of marital and family systems: I. Cohesion and adaptability di-mensions, family types, and clinical applications. Fam. Process 1979, 18, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Olson, D.H.; Gorall, D.M.; Tiesel, J.W. FACES IV. Package; Administration Manual; Life Innovations: Minneapolis, MN, USA, 2006. [Google Scholar]
- Koutra, K.; Triliva, S.; Roumeliotaki, T.; Basta, M.; Lionis, C.; Vgontzas, A.N. Family functioning in first-episode and chronic psychosis: The role of patient’s symptom severity and psychosocial functioning. Community Ment. Health J. 2016, 52, 710–723. [Google Scholar] [CrossRef] [PubMed]
- Shalev, A.; Merranko, J.; Goldstein, T.; Miklowitz, D.J.; Axelson, D.; Goldstein, B.I.; Brent, D.; Monk, K.; Hickey, M.B.; Hafeman, D.M.; et al. A longitudinal study of family functioning in offspring of parents diagnosed with bipolar disorder. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 961–970. [Google Scholar] [CrossRef]
- Freed, R.D.; Tompson, M.C.; Wang, C.H.; Otto, M.W.; Hirshfeld-Becker, D.R.; Nierenberg, A.A.; Henin, A. Family functioning in the context of parental bipolar disorder: Associations with offspring age, sex, and psychopathology. J. Fam. Psychol. 2015, 29, 108–118. [Google Scholar] [CrossRef]
- Reinares, M.; Bonnín, C.D.M.; Hidalgo-Mazzei, D.; Colom, F.; Solé, B.; Jimenez, E.; Torrent, C.; Comes, M.; Martinez-Aran, A.; Sanchez-Moreno, J.; et al. Family functioning in bipolar disorder: Characteristics, congruity between patients and relatives, and clinical correlates. Psychiatry Res. 2016, 245, 66–73. [Google Scholar] [CrossRef]
- Mueser, K.T.; Glynn, S.M.; Cather, C.; Zarate, R.; Fox, L.; Feldman, J.; Wolfe, R.; Clark, R.E. Family intervention for co-occurring substance use and severe psychiatric disorders: Participant characteristics and correlates of initial engagement and more extended exposure in a randomized controlled trial. Addict. Behav. 2009, 34, 867–877. [Google Scholar] [CrossRef] [Green Version]
- Suresky, M.J.; Zauszniewski, J.A.; Bekhet, A.K. Factors affecting disruption in families of adults with mental illness. Perspect. Psychiatr. Care 2014, 50, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Sveinbjarnardottir, E.K.; Svavarsdottir, E.K.; Wright, L.M. What are the benefits of a short therapeutic conversation intervention with acute psychiatric patients and their families? A controlled before and after study. Int. J. Nurs. Stud. 2013, 50, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Fitzhenry, M.; Harte, E.; Carr, A.; Keenleyside, M.; O’Hanrahan, K.; White, M.D.; Hayes, J.; Cahill, P.; Noonan, H.; O’Shea, H.; et al. Child maltreatment and adult psychopathology in an Irish context. Child Abus. Negl. 2015, 45, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.H.; Jovanoska, J.; Calam, R.; Wainwright, L.D.; Vincent, H.; Asar, O.; Diggle, P.J.; Parker, R.; Long, R.; Sanders, M.; et al. Web-based integrated bipolar parenting intervention for parents with bipolar disorder: A randomised controlled pilot trial. J. Child Psychol. Psychiatry 2017, 58, 1033–1041. [Google Scholar] [CrossRef]
- Clarkin, J.F.; Glick, I.D.; Haas, G.L.; Spencer, J.H.; Lewis, A.B.; Peyser, J.; DeMane, N.; Good-Ellis, M.; Harris, E.; Lestelle, V. A randomized clinical trial of inpatient family intervention V. results for affective disorders. J. Affect. Disord. 1990, 18, 17–28. [Google Scholar] [CrossRef]
- Weintraub, S. Risk factors in Schizophrenia: The stony brook high-risk project. Schizophr. Bull. 1987, 13, 439–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.Y.; Henning, M. Family involvement in Chinese immigrants with bipolar disorder in New Zealand. N. Z. Med. J. 2012, 126, 45–52. [Google Scholar]
- Wright, L.M.; Leahey, M. Nurses and Families. A Guide to Family Assessment and Intervention; F.A. Davis Company: Philadelphia, PA, USA, 2009; Volume 5. [Google Scholar]
- Lau, P.; Hawes, D.J.; Hunt, C.; Frankland, A.; Roberts, G.; Wright, A.; Costa, D.S.; Mitchell, P.B. Family environment and psychopathology in offspring of parents with bipolar disorder. J. Affect. Disord. 2018, 226, 12–20. [Google Scholar] [CrossRef]
- MacPherson, H.A.; Ruggieri, A.L.; Christensen, R.E.; Schettini, E.; Kim, K.L.; Thomas, S.A.; Dickstein, D.P. Developmental evaluation of family functioning deficits in youths and young adults with childhood-onset bipolar disorder. J. Affect. Disord. 2018, 235, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Berutti, M.; Dias, R.D.S.; Pereira, V.A.; Lafer, B.; Nery, F.G. Association between history of suicide attempts and family functioning in bipolar disorder. J. Affect. Disord. 2016, 192, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Koyama, A.; Akiyama, T.; Miyake, Y.; Kurita, H. Family functioning perceived by patients and their family members in three Diagnostic and Statistical Manual-IV diagnostic groups. Psychiatry Clin. Neurosci. 2004, 58, 495–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, A.D.; Gjøde, I.C.T.; Eigil, M.S.; Busck, H.; Bonne, M.; Nordentoft, M.; Thorup, A.A.E. VIA Family—A family-based early intervention versus treatment as usual for familial high-risk children: A study protocol for a randomized clinical trial. Trials 2019, 20, 1–17. [Google Scholar] [CrossRef]
- Park, M.-H.; Chang, K.D.; Hallmayer, J.; Howe, M.E.; Kim, E.; Hong, S.C.; Singh, M.K. Preliminary study of anxiety symptoms, family dysfunction, and the brain-derived neurotrophic factor (BDNF) Val66Met genotype in offspring of parents with bipolar disorder. J. Psychiatr. Res. 2015, 61, 81–88. [Google Scholar] [CrossRef]
- Weinstock, L.M.; Wenze, S.J.; Munroe, C.; Miller, I.W. Concordance Between Patient and Family Reports of Family Functioning in Bipolar I Disorder and Major Depressive Disorder. J. Nerv. Ment. Dis. 2013, 201, 377–383. [Google Scholar] [CrossRef] [Green Version]
- Paulhus, D. Measurement and control of response bias. In Measures of Personality and Social Psychological Attitudes; Robinson, J., Shaver, P.R., Wrightsman, Eds.; Academic Press: New York, NY, USA, 1991; Volume 1, pp. 17–59. [Google Scholar]
- Schmier, J.K.; Halpern, M.T. Patient recall and recall bias of health state and health status. Expert Rev. Pharm. Outcomes Res. 2004, 4, 159–163. [Google Scholar] [CrossRef]
- Irwing, P.; Booth, T.; Hughes, D.J. (Eds.) The Wiley Handbook of Psychometric Testing: A Multidisciplinary Reference on Survey, Scale and Test Development; Wiley-Blackwell: Chichester, UK, 2018; Volume 1. [Google Scholar]
- Merikangas, K.R.; Akiskal, H.S.; Angst, J.; Greenberg, P.E.; Hirschfeld, R.M.A.; Petukhova, M.; Kessler, R.C. Lifetime and 12-month prevalence of bipolar spectrum disorder in the national comorbidity survey replication. Arch. Gen. Psychiatry 2007, 64, 543–552. [Google Scholar] [CrossRef]
- Merikangas, K.R.; Jin, R.; He, J.-P.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and Correlates of Bipolar Spectrum Disorder in the World Mental Health Survey Initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef]
- Kupfer, D.J.; Frank, E.; Ritchey, F.C. Staging bipolar disorder: What data and what models are needed? Lancet Psychiatry 2015, 2, 564–570. [Google Scholar] [CrossRef]
- Barron, E.; Sharma, A.; Le Couteur, J.; Rushton, S.; Close, A.; Kelly, T.; Grunze, H.; Ferrier, I.N.; Le Couteur, A. Family environment of bipolar families: A UK study. J. Affect. Disord. 2014, 152–154, 522–525. [Google Scholar] [CrossRef]
- Smilkstein, G. The family APGAR: A proposal for a family function test and its use by physicians. J. Fam. Pract. 1978, 6, 1231–1239. [Google Scholar]
- Pardo, E.; Fierro, M.; Ibáñez, M. Prevalencia y factores asociados a la no adherencia en el tratamiento farmacológico de mantenimiento en adultos con trastorno afectivo bipolar. Rev. Colomb. Psiquiat. 2011, 40, 85–98. [Google Scholar]
- Doornbos, M.M. The strengths of families coping with serious mental illness. Arch. Psychiatr. Nurs. 1996, 10, 214–220. [Google Scholar] [CrossRef]
- Fernandes, B.S.; Williams, L.M.; Steiner, J.; Leboyer, M.; Carvalho, A.F.; Berk, M. The new field of ‘precision psychiatry’. BMC Med. 2017, 15, 80. [Google Scholar] [CrossRef] [PubMed]
- Ozomaro, U.; Wahlestedt, C.; Nemeroff, C.B. Personalized medicine in psychiatry: Problems and promises. BMC Med. 2013, 11, 132–135. [Google Scholar] [CrossRef] [Green Version]
- Bergman, L.R.; Wångby, M. The person-oriented approach: A short theoretical and practical guide. Estonian J. Educ. 2014, 2, 29–49. [Google Scholar] [CrossRef] [Green Version]
- Howard, M.C.; Hoffman, M.E. Variable-centered, person-centered, and person-specific approaches. Organ. Res. Methods 2018, 21, 846–876. [Google Scholar] [CrossRef]
- Laursen, B.P.; Hoff, E. Person-centered and variable-centered approaches to longitudinal data. Merrill-Palmer Q. 2006, 52, 377–389. [Google Scholar] [CrossRef]
- Tversky, A.; Kahneman, D. Judgment under uncertainty: Heuristics and biases. Science 1974, 185, 1124–1131. [Google Scholar] [CrossRef]
- Wolfson, A.M.; Doctor, J.N.; Burns, S.P. Clinician judgments of functional outcomes: How bias and perceived accuracy affect rating. Arch. Phys. Med. Rehabil. 2000, 81, 1567–1574. [Google Scholar] [CrossRef]
- Averous, P.; Charbonnier, E.; Lagouanelle-Simeoni, M.C.; Prosperi, A.; Dany, L. Illness perceptions and adherence in bipolar disorder: An exploratory study. Compr. Psychiatry 2018, 80, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Lobban, F.; ERP Group; Solis-Trapala, I.; Tyler, E.; Chandler, C.; Morriss, R.K. The role of beliefs about mood swings in determining outcome in bipolar disorder. Cogn. Ther. Res. 2013, 37, 51–60. [Google Scholar] [CrossRef]
- Tohen, M.; Frank, E.; Bowden, C.L.; Colom, F.; Ghaemi, S.N.; Yatham, L.N.; Malhi, G.S.; Calabrese, J.R.; Nolen, W.A.; Vieta, E.; et al. The International Society for Bipolar Disorders (ISBD) Task Force report on the nomenclature of course and outcome in bipolar disorders. Bipolar Disord. 2009, 11, 453–473. [Google Scholar] [CrossRef] [PubMed]
- Watzlawick, P. (Ed.) The Invented Reality: How Do We Know What We Believe We Know? W.W. Norton & Company: New York, NY, USA, 1980. [Google Scholar]
- Kenny, D.A.; Kashy, D.A.; Cook, W.L. Dyadic Data Analysis; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Stas, L.; Kenny, D.A.; Mayer, A.; Loeys, T. Giving dyadic data analysis away: A user-friendly app for actor–partner interdependence models. Pers. Relatsh. 2018, 25, 103–119. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.; Carrington, P.J. (Eds.) The SAGE Handbook of Social Network Analysis; SAGE Publications Ltd: London, UK, 2011; ISBN 9781847873958. [Google Scholar]
- Wikle, J.S.; Hoagland, A. Adolescent interactions with family and emotions during interactions: Variation by family structure. J. Fam. Psychol. 2020, 34, 544–554. [Google Scholar] [CrossRef]
- Henry, C.; Etain, B.; Godin, O.; Dargel, A.A.; Azorin, J.-M.; Gard, S.; Bellivier, F.; Bougerol, T.; Kahn, J.-P.; Passerieux, C.; et al. Bipolar patients referred to specialized services of care: Not resistant but impaired by sub-syndromal symptoms. Results from the FACE-BD cohort. Aust. N. Z. J. Psychiatry 2015, 49, 898–905. [Google Scholar] [CrossRef]
- Judd, L.L.; Akiskal, H.S.; Schettler, P.J.; Endicott, J.; Leon, A.C.; Solomon, D.A.; Coryell, W.; Maser, J.D.; Keller, M.B. Psychosocial disability in the course of bipolar I and II disorders: A prospective, comparative, longitudinal study. Arch. Gen. Psychiatry 2005, 62, 1322–1330. [Google Scholar] [CrossRef] [Green Version]
- MacQueen, G.M.; Young, L.T.; Joffe, R.T. A review of psychosocial outcome in patients with bipolar disorder. Acta Psychiatr. Scand. 2001, 103, 163–170. [Google Scholar] [CrossRef]
- Magnusson, D. Interactionism and the person approach in developmental psychology. Eur. Child Adolesc. Psychiatry 1996, 5, 18–22. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development. Experiments by Nature and Design; Havard University Press: Cambridge, UK, 1979. [Google Scholar]
- Compagnone, P.D.; Strayer, F. A person centered analysis of health profiles during middle childhood. Eur. Rev. Appl. Psychol. 2004, 54, 179–187. [Google Scholar] [CrossRef]

| Population | Country | Socio-Demographic and Clinical Characteristics of People with BD 1 | Socio-Demographic and Clinical Characteristics of Other Family Members | Family Structure |
| Objective(s) | As reported in the main text or in the abstract | |||
| Outcome(s) | Outcomes considered to assess FF 2 | |||
| Instrument(s) | Instrument assessing FF 2 | Validation | Specified if cut-off is considered | |
| Informant(s) | Who is the informant for FF? 2 | |||
| Underlying theoretical framework | Definition of family | Is the assessment of FF 2 based on a theoretical framework? | ||
| Results | Relevant results concerning FF 2 in BD 1 specifically |
| Number of Informants | Informant Status | ||||
|---|---|---|---|---|---|
| One | Several | Person with a BD | One Family Member of the Person BD | Several Family Members of the Person with BD | |
| [22] Cohen et al. (2013) | x | x | |||
| [23] Du Rocher Schudlich et al. (2008) | x | x | x | ||
| [24] Robinson (1996) | x | x | x | ||
| [25] Sheets et al. (2010) | x | x | x | ||
| [26] Uebelacker et al. (2006) | x | x | x | ||
| [27] Weinstock and Miller (2010) | x | x | |||
| [28] Friedmann et al. (1997) | x | x | x | ||
| [29] Heru and Ryan (2004) | x | x | |||
| [30] Miller et al. (1986) | x | x | x | ||
| [31] Weinstock et al. (2006) | x | x | x | ||
| [35] Koutra et al. (2016) | x | x | |||
| [36] Shalev et al. (2019) | x | x | x | ||
| [37] Freed et al. (2015) | x | x | |||
| [38] Reinares et al. (2016) | x | x | x | ||
| [39] Mueser et al. (2009) | x | x | x | ||
| [40] Suresky et al. (2014) | x | x | |||
| [41] Sveinbjarnardottir et al. (2013) | x | x | |||
| [42] Fitzhenry et al. (2015) | x | x | |||
| [43] Jones et al. (2017) | x | x | |||
| [44] Clarkin et al. (1990) | x † | x † | x † | ||
| [45] Weintraub (1987) | x | x | x | ||
| [46] Wang and Henning (2012) | x | x | |||
| [48] Lau et al. (2018) | x | x | x | ||
| [49] MacPherson et al. (2018) | x | x | |||
| [50] Berutti et al. (2016) | x | x | x | ||
| [51] Koyama et al. (2004) | x | x | x | ||
| [52] Müller et al. (2019) | x | x | x | ||
| [53] Park et al. (2015) | x | x | x | ||
| [54] Weinstock et al. (2013) | x | x | x | ||
| TOTAL | 41.4% | 58.6% | 86.2% | 34.5% | 41.4% |
| Country | Total Sample | Persons with BD Characteristics | Family Members’ Characteristics of the Person with a BD | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | BD Type | Patient Status | BD Period | Sex (% of Females) | Age Mean (SD) | Status in Family | Sample Size | Status in Family | |||
| [22] Cohen et al. (2013) | USA | 104 | 104 | NI | Outpatient | NI | Confused | Confused | NI | Not included | |
| [23] Du Rocher Schudlich et al. (2008) | USA | 231 | 77 | NI | NI | NI | Confused | Confused | Parent | 154 | Offspring with mental illness |
| [24] Robinson (1996) | USA | NI | 7 | NI | NI | NI | Confused | Confused | Child | Confused | Parent Sibling |
| [25] Sheets et al. (2010) | USA | 112 | 56 | Type I | Inpatient Outpatient Partial | Acute Manic (82%) | 55% | 41.77 (None) | NI | 56 | Partner |
| [26] Uebelacker et al. (2006) | USA | 62 | 62 | Type I | NI | Acute | 58% | 40.6 (12.5) | NI | None | Partner (63%) Parent (21%) Adult child/another adult (16%) |
| [27] Weinstock and Miller (2010) | USA | 92 | 92 | Type I | Inpatient Outpatient Partial | Manic (75%) Depressive (20%) Mixed (5%) | 57% | 39 (11.5) | NI | Not included | |
| [28] Friedmann et al. (1997) | USA | 171 | 60 | NI | Inpatient | Acute | 77% | 38.2 (12.9) | Partner (74%) Child (26%) | 111 | Over the age of 12 |
| [29] Heru and Ryan (2004) | USA | 10 | Non included | NI | Inpatient | Any | NI | Confused | NI | 10 | Confused |
| [30] Miller et al. (1986) | USA | 30 | 15 | NI | Inpatient | Manic | Confused | Confused | Partner (80%) Child (20%) | 15 | Over the age of 12 |
| [31] Weinstock et al. (2006) | USA | NI | 69 | Type I | Inpatient Outpatient Partial | Manic | 59.4% | 38.80 (11.03) | NI | Average of 1.54 per patient | Partner (71%) Parent (21.7%) Child/other (2.9%) |
| [35] Koutra et al. (2016) | Greece | 18 | 18 | NI | Inpatient | Euthymic | Confused | Confused | NI | 18 | Confused |
| [36] Shalev et al. (2019) | USA | 737 | 256 | Type I Type II | NI | NI | NI | NI | Parent | 481 | Offspring |
| [37] Freed et al. (2015) | USA | 192 | 75 | NI | Inpatient | NI | 68% | 43.62 (6.77) | Parent | 117 | Offspring |
| [38] Reinares et al. (2016) | Spain | 164 | 82 | Type I (83%) Type II (17%) | NI | Euthymic | 51% | 34.67 (10.0) | NI | 82 | Partner (40%) Parent (54%) Adult child/Sibling (6%) |
| [39] Mueser et al. (2009) | USA | 58 | 29 | NI | NI | NI | Confused | Confused | NI | 29 | Confused |
| [40] Suresky et al. (2014) | USA | 33 | Non included | NI | NI | NI | NI | NI | NI | 33 | Woman family member |
| [41] Sveinbjarnardottir et al. (2013) | Iceland | 68 | 34 | NI | Inpatient | Acute | Confused | Confused | NI | 34 | Confused |
| [42] Fitzhenry et al. (2015) | Ireland | 18 | 18 | NI | Confused | NI | Confused | Confused | Confused | Not included | |
| [43] Jones et al. (2017) | UK | 97 | 97 | Type I (94%) Type II (6%) | NI | NI | 78% | 36.65 (None) | Parent | Not included | |
| [44] Clarkin et al. (1990) | USA | 21 | 21 | NI | Inpatient | Manic (61.9%) Depressive (33.3%) Mixed (4.8%) | 67% | 32.3 (15.4) | NI | Not included | |
| [45] Weintraub (1987) | USA | 250 | 58 | NI | Inpatient | NI | 44.83% | NI | Parent | 58 134 | Partner Child |
| [46] Wang and Henning (2012) | New Zealand | 9 | 9 | NI | NI | NI | 55.56% | 41 (None) | NI | Not included | |
| [48] Lau et al. (2018) | Australia | 149 | 59 | Type I (79.6%) Type II (20.3%) | NI | NI | NI | NI | Parent | 90 | Offspring |
| [49] MacPherson et al. (2018) | USA | 46 | 46 | Type I (60.9%) Type II (6.5%) Nos (32.6%) | NI | Euthymic (80%) | 61% | 21.16 (2.77) | NI | Not included | |
| [50] Berutti et al. (2016) | Brazil | 113 | 62 | Type I | Outpatient | Euthymic | 60.9% | 41 (None) | NI | 51 | Partner Parent |
| [51] Koyama et al. (2004) | Japan | 36 | 18 | NI | Outpatient | NI | 44.4% | 49.4 (10.5) | NI | 18 | Partner (94.4%) Parent (5.6%) |
| [52] Müller et al. (2019) | Denmark | NI | NI | NI | NI | NI | NI | NI | Parent | NI | Partner Child |
| [53] Park et al. (2015) | USA | 64 | NI | Type I Type II | NI | NI | NI | NI | Parent | 64 | Offspring |
| [54] Weinstock et al. (2013) | USA | 227 | 92 | Type I | Inpatient Outpatient Partial | Manic (75%) Depressive (20%) Mixed (5%) | 57% | 39.57 (11.30) | NI | 135 | Partner (67%) At least 1 parent (20%) At least 1 sibling (3%) At least 1 other (10%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munuera, C.; Compagnone, P.; Husky, M.M.; Lebourleux, P.; Petit, F.; M’bailara, K. Improving the Assessment Process of Family Functioning in Adult Bipolar Disorders: A PRISMA Systematic Review. J. Clin. Med. 2022, 11, 841. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030841
Munuera C, Compagnone P, Husky MM, Lebourleux P, Petit F, M’bailara K. Improving the Assessment Process of Family Functioning in Adult Bipolar Disorders: A PRISMA Systematic Review. Journal of Clinical Medicine. 2022; 11(3):841. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030841
Chicago/Turabian StyleMunuera, Caroline, Philippe Compagnone, Mathilde M. Husky, Paul Lebourleux, Fanny Petit, and Katia M’bailara. 2022. "Improving the Assessment Process of Family Functioning in Adult Bipolar Disorders: A PRISMA Systematic Review" Journal of Clinical Medicine 11, no. 3: 841. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030841