
Mycoplasma pneumoniae Pleural Effusion in Adults


Department of Internal Medicine, School of Medicine, Kyungpook National University, 680 Gukchaebosang-ro, Jung-gu, Daegu 700-842, Korea
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2022, 11(5), 1281; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051281
Submission received: 27 January 2022
/
Revised: 20 February 2022
/
Accepted: 24 February 2022
/
Published: 26 February 2022
(This article belongs to the Special Issue Advances in Mycoplasma pneumoniae Infections)
Abstract
:Parapneumonic effusions often complicate Mycoplasma pneumoniae (MP) pneumonia, contrary to the notion that they are a rare feature of MP infection. Increased research and evidence on MP parapneumonic effusions (MPPE) can help elucidate its clinical significance as one of the variable manifestations of MP infection. This article aims to summarize the existing literature about the clinical characteristics of MPPE in adults and discuss its diagnostic implications from the perspective of pleural fluid analysis. Approximately 20–25% of adult patients with MP pneumonia develop MPPE, and its frequency in children and adults seems to be similar. Although the pathogenesis of MPPE remains to be elucidated, MP-induced cell-mediated immune mechanisms might be partially associated with the development of MPPE. MPPE usually shows mononuclear leukocyte predominance with elevated adenosine deaminase (ADA) activity, similar to tuberculous pleural effusion (TPE). The degree of increase in pleural fluid ADA levels and serum inflammatory biomarkers may help differentiate between MPPE and TPE. During the acute phase, a single positive IgM and positive polymerase chain reaction results allow for a precise and reliable MP infection diagnosis. The mainstay of treatment is the selection of adequate anti-mycoplasma antibiotics with or without corticosteroid, based on the local epidemiologic data on macrolide resistance.
1. Introduction
Mycoplasma pneumoniae (MP), which was first discovered in the 1940s, causes a wide spectrum of clinical symptoms and diseases [1,2]. Pleural effusions frequently complicate MP pneumonia similar to complications in pneumonia caused by other bacterial pathogens [3,4,5,6,7,8], which is contrary to the notion that MP parapneumonic effusions (MPPE) are so rare that they receive a different diagnosis than MP infections [9]. Based on the literature from the last few decades, approximately 20–25% of patients with MP pneumonia develop parapneumonic effusion [3,4,5,6,8]. The latest reports suggest that the clinical significance of MPPE needs to be emphasized in terms of differential diagnosis with tuberculous pleural effusions (TPE) [8,10,11,12,13,14]. A better understanding of the characteristics of MPPE will contribute to the accurate diagnosis and appropriate treatment of the condition. Thus, the present review focuses on the clinical and diagnostic implications of MPPE from the perspective of pleural fluid analysis in adults.
2. Epidemiology
MP infections occur both endemically and epidemically worldwide [15] and are estimated in the range of 2–12% among adults with community-acquired pneumonia [16,17,18]. The occurrence of MPPE has been reported in 4–28% of MP pneumonia cases [3,4,5,6,7,8,19,20,21]. This variable incidence of MPPE may be influenced by the radiologic modalities used to detect pleural effusions [3]. A prospective study using serial chest X-rays, including lateral decubitus views by Fine et al. [5] reported that pleural effusions were identified in 21% of patients with MP pneumonia. They suggested not dismissing the possibility of MP infections in patients with parapneumonic effusion. Another study reported that, among 54 adult patients with MP pneumonia, pleural effusions were detected in 24% of them using computed tomography (CT), while only a half of them could be detected using posteroanterior and lateral chest X-rays [3]. Similarly, a study performed during an epidemic of MP infection revealed that 28% of patients with MP pneumonia had pleural effusions based on chest CT images [8]. The tendency of increase in the frequency of MPPE may be due to the advanced diagnostic methods for MP infection and widespread use of CT modality. The reported incidences of MPPE in children and young adults were similar [4,5,6,7,8].
3. Pathogenesis
The mechanisms by which MP, the smallest self–replicating bacteria lacking a cell wall, causes infection are complex [15,22,23,24,25]. MP can cause direct damage to the host via adhesion, membrane fusion, nutrition depletion, invasion, and toxin-like effects [25]. In addition, MP induces collateral damage to host tissues by immune responses during MP infection, which include humoral and cellular immune responses, inflammatory and antigenic damage, and immunosuppression [25]. Adhesion to the host cell is the first step in its pathogenicity mechanism [15,24]. The adhesion protein complex, which consists of the key protein P1 and several auxiliary proteins, enables P1 proteins to adhere to host cells [24,25]. Once attached, MP produces a variety of substances that cause local damage to epithelial cells and stimulates the release of inflammatory mediators from host immune cells [22,23,24,25].
Parapneumonic effusions usually occur when the pathogens enter the pleural space directly by breaching the pleural barrier through the alveolar air space [26]. Pleural mesothelial cells, the first to encounter the invading pathogens, have surface molecules including Toll-like receptors, monosialyl containing receptors, and glycoproteins to serve as receptors for bacterial determinants [26,27]. MP is likely to first interact with mesothelial cells during pleural infection, similar to the way that it adheres to host respiratory epithelial cells during lung infection [24]. Previous reports on mesothelial cell proliferation in the pleural fluid of patients with MPPE [28,29] support this speculation. Subsequently, MP may induce host innate and acquired immune responses via enhanced expression of Toll-like receptors within the pleural space [15,23,24,25].
A characteristic feature of parapneumonic effusions is generally the accumulation of neutrophils and mononuclear phagocytes, which are the most important components of the initial innate immune response during bacterial infection [30,31,32]. This finding contrasts with previous studies on adult patients with MPPE, which report that lymphocytes are usually predominant in the acute stage (Table 1) [6,8,10,11,29,33,34,35,36,37,38,39,40]. Histopathological examination also revealed chronic inflammation and accumulation of numerous lymphocytes and mononuclear cells on the pleural tissue obtained from a patient with MPPE [11]. This pleural fluid feature of MPPE is consistent with what may be expected from an intracellular pathogen, such as Mycobacterium tuberculosis (MTB), or a virus. Lymphocytic exudate of TPE develops due to the proliferation of antigen-specific T cells under the cell-mediated immune response to MTB [41]. Even though MP is primarily an extracellular pathogen, cell-mediated immune mechanisms play an important role in the development of MP infection [15,22,23]. T–lymphocyte activation and different cytokine stimulation patterns have been reported to be related to the evolution of MPPE [42,43]. It remains to be elucidated whether the different cellular predominance in a pleural fluid depends on the degree of cell-mediated immune response and reflects the disease severity or phase of MPPE.
4. Clinical Manifestations
4.1. Clinical, Radiologic, and Laboratory Features
MPPE usually occurs as an acute illness with gradual onset. The most common presenting symptoms are high fever, nonproductive coughing, and pleuritic chest pain [6,8,11,29,33,34,35,36,37,38,39]. Other common symptoms include headache, malaise, and other extra-pulmonary phenomena [6,29,33,34,35,36,37,38,39]. MPPE mainly occurs in young adults (Table 1). The effusions are generally unilateral and small, and resolve with appropriate antimicrobial therapy [10,36]; however, they can be bilateral and large, and lead to shortness of breath occasionally [37,38,44]. The presence of pleural effusion in child and adult patients with MP pneumonia suggests a more severe clinical course, including higher levels of serum inflammatory biomarkers, increased extent of pneumonic infiltration, and prolonged hospitalization when compared to those without pleural effusion [4,8].
Effusions are always associated with pulmonary infiltrates, which are usually unilateral and located in the lower lobe [34,38,39,45]. Pleural effusions are more associated with alveolar or lobar pneumonia patterns than with interstitial pneumonia patterns in adults as well as children with MP pneumonia [3,46,47]. However, radiologic findings are nonspecific and are usually indistinguishable from other bacterial pneumonia patterns.
White blood cell (WBC) count is normal or mildly elevated. Serum C-reactive protein (CRP) and lactate dehydrogenase (LDH) are more elevated in patients with pleural effusion than in those without pleural effusion [4,10]. These findings suggest highly severe systemic inflammation as seen in other bacterial parapneumonic effusions. Other laboratory features are nonspecific.
4.2. Pleural Fluid Analysis
The MPPE is usually serous colored but may be purulent or bloody as other bacterial parapneumonic effusions [11,29,33,34,35]. The effusion is virtually always an exudate. Total leukocyte counts and routine biochemistries of MPPE are not different from the other bacterial parapneumonic effusions. The most distinct characteristics of MPPE are differential WBC counts and adenosine deaminase (ADA) levels.
4.2.1. Differential WBC Counts
MPPE commonly shows mononuclear leukocyte (MN) predominance even during the acute stage, which is different from other bacterial parapneumonic effusions that exhibit polymorphonuclear leukocyte (PMN) predominance. In the data collected from reports of cases and small series providing differential leukocyte counts, MN was predominant in 68% of the cases (Table 1). Generally, the predominant cell population is determined by the cause and phase of pleural injury and the timing of thoracentesis in relation to the onset of pleural injury [45,48]. The acute response to most pleural injuries, whether infectious, immunologic, or malignant, is the attraction of neutrophils to the pleural space [49,50]. Thus, the PMN predominance usually suggests early-stage inflammation than MN predominance. However, shifting to MN predominance in MPPE seems to rapidly occur even during acute clinical illness compared to that in other common bacterial parapneumonic effusions. This phenomenon may be attributable to a particular feature of the MP pathogen mediating cellular immunity like intracellular pathogens, such as MTB, as stated in the section on pathogenesis.
4.2.2. Adenosine Deaminase Levels
Roughly one in ten bacterial uncomplicated parapneumonic effusions, one-third of complicated parapneumonic effusions, and two-thirds of empyema have pleural fluid ADA levels above 40 U/L [51]. Despite neither complicated parapneumonic effusions nor empyema, MPPE seems to have a higher frequency of elevated ADA levels compared to that in other usual bacterial parapneumonic effusions. There was no data comparing pleural fluid ADA levels between MPPEs and other bacterial parapneumonic effusions. However, data from previous studies on adult patients with MPPE often reported higher levels of pleural fluid ADA; ADA levels of 7 out of 14 patients (50%) exceeded 40 U/L (Table 1). Additionally, elevated pleural fluid ADA levels are supported by the findings that serum ADA levels were higher in MP pneumonia cases than in other typical bacterial pneumonia cases [52,53,54]. These findings in conjunction with MN predominance led to confusion among the differential diagnosis between MPPE and TPE [11,14]. However, pleural fluid ADA levels of MPPE showed modest elevation like other bacterial parapneumonic effusions with elevated ADA activity, when compared to those of TPE. In contrast, systemic inflammatory biomarkers, such as serum CRP or LDH levels of MPPE were higher due to bacterial pneumonia compared to those of TPE [10,55]. These different properties may help distinguish MPPE from TPE.
5. Diagnosis
A definitive diagnosis of MP infection is a constantly challenging issue due to the fastidious nature of the pathogen, the considerable seroprevalence, and the possibility of transient asymptomatic carriage [56,57]. However, the early and precise diagnosis of MP infection and the use of appropriate anti-mycoplasma drugs are crucial factors to prevent the development of fulminant or fatal MP pneumonia [47,58,59]. Pleural fluid provides additional information and can be used for the diagnosis of MP infections. The current best algorithm to improve the sensitivity and specificity for acute MP infection diagnosis is a combination of polymerase chain reaction (PCR) and serology tests [56,57]. Although the isolation of MP from the pleural fluid, as well as sputum in patients with MPPE, has been reported [37,39,60], MP culture is time-consuming, requires special culture media, and has a high potential for false negatives, which is why it is not available in many centers [56].
5.1. Nucleic Acid Amplification Test
PCR tests as single or multiplex assays are the diagnostic method of choice for acute MP infection [56]. MP PCR using respiratory tract samples (nasopharyngeal swab, sputum, bronchial washing, bronchoalveolar lavage fluid, and pleural fluid and tissue) is fast and sensitive. However, it lacks specificity because it cannot distinguish between true patients and asymptomatic carriers [61]. Thus, positive results should be interpreted cautiously in context with clinical findings. Positive PCR results in the pleural fluid or tissue can establish a definite diagnosis [11,62]. Given the recent evidence that pleural biopsies improved microbiological yield in pleural infection [63], pleural tissue, only when available, may be a good sample for detection of MP, particularly through PCR tests.
5.2. Serologic Test
Enzyme immunoassay (EIA) is the preferred method for the detection of the specific anti-mycoplasma antibody and has largely replaced the complement fixation and microparticle agglutination tests [56,57]. EIA test also allows for the separate detection of IgM, IgA, or IgG. The gold standard of serologic diagnosis is a four-fold or greater increase of MP specific IgG when comparing acute and convalescent sera collected with an interval of 2–4 weeks. However, the need for a convalescent serum makes it impractical for the early management of acute illness. Using a single high IgM or IgA titer to make a presumptive diagnosis is an alternate strategy, although using only acute phase serology lacks both specificity and sensitivity [1].
5.3. Combination of Tests
There is currently no test that unequivocally distinguishes MP infection from a carriage or from a previous MP infection, except for positive PCR or culture result from pleural fluid or tissue. During the acute phase, a single positive IgM in combination with a positive PCR result allows for a precise and reliable MP infection diagnosis [64,65]. The clinician should attempt to incorporate patient characteristics, especially pleural fluid characteristics while considering the limitation described above [1].
5.4. Diagnostic Approach for Discriminating between MPPE and TPE
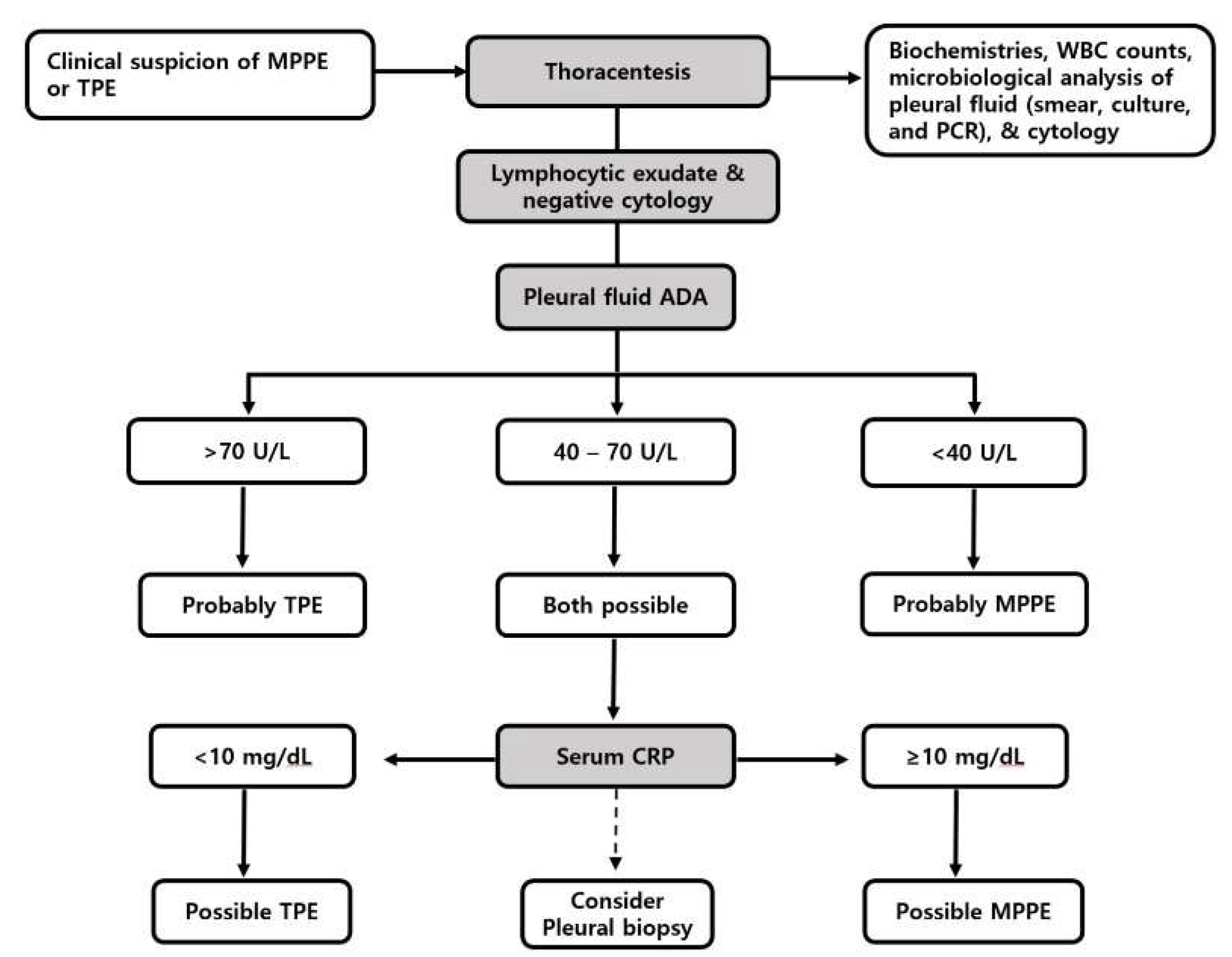
Recently, two reports of misdiagnosed MPPE and TPE were presented [11,14]. Because of the similar clinical course and characteristics of pleural effusion between MPPE and TPE, misdiagnosis is likely to occur in countries with intermediate or high prevalence of tuberculosis [11,13]. Figure 1 shows a diagnostic approach suggested for discrimination between MPPE and TPE. As with the investigation of any exudative pleural effusion, pleural fluid tests, including biochemistries, WBC counts, microbiological studies, and cytology are routinely performed [66]. In cases with an exudative pleural effusion of lymphocytic predominance without convincing evidence of etiology, routine pleural fluid ADA levels can be used as a predictive factor for TPE regardless of the prevalence of tuberculosis in the specific geographical area [66,67]. ADA levels below 40 U/L virtually rule out TPE and favor MPPE or other lymphocytic exudative pleural diseases. In contrast, pleural fluid ADA levels above 70 U/L suggest TPE rather than MPPE or others [10,68]. Alternatively, if pleural fluid ADA levels are between 40 and 70 U/L, many etiologies are possible. When the differential diagnosis is confined to MPPE and TPE, serum CRP levels exceeding 10 mg/dL that reflect more systemic inflammation usually accompanied with bacterial infection [69], are likely to favor MPPE, while those favoring TPE are usually less than 10 mg/dL [10,55]. Similarly, serum LDH levels reflect the inflammatory degree of MPPE, which is more elevated than those of TPE. Thus, the serum LDH/pleural fluid ADA ratio may be used as a parameter for distinguishing between MPPE and TPE [10,13]. In cases with an uncertain or atypical clinical picture, the final diagnosis can be established by pleural biopsy with tissue PCR and culture.
6. Management
Macrolide, tetracyclines, and respiratory fluoroquinolone are effective against MP. One of these agents is selected based on patient comorbidities, potential drug interactions, and the likelihood of macrolide resistance [70,71]. Due to the lack of a cell wall, MP is insensitive to ꞵ-lactam antibiotics. The optimal duration of therapy is not clear; however, 10–14 days or longer is generally recommended, according to clinical responses [15]. Pleural drainage can be considered in patients with worsening MPPE despite treatment with appropriate antimicrobials [36,39]. Corticosteroids with adequate antibiotics are a reasonable treatment option, especially in fulminant or refractory MP pneumonia patients that present with a hyperactive immune response [1,47,58].
The frequency of macrolide resistance has been increasing in various regions worldwide, particularly in Asia. In regions where the development of macrolide resistance is suspected based on local epidemiology research, such as most of Asia, alternative therapy (doxycycline or fluoroquinolone) should be considered in patients with severe or refractory diseases [71]. Macrolide resistance tests have been developed using a molecular method and are expected to be conducted more frequently [72].
7. Future Directions
Although there has been recent progress in the field of understanding MP infection, there remains a lack of high-quality data on MPPE. Therefore, a prospective investigation is warranted for a better understanding of this underexplored disease. In addition, further research is needed to explore how ADA, the levels of which are increased in various pleural effusions, acts differently and how we distinguish between these results.
8. Conclusions
Approximately one–fifth of adult patients with MP pneumonia develop MPPE. MPPE frequently shows MN predominance with modestly elevated ADA levels. These findings suggest a clinical implication of differential diagnosis with TPE. The degree of elevated pleural fluid ADA levels and serum inflammatory biomarkers may help differentiate between MPPE and TPE. The best current method to diagnose acute MP infection is a combination of PCR and serology. The mainstay of treatment is the selection of adequate antibiotics, such as macrolide, tetracycline, and respiratory fluoroquinolone, with or without corticosteroid, based on the local epidemiologic data for macrolide-resistance.
Author Contributions
Conceptualization, C.H.K. and J.L.; methodology, C.H.K. and J.L.; software analysis, J.L.; validation, C.H.K. and J.L.; formal analysis, J.L.; investigation, C.H.K. and J.L.; resources, C.H.K. and J.L.; data curation, C.H.K. and J.L.; writing—original draft preparation, C.H.K. and J.L.; writing—review and editing, C.H.K. and J.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- De Groot, R.C.A.; Meyer Sauteur, P.M.; Unger, W.W.J.; van Rossum, A.M.C. Things that could be Mycoplasma pneumoniae. J. Infect. 2017, 74, S95–S100. [Google Scholar] [CrossRef]
- Saraya, T. The History of Mycoplasma pneumoniae Pneumonia. Front. Microbiol. 2016, 7, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Koba, H.; Honma, S.; Sugaya, F.; Abe, S. Relationships between radiological pattern and cell-mediated immune response in Mycoplasma pneumoniae pneumonia. Eur. Respir. J. 1996, 9, 669–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Lee, E.; Song, E.S.; Lee, Y.Y. Clinical Significance of Pleural Effusion in Mycoplasma pneumoniae Pneumonia in Children. Pathogens 2021, 10, 1075. [Google Scholar] [CrossRef]
- Fine, N.L.; Smith, L.R.; Sheedy, P.F. Frequency of pleural effusions in mycoplasma and viral pneumonias. N. Engl. J. Med. 1970, 283, 790–793. [Google Scholar] [CrossRef]
- Linz, D.H.; Tolle, S.W.; Elliot, D.L. Mycoplasma pneumoniae pneumonia. Experience at a referral center. West. J. Med. 1984, 140, 895–900. [Google Scholar]
- Miyashita, N.; Sugiu, T.; Kawai, Y.; Oda, K.; Yamaguchi, T.; Ouchi, K.; Kobashi, Y.; Oka, M. Radiographic features of Myco-plasma pneumoniae pneumonia: Differential diagnosis and performance timing. BMC Med. Imaging 2009, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.I.; Shin, K.M.; Jeon, K.N.; Yoo, S.S.; Lee, J.; Lee, S.Y.; Kim, C.H.; Park, J.Y.; Jung, T.H. Clinical relevance and characteris-tics of pleural effusion in patients with Mycoplasma pneumoniae pneumonia. Scand. J. Infect. Dis. 2012, 44, 793–797. [Google Scholar] [CrossRef]
- Herbert, D.H. The roentgen features of Eaton agent pneumonia. Am. J. Roentgenol. 1966, 98, 300–304. [Google Scholar] [CrossRef]
- Kim, C.H.; Park, J.E.; Yoo, S.S.; Lee, S.Y.; Cha, S.I.; Park, J.Y.; Lee, J. Usefulness of serum lactate dehydrogenase/pleural fluid adenosine deaminase ratio for differentiating Mycoplasma pneumoniae parapneumonic effusion and tuberculous pleural effusion. J. Infect. 2017, 75, 581–583. [Google Scholar] [CrossRef]
- Wen, P.; Wei, M.; Guo, X.; Xu, Y.R. Mycoplasma pneumoniae infection mimicking tuberculous pleurisy in a young woman: A case report and literature review. J. Int. Med. Res. 2020, 48, 0300060520918701. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Hur, W.K.; Baek, H.S.; Oh, J.W.; Lee, H.B. Usefulness of Pleural Adenosine Deaminase in Children for the Differen-tiation Tuberculous Pleural Effusion from Mycoplasma pneumonia with Pleural Effusion. Pediatr. Allergy Respir. Dis. 2012, 22, 404–410. [Google Scholar] [CrossRef]
- Xu, H.; Feng, G.; Cai, S.; Liu, J.; Tang, X.; Liu, H.; Yang, H.; Li, H.; Zhao, S. Predictive Model for Discrimination of Tuberculous Pleural Effusion From Severe Mycoplasma pneumoniae Pneumonic Effusion in Children. Pediatr. Infect. Dis. J. 2019, 38, 1100–1103. [Google Scholar] [CrossRef]
- Yaguchi, D.; Ichikawa, M.; Shizu, M.; Inoue, N.; Kobayashi, D.; Imai, N.; Ito, M. Tuberculous pleurisy mimicking Mycoplasma pneumoniae infection in a previously healthy young adult: A case report. Medicine 2018, 97, e10811. [Google Scholar] [CrossRef]
- Parrott, G.L.; Kinjo, T.; Fujita, J. A Compendium for Mycoplasma pneumoniae. Front. Microbiol. 2016, 7, 513. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Self, W.H.; Wunderink, R.G.; Fakhran, S.; Balk, R.; Bramley, A.M.; Reed, C.; Grijalva, C.G.; Anderson, E.J.; Courtney, D.M.; et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. N. Engl. J. Med. 2015, 373, 415–427. [Google Scholar] [CrossRef] [Green Version]
- Bjarnason, A.; Westin, J.; Lindh, M.; Andersson, L.M.; Kristinsson, K.G.; Love, A.; Baldursson, O.; Gottfredsson, M. Incidence, Etiology, and Outcomes of Community-Acquired Pneumonia: A Population-Based Study. Open Forum Infect. Dis. 2018, 5, ofy010. [Google Scholar] [CrossRef]
- Gramegna, A.; Sotgiu, G.; Di Pasquale, M.; Radovanovic, D.; Terraneo, S.; Reyes, L.F.; Vendrell, E.; Neves, J.; Menzella, F.; Blasi, F.; et al. Atypical pathogens in hospitalized patients with community-acquired pneumonia: A worldwide perspective. BMC Infect. Dis. 2018, 18, 677. [Google Scholar] [CrossRef] [Green Version]
- Suzuyama, Y.; Iwasaki, H.; Izumikawa, K.; Hara, K. Clinical complications of Mycoplasma pneumoniae disease–other organs. Yale J. Biol. Med. 1983, 56, 487–491. [Google Scholar]
- Nagayama, Y.; Sakurai, N.; Yamamoto, K. Clinical observations of children with pleuropneumonia due to Mycoplasma pneumoniae. Pediatr. Pulmonol. 1990, 8, 182–187. [Google Scholar] [CrossRef]
- Okada, F.; Ando, Y.; Wakisaka, M.; Matsumoto, S.; Mori, H. Chlamydia pneumoniae pneumonia and Mycoplasma pneu-moniae pneumonia: Comparison of clinical findings and CT findings. J. Comput. Assist. Tomogr. 2005, 29, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Waites, K.B.; Talkington, D.F. Mycoplasma pneumoniae and its role as a human pathogen. Clin. Microbiol. Rev. 2004, 17, 697–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraya, T.; Kurai, D.; Nakagaki, K.; Sasaki, Y.; Niwa, S.; Tsukagoshi, H.; Nunokawa, H.; Ohkuma, K.; Tsujimoto, N.; Hirao, S.; et al. Novel aspects on the pathogenesis of Mycoplasma pneumoniae pneumonia and therapeutic implications. Front. Microbiol. 2014, 5, 410. [Google Scholar] [CrossRef] [PubMed]
- Waites, K.B.; Balish, M.F.; Atkinson, T.P. New insights into the pathogenesis and detection of Mycoplasma pneumoniae infec-tions. Future Microbiol. 2008, 3, 635–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.; Liu, M.; Ye, Z.; Tan, T.; Liu, X.; You, X.; Zeng, Y.; Wu, Y. Insights into the pathogenesis of Mycoplasma pneumoniae (Review). Mol. Med. Rep. 2016, 14, 4030–4036. [Google Scholar] [CrossRef] [Green Version]
- Hage, C.A.; Abdul-Mohammed, K.; Antony, V.B. Pathogenesis of pleural infection. Respirology 2004, 9, 12–15. [Google Scholar] [CrossRef]
- Ohtsuka, A.; Yamana, S.; Murakami, T. Localization of membrane-associated sialomucin on the free surface of mesothelial cells of the pleura, pericardium, and peritoneum. Histochem. Cell Biol. 1997, 107, 441–447. [Google Scholar] [CrossRef]
- Buckmaster, N.; Bellomo, R. Mycoplasma infection mimicking hypersensitivity pneumonitis. Chest 1993, 103, 1928. [Google Scholar] [CrossRef]
- Feizi, O.; Grubb, C.; Skinner, J.I.; Constandou, M.; Henderson, W.G. Unusual complications of primary atypical pneumonia due to M. pneumoniae. Br. Med. J. 1971, 4, 751. [Google Scholar] [CrossRef] [Green Version]
- Sibille, Y.; Reynolds, H.Y. Macrophages and polymorphonuclear neutrophils in lung defense and injury. Am. Rev. Respir. Dis. 1990, 141, 471–501. [Google Scholar] [CrossRef]
- Craig, A.; Mai, J.; Cai, S.; Jeyaseelan, S. Neutrophil recruitment to the lungs during bacterial pneumonia. Infect. Immun. 2009, 77, 568–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batra, H.; Antony, V.B. Pleural mesothelial cells in pleural and lung diseases. J. Thorac. Dis. 2015, 7, 964–980. [Google Scholar] [PubMed]
- Lewis, J.E.; Sheptin, C. Mycoplasmal pneumonia associated with abscess of the lung. Calif. Med. 1972, 117, 69–72. [Google Scholar]
- Solanki, D.L.; Berdoff, R.L. Severe mycoplasma pneumonia with pleural effusions in a patient with sickle cell-hemoglobin C(SC) disease. Case report and review of the literature. Am. J. Med. 1979, 66, 707–710. [Google Scholar] [CrossRef]
- Bajantri, B.; Danial, S.; Duncalf, R.; Khaja, M. Rare complicated parapneumonic effusion, Mycoplasma pneumoniae with new-onset lupus flare: Case report and literature review. Respir. Med. Case Rep. 2017, 22, 287–291. [Google Scholar] [CrossRef]
- Hassan, K.S.; Al-Khadouri, G. Mycoplasma pneumoniae Pneumonia with Worsening Pleural Effusion Despite Treatment with Appropriate Antimicrobials: Case report. Sultan Qaboos Univ. Med. J. 2018, 18, e239–e242. [Google Scholar] [CrossRef] [Green Version]
- Murray, H.W.; Masur, H.; Senterfit, L.B.; Roberts, R.B. The protean manifestations of Mycoplasma pneumoniae infection in adults. Am. J. Med. 1975, 58, 229–242. [Google Scholar] [CrossRef]
- Chester, A.; Kane, J.; Garagusi, V. Mycoplasma pneumonia with bilateral pleural effusions. Am. Rev. Respir. Dis. 1975, 112, 451–456. [Google Scholar]
- Gump, D.W.; Hawley, H.B. Severe Mycoplasma pneumoniae pneumonia. Respiration 1976, 33, 475–486. [Google Scholar] [CrossRef]
- Ding, L.; Zhao, Y.; Li, X.; Wang, R.; Li, Y.; Tang, X.; Sun, B.; He, H. Early diagnosis and appropriate respiratory support for Mycoplasma pneumoniae pneumonia associated acute respiratory distress syndrome in young and adult patients: A case series from two centers. BMC Infect. Dis. 2020, 20, 367. [Google Scholar] [CrossRef]
- Wilkinson, K.A.; Wilkinson, R.J.; Pathan, A.; Ewer, K.; Prakash, M.; Klenerman, P.; Maskell, N.; Davies, R.; Pasvol, G.; Lalvani, A. Ex vivo characterization of early secretory antigenic target 6-specific T cells at sites of active disease in pleural tuberculosis. Clin. Infect. Dis. 2005, 40, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Narita, M.; Teramoto, S.; Saikai, T.; Oashi, K.; Igarashi, T.; Abe, S. Role of interleukin-18 and T-helper type 1 cyto-kines in the development of Mycoplasma pneumoniae pneumonia in adults. Chest 2002, 121, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Narita, M.; Tanaka, H. Two distinct patterns of pleural effusions caused by Mycoplasma pneumoniae infection. Pediatr. Infect. Dis. J. 2004, 23, 1069. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.Y.; Chiang, L.M.; Chen, T.P. Mycoplasma pneumoniae infection complicated by necrotizing pneumonitis with mas-sive pleural effusion. Eur. J. Pediatr. 2006, 165, 275–277. [Google Scholar] [CrossRef]
- Sahn, S.A. State of the art. The pleura. Am. Rev. Respir. Dis. 1988, 138, 184–234. [Google Scholar] [CrossRef]
- Jayantha, U. Study on pleural effusions due to Mycoplasma pneumoniae infection. Sri Lanka J. Child Health 2009, 34, 5–6. [Google Scholar] [CrossRef] [Green Version]
- Izumikawa, K.; Izumikawa, K.; Takazono, T.; Kosai, K.; Morinaga, Y.; Nakamura, S.; Kurihara, S.; Imamura, Y.; Miyazaki, T.; Tsukamoto, M.; et al. Clinical features, risk factors and treatment of fulminant Mycoplasma pneumoniae pneumonia: A review of the Japanese literature. J. Infect. Chemother. 2014, 20, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Sahn, S.A. The value of pleural fluid analysis. Am. J. Med. Sci. 2008, 335, 7–15. [Google Scholar] [CrossRef]
- Light, R.W.; Erozan, Y.S.; Ball, W.C., Jr. Cells in pleural fluid. Their value in differential diagnosis. Arch. Intern. Med. 1973, 132, 854–860. [Google Scholar] [CrossRef]
- Pettersson, T.; Riska, H. Diagnostic value of total and differential leukocyte counts in pleural effusions. Acta Med. Scandi-Navica 1981, 210, 129–135. [Google Scholar] [CrossRef]
- Porcel, J.M.; Vives, M.; Esquerda, A.; Ruiz, A. Usefulness of the British Thoracic Society and the American College of Chest Physicians guidelines in predicting pleural drainage of non-purulent parapneumonic effusions. Respir. Med. 2006, 100, 933–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klockars, M.; Kleemola, M.; Leinonen, M.; Koskela, M. Serum adenosine deaminase in viral and bacterial pneumonia. Chest 1991, 99, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Suga, M.; Ando, M.; Tanaka, F.; Araki, S. Serum adenosine deaminase activity with Mycoplasma pneumoniae. Chest 1988, 94, 1315. [Google Scholar] [CrossRef] [PubMed]
- Yurt, S.; Kucukergin, C.; Yigitbas, B.A.; Seckin, S.; Tigin, H.C.; Kosar, A.F. Diagnostic utility of serum and pleural levels of adenosine deaminase 1-2, and interferon-gamma in the diagnosis of pleural tuberculosis. Multidiscip. Respir. Med. 2014, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Yoo, S.S.; Lee, S.Y.; Cha, S.I.; Park, J.Y.; Kim, C.H. Pleural fluid adenosine deaminase/serum C-reactive protein ratio for the differentiation of tuberculous and parapneumonic effusions with neutrophilic predominance and high adenosine deami-nase levels. Infection 2017, 45, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Daxboeck, F.; Krause, R.; Wenisch, C. Laboratory diagnosis of Mycoplasma pneumoniae infection. Clin. Microbiol. Infect. 2003, 9, 263–273. [Google Scholar] [CrossRef] [Green Version]
- Montagnani, F.; Rossetti, B.; Vannoni, A.; Cusi, M.G.; De Luca, A. Laboratory diagnosis of Mycoplasma pneumoniae infec-tions: Data analysis from clinical practice. New Microbiol. 2018, 41, 203–207. [Google Scholar]
- Miyashita, N.; Obase, Y.; Ouchi, K.; Kawasaki, K.; Kawai, Y.; Kobashi, Y.; Oka, M. Clinical features of severe Mycoplasma pneumoniae pneumonia in adults admitted to an intensive care unit. J. Med. Microbiol. 2007, 56, 1625–1629. [Google Scholar] [CrossRef] [Green Version]
- Chan, E.D.; Welsh, C.H. Fulminant Mycoplasma pneumoniae pneumonia. West. J. Med. 1995, 162, 133–142. [Google Scholar]
- Nagayama, Y.; Sakurai, N.; Tamai, K.; Niwa, A.; Yamamoto, K. Isolation of Mycoplasma pneumoniae from pleural fluid and/or cerebrospinal fluid: Report of four cases. Scand. J. Infect. Dis. 1987, 19, 521–524. [Google Scholar] [CrossRef]
- Spuesens, E.B.; Fraaij, P.L.; Visser, E.G.; Hoogenboezem, T.; Hop, W.C.; van Adrichem, L.N.; Weber, F.; Moll, H.A.; Broekman, B.; Berger, M.Y.; et al. Carriage of Mycoplasma pneumoniae in the upper respiratory tract of symptomatic and asymptomatic children: An observational study. PLoS Med. 2013, 10, e1001444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuvy, M.; Rav-Acha, M.; Izhar, U.; Ron, M.; Nir-Paz, R. Massive empyema caused by Mycoplasma pneumoniae in an adult: A case report. BMC Infect. Dis. 2006, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psallidas, I.; Kanellakis, N.I.; Bhatnagar, R.; Ravindran, R.; Yousuf, A.; Edey, A.J.; Mercer, R.M.; Corcoran, J.P.; Hallifax, R.J.; Asciak, R.; et al. A Pilot Feasibility Study in Establishing the Role of Ultrasound-Guided Pleural Biopsies in Pleural Infection (The AUDIO Study). Chest 2018, 154, 766–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loens, K.; Ieven, M. Mycoplasma pneumoniae: Current Knowledge on Nucleic Acid Amplification Techniques and Serologi-cal Diagnostics. Front. Microbiol. 2016, 7, 448. [Google Scholar] [CrossRef] [PubMed]
- Medjo, B.; Atanaskovic-Markovic, M.; Radic, S.; Nikolic, D.; Lukac, M.; Djukic, S. Mycoplasma pneumoniae as a causative agent of community-acquired pneumonia in children: Clinical features and laboratory diagnosis. Ital. J. Pediatr. 2014, 40, 104. [Google Scholar] [CrossRef] [Green Version]
- Porcel, J.M. Tuberculous pleural effusion. Lung 2009, 187, 263–270. [Google Scholar] [CrossRef]
- Zaric, B.; Kuruc, V.; Milovancev, A.; Markovic, M.; Sarcev, T.; Canak, V.; Pavlovic, S. Differential diagnosis of tuberculous and malignant pleural effusions: What is the role of adenosine deaminase? Lung 2008, 186, 233–240. [Google Scholar] [CrossRef]
- Jeon, D. Tuberculous pleurisy: An update. Tuberc. Respir. Dis. 2014, 76, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.J.; Kushner, I. Serum C-reactive protein levels in disease. Ann. N. Y. Acad. Sci. 1982, 389, 406–418. [Google Scholar] [CrossRef]
- Antoni, T.; Adamantia, L. Diagnosis and management of community-acquired pneumonia. In Oxford Textbook of Critical Care, 2nd ed.; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Pereyre, S.; Goret, J.; Bebear, C. Mycoplasma pneumoniae: Current Knowledge on Macrolide Resistance and Treatment. Front. Microbiol. 2016, 7, 974. [Google Scholar] [CrossRef] [Green Version]
- Leal, S.M., Jr.; Totten, A.H.; Xiao, L.; Crabb, D.M.; Ratliff, A.; Duffy, L.B.; Fowler, K.B.; Mixon, E.; Winchell, J.M.; Diaz, M.H.; et al. Evaluation of Commercial Molecular Diagnostic Methods for Detection and Determination of Macrolide Resistance in Mycoplasma pneumoniae. J. Clin. Microbiol. 2020, 58, e00242-20. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Proposed diagnostic algorithm for suspected patients with Mycoplasma pneumoniae parapneumonic effusion or tuberculous pleural effusion. MPPE = Mycoplasma pneumoniae parapneumonic effusion; TPE = tuberculous pleural effusion; WBC = white blood cell; PCR = polymerase chain reaction; ADA = adenosine deaminase; CRP = C-reactive protein.
Figure 1.
Proposed diagnostic algorithm for suspected patients with Mycoplasma pneumoniae parapneumonic effusion or tuberculous pleural effusion. MPPE = Mycoplasma pneumoniae parapneumonic effusion; TPE = tuberculous pleural effusion; WBC = white blood cell; PCR = polymerase chain reaction; ADA = adenosine deaminase; CRP = C-reactive protein.


{kind=link}
Table 1.
Literature review of pleural fluid analysis providing differential leukocyte counts or ADA levels in adult patients with Mycoplasma pneumoniae parapneumonic effusions.
Table 1.
Literature review of pleural fluid analysis providing differential leukocyte counts or ADA levels in adult patients with Mycoplasma pneumoniae parapneumonic effusions.
| No. | No. of Patients | Age (y)/Sex | Pleural Fluid | Year of Publication [Authors] [Reference No.] | |||||
|---|---|---|---|---|---|---|---|---|---|
| Amount | Total WBC (cells/μL) | Predominant Cell Type | Protein (g/dL) | LDH (U/L) | ADA (U/L) | ||||
| 1 | 1 | 30/F | NA | NA | Ly | 3.5 | NA | NA | 1971 [Feizi et al.] [29] |
| 2 | 1 | 24/M | L | 4800 | Ly = Ne | 5.4 | NA | NA | 1972 [Lewis et al.] [33] |
| 3 | 1 | 23/M | L | 650 | Ly | 3.6 | NA | NA | 1975 [Murray et al.] [37] |
| 4 | 1 | 62/F | Mo | 2600 | Ly | 1.8 | 104 | NA | 1975 [Chester et al.] [38] |
| 5 | 1 | 21/F | L | 4025 | Ne | 3.6 | NA | NA | 1976 [Gump et al.] [39] |
| 6 | 1 | 18/M | L | 41,000 | Ne | 4.0 | 835 | NA | 1979 [Solanki et al.] [34] |
| 7 | 1 | 24/M | Mo | 8350 | Ne | NA | NA | NA | 1984 [Linz et al.] [6] |
| 2 | 31/F | L | 1320 | Ne | NA | NA | NA | ||
| 8 | 1 | 37/F | S | 10,000 | Ne | 5.4 | 469 | 19 | 2012 [Cha et al.] [8] |
| 2 | 18/F | S | 500 | Ly | 5.5 | 632 | 88 | ||
| 3 | 20/F | S | 475 | Ly | 2.3 | 330 | 43 | ||
| 4 | 24/F | Mo | 5200 | Ly | 5.2 | 651 | 66 | ||
| 5 | 20/M | S | 250 | Ly | 4.3 | 2320 | 51 | ||
| 9 | 1 | 26/M | Mo | 3540 | Ne | 3.5 | 452 | 18 | 2017 [Bajantri et al.] [35] |
| 10 * | 1 | 76/F | S | 1600 | Ly | 5.3 | 1058 | 28 | 2017 [Kim et al.] [10] |
| 2 | 30/F | S | 425 | Ne | 2.5 | 244 | 10 | ||
| 3 | 42/F | S | 1825 | Ly | 3.0 | 935 | 49 | ||
| 4 | 19/M | S | 4502 | Ly | 3.8 | 1580 | 72 | ||
| 5 | 19/M | S | 2145 | Ly | 3.8 | 948 | 31 | ||
| 11 | 1 | 22/F | Mo | NA | Ly | NA | NA | NA | 2018 [Hassan et al.] [36] |
| 12 | 1 | 30/F | Mo | NA | Ly | 4.8 | 685 | 46 | 2020 [Wen et al.] [11] |
| 13 † | 1 | 34/F | NA | 163 | Ly | 2.1 | NA | 11 | 2020 [Ding et al.] [40] |
| 2 | 32/M | NA | 413 | Ly | 3.0 | 2322 | 25 | ||
| Total, median (IQR)/% | 23 | 24 (20–32)/ F (61%) | S (45%) | 1985 (481–4726) | Ly (68%) | 3.7 (3.0–5.1) | 685 (452–1058) | 37 (19–55)/ ADA > 40 (50%) | |
ADA = adenosine deaminase; WBC = white blood cell; LDH = lactate dehydrogenase; F = female; M = male; NA = not available; Ly = lymphocytic; Ne = neutrophilic; L = large; Mo = moderate; S = small; IQR = interquartile range. * Data for the remaining five patients were expressed after five patients included in the previous study (No. 8) were excluded. † Cases with severe M. pneumoniae pneumonia and acute respiratory distress syndrome.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kim, C.H.; Lee, J. Mycoplasma pneumoniae Pleural Effusion in Adults. J. Clin. Med. 2022, 11, 1281. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051281
AMA Style
Kim CH, Lee J. Mycoplasma pneumoniae Pleural Effusion in Adults. Journal of Clinical Medicine. 2022; 11(5):1281. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051281
Chicago/Turabian StyleKim, Chang Ho, and Jaehee Lee. 2022. "Mycoplasma pneumoniae Pleural Effusion in Adults" Journal of Clinical Medicine 11, no. 5: 1281. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11051281
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.