
Recombinase Polymerase Amplification Combined with Real-Time Fluorescent Probe for Mycoplasma pneumoniae Detection

Abstract
:1. Introduction
2. Materials and Methods
2.1. Experiment Design
2.2. RPA Assay
2.3. Specificity and Sensitivity of RPA Assay
2.4. The Application of RPA Assay in Clinical Specimens
3. Results
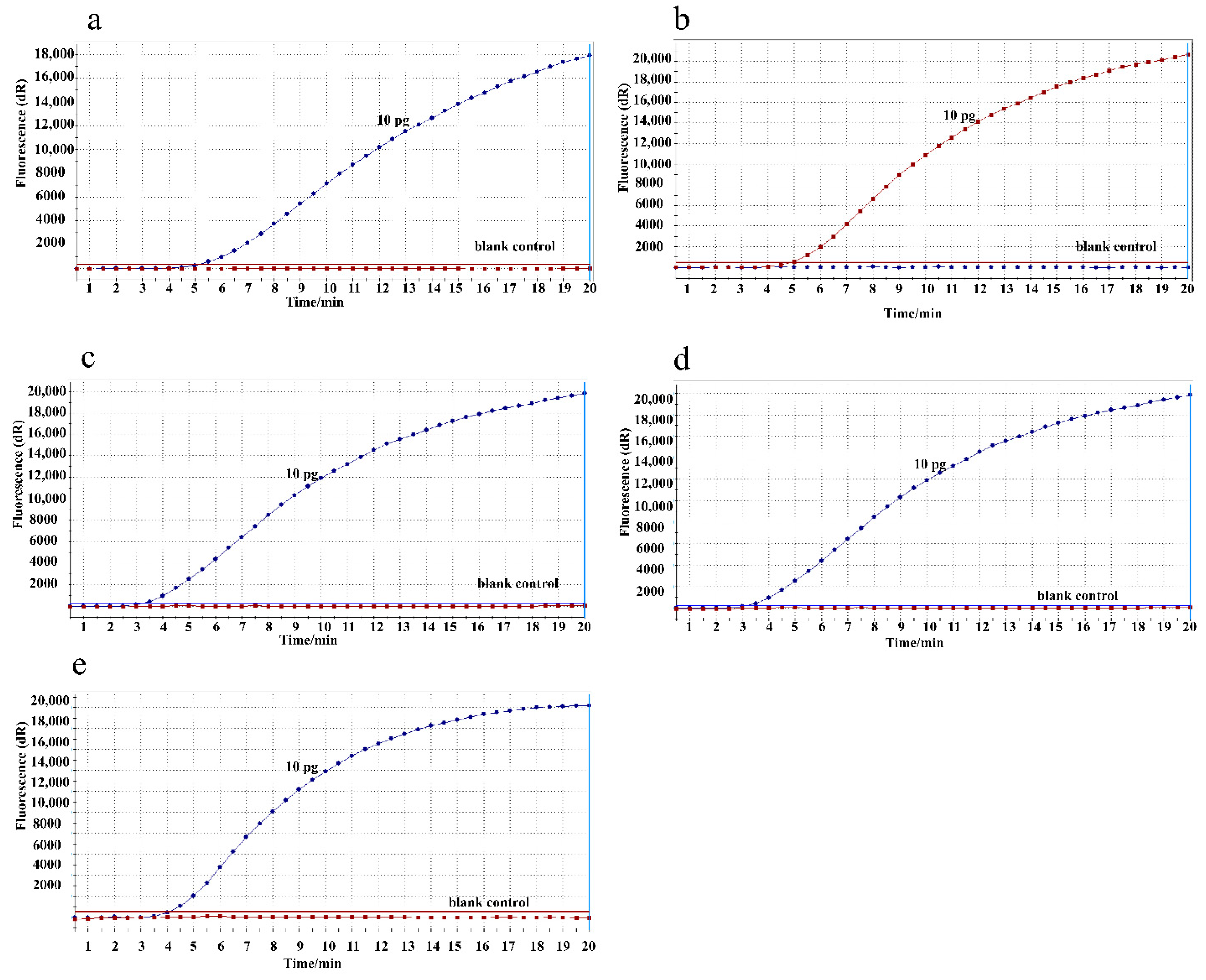
3.1. Amplification Temperature Optimization
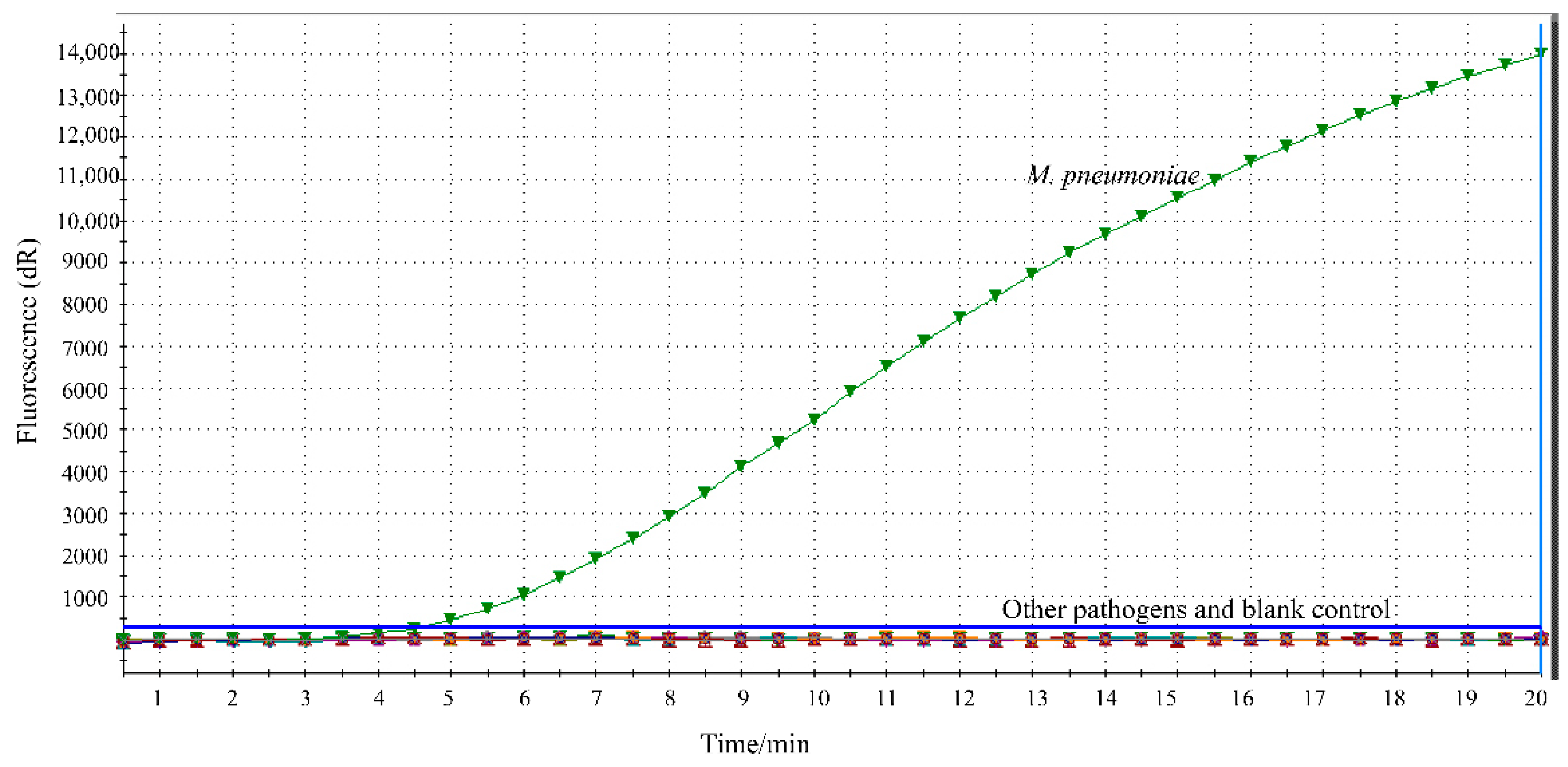
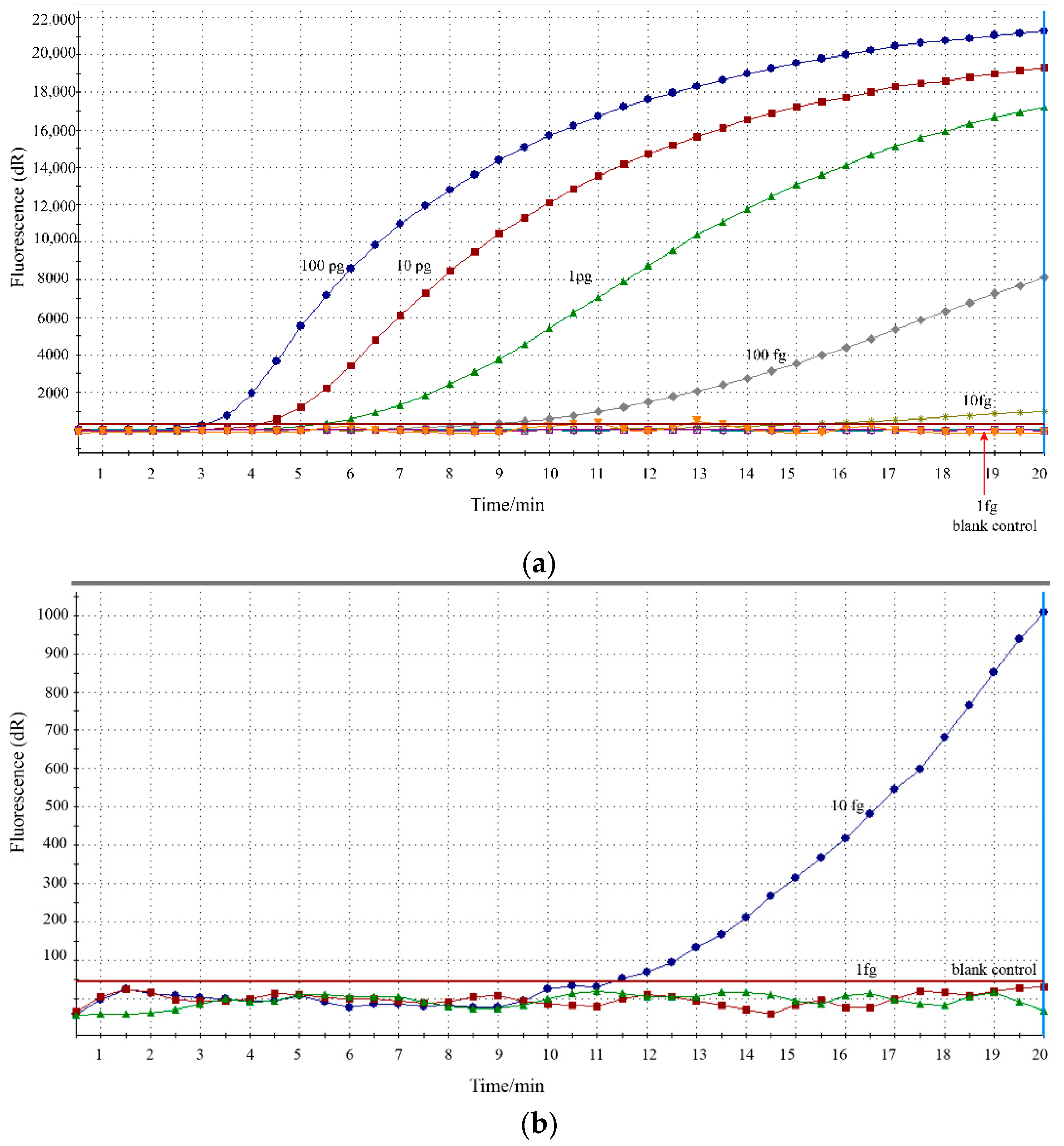
3.2. Analytical Specificity and Sensitivity of RPA Assay
3.3. Performance of RPA Assay in Clinical Specimens
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, L.-W.; Yin, J.; Hu, Y.-H.; Liu, X.-Y.; Feng, X.-L.; He, J.-X.; Liu, J.; Guo, Y.; Xu, B.-P.; Shen, K.-L. The epidemiology of paediatric Mycoplasma pneumoniae pneumonia in North China: 2006 to 2016. Epidemiol. Infect. 2019, 147, e192. [Google Scholar] [CrossRef] [Green Version]
- Oishi, T.; Fukuda, Y.; Wakabayashi, S.; Kono, M.; Ono, S.; Kato, A.; Kondo, E.; Nakamura, Y.; Tanaka, Y.; Teranishi, H.; et al. Low prevalence of Chlamydia pneumoniae infections during the Mycoplasma pneumoniae epidemic season: Results of nationwide surveillance in Japan. J. Infect. Chemother. 2020, 26, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Waites, K.B.; Talkington, D.F. Mycoplasma pneumoniae and Its Role as a Human Pathogen. Clin. Microbiol. Rev. 2004, 17, 697–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.-L.; Lee, C.-M.; Yang, T.-L.; Yen, T.-Y.; Chang, L.-Y.; Chen, J.-M.; Lee, P.-I.; Huang, L.-M.; Lu, C.-Y. Severe Mycoplasma pneumoniae pneumonia requiring intensive care in children, 2010–2019. J. Formos. Med. Assoc. 2021, 120 Pt 1, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.; Xue, G.; Zhao, H.; Feng, Y.; Li, S.; Cui, J.; Ni Mb, S.; Sun, H. Molecular and clinical characteristics of severe Mycoplasma pneumoniae pneumonia in children. Pediatr. Pulmonol. 2019, 54, 1012–1021. [Google Scholar] [CrossRef]
- Sauteur, P.M.M.; Unger, W.W.J.; van Rossum, A.M.C.; Berger, C. The Art and Science of Diagnosing Mycoplasma pneumoniae Infection. Pediatric Infect. Dis. J. 2018, 37, 1192–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Xu, B.; Wu, X.; Yin, Q.; Wang, Y.; Li, J.; Jiao, W.; Quan, S.; Sun, L.; Wang, Y.; et al. Increased Macrolide Resistance Rate of M3562 Mycoplasma pneumoniae Correlated with Macrolide Usage and Genotype Shifting. Front. Cell. Infect. Microbiol. 2021, 11, 675466. [Google Scholar] [CrossRef] [PubMed]
- Waites, K.B.; Xiao, L.; Liu, Y.; Balish, M.F.; Atkinson, T.P. Mycoplasma pneumoniae from the Respiratory Tract and Beyond. Clin. Microbiol. Rev. 2017, 30, 747–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daxboeck, F.; Kircher, K.; Krause, R.; Heinzl, H.; Wenisch, C.; Stanek, G. Effect of age on antibody titer to Mycoplasma pneumoniae. Scand. J. Infect. Dis. 2002, 34, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Gullsby, K.; Storm, M.; Bondeson, K. Simultaneous Detection of Chlamydophila pneumoniae and Mycoplasma pneumoniae by Use of Molecular Beacons in a Duplex Real-Time PCR. J. Clin. Microbiol. 2008, 46, 727–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loens, K.; Van Heirstraeten, L.; Malhotra-Kumar, S.; Goossens, H.; Ieven, M. Optimal Sampling Sites and Methods for Detection of Pathogens Possibly Causing Community-Acquired Lower Respiratory Tract Infections. J. Clin. Microbiol. 2009, 47, 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobato, I.M.; O’Sullivan, C.K. Recombinase polymerase amplification: Basics, applications and recent advances. TrAC Trends Anal. Chem. 2018, 98, 19–35. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Quan, S.; Jiao, W.; Li, J.; Sun, L.; Wang, Y.; Qi, X.; Wang, X.; Shen, A. Establishment and Application of a Multiple Cross Displacement Amplification Coupled with Nanoparticle-Based Lateral Flow Biosensor Assay for Detection of Mycoplasma pneumoniae. Front. Cell. Infect. Microbiol. 2019, 9, 325. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, Y.; Jiao, W.; Li, J.; Quan, S.; Sun, L.; Wang, Y.; Qi, X.; Wang, X.; Shen, A. Development of loop-mediated isothermal amplification coupled with nanoparticle-based lateral flow biosensor assay for Mycoplasma pneumoniae detection. AMB Express 2019, 9, 196. [Google Scholar] [CrossRef] [Green Version]
- Kissenkötter, J.; Böhlken-Fascher, S.; Forrest, M.S.; Piepenburg, O.; Czerny, C.-P.; El Wahed, A.A. Recombinase polymerase amplification assays for the identification of pork and horsemeat. Food Chem. 2020, 322, 126759. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, Y.; Zhang, R.; Han, Q.; Wang, J.; Liu, L.; Li, R.; Yuan, W. Recombinase polymerase amplification assay for rapid detection of porcine circovirus 3. Mol. Cell. Probes 2017, 36, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhang, X.; Wang, Y.; Shen, H.; Jiang, G.; Dong, J.; Zhao, P.; Gao, S. A Real-Time Recombinase Polymerase Amplification Method for Rapid Detection of Vibrio vulnificus in Seafood. Front. Microbiol. 2020, 11, 586981. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.-K.; Zhao, W.; Ye, M.-D.; Ali, F.; Wang, T.; Qi, R.-D. Evaluation of Recombinase Polymerase Amplification Assay for Detecting Meloidogyne javanica. Plant Dis. 2020, 104, 801–807. [Google Scholar] [CrossRef]
- Zhu, Y.; Zeng, F.; Sun, J.; Liu, X.; Wu, M.; Huang, B.; Lian, Y.; Xiao, L.; Ma, L.; Zhang, S.; et al. Application of recombinase polymerase amplification method for rapid detection of infectious laryngotracheitis virus. Mol. Cell. Probes 2020, 54, 101646. [Google Scholar] [CrossRef]
- Liu, L.; Li, R.; Zhang, R.; Wang, J.; An, Q.; Han, Q.; Wang, J.; Yuan, W. Rapid and sensitive detection of Mycoplasma hyopneumoniae by recombinase polymerase amplification assay. J. Microbiol. Methods 2019, 159, 56–61. [Google Scholar] [CrossRef]
- El Wahed, A.A.; Patel, P.; Maier, M.; Pietsch, C.; Rüster, D.; Böhlken-Fascher, S.; Kissenkötter, J.; Behrmann, O.; Frimpong, M.; Diagne, M.M.; et al. Suitcase Lab for Rapid Detection of SARS-CoV-2 Based on Recombinase Polymerase Amplification Assay. Anal. Chem. 2021, 93, 2627–2634. [Google Scholar] [CrossRef]
- McQuillan, J.S.; Wilson, M.W. Recombinase polymerase amplification for fast, selective, DNA-based detection of faecal indicator Escherichia coli. Lett. Appl. Microbiol. 2021, 72, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Kersting, S.; Rausch, V.; Bier, F.F.; Von Nickisch-Rosenegk, M. Rapid detection of Plasmodium falciparum with isothermal recombinase polymerase amplification and lateral flow analysis. Malar. J. 2014, 13, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandu, D.; Paul, S.; Parker, M.; Dudin, Y.; King-Sitzes, J.; Perez, T.; Mittanck, D.W.; Shah, M.; Glenn, K.C.; Piepenburg, O. Development of a Rapid Point-of-Use DNA Test for the Screening of Genuity® Roundup Ready 2 Yield® Soybean in Seed Samples. BioMed Res. Int. 2016, 2016, 3145921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Torres, J.E.P.; Goossens, J.; Stijlemans, B.; Sterckx, Y.G.-J.; Magez, S. Development of a recombinase polymerase amplification lateral flow assay for the detection of active Trypanosoma evansi infections. PLoS Negl. Trop. Dis. 2020, 14, e0008044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Xiao, L.; Cong, X.; Zhu, Y.; Huang, B.; Cong, F. Development of a recombinase polymerase amplification fluorescence assay to detect feline coronavirus. Mol. Cell. Probes 2020, 54, 101669. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, M.-C.; Liu, H.-C.; Lin, S.-Q.; Zhao, X.-Q.; Liu, Z.-G.; Zhao, L.-L.; Wan, K.-L. Detecting Mycobacterium tuberculosis complex and rifampicin resistance via a new rapid multienzyme isothermal point mutation assay. Anal. Biochem. 2021, 630, 114341. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Primers/Probes | Sequence (5′-3′) | Amplicon Size (bp) | Gene |
|---|---|---|---|
| Forward primer | TGACACCGCAAGACAGTGCAATAACTCAGT | ||
| Reverse primer | CTGAACATCAACAAAGAAGGTGCTAGCTGC | 179 bp | CARDS * |
| probe | ATACCAAGAGTGGTTCACAACACGATT/i6FAMdT//idsp//Ibhq1dt/ATGTATGTCCTTTG # |
| Strains | Source of Strains | Number of Strains | RPA Results |
|---|---|---|---|
| Mycoplasma pneumoniae | M129 | 1 | P |
| Mycoplasma genitalium | ATCC33530 | 1 | N |
| Mycoplasma orale | ATCC23714 | 1 | N |
| Mycoplasma hominis | ATCC23114 | 1 | N |
| Mycoplasma penetrans | ATCC55252 | 1 | N |
| Mycoplasma primatum | ATCC25960 | 1 | N |
| Streptococcus pneumoniae | Isolated strain (BCH) | 1 | N |
| Staphylococcus aureus | Isolated strain (BCH) | 1 | N |
| Klebsiella pneumoniae | Isolated strain (BCH) | N | |
| Pseudomonas aeruginosa | Isolated strain (BCH) | 1 | N |
| Mycobacterium tuberculosis | Isolated strain (BCH) | 1 | N |
| Haemophilus influenzae | Isolated strain (BCH) | 1 | N |
| Acinetobacter baumannii | Isolated strain (BCH) | N | |
| Stenotrophomonas maltophilia | Isolated strain (BCH) | 1 | N |
| Bordetella pertussis | Isolated strain (BCH) | 1 | N |
| Legionella pneumophila | Isolated strain (BCH) | 1 | N |
| Respiratory syncytial virus | Isolated strain (BCH) | 1 | N |
| Adenovirus type 3 | Isolated strain (BCH) | 1 | N |
| Rhinovirus | Isolated strain (BCH) | 1 | N |
| H1N1 influenza | Isolated strain (BCH) | 1 | N |
| RPA | Real-Time PCR | Total | Kappa | Performance of RPA Assay in Comparison to Real-Time PCR | ||
|---|---|---|---|---|---|---|
| Positive | Negative | Sensitivity | Specificity | |||
| Positive | 88 | 4 | 92 | 0.958 | 100% | 96.1% |
| Negative | 0 | 98 | 98 | |||
| Total | 88 | 102 | 190 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, T.; Wang, Y.; Jiao, W.; Song, Y.; Zhao, Q.; Wang, T.; Bi, J.; Shen, A. Recombinase Polymerase Amplification Combined with Real-Time Fluorescent Probe for Mycoplasma pneumoniae Detection. J. Clin. Med. 2022, 11, 1780. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11071780
Jiang T, Wang Y, Jiao W, Song Y, Zhao Q, Wang T, Bi J, Shen A. Recombinase Polymerase Amplification Combined with Real-Time Fluorescent Probe for Mycoplasma pneumoniae Detection. Journal of Clinical Medicine. 2022; 11(7):1780. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11071780
Chicago/Turabian StyleJiang, Tingting, Yacui Wang, Weiwei Jiao, Yiqin Song, Qing Zhao, Tianyi Wang, Jing Bi, and Adong Shen. 2022. "Recombinase Polymerase Amplification Combined with Real-Time Fluorescent Probe for Mycoplasma pneumoniae Detection" Journal of Clinical Medicine 11, no. 7: 1780. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11071780