
Iatrogenic Atrial Septal Defect after Intracardiac Echocardiography-Guided Left Atrial Appendage Closure: Incidence, Size, and Clinical Outcomes

Abstract
:1. Introduction
2. Materials and Methods
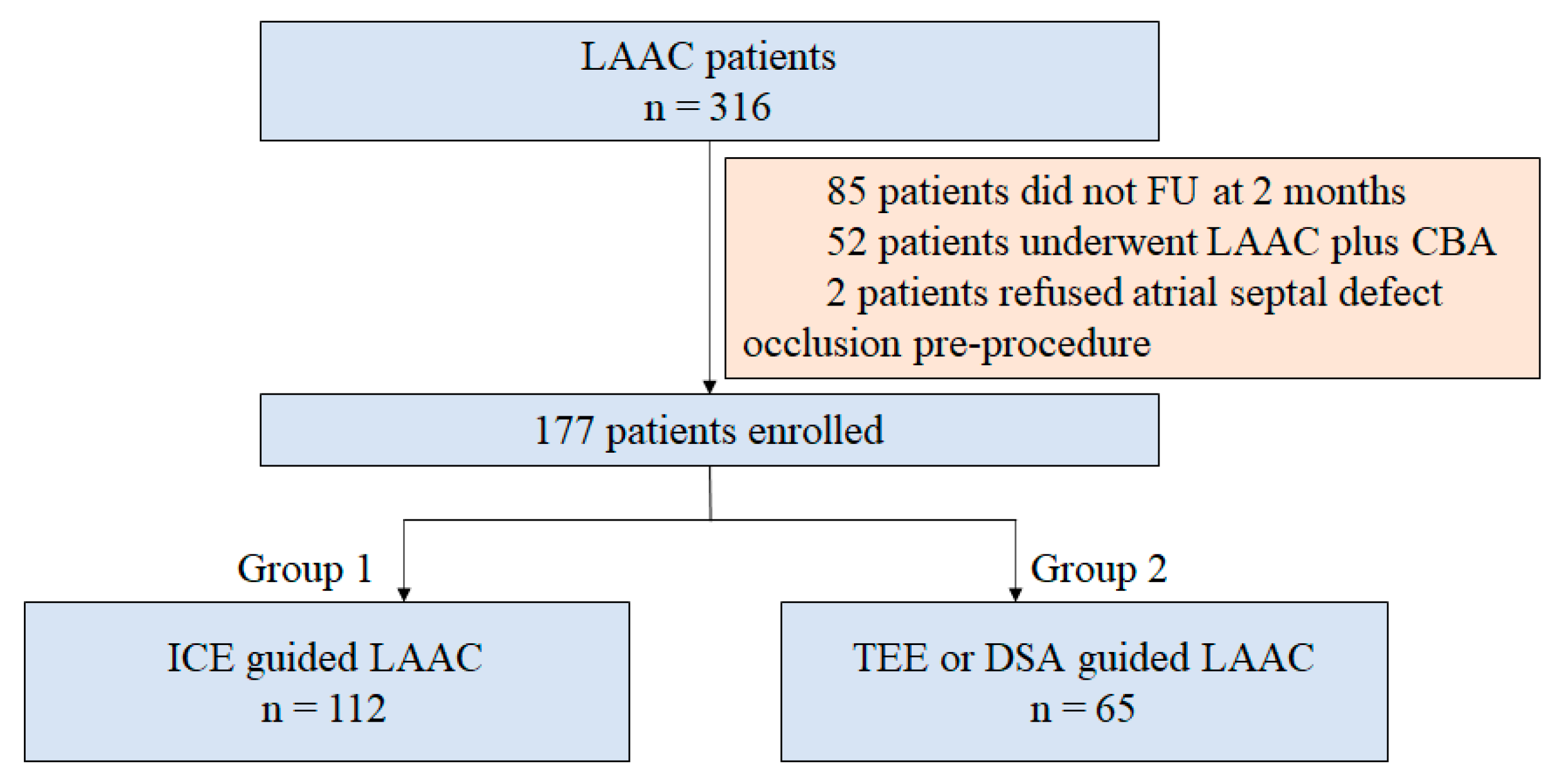
2.1. Study Population
2.2. Procedure
2.2.1. ICE-Guided TP Procedure
2.2.2. TEE- or DSA-Guided TP Procedure
2.3. Outpatient Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics at Baseline
3.2. Procedure Characteristics
3.3. Two Months FU
3.4. Twelve Months FU
3.5. Relationship between Patent iASD and ICE-Guided LAAC
4. Discussion
4.1. Incidence and Size of Patent iASD after LAAC
4.2. Predictive Indicators of iASD
4.3. Clinical Outcomes of Patent iASD
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reddy, V.Y.; Möbius-Winkler, S.; Miller, M.A.; Neuzil, P.; Schuler, G.; Wiebe, J.; Sick, P.; Sievert, H. Left atrial appendage closure with the Watchman device in patients with a contraindication for oral anticoagulation: The ASAP study (ASA Plavix Feasibility Study with Watchman Left Atrial Appendage Closure Technology). J. Am. Coll. Cardiol. 2013, 61, 2551–2556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osmancik, P.; Herman, D.; Neuzil, P.; Hala, P.; Taborsky, M.; Kala, P.; Poloczek, M.; Stasek, J.; Haman, L.; Branny, M.; et al. Left Atrial Appendage Closure Versus Direct Oral Anticoagulants in High-Risk Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 75, 3122–3135. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Rich, M.E.; Tseng, A.; Lim, H.W.; Wang, P.J.; Su, W.W. Reduction of Iatrogenic Atrial Septal Defects with an Anterior and Inferior Transseptal Puncture Site when Operating the Cryoballoon Ablation Catheter. J. Vis. Exp. 2015, 100, e52811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, B.; Blaauw, Y.; Khattab, A.A.; Lewalter, T.; Sievert, H.; Tondo, C.; Glikson, M.; ESC Scientific Document Group. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion. Europace 2014, 16, 1397–1416. [Google Scholar] [CrossRef] [PubMed]
- Berti, S.; Paradossi, U.; Meucci, F.; Trianni, G.; Tzikas, A.; Rezzaghi, M.; Stolkova, M.; Palmieri, C.; Mori, F.; Santoro, G. Periprocedural intracardiac echocardiography for left atrial appendage closure: A dual-center experience. JACC Cardiovasc. Interv. 2014, 7, 1036–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuniadi, Y.; Hanafy, D.A.; Raharjo, S.B.; Yugo, D. Left atrial appendage closure device implantation guided with fluoroscopy only: Long-term results. J. Arrhythm. 2019, 35, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korsholm, K.; Jensen, J.M.; Nielsen-Kudsk, J.E. Intracardiac Echocardiography from the Left Atrium for Procedural Guidance of Transcatheter Left Atrial Appendage Occlusion. JACC Cardiovasc. Interv. 2017, 10, 2198–2206. [Google Scholar] [CrossRef] [PubMed]
- Puga, L.; Teixeira, R.; Paiva, L.; Ribeiro, J.M.; Gameiro, J.; Sousa, J.P.; Costa, M.; Gonçalves, L. Iatrogenic atrial septal defect after percutaneous left atrial appendage closure: A single-center study. Int. J. Cardiovasc. Imaging 2021, 37, 2359–2368. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, T.; Miyasaka, M.; Flint, N.; Manabe, O.; Dawkins, S.; Cheng, R.; Hussaini, A.; Makar, M.; Kar, S.; Nakamura, M. Right-to-Left Shunt Through Iatrogenic Atrial Septal Defect After MitraClip Procedure. JACC Cardiovasc. Interv. 2020, 13, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- Rosu, R.; Cismaru, G.; Muresan, L.; Puiu, M.; Gusetu, G.; Istratoaie, S.; Pop, D.; Zdrenghea, D. Intracardiac echocardiography for transseptal puncture. A guide for cardiac electrophysiologists. Med. Ultrason. 2019, 21, 183–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.H.; Wang, L.G.; Zhou, X.D.; Fang, Y.; Su, L.; Wu, S.J.; Huang, W.J.; Xiao, F.Y. Outcome and safety of intracardiac echocardiography guided left atrial appendage closure within zero-fluoroscopy atrial fibrillation ablation procedures. J. Cardiovasc. Electrophysiol. 2022, 33, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Nelles, D.; Vij, V.; Al-Kassou, B.; Weber, M.; Vogelhuber, J.; Beiert, T.; Nickenig, G.; Schrickel, J.W.; Sedaghat, A. Incidence, persistence, and clinical relevance of iatrogenic atrial septal defects after percutaneous left atrial appendage occlusion. Echocardiography 2022, 39, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.M.; Douglas, P.S.; Reddy, V.Y. The incidence and long-term clinical outcome of iatrogenic atrial septal defects secondary to transseptal catheterization with a 12F transseptal sheath. Circ. Arrhythm. Electrophysiol. 2011, 4, 166–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkhouli, M.; Sarraf, M.; Holmes, D.R. Iatrogenic Atrial Septal Defect. Circ. Cardiovasc. Interv. 2016, 9, e003545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, T.; Takatsuki, S.; Inagawa, K.; Katsumata, Y.; Nishiyama, T.; Nishiyama, N.; Fukumoto, K.; Aizawa, Y.; Tanimoto, Y.; Tanimoto, K.; et al. Anatomical characteristics of the left atrial appendage in cardiogenic stroke with low CHADS2 scores. Heart. Rhythm. 2013, 10, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.Y.; Choy, C.C.; Yuen, H.C.; Chow, H.F.; Fong, H.F. A Very Long-term Longitudinal Study on the Evolution and Clinical Outcomes of Persistent Iatrogenic Atrial Septal Defect After Cryoballoon Ablation. Can. J. Cardiol. 2019, 35, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Schueler, R.; Öztürk, C.; Wedekind, J.A.; Werner, N.; Stöckigt, F.; Mellert, F.; Nickenig, G.; Hammerstingl, C. Persistence of iatrogenic atrial septal defect after interventional mitral valve repair with the MitraClip system: A note of caution. JACC Cardiovasc. Interv. 2015, 8, 450–459. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (n = 112) | Group 2 (n = 65) | p-Value | |
|---|---|---|---|
| Demographics | |||
| Age, years | n = 112, 64.6 ± 8.8 | n = 65, 64.4 ± 9.6 | 0.844 |
| Male sex | n = 112, 72 (64.3) | n = 65, 44 (67.7) | 0.743 |
| BMI, kg/m2 | n = 112, 25.1 ± 3.2 | n = 65, 25.0 ± 3.5 | 0.783 |
| AF overview | |||
| Paroxysmal AF | n = 112, 43 (38.4) | n = 65, 11 (16.9) | 0.004 |
| Non-paroxysmal AF | n = 112, 69 (61.6) | n = 65, 54 (83.1) | 0.004 |
| AF duration, months | n = 112, 12.0 (4.0, 48.0) | n = 65, 24.0 (6.0, 90.0) | 0.041 |
| Risk factors | |||
| CHA2DS2-VASc score | n = 112, 3.3 ± 1.7 | n = 65, 3.5 ± 1.9 | 0.551 |
| Heart failure | n = 112, 34 (30.4) | n = 65, 22 (33.8) | 0.738 |
| Hypertension | n = 112, 58 (51.8) | n = 65, 41 (63.1) | 0.160 |
| Age ≥ 75 years | n = 112, 11 (9.8) | n = 65, 9 (13.8) | 0.464 |
| Stroke/TIA/SE | n = 112, 39 (34.8) | n = 65, 19 (29.2) | 0.508 |
| Coronary artery disease | n = 112, 32 (28.6) | n = 65, 19 (29.2) | 1.000 |
| Age 65–74 years | n = 112, 50 (44.6) | n = 65, 25 (38.5) | 0.435 |
| HASBLED score | n = 112, 1.8 ± 1.1 | n = 65, 1.8 ± 1.2 | 0.812 |
| Echocardiographic index | |||
| LAD, mm | n = 112, 44.6 ± 5.6 | n = 65, 46.1 ± 6.7 | 0.120 |
| LVEF, % | n = 112, 55.4 ± 6.0 | n = 65, 55.3 ± 5.8 | 0.886 |
| Pathological mitral regurgitation | n = 112, 28 (25.0) | n = 65, 17 (26.2) | 0.860 |
| Pathological tricuspid regurgitation | n = 112, 37 (33.0) | n = 65, 26 (40.0) | 0.416 |
| Pulmonary hypertension | n = 112, 7 (6.3) | n = 65, 16 (24.6) | 0.001 |
| Mean pressure, mmHg | n = 7, 45.0 ± 3.5 | n = 16, 43.6 ± 8.6 | 0.678 |
| Group 1 (n = 112) | Group 2 (n = 65) | p-Value | |
|---|---|---|---|
| Device | 0.414 | ||
| WATCHMAN | n = 112, 90 (80.4) | n = 65, 55 (84.6) | |
| LACbes | n = 112, 22 (19.6) | n = 65, 9 (13.8) | |
| Intra-procedure details | |||
| LAAC success | n = 112, 111 (99.1) | n = 65, 64 (98.5) | 1.000 |
| Combined with RFCA | n = 112, 101 (90.2) | n = 65, 26 (40.0) | 0.000 |
| PFO occlusion | n = 112, 0 (0.0) | n = 65, 9 (13.8) | 0.000 |
| Discharge medication | 0.011 | ||
| OAC monotherapy | n = 112, 107 (95.5) | n = 65, 57 (87.7) | |
| OAC plus single antiplatelet therapy | n = 112, 5 (4.5) | n = 65, 3 (4.6) | |
| Dual antiplatelet therapy | n = 112, 0 (0.0) | n = 65, 5 (7.7) |
| Group 1 (n = 112) | Group 2 (n = 65) | p-Value | |
|---|---|---|---|
| First FU (month 2) | |||
| Time to review, days | n = 112, 57.5 (44.0, 75.0) | n = 65, 57.0 (50.0, 71.0) | 0.236 |
| Examination | 0.001 | ||
| TEE | n = 112, 33 (29.5) | n = 65, 35 (53.8) | |
| TTE | n = 112, 79 (70.5) | n = 65, 30 (46.2) | |
| Patent iASD | n = 112, 24 (21.4) | n = 65, 10 (15.4) | 0.429 |
| TEE-detected | n = 33, 9 (27.3) | n = 35, 4 (11.4) | 0.128 |
| TTE-detected | n = 79, 15 (19.0) | n = 30, 6 (20.0) | 1.000 |
| Shunt | 1.000 | ||
| LR shunt | n = 24, 24 (100.0) | n = 10, 10 (100.0) | |
| RL shunt | n = 24, 0 (0.0) | n = 10, 0 (0.0) | |
| Size, mm | n = 24, 2.8 ± 0.9 | n = 10, 2.2 ± 0.8 | 0.065 |
| New-onset pulmonary hypertension | n = 112, 3 (2.68) | n = 65, 0 (0.0) | 0.299 |
| Final FU (month 12) | |||
| Time to review, days | n = 17, 221.0 (161.0, 392.0) | n = 7, 260.0 (204.0, 364.0) | 0.619 |
| Residual iASD | n = 17, 5 (29.4) | n = 7, 2 (28.6) | 1.000 |
| Shunt | 1.000 | ||
| LR shunt | n = 5, 5 (100.0) | n = 2, 2 (100.0) | |
| RL shunt | n = 5, 0 (0.0) | n = 2, 0 (0.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Guo, L.; Li, J.; Liu, H.; Xu, J.; Du, H.; Wang, Y.; Li, H.; Yi, F. Iatrogenic Atrial Septal Defect after Intracardiac Echocardiography-Guided Left Atrial Appendage Closure: Incidence, Size, and Clinical Outcomes. J. Clin. Med. 2023, 12, 160. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12010160
Ma Y, Guo L, Li J, Liu H, Xu J, Du H, Wang Y, Li H, Yi F. Iatrogenic Atrial Septal Defect after Intracardiac Echocardiography-Guided Left Atrial Appendage Closure: Incidence, Size, and Clinical Outcomes. Journal of Clinical Medicine. 2023; 12(1):160. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12010160
Chicago/Turabian StyleMa, Yibo, Lanyan Guo, Jie Li, Haitao Liu, Jian Xu, Hui Du, Yi Wang, Huihui Li, and Fu Yi. 2023. "Iatrogenic Atrial Septal Defect after Intracardiac Echocardiography-Guided Left Atrial Appendage Closure: Incidence, Size, and Clinical Outcomes" Journal of Clinical Medicine 12, no. 1: 160. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12010160