Idiopathic Nephrotic Syndrome: Characteristics and Identification of Prognostic Factors

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Population
2.2. Clinical Data
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Immunosuppressive Therapy
3.3. INS Evolution
3.4. Risk Factors
3.5. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Audard, V.; Lang, P.; Sahali, D. Pathogénie du syndrome néphrotique à lesions glomérulaires minimes. Médecine/Sciences 2008, 24, 853–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rea, R.; Smith, C.; Sandhu, K.; Kwan, J.; Tomson, C. Successful transplant of a kidney with focal segmental glomerulosclerosis. Nephrol. Dial. Transplant. 2001, 16, 416–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feld, S.M.; Figueroa, P.; Savin, V.; Nast, C.C.; Sharma, R.; Sharma, M.; Hirschberg, R.; Adler, S.G. Plasmapheresis in the treatment of steroid-resistant focal segmental glomerulosclerosis in native kidneys. Am. J. Kidney Dis. 1998, 32, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Davenport, R.D. Apheresis treatment of recurrent focal segmental glomerulosclerosis after kidney transplantation: Re-analysis of published case-reports and case-series. J. Clin. Aphere. 2001, 16, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Kemper, M.J.; Wolf, G.; Müller-Wiefel, D.E. Transmission of glomerular permeability factor from a mother to her child. N. Engl. J. Med. 2001, 344, 386–387. [Google Scholar] [CrossRef] [PubMed]
- Lagrue, G.; Xheneumont, S.; Branellec, A.; Hirbec, G.; Weil, B. A vascular permeability factor elaborated from lymphocytes. I. Demonstration in patients with nephrotic syndrome. Biomedicine 1975, 23, 37–40. [Google Scholar] [PubMed]
- Zimmerman, S.W. Increased urinary protein excretion in the rat produced by serum from a patient with recurrent focal glomerular sclerosis after renal transplantation. Clin. Nephrol. 1984, 22, 32–38. [Google Scholar] [PubMed]
- Lai, K.-W.; Wei, C.-L.; Tan, L.-K.; Tan, P.-H.; Chiang, G.S.C.; Lee, C.G.L.; Jordan, S.C.; Yap, H.K. Overexpression of interleukin-13 induces minimal-change-like nephropathy in rats. JASN 2007, 18, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Lennon, R.; Singh, A.; Welsh, G.I.; Coward, R.J.; Satchell, S.; Ni, L.; Mathieson, P.W.; Bakker, W.W.; Saleem, M.A. Hemopexin induces nephrin-dependent reorganization of the actin cytoskeleton in podocytes. JASN 2008, 19, 2140–2149. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Trachtman, H.; Li, J.; Dong, C.; Friedman, A.L.; Gassman, J.J.; McMahan, J.L.; Radeva, M.; Heil, K.M.; Trautmann, A.; et al. Circulating suPAR in two cohorts of primary FSGS. JASN 2012, 23, 2051–2059. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, E.T.; Sharma, M.; Savin, V.J. Circulating permeability factors in idiopathic nephrotic syndrome and focal segmental glomerulosclerosis. Clin. J. Am. Soc. Nephrol. 2010, 5, 2115–2121. [Google Scholar] [CrossRef] [PubMed]
- Delville, M.; Sigdel, T.K.; Wei, C.; Li, J.; Hsieh, S.-C.; Fornoni, A.; Burke, G.W.; Bruneval, P.; Naesens, M.; Jackson, A.; et al. A circulating antibody panel for pretransplant prediction of FSGS recurrence after kidney transplantation. Sci. Transl. Med. 2014, 6, 256ra136. [Google Scholar] [CrossRef] [PubMed]
- Shalhoub, R.J. Pathogenesis of lipoid nephrosis: A disorder of T-cell function. Lancet 1974, 2, 556–560. [Google Scholar] [CrossRef]
- Grimbert, P.; Audard, V.; Remy, P.; Lang, P.; Sahali, D. Recent approaches to the pathogenesis of minimal-change nephrotic syndrome. Nephrol. Dial. Transplant. 2003, 18, 245–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolasco, F.; Cameron, J.S.; Heywood, E.F.; Hicks, J.; Ogg, C.; Williams, D.G. Adult-onset minimal change nephrotic syndrome: A long-term follow-up. Kidney Int. 1986, 29, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Mak, S.K.; Short, C.D.; Mallick, N.P. Long-term outcome of adult-onset minimal-change nephropathy. Nephrol. Dial. Transplant. 1996, 11, 2192–2201. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Yoo, K.D.; Oh, Y.K.; Kim, D.K.; Oh, K.-H.; Joo, K.W.; Kim, Y.S.; Ahn, C.; Han, J.S.; Lim, C.S. Predictors of relapse in adult-onset nephrotic minimal change disease. Medicine 2016, 95, e3179. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. KDIGO Clinical Practice Guideline for Glomerulonephritis. Kidney Int. Suppl. 2012, 2, 139–274. [Google Scholar]
- Fujimoto, S.; Yamamoto, Y.; Hisanaga, S.; Morita, S.; Eto, T.; Tanaka, K. Minimal change nephrotic syndrome in adults: Response to corticosteroid therapy and frequency of relapse. Am. J. Kidney Dis. 1991, 17, 687–692. [Google Scholar] [CrossRef]
- Fernandez-Juarez, G.; Villacorta, J.; Ruiz-Roso, G.; Panizo, N.; Martinez-Marín, I.; Marco, H.; Arrizabalaga, P.; Díaz, M.; Perez-Gómez, V.; Vaca, M.; et al. Therapeutic variability in adult minimal change disease and focal segmental glomerulosclerosis. Clin. Kidney J. 2016, 9, 381–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stirling, C.M.; Mathieson, P.; Boulton-Jones, J.M.; Feehally, J.; Jayne, D.; Murray, H.M.; Adu, D. Treatment and outcome of adult patients with primary focal segmental glomerulosclerosis in five UK renal units. QJM 2005, 98, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwood, A.M.; Gunnarsson, R.; Neuen, B.L.; Oliver, K.; Green, S.J.; Baer, R.A. Clinical presentation, treatment and outcome of focal segmental glomerulosclerosis in Far North Queensland Australian adults. Nephrology 2017, 22, 520–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinzawa, M.; Yamamoto, R.; Nagasawa, Y.; Oseto, S.; Mori, D.; Tomida, K.; Hayashi, T.; Izumi, M.; Fukunaga, M.; Yamauchi, A.; et al. Comparison of methylprednisolone plus prednisolone with prednisolone alone as initial treatment in adult-onset minimal change disease: A retrospective cohort study. Clin. J. Am. Soc. Nephrol. 2014, 9, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Chun, M.J.; Korbet, S.M.; Schwartz, M.M.; Lewis, E.J. Focal segmental glomerulosclerosis in nephrotic adults: Presentation, prognosis, and response to therapy of the histologic variants. JASN 2004, 15, 2169–2177. [Google Scholar] [CrossRef] [PubMed]
- Waldman, M.; Crew, R.J.; Valeri, A.; Busch, J.; Stokes, B.; Markowitz, G.; D’Agati, V.; Appel, G. Adult minimal-change disease: Clinical characteristics, treatment, and outcomes. Clin. J. Am. Soc. Nephrol. 2007, 2, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.-C.; Lai, F.M.-M.; Chow, K.-M.; Kwan, B.C.-H.; Kwong, V.W.-K.; Leung, C.-B.; Li, P.K.-T. Long-term outcome of biopsy-proven minimal change nephropathy in Chinese adults. Am. J. Kidney Dis. 2015, 65, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.B.; Date, A.; Kirubakaran, M.G.; Shastry, J.C. Minimal-change nephrotic syndrome in adults treated with alternate-day steroids. Nephron 1987, 47, 209–210. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.J.; Hsu, S.C.; Chen, F.F.; Sung, J.M.; Tseng, C.C.; Wang, M.C. Adult-onset minimal change disease among Taiwanese: Clinical features, therapeutic response, and prognosis. Am. J. Nephrol. 2001, 21, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gonzalez, J.G.; Mireles-Zavala, L.G.; Rodriguez-Gutierrez, R.; Gomez-Almaguer, D.; Lavalle-Gonzalez, F.J.; Tamez-Perez, H.E.; Gonzalez-Saldivar, G.; Villarreal-Perez, J.Z. Hyperglycemia related to high-dose glucocorticoid use in noncritically ill patients. Diabetol. Metab. Syndr. 2013, 5, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Idiopathic MCD | Idiopathic FSGS | p | ||
|---|---|---|---|---|
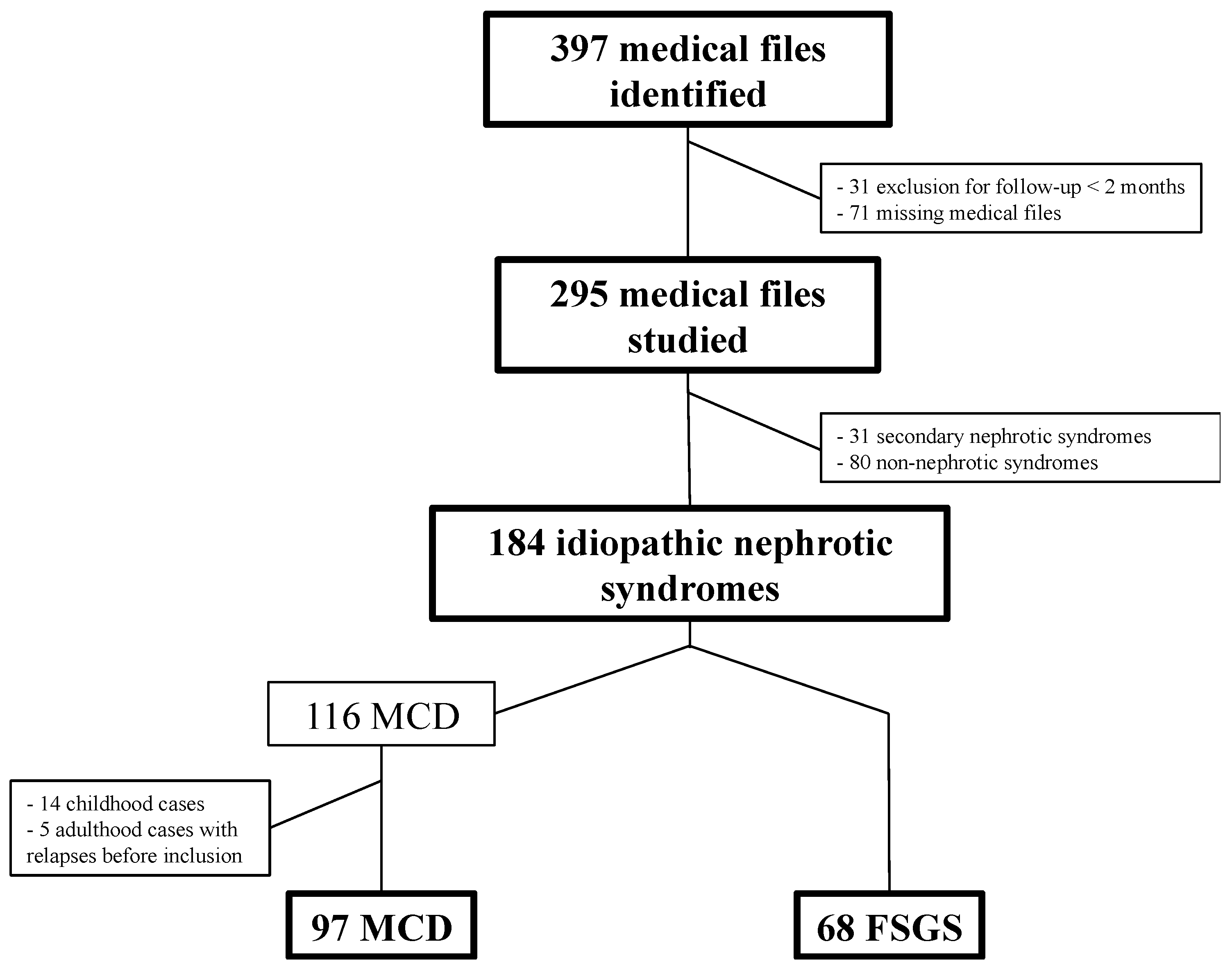
| n | Total | 97 | 68 | - |
| <30 years | 26.80% | 13.20% | ||
| 30–59 years | 39.20% | 48.50% | ||
| ≥60 years | 34% | 38.20% | ||
| Age | Median (IQR) | 47 (27.5–64) | 57 (42.2–66.7) | 0.01 |
| Sex ratio | Men/women | 55/42 | 48/20 | - |
| Hypertension | Total | 48.80% | 46.30% | 0.8 |
| <30 years | 21.70% | 33.30% | ||
| 30–59 years | 53.30% | 25% | ||
| ≥60 years | 35.50% | 80% | ||
| Body mass index | Median | 27 | 29 | 0.27 |
| (IQR) | (23–30) | (25–33) | ||
| Genetic factor | Research Identification | 7 (7.2%) | 1 (1.5%) | - |
| 1 (1%) | 0 | |||
| Familial INS | 4 (4.1%) | 0 | - | |
| Thrombosis history | Venous | 3 (3.1%) | 1 (1.5%) | - |
| Arterial | 3 (3.1%) | 5 (7.3%) | ||
| Cardiovascular risk factors | Median | 1 | 1 | - |
| (IQR) | (0–1.5) | (1–2) | ||
| Initial eGFR (MDRD, mL/min/1.73 m2) | Median (IQR) | 79 (49–103) | 42.5 (29–58) | <0.0001 |
| ≥90 | 36.80% | 6.20% | ||
| 60–89 | 28.70% | 12.50% | ||
| 30–59 | 26.50% | 51.60% | ||
| 15–29 | 3.40% | 28.10% | ||
| <15 | 4.60% | 1.60% | ||
| Proteinuria (g/day) | Median | 6.5 | 6 | 0.4 |
| (IQR) | (4.2–11) | (3.9–9) | ||
| Albuminemia (g/L) | Median (IQR) | 21 (16–23.5) | 29 (23–37) | <0.0001 |
| <30 g/L | 88.20% | 51.20% | ||
| <20 g/L | 42.30% | 13.90% | ||
| Cholesterol (g/L) | Median | 3.7 | 2.6 | - |
| (IQR) | (2.4–5) | (1.8–3.4) | ||
| Triglycerides (g/L) | Median | 1.9 | 2 | - |
| (IQR) | (1.2–2.7) | (1–3) |
| Idiopathic MCD | Idiopathic FSGS | p | ||
|---|---|---|---|---|
| n | 97 | 68 | ||
| Steroid therapy duration (months) | n | 89 (91.7%) | 35 (51.5%) | <0.0001 |
| First line | 8 (5–14.7) | 12 (8–18) | - | |
| Total | 13 (7–20.5) | 15 (8–36) | 0.26 | |
| Other immune suppressors | Cyclosporine | 37.10% | 23 (33.8%) | 0.7 |
| MMF | 19.80% | 7 (10.3%) | ||
| Cyclophosphamide | 5.20% | 1 (1.5%) | ||
| Tacrolimus | 3.40% | 0 | ||
| Azathioprine | 0.90% | 0 | ||
| Rituximab | n | 9 (9.3%) | 3 (4.4%) | - |
| Injections | 2 (2–3) | 4 (2–4) | ||
| Anticoagulation indication | n | 45 (46.4%) | 12 (17.6%) | 0.0002 |
| Atrial Fibrillation | 2 | 7 | ||
| Thrombosis | 6 | 0 | ||
| Albumin <20 | 35 | 5 | ||
| Unknown | 2 | 0 | ||
| RAS blockade | None | 24 (24.7%) | 3 (4.4%) | 0.003 |
| ACEi | 37 (38.1%) | 32 (47.1%) | ||
| ARB | 24 (24.7%) | 14 (20.6%) | ||
| ACEi + ARB | 12 (12.4%) | 19 (27.9%) |
| Idiopathic MCD | Idiopathic FSGS | p | ||
|---|---|---|---|---|
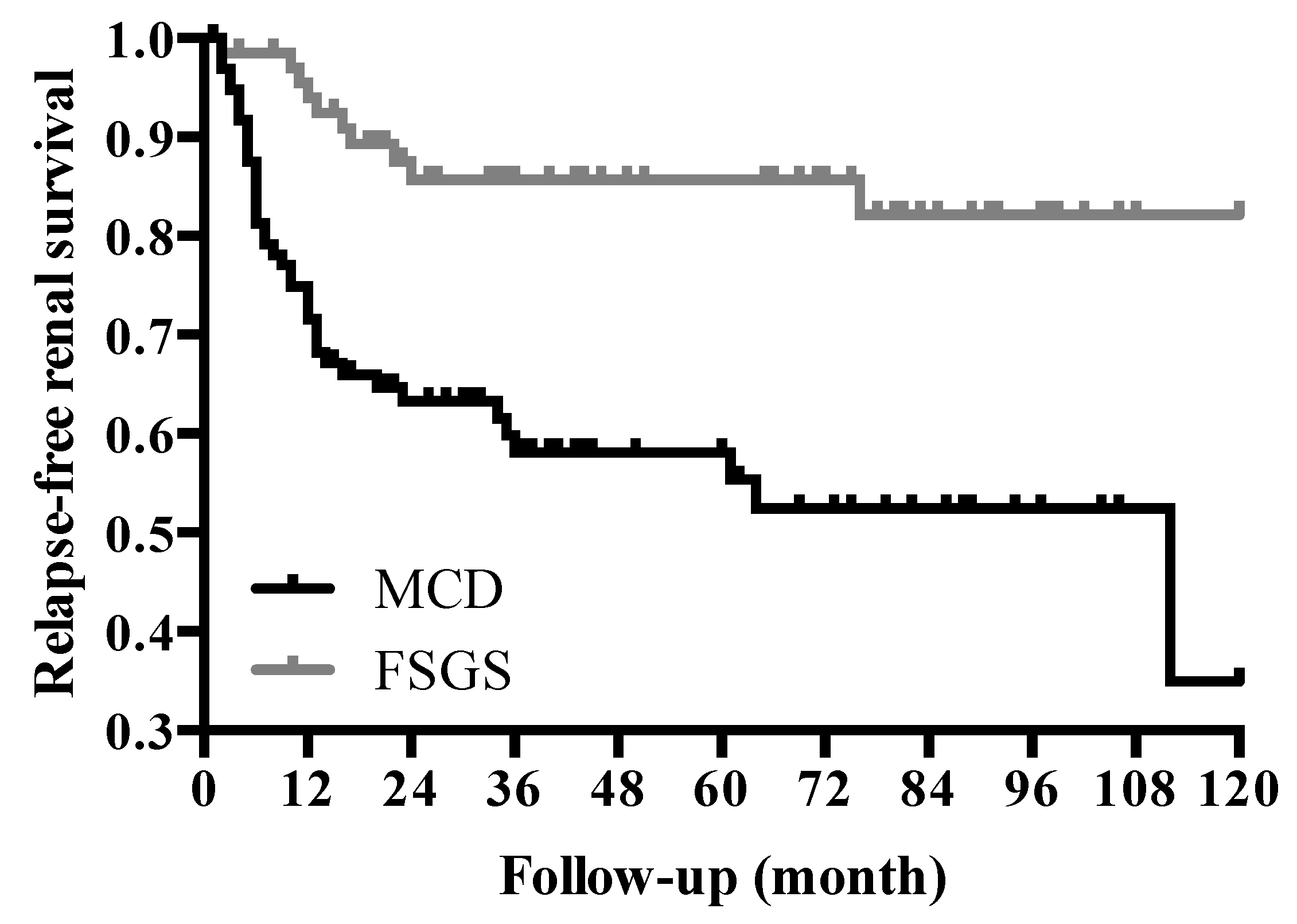
| n | 97 | 68 | - | |
| Follow-up | Median (IQR) | 45 (27–80.5) | 66 (30–92) | 0.11 |
| Remission | 90 (92.8%) | 50 (73.5%) | 0.001 | |
| Remission (8 weeks) | Complete remission | 43.40% | 4.20% | - |
| Partial remission | 31.30% | 44.70% | ||
| Total | 74.70% | 48.90% | ||
| Relapse | n | 41 (45.5%) | 10 (20%) | 0.003 |
| Relapse number | Median (IQR) | 2 (1–2.5) | 1 (1–1.25) | - |
| First relapse delay (month) | Median (IQR) | 7 (5.1–13.6) | 14.5 (10.7–22.5) | 0.06 |
| Variable | Odds Ratio (OR) | Confidence Interval (CI) 95% | p | |
|---|---|---|---|---|
| Age | 0.97 | 0.94–1.01 | 0.14 | |
| Initial presentation | Isolated | 1 | ||
| Associated * | 0.79 | 0.23–2.71 | 0.7 | |
| Hypertension | 2.06 | 0.63–6.77 | 0.23 | |
| eGFR (MDRD) | <60 | 1 | 0.58 | |
| 60–90 | 0.52 | 0.14–1.89 | ||
| >90 | 0.9 | 0.21–3.83 | ||
| Albuminemia | <20 | 1 | 0.91 | |
| >20 | 0.94 | 0.32–2.76 | ||
| RAS blockade | None | 1 | 0.3 | |
| ACEi | 2.16 | 0.5–9.39 | ||
| ARB | 3.41 | 0.63–18.70 | ||
| ACEi + ARB | 6.63 | 0.85–51.45 | ||
| Response (8 weeks) | Non responder | 1 | 0.48 | |
| Partial response | 1.65 | 0.36–7.52 | ||
| Complete response | 2.47 | 0.56–10.81 |
| Adverse Events | Histology | Total | <30 Years | 30–59 Years | ≥60 Years | p |
|---|---|---|---|---|---|---|
| Steroid-induced diabetes | MCD | 11.20% | 3.80% | 11.10% | 18.50% | 0.24 |
| FSGS | 11.40% | 0% | 5.50% | 33.30% | 0.07 | |
| Total | 11.30% | 3.80% | 8.90% | 19.10% | 0.16 | |
| Thrombosis | MCD | 7.20% | 3.80% | 7.90% | 9.10% | 0.73 |
| FSGS | 2.90% | 0% | 0% | 7.70% | 0.19 | |
| Total | 3.30% | 5.60% | 4.80% | 0.95 | ||
| Infection | MCD | 26.80% | 23.10% | 31.60% | 29.60% | 0.03 |
| FSGS | 13.20% | 33.30% | 3.30% | 19.2 | 0.03 | |
| Total | 23.30% | 19.40% | 22.60% | 0.86 | ||
| Neoplasia | MCD | 7.70% | 3% | 10.50% | 9.10% | 0.62 |
| FSGS | 0% | - | - | - | - | |
| Total | 0% | 6.90% | 4.80% | 0.45 | ||
| Death | MCD | 4.30% | 0% | 2.60% | 12.10% | 0.07 |
| FSGS | 5.90% | 0% | 3% | 11.50% | 0.28 | |
| Total | 0% | 2.80% | 11.10% | 0.049 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumas De La Roque, C.; Prezelin-Reydit, M.; Vermorel, A.; Lepreux, S.; Deminière, C.; Combe, C.; Rigothier, C. Idiopathic Nephrotic Syndrome: Characteristics and Identification of Prognostic Factors. J. Clin. Med. 2018, 7, 265. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7090265
Dumas De La Roque C, Prezelin-Reydit M, Vermorel A, Lepreux S, Deminière C, Combe C, Rigothier C. Idiopathic Nephrotic Syndrome: Characteristics and Identification of Prognostic Factors. Journal of Clinical Medicine. 2018; 7(9):265. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7090265
Chicago/Turabian StyleDumas De La Roque, Charlotte, Mathilde Prezelin-Reydit, Agathe Vermorel, Sébastien Lepreux, Colette Deminière, Christian Combe, and Claire Rigothier. 2018. "Idiopathic Nephrotic Syndrome: Characteristics and Identification of Prognostic Factors" Journal of Clinical Medicine 7, no. 9: 265. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7090265