Microangiopathy in Naifold Videocapillaroscopy and Its Relations to sE- Selectin, Endothelin-1, and hsCRP as Putative Endothelium Dysfunction Markers among Adolescents with Raynaud’s Phenomenon

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Methods
2.2.1. Nailfold Capillaroscopy
2.2.2. Qualitative Measurements
- non-specific pattern with a presence in at least two fingers: meandering and crossed capillaries, non-homogeneous distribution or size of loops (irregular arrangement), focal distribution of capillary hemorrhages, capillary spasm, widening of the afferent, apical and efferent parts of a loop, prominent subpapillary plexus [27].
- specific pathological (scleroderma pattern) with a presence of giant capillaries (3–4 times wider than the neighboring ones), frequent capillary hemorrhages, loss of capillaries (decrease of the capillary density <6 capillaries/linear mm), mild disorganization of the capillary architecture, the presence of avascular areas [29].
2.2.3. Analytical Methods
- sE-selectin concentration was determined by the ELISA immunoenzymatic test method, using R&D Systems Quantikine kit, according to the test manufacturer’s instructions. The intensity of the color reaction was determined at 450 nm wavelength. The test sensitivity was 0.027 ng/mL;
- endothelin-1 concentrations were determined by the ELISA method, using a kit produced by IBL International. The degree of staining was measured at 450 nm wavelength and was proportional to serum ET-1 concentration. The measurement range was from 0.78 to 100 pg/mL and the test sensitivity was 0.23 pg/mL;
- hsCRP concentration was determined by the immunoturbidimetric method with Roche Tina-quant CRP HS reagent, using HITACHI 912 biochemical analyzer. The normal range was 0–0.5 mg/dL.
2.2.4. The Statistical Analysis
2.2.5. Ethical Issues
3. Results
3.1. Analysis of Capillaroscopic Parameters
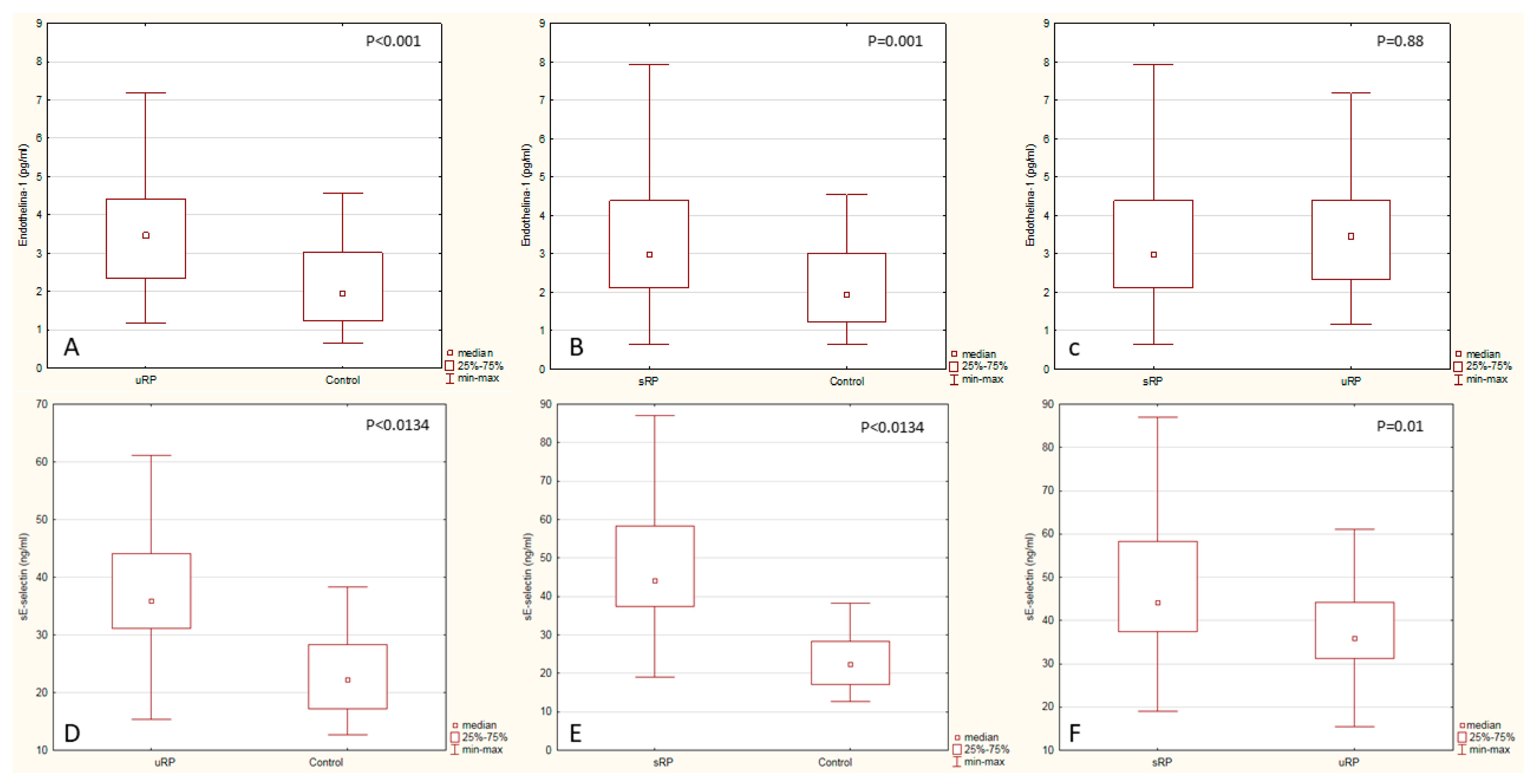
3.2. Analysis of Biochemical Tests
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- De Boer, M.P.; Meijer, R.I.; Wijnstok, N.J.; Jonk, A.M.; Houben, A.J.; Stehouwer, C.D.; Smulders, Y.M.; Eringa, E.C.; Serne, E.H. Microvascular dysfunction: A potential mechanism in the pathogenesis of obesity-associated insulin resistance and hypertension. Microcirculation 2012, 19, 5–18. [Google Scholar] [CrossRef]
- Heinen, Y.; Stegemann, E.; Sansone, R.; Benedens, K.; Wagstaff, R.; Balzer, J.; Rassaf, T.; Lauer, T.; Kelm, M.; Heiss, C. Local association between endothelial dysfunction and intimal hyperplasia: Relevance in peripheral artery disease. J. Am. Heart Assoc. 2015, 4, e001472. [Google Scholar] [CrossRef]
- Iurciuc, S.; Cimpean, A.M.; Mitu, F.; Heredea, R.; Iurciuc, M. Vascular aging and subclinical atherosclerosis: Why such a “never ending” and challenging story in cardiology? Clin. Interv. Aging 2017, 12, 1339. [Google Scholar] [CrossRef]
- Stringer, T.; Femia, A.N. Raynaud’s phenomenon: Current concepts. Clin. Dermatol. 2018, 36, 498–507. [Google Scholar] [CrossRef]
- Montesinos, B.L.; Fernandez, M.I.G.; Silveira, L.F.; Penades, I.C. Capillaroscopic findings in children and adolescents with raynaud’s phenomenon: Results from study in 92 patients. Pediatr. Rheumatol. 2014, 12, P283. [Google Scholar] [CrossRef]
- Ingegnoli, F.; Boracchi, P.; Gualtierotti, R.; Biganzoli, E.M.; Zeni, S.; Lubatti, C.; Fantini, F. Improving outcome prediction of systemic sclerosis from isolated Raynaud’s phenomenon: Role of autoantibodies and nail-fold capillaroscopy. Rheumatology 2010, 49, 797–805. [Google Scholar] [CrossRef]
- Ingegnoli, F.; Smith, V.; Sulli, A.; Cutolo, M. Capillaroscopy in Routine Diagnostics: Potentials and Limitations. Curr. Rheumatol. Rev. 2018, 14, 5–11. [Google Scholar] [CrossRef]
- Lambova, S.N.; Müller-Ladner, U. The specificity of capillaroscopic pattern in connective autoimmune diseases. A comparison with microvascular changes in diseases of social importance: Arterial hypertension and diabetes mellitus. Mod. Rheumatol. 2009, 19, 600–605. [Google Scholar] [CrossRef]
- Cutolo, M.; Sulli, A.; Secchi, M.E.; Paolino, S.; Pizzorni, C. Nailfold capillaroscopy is useful for the diagnosis and follow-up of autoimmune rheumatic diseases. A future tool for the analysis of microvascular heart involvement? Rheumatology 2006, 45, iv43–iv46. [Google Scholar] [CrossRef]
- Klein-Weigel, P.F.; Sunderkötter, C.; Sander, O. Nailfold capillaroscopy microscopy—An interdisciplinary appraisal. Vasa 2016, 45, 353–364. [Google Scholar] [CrossRef]
- Nakamura, Y.; Shinozaki, N.; Hirasawa, M.; Kato, R.; Shiraishi, K.; Kida, H.; Usuda, K.; Ishikawa, T. Prevalence of migraine and Raynaud’s phenomenon in Japanese patients with vasospastic angina. Jpn. Circ. J. 2000, 64, 239–242. [Google Scholar] [CrossRef]
- Le, J.H.; Im Cho, K. Association between endothelial function and microvascular changes in patients with secondary Raynaud’s phenomenon. Clin. Rheumatol. 2014, 33, 1627–1633. [Google Scholar] [CrossRef]
- Michalska-Jakubus, M.; Kowal-Bielecka, O.; Smith, V.; Cutolo, M.; Krasowska, D. Plasma endothelial microparticles reflect the extent of capillaroscopic alterations and correlate with the severity of skin involvement in systemic sclerosis. Microvasc. Res. 2017, 110, 24–31. [Google Scholar] [CrossRef]
- Saigal, R.; Kansal, A.; Mittal, M.; Singh, Y.; Ram, H. Raynaud’s phenomenon. J. Assoc. Phys. India 2010, 58, 309–313. [Google Scholar]
- Sulli, A.; Soldano, S.; Pizzorni, C.; Montagna, P.; Secchi, M.E.; Villaggio, B.; Seriolo, B.; Brizzolara, R.; Cutolo, M. Raynaud’s phenomenon and plasma endothelin: Correlations with capillaroscopic patterns in systemic sclerosis. J. Rheumatol. 2009, 36, 1235–1239. [Google Scholar] [CrossRef]
- Yamane, K. Endothelin and collagen vascular disease: A review with special reference to Raynaud’s phenomenon and systemic sclerosis. Intern. Med. Tokyo Jpn. 1994, 33, 579–582. [Google Scholar] [CrossRef]
- McEver, R.P. Selectins: Initiators of leucocyte adhesion and signalling at the vascular wall. Cardiovasc. Res. 2015, 107, 331–339. [Google Scholar] [CrossRef]
- Kuryliszyn-Moskal, A.; Dubicki, A.; Zarzycki, W.; Zonnenberg, A.; Górska, M. Microvascular abnormalities in capillaroscopy correlate with higher serum IL-18 and sE-selectin levels in patients with type 1 diabetes complicated by microangiopathy. Folia Histochem. Cytobiol. 2011, 49, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Hebbar, M.; Lassalle, P.; Janin, A.; Vanhée, D.; Bisiau, S.; Hatron, P.Y.; Tonnel, A.B.; Gosselin, B. E-selectin expression in salivary endothelial cells and sera from patients with systemic sclerosis. Role of resident mast cell-derived tumor necrosis factor alpha. Arthritis Rheum. 1995, 38, 406–412. [Google Scholar] [CrossRef]
- Kavazarakis, E.; Moustaki, M.; Gourgiotis, D.; Zeis, P.M.; Bossios, A.; Mavri, A.; Chronopoulou, A.; Karpathios, T. The impact of serum lipid levels on circulating soluble adhesion molecules in childhood. Pediatr. Res. 2002, 52, 454–458. [Google Scholar] [CrossRef]
- Glowinska, B.; Urban, M.; Peczynska, J.; Florys, B. Soluble adhesion molecules (sICAM-1, sVCAM-1) and selectins (sE selectin, sP selectin, sL selectin) levels in children and adolescents with obesity, hypertension, and diabetes. Metabolism 2005, 54, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Södergren, A.; Karp, K.; Boman, K.; Eriksson, C.; Lundström, E.; Smedby, T.; Söderlund, L.; Rantapää-Dahlqvist, S.; W\a allberg-Jonsson, S. Atherosclerosis in early rheumatoid arthritis: Very early endothelial activation and rapid progression of intima media thickness. Arthritis Res. Ther. 2010, 12, R158. [Google Scholar] [CrossRef] [PubMed]
- Amaya-Amaya, J.; Sarmiento-Monroy, J.C.; Mantilla, R.-D.; Pineda-Tamayo, R.; Rojas-Villarraga, A.; Anaya, J.-M. Novel risk factors for cardiovascular disease in rheumatoid arthritis. Immunol. Res. 2013, 56, 267–286. [Google Scholar] [PubMed]
- Ambrosino, P.; Lupoli, R.; Di Minno, A.; Tasso, M.; Peluso, R.; Di Minno, M.N.D. Subclinical atherosclerosis in patients with rheumatoid arthritis. Thromb. Haemost. 2015, 113, 916–930. [Google Scholar] [CrossRef] [PubMed]
- Vlahos, A.P.; Theocharis, P.; Bechlioulis, A.; Naka, K.K.; Vakalis, K.; Papamichael, N.D.; Alfantaki, S.; Gartzonika, K.; Mavridis, A.; Michalis, L.K. Changes in vascular function and structure in juvenile idiopathic arthritis. Arthritis Care Res. 2011, 63, 1736–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latuskiewicz-Potemska, J.; Chmura-Skirlinska, A.; Gurbiel, R.J.; Smolewska, E. Nailfold capillaroscopy assessment of microcirculation abnormalities and endothelial dysfunction in children with primary or secondary Raynaud syndrome. Clin. Rheumatol. 2016, 35, 1993–2001. [Google Scholar] [CrossRef] [PubMed]
- Ingegnoli, F.; Zeni, S.; Gerloni, V.; Fantini, F. Capillaroscopic observations in childhood rheumatic diseases and healthy controls. Clin. Exp. Rheumatol. 2005, 23, 905. [Google Scholar]
- Gerhold, K.; Becker, M.O. Nailfold capillaroscopy in juvenile rheumatic diseases: Known measures, patterns and indications. Clin. Exp. Rheumatol. 2014, 32, S183–S188. [Google Scholar]
- Cutolo, M.; Sulli, A.; Pizzorni, C.; Accardo, S. Nailfold videocapillaroscopy assessment of microvascular damage in systemic sclerosis. J. Rheumatol. 2000, 27, 155–160. [Google Scholar]
- Dolezalova, P.; Young, S.P.; Bacon, P.A.; Southwood, T.R. Nailfold capillary microscopy in healthy children and in childhood rheumatic diseases: A prospective single blind observational study. Ann. Rheum. Dis. 2003, 62, 444–449. [Google Scholar] [CrossRef]
- Pavlov-Dolijanovic, S.; Damjanov, N.S.; Stojanovic, R.M.; Stupar, N.Z.V.; Stanisavljevic, D.M. Scleroderma pattern of nailfold capillary changes as predictive value for the development of a connective tissue disease: A follow-up study of 3,029 patients with primary Raynaud’s phenomenon. Rheumatol. Int. 2012, 32, 3039–3045. [Google Scholar] [CrossRef] [PubMed]
- Ingegnoli, F.; Herrick, A.L. Nailfold capillaroscopy in pediatrics. Arthritis Care Res. 2013, 65, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Herrick, A.L.; Moore, T.; Hollis, S.; Jayson, M.I. The influence of age on nailfold capillary dimensions in childhood. J. Rheumatol. 2000, 27, 797–800. [Google Scholar] [PubMed]
- Smith, V.; Riccieri, V.; Pizzorni, C.; Decuman, S.; Deschepper, E.; Bonroy, C.; Sulli, A.; Piette, Y.; De Keyser, F.; Cutolo, M. Nailfold capillaroscopy for prediction of novel future severe organ involvement in systemic sclerosis. J. Rheumatol. 2013, 40, 2023–2028. [Google Scholar] [CrossRef] [PubMed]
- Tudor, A.; Musat, A.; Teleianu, C.; Zapucioiu, C.; Bari, M.; Comanici, A. Aspects of nailfold capillaroscopy in children and young people with rheumatic disease. Romanian J. Intern. Med. Rev. Roum. Med. Interne 2004, 42, 211–215. [Google Scholar]
- Hirschl, M.; Hirschl, K.; Lenz, M.; Katzenschlager, R.; Hutter, H.-P.; Kundi, M. Transition from primary Raynaud’s phenomenon to secondary Raynaud’s phenomenon identified by diagnosis of an associated disease: Results of ten years of prospective surveillance. Arthritis Rheum. 2006, 54, 1974–1981. [Google Scholar] [CrossRef] [PubMed]
- Järvisalo, M.J.; Juonala, M.; Raitakari, O.T. Assessment of inflammatory markers and endothelial function. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 547–552. [Google Scholar] [CrossRef]
- Prete, M.; Fatone, M.C.; Favoino, E.; Perosa, F. Raynaud’s phenomenon: From molecular pathogenesis to therapy. Autoimmun. Rev. 2014, 13, 655–667. [Google Scholar] [CrossRef]
- Cimminiello, C.; Milani, M.; Uberti, T.; Arpaia, G.; Perolini, S.; Bonfardeci, G. Endothelin, vasoconstriction, and endothelial damage in Raynaud’s phenomenon. Lancet Lond. Engl. 1991, 337, 114–115. [Google Scholar] [CrossRef]
- Cooke, J.P.; Marshall, J.M. Mechanisms of Raynaud’s disease. Vasc. Med. 2005, 10, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-S.; Park, M.-K.; Kim, H.-Y.; Park, S.-H. Capillary dimension measured by computer-based digitalized image correlated with plasma endothelin-1 levels in patients with systemic sclerosis. Clin. Rheumatol. 2010, 29, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Unoki, H.; Iwasa, S.; Watanabe, T. Role of endothelin-1 in atherosclerosis. Ann. N. Y. Acad. Sci. 2000, 902, 84–94. [Google Scholar] [CrossRef]
- Stefan, J.; JACOBI, J.; DELLES, C.; SCHLAICH, M.P.; ALTER, O.; SCHMIEDER, R.E. Plasma soluble adhesion molecules and endothelium-dependent vasodilation in early human atherosclerosis. Clin. Sci. 2000, 98, 521–529. [Google Scholar]
- Glowińska-Olszewska, B.; Bossowski, A.; Dobreńko, E.; Hryniewicz, A.; Konstantynowicz, J.; Milewski, R.; Luczyński, W.; Piotrowska-Jastrzębska, J.; Kowal-Bielecka, O. Subclinical cardiovascular system changes in obese patients with juvenile idiopathic arthritis. Mediators Inflamm. 2013, 2013, 436702. [Google Scholar] [CrossRef] [PubMed]
- Gualtierotti, R.; Ingegnoli, F.; Griffini, S.; Grovetti, E.; Borghi, M.O.; Bucciarelli, P.; Meroni, P.L.; Cugno, M. Detection of early endothelial damage in patients with Raynaud’s phenomenon. Microvasc. Res. 2017, 113, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Valentini, G.; Marcoccia, A.; Cuomo, G.; Vettori, S.; Iudici, M.; Bondanini, F.; Santoriello, C.; Ciani, A.; Cozzolino, D.; De Matteis, G.M.; et al. Early systemic sclerosis: Marker autoantibodies and videocapillaroscopy patterns are each associated with distinct clinical, functional and cellular activation markers. Arthritis Res. Ther. 2013, 15, R63. [Google Scholar] [CrossRef]
- Ciolkiewicz, M.; Kuryliszyn-Moskal, A.; Klimiuk, P.A. Analysis of correlations between selected endothelial cell activation markers, disease activity, and nailfold capillaroscopy microvascular changes in systemic lupus erythematosus patients. Clin. Rheumatol. 2010, 29, 175. [Google Scholar] [CrossRef]
- Yamane, K.; Ihn, H.; Kubo, M.; Yazawa, N.; Kikuchi, K.; Soma, Y.; Tamaki, K. Increased serum levels of soluble vascular cell adhesion molecule 1 and E-selectin in patients with localized scleroderma. J. Am. Acad. Dermatol. 2000, 42, 64–69. [Google Scholar] [CrossRef]
- Nielen, M.M.; Van Schaardenburg, D.; Reesink, H.W.; Twisk, J.W.; Van De Stadt, R.J.; Van Der Horst-Bruinsma, I.E.; De Gast, T.; Habibuw, M.R.; Vandenbroucke, J.P.; Dijkmans, B.A. Increased levels of C-reactive protein in serum from blood donors before the onset of rheumatoid arthritis. Arthritis Rheum. 2004, 50, 2423–2427. [Google Scholar] [CrossRef] [Green Version]
- Schiopu, E.; Au, K.M.; McMahon, M.A.; Kaplan, M.J.; Divekar, A.; Singh, R.R.; Furst, D.E.; Clements, P.J.; Ragvendra, N.; Zhao, W. Prevalence of subclinical atherosclerosis is increased in systemic sclerosis and is associated with serum proteins: A cross-sectional, controlled study of carotid ultrasound. Rheumatology 2013, 53, 704–713. [Google Scholar] [CrossRef]
- Dalbeni, A.; Giollo, A.; Tagetti, A.; Atanasio, S.; Orsolini, G.; Cioffi, G.; Ognibeni, F.; Rossini, M.; Minuz, P.; Fava, C. Traditional cardiovascular risk factors or inflammation: Which factors accelerate atherosclerosis in arthritis patients? Int. J. Cardiol. 2017, 236, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Gorska, A.; Kowal-Bielecka, O.; Urban, M.; Chlabicz, S.; Sienkiewicz, J.; Gorski, S. Impairment of microcirculation in juvenile idiopathic arthritis-studies by nailfold videocapillaroscopy and correlation with serum levels of sICAM and VEGF. Folia Histochem. Cytobiol. 2008, 46, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Mueller, M.; Gschwandtner, M.E.; Gamper, J.; Giurgea, G.-A.; Kiener, H.P.; Perkmann, T.; Koppensteiner, R.; Schlager, O. Chronic inflammation predicts long-term mortality in patients with Raynaud’s phenomenon. J. Intern. Med. 2018, 283, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Górska, A.; Bartnicka, M.; Rutkowska-Sak, L. Value of nailfold videocapillaroscopy and high-sensitivity C-reactive protein test in diagnosis of microangiopathy in adolescents with Raynaud’s phenomenon. Reumatologia/Rheumatology 2013, 51, 189–194. [Google Scholar] [CrossRef]
- Koenig, M.; Joyal, F.; Fritzler, M.J.; Roussin, A.; Abrahamowicz, M.; Boire, G.; Goulet, J.-R.; Rich, E.; Grodzicky, T.; Raymond, Y.; et al. Autoantibodies and microvascular damage are independent predictive factors for the progression of Raynaud’s phenomenon to systemic sclerosis: A twenty-year prospective study of 586 patients, with validation of proposed criteria for early systemic sclerosis. Arthritis Rheum. 2008, 58, 3902–3912. [Google Scholar] [CrossRef] [PubMed]
- Narshi, C.B.; Giles, I.P.; Rahman, A. The endothelium: An interface between autoimmunity and atherosclerosis in systemic lupus erythematosus? Lupus 2011, 20, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Viikari, J.S.A.; Rönnemaa, T.; Taittonen, L.; Marniemi, J.; Raitakari, O.T. Childhood C-reactive protein in predicting CRP and carotid intima-media thickness in adulthood: The Cardiovascular Risk in Young Finns Study. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 1883–1888. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gay, M.A.; Gonzalez-Juanatey, C.; Piñeiro, A.; Garcia-Porrua, C.; Testa, A.; Llorca, J. High-grade C-reactive protein elevation correlates with accelerated atherogenesis in patients with rheumatoid arthritis. J. Rheumatol. 2005, 32, 1219–1223. [Google Scholar]
- Haak, T.; März, W.; Jungmann, E.; Hausser, S.; Siekmeier, R.; Gross, W.; Usadel, K.H. Elevated endothelin levels in patients with hyperlipoproteinemia. Clin. Investig. 1994, 72, 580–584. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Capillary Parameters | Group with RP n = 66 | Control Group n = 20 | Chi-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Reduced number of capillaries (≤6/mm linear) | 16 | 24.24 | 0 | 0.00 | p = 0.015 |
| Irregular arrangement | 40 | 66.67 | 0 | 0.00 | p < 0.001 |
| Tortuous capillaries | 23 | 34.85 | 7 | 35.00 | NS |
| Meandering capillaries | 33 | 50.00 | 4 | 20.00 | p = 0.018 |
| Avascular areas | 11 | 16.67 | 0 | 0.00 | NS |
| Giant capillaries | 36 | 54.55 | 0 | 0.00 | p = 0.008 |
| Hemorrhages | 13 | 19.70 | 0 | 0.00 | p = 0.031 |
| Spastic loops | 16 | 24.24 | 5 | 25.00 | NS |
| Neoangiogenesis | 5 | 7.58 | 0 | 0.00 | p = 0.205 |
| Capillaroscopic Parameters | Male n = 21 | Female n = 45 | Ch-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Reduced number of capillaries (<6/mm) | 4 | 19.08 | 12 | 18.18 | NS |
| Irregular arrangement | 11 | 52.38 | 29 | 64.44 | NS |
| Tortuous capillaries | 6 | 28.57 | 17 | 37.78 | NS |
| Meandering capillaries | 6 | 28.57 | 27 | 60.00 | p = 0.017 |
| Avascular areas | 4 | 19.05 | 7 | 15.56 | NS |
| Giant capillaries | 7 | 33.33 | 29 | 64.44 | p = 0.018 |
| Microhemorrhages | 5 | 23.81 | 8 | 17.78 | NS |
| Spastic loops | 5 | 23.81 | 11 | 24.44 | NS |
| Neoangiogenesis | 3 | 10.90 | 2 | 4.28 | p < 0.001 |
| Capillaroscopic Parameters | Age ≤ 15 Years n = 13 | Age >15 Years n = 53 | Chi-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Reduced number of capillaries (<6/mm) | 3 | 23.08 | 13 | 24.53 | NS |
| Irregular arrangement | 4 | 30.77 | 36 | 67.92 | p =0.014 |
| Tortuous capillaries | 1 | 7.70 | 22 | 41.51 | p = 0.022 |
| Meandering capillaries | 2 | 15.38 | 31 | 58.49 | p = 0.005 |
| Avascular areas | 3 | 23.08 | 8 | 15.09 | NS |
| Giant capillaries | 3 | 23.08 | 33 | 62.26 | p = 0.011 |
| Microhemorrhages | 4 | 30.77 | 9 | 16.98 | NS |
| Spastic loops | 4 | 30.77 | 12 | 22.64 | NS |
| Neoangiogenesis | 1 | 7.70 | 4 | 7.55 | NS |
| Capillaroscopic Parameters | Group with sRP n = 32 | Control Group n = 20 | Chi-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Reduced number of capillaries (≤6/mm) | 12 | 37.50 | 0 | 0.00 | p = 0.002 |
| Irregular arrangement | 22 | 67.58 | 0 | 0.00 | p < 0.001 |
| Tortuous capillaries | 12 | 37.50 | 7 | 35.00 | NS |
| Meandering capillaries | 12 | 37.50 | 2 | 10 | p = 0.030 |
| Giant capillaries | 17 | 53.13 | 0 | 0.00 | p < 0.001 |
| Microhemorrhages | 8 | 25.00 | 0 | 0.00 | p = 0.015 |
| Avascular areas | 11 | 34.38 | 0 | 0.00 | p = 0.003 |
| Spastic loops | 9 | 24.24 | 5 | 25.00 | NS |
| Neoangiogenesis | 3 | 9.38 | 0 | 0.00 | NS |
| Capillaroscopic Parameters | Group with uRP n = 34 | Control Group n = 20 | Chi-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Reduced number of capillaries (≤6/mm) | 4 | 11.76 | 0 | 0.00 | NS |
| Irregular arrangement | 18 | 52.94 | 0 | 0.00 | p < 0001 |
| Tortuous capillaries | 11 | 32.35 | 7 | 35.00 | NS |
| Meandering capillaries | 10 | 29.41 | 3 | 15.00 | NS |
| Avascular areas | 0 | 0.00 | 0 | 0.00 | - |
| Giant capillaries | 19 | 55.88 | 0 | 0.00 | p < 0.001 |
| Microhemorrhages | 5 | 14.71 | 0 | 0.00 | NS |
| Spastic loops | 7 | 20.59 | 5 | 25.00 | NS |
| Neoangiogenesis | 2 | 5.88 | 0 | 0.00 | NS |
| Feature/Parameter | Group with uRP (n = 34) Mean ± SD | Group with sRP (n = 32) Mean ± SD | Control Group (n = 20) Mean ± SD | ANOVA Kruskal-Wallis Test |
|---|---|---|---|---|
| Age, years | 13.07 ± 3.85 | 15.29 ± 4.52 | 14.73 ± 3.10 | NS |
| RP duration, years | 4.63 ± 2.34 | 5.74 ± 4.25 | - | NS |
| hsCRP, mg/dL | 0.42 ± 0.43 | 0.59 ± 0.51 | 0.078 ± 0.03 | p < 0.001 |
| Endothelin-1, pg/mL | 4.67 ± 3.38 | 5.74 ± 3,74 | 2.14 ± 0.6 | p = 0.0134 |
| sE-selectin, ng/mL | 39.06 ± 10.98 | 47.51 ± 16.96 | 20.92 ± 5.87 | p < 0.001 |
| Total cholesterol, mg/dL | 159.62 ± 25.17 | 163.25 ± 27.12 | 143.4 ± 20.58 | NS |
| TG, mg/dL | 70.29 ± 25.52 | 73.19 ± 40.31 | 83.2 ± 22.95 | NS |
| LDL, mg/dL | 85.11 ± 20.55 | 85.13 ± 21.02 | 81.52 ± 17.25 | NS |
| HDL, mg/dL | 60.41 ± 14.15 | 63.66 ± 15.52 | 78.54 ± 18.35 | p = 0.001 |
| Biochemical Parameters | Male n = 21 | Female n = 45 | Chi-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Total cholesterol > 180 mg/dL | 1 | 4.76 | 7 | 15.56 | NS |
| LDL cholesterol > 115 mg/dL | 14 | 66.67 | 16 | 35.56 | p = 0.018 |
| HDL cholesterol ≤ 48 mg/dL | 15 | 71.43 | 27 | 60.00 | NS |
| Triglicerides > 110 mg/dL | 5 | 23.81 | 18 | 40.00 | NS |
| hsCRP ≥ 0.5 mg/dL | 6 | 28.57 | 27 | 60.00 | p = 0.017 |
| sEselectin ≥ 40 ng/mL | 15 | 71.43 | 17 | 37.78 | p = 0.011 |
| Endothelin-1 ≥ 2.5 pg/mL | 13 | 61.19 | 31 | 68.89 | NS |
| Biochemical Parameters | Age ≤ 15 Years n = 13 | Age >15 Years n = 53 | Chi-Square Test | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Total cholesterol > 180 mg/dL | 2 | 15.38 | 6 | 11.32 | NS |
| LDL cholesterol > 115 mg/dL | 1 | 7.69 | 29 | 54.72 | p = 0.002 |
| HDL cholesterol ≤ 48 mg/dL | 3 | 23.08 | 39 | 73.58 | p < 0.001 |
| Triglycerides > 110 mg/dL | 1 | 7.69 | 22 | 41.51 | p = 0.022 |
| E - selectin ≥ 40 ng/mL | 7 | 53.85 | 25 | 47.17 | NS |
| Endothelin ≥ 2.5 pg/mL | 5 | 38.46 | 39 | 73.58 | p = 0.016 |
| hsCRP≥ 0.5 mg/dL | 3 | 23.08 | 30 | 56.60 | p = 0.030 |
| Variable | BETA | Standard Error BETA | p |
|---|---|---|---|
| Reduced number of capillaries (<6/mm) | 0.45 | 0.25 | 0.08 |
| Irregular arrangement | 0.03 | 0.21 | 0.88 |
| Tortuous capillaries | −0.06 | 0.15 | 0.71 |
| Meandering capillaries | 0.00 | 0.14 | 0.99 |
| Presence of avascular areas | 0.09 | 0.15 | 0.52 |
| Giant capillaries/microhemorrhages | 0.29 | 0.14 | 0.04 |
| Spastic capillaries | −0.11 | 0.13 | 0.37 |
| Neoangiogenesis | −0.08 | 0.13 | 0.55 |
| Variable | BETA | Standard Error BETA | p |
|---|---|---|---|
| Reduced number of capillaries (<6/mm) | 0.45 | 0.25 | 0.08 |
| Irregular pattern | 0.04 | 0.17 | 0.81 |
| Tortuous capillaries | −0.08 | 0.16 | 0.64 |
| Meandering capillaries | 0.29 | 0.16 | 0.07 |
| Giant capillaries/microhemorrhages | 0.20 | 0.13 | 0.03 |
| Presence of avascular areas | 0.32 | 0.14 | 0.03 |
| Spastic capillaries | −0.11 | 0.13 | 0.37 |
| Neoangiogenesis | −0.08 | 0.13 | 0.55 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorski, S.; Bartnicka, M.; Citko, A.; Żelazowska-Rutkowska, B.; Jablonski, K.; Gorska, A. Microangiopathy in Naifold Videocapillaroscopy and Its Relations to sE- Selectin, Endothelin-1, and hsCRP as Putative Endothelium Dysfunction Markers among Adolescents with Raynaud’s Phenomenon. J. Clin. Med. 2019, 8, 567. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050567
Gorski S, Bartnicka M, Citko A, Żelazowska-Rutkowska B, Jablonski K, Gorska A. Microangiopathy in Naifold Videocapillaroscopy and Its Relations to sE- Selectin, Endothelin-1, and hsCRP as Putative Endothelium Dysfunction Markers among Adolescents with Raynaud’s Phenomenon. Journal of Clinical Medicine. 2019; 8(5):567. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050567
Chicago/Turabian StyleGorski, Stanislaw, Marta Bartnicka, Anna Citko, Beata Żelazowska-Rutkowska, Konrad Jablonski, and Anna Gorska. 2019. "Microangiopathy in Naifold Videocapillaroscopy and Its Relations to sE- Selectin, Endothelin-1, and hsCRP as Putative Endothelium Dysfunction Markers among Adolescents with Raynaud’s Phenomenon" Journal of Clinical Medicine 8, no. 5: 567. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050567