May VelScope Be Deemed an Opportunistic Oral Cancer Screening by General Dentists? A Pilot Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Material and Methods
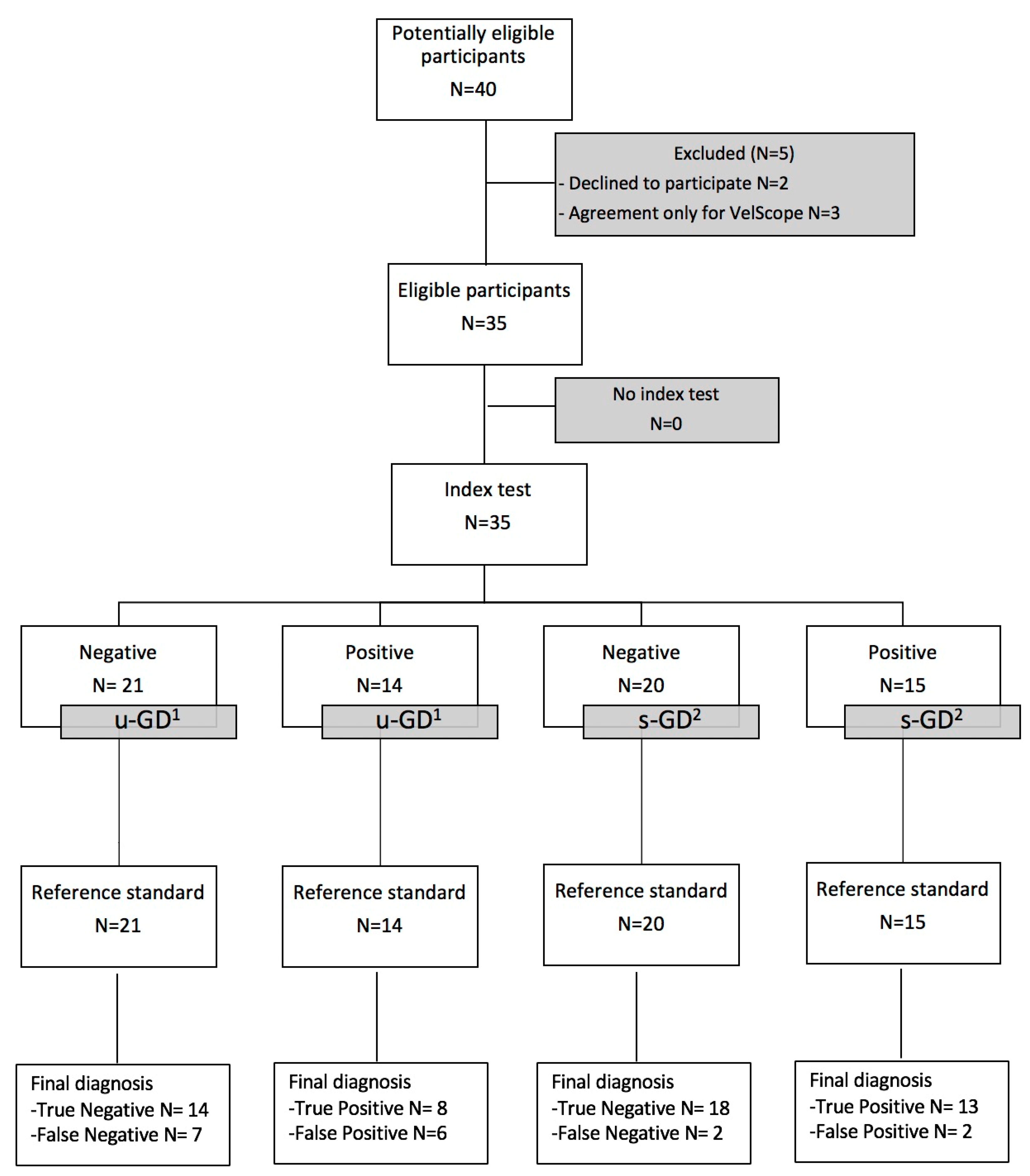
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The World Health Report 2004: Changing History; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Petersen, P.E. Oral cancer prevention and control—The approach of the World Health Organization. Oral Oncol. 2009, 45, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.B.; Güneri, P.; Boyacioglu, H.; Abt, E. The limitations of the clinical oral examination in detecting dysplastic oral lesions and oral squamous cell carcinoma. J. Am. Dent. Assoc. 2012, 143, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Nagi, R.; Reddy-Kantharaj, Y.B.; Rakesh, N.; Janardhan-Reddy, S.; Sahu, S. Efficacy of light based detection systems for early detection of oral cancer and oral potentially malignant disorders: Systematic review. Med. Oral Patol. Oral Y Cir. Bucal 2016, 21, e447–e455. [Google Scholar] [CrossRef] [PubMed]
- Farah, C.S.; McIntosh, L.; Georgiou, A.; McCullough, M.J. Efficacy of tissue autofluorescence imaging (VELScope) in the visualization of oral mucosal lesions. Head Neck 2012, 34, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Herford, A.S.; Cervino, G.; Troiano, G.; Lauritano, F.; Laino, L. Tissue fluorescence imaging (VELscope) for quick non-invasive diagnosis in oral pathology. J. Craniofac. Surg. 2017, 28, e112–e115. [Google Scholar] [CrossRef] [PubMed]
- Pavlova, I.; Williams, M.; El-Naggar, A.; Richards-Kortum, R.; Gillenwater, A. Understanding the biological basis of autofluorescence imaging for oral cancer detection: High-resolution fluorescence microscopy in viable tissue. Clin. Cancer Res. 2008, 14, 2396–2404. [Google Scholar] [CrossRef] [Green Version]
- Hashim, R.; Abo-Fanas, A.; Al-Tak, A.; Al-Kadri, A.; Abu Ebaid, Y. Early Detection of Oral Cancer-Dentists’ Knowledge and Practices in the United Arab Emirates. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 2351–2355. [Google Scholar]
- Leonel, A.C.L.D.S.; Soares, C.B.R.B.; Lisboa de Castro, J.F.; Bonan, P.R.F.; Ramos-Perez, F.M.M.; Perez, D.E.D.C. Knowledge and attitudes of primary health care dentists regarding oral cancer in brazil. Acta Stomatol. Croat. 2019, 53, 55–63. [Google Scholar] [CrossRef]
- Cicciù, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Oteri, G.; Troiano, G.; Zhurakivska, K.; Lo Muzio, L.; Herford, A.S.; Crimi, S.; et al. Early diagnosis on oral and potentially oral malignant lesions: A systematic review on the VELscope® Fluorescence method. Dent. J. (Basel) 2019, 7, 93. [Google Scholar] [CrossRef] [Green Version]
- Awan, K.H.; Morgan, P.R.; Warnakulasuriya, S. Evaluation of an autofluorescence based imaging system (VELscope™) in the detection of oral potentially malignant disorders and benign keratosis. Oral Oncol. 2011, 47, 274–277. [Google Scholar] [CrossRef]
- Hashim, D.; Genden, E.; Posner, M.; Hashibe, M.; Boffetta, P. Head and neck cancer prevention: From primary prevention to impact of clinicians on reducing burden. Ann. Oncol. 2019, 30, 744–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.A.; Andrews, K.S.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Brawley, O.W.; Wender, R.C. Cancer screening in the United States, 2018: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J. Clin. 2018, 68, 297–316. [Google Scholar] [CrossRef] [PubMed]
- Lingen, M.W.; Abt, E.; Agrawal, N.; Chaturvedi, A.K.; Cohen, E.; D’Souza, G.; Gurenlian, J.; Kalmar, J.R.; Kerr, A.R.; Lambert, P.M.; et al. Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity: A report of the American Dental Association. J. Am. Dent. Assoc. 2017, 148, 712–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mignogna, M.D.; Fedele, S. Oral cancer screening: 5 minutes to save a life. Lancet 2005, 365, 1905–1906. [Google Scholar] [CrossRef]
- Chakraborty, D.; Natarajan, C.; Mukherjee, A. Advances in oral cancer detection. Adv. Clin. Chem. 2019, 91, 181–200. [Google Scholar]
- Rashid, A.; Warnakulasuriya, S. The use of light-based (optical) detection systems as adjuncts in the detection of oral cancer and oral potentially malignant disorders: A systematic review. J. Oral Pathol. Med. 2015, 44, 307–328. [Google Scholar] [CrossRef]
- Brocklehurst, P.; Kujan, O.; O’Malley, L.A.; Ogden, G.; Shepherd, S.; Glenny, A.M. Screening programmes for the early detection and prevention of oral cancer. Cochrane Database Syst. Rev. 2013, CD004150. [Google Scholar] [CrossRef] [Green Version]
- Awan, K.H.; Patil, S. Efficacy of autofluorescence imaging as an adjunctive technique for examination and detection of oral potentially malignant disorders: A systematic review. J. Contemp. Dent. Pract. 2015, 16, 744–749. [Google Scholar] [CrossRef]
- Cânjău, S.; Todea, D.C.M.; Sinescu, C.; Pricop, M.O.; Duma, V.F. Fluorescence influence on screening decisions for oral malignant lesions. Rom. J. Morphol. Embryol. 2018, 59, 203–209. [Google Scholar]
- Tomo, S.; Miyahara, G.I.; Simonato, L.E. History and future perspectives for the use of fluorescence visualization to detect oral squamous cell carcinoma and oral potentially malignant disorders. Photodiagn. Photodyn. Ther. 2019, 28, 308–317. [Google Scholar] [CrossRef]
- Huff, K.; Stark, P.C.; Solomon, L.W. Sensitivity of direct tissue fluorescence visualization in screening for oral premalignant lesions in general practice. Gen Dent. 2009, 57, 34–38. [Google Scholar] [PubMed]
- Simonato, L.E.; Tomo, S.; Miyahara, G.I.; Navarro, R.S.; Villaverde, A.G.J.B. Fluorescence visualization efficacy for detecting oral lesions more prone to be dysplastic and potentially malignant disorders: A pilot study. Photodiagn. Photodyn. Ther. 2017, 17, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ganga, R.S.; Gundre, D.; Bansal, S.; Shirsat, P.M.; Prasad, P.; Desai, R.S. Evaluation of the diagnostic efficacy and spectrum of autofluorescence of benign, dysplastic and malignant lesions of the oral cavity using VELscope. Oral Oncol. 2017, 75, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Waknis, P.; Saha, A.; Setiya, S.; Ratra, T.; Vaswani, V. The use of Velscope to assess cellular changes occuring in oral premalignancy. J. Oral Biol. Craniofacial Res. 2020, 10, 99–103. [Google Scholar] [CrossRef]
- Leuci, S.; Aria, M.; Nicolò, M.; Spagnuolo, G.; Warnakulasuriya, K.; Mignogna, M.D. Comparison of views on the need for continuing education on oral cancer between general dentists and oral medicine experts: A Delphi survey. J. Int. Soc. Prev. Community Dent. 2016, 6, 465–473. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (%) |
|---|---|
| Age (mean year) | 58.5 |
| Gender | |
| Male | 17 (48.6%) |
| Female | 18 (51.4%) |
| Risk factor | |
| Smoking status | |
| Never | 15 (42.9%) |
| Former smoker | 7 (20%) |
| Current smoker | 13 (37.1%) |
| Alcohol use | |
| Never | 21 (60%) |
| Former drinker | 9 (25.7%) |
| Current drinker | 5 (14.3%) |
| Oral Lesions | |
| COE 1 u-GD 2 | |
| Suspected malignant lesions | 15 (42.9%) |
| Suspected benign lesions | 20 (57.1%) |
| COE 1 s-GD 3 | |
| Suspected malignant lesions | 18 (51.4%) |
| Suspected benign lesions | 17 (48.6%) |
| VEL-E 4 u-GD 2 | |
| Positive | 14 (40%) |
| Negative | 21 (60%) |
| VEL-E 4 s-GD 3 | |
| Positive | 15 (42.9%) |
| Negative | 20 (57.1%) |
| Histopathological diagnosis | |
| Benign | |
| OLP 5 | 9 (25.7%) |
| OLL 6 | 5 (14.3%) |
| Cheratotic lesion | 2 (5.7%) |
| OL 7 | 4 (11.4%) |
| Malignant | |
| Erythroplakia | 4 (11.4%) |
| CIS 8 | 3 (8.6%) |
| OSCC 9 | 6 (17.1%) |
| Verrucous carcinoma | 2 (5.7%) |
| u-GD 1 (COE 2) | u-GD 1 (Vel-E 3) | s-GD 4 (COE 2) | s-GD 4 (Vel-E 3) | |
|---|---|---|---|---|
| Sensitivity | 53.3% (26.59–78.73%) | 53.3% (26.59–78.73%) | 73.3% (44.90–92.21%) | 86.7% (59.54–98.34%) |
| specificity | 65% (40.78–84.61%) | 70% (45.72–88.11%) | 65% (40.78–84.61%) | 90% (68.30–98.77%) |
| ppv 5 | 53.3% (34.78–71.01%) | 57.1% (37.00–75.17%) | 61.1% (44.55–75.45%) | 86.7% (63.23–96.09%) |
| npv 6 | 76.5% (49.74–77.70%) | 66.7% (52.02–78.68%) | 76.5% (56.95–88.87%) | 90% (71.07–97.06%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leuci, S.; Coppola, N.; Turkina, A.; Bizzoca, M.E.; Favia, G.; Spagnuolo, G.; Mignogna, M.D. May VelScope Be Deemed an Opportunistic Oral Cancer Screening by General Dentists? A Pilot Study. J. Clin. Med. 2020, 9, 1754. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061754
Leuci S, Coppola N, Turkina A, Bizzoca ME, Favia G, Spagnuolo G, Mignogna MD. May VelScope Be Deemed an Opportunistic Oral Cancer Screening by General Dentists? A Pilot Study. Journal of Clinical Medicine. 2020; 9(6):1754. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061754
Chicago/Turabian StyleLeuci, Stefania, Noemi Coppola, Anna Turkina, Maria Eleonora Bizzoca, Gianfranco Favia, Gianrico Spagnuolo, and Michele Davide Mignogna. 2020. "May VelScope Be Deemed an Opportunistic Oral Cancer Screening by General Dentists? A Pilot Study" Journal of Clinical Medicine 9, no. 6: 1754. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061754