Pain Trajectories in Knee Osteoarthritis—A Systematic Review and Best Evidence Synthesis on Pain Predictors

 ,
,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search
2.5. Study Selection
2.6. Data Collection Process
2.7. Data Items
2.8. Risk of Bias in Individual Studies
2.9. Summary Measures
2.10. Synthesis of Results
2.11. Risk of Bias Across Studies
3. Results
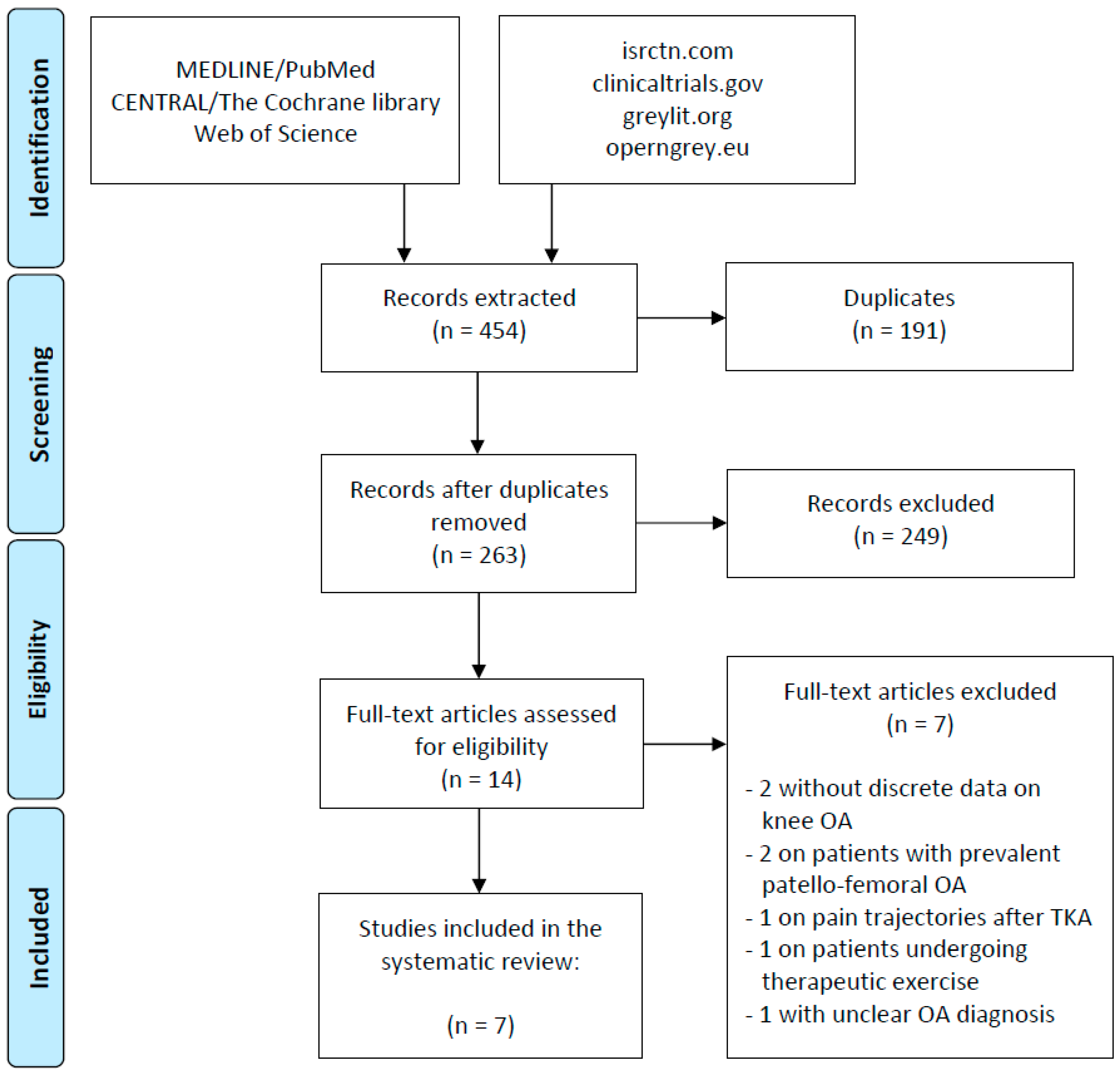
3.1. Article Selection and Characteristics
3.2. Characteristics of Pain Trajectories in Knee OA Patients
3.3. Risk of Bias of the Included Studies
3.4. Best Evidence Synthesis of the Predictors of Pain Trajectories
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Bartlett, S.J.; Ling, S.M.; Mayo, N.E.; Scott, S.C.; Bingham, C.O., 3rd. Identifying common trajectories of joint space narrowing over two years in knee osteoarthritis. Arthritis Care Res. (Hoboken) 2011, 63, 1722–1728. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.E.; Katz, J.N.; Dervan, E.E.; Losina, E. Trajectories and risk profiles of pain in persons with radiographic, symptomatic knee osteoarthritis: Data from the osteoarthritis initiative. Osteoarthr. Cartil. 2014, 22, 622–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, U.S.; Zhang, Y.; Zhu, Y.; Niu, J.; Zhang, B.; Felson, D.T. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: Survey and cohort data. Ann. Intern. Med. 2011, 155, 725–732. [Google Scholar] [CrossRef]
- Peat, G.; McCarney, R.; Croft, P. Knee pain and osteoarthritis in older adults: A review of community burden and current use of primary health care. Ann. Rheum. Dis. 2001, 60, 91–97. [Google Scholar] [CrossRef]
- Zhang, W.; Robertson, J.; Jones, A.C.; Dieppe, P.A.; Doherty, M. The placebo effect and its determinants in osteoarthritis: Meta-analysis of randomised controlled trials. Ann. Rheum. Dis. 2008, 67, 1716–1723. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Longo, U.G.; Madry, H.; Marchettini, P.; Marmotti, A.; Van Assche, D.; Zanon, G.; Peretti, G.M. Non-surgical treatments for the management of early osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1775–1785. [Google Scholar] [CrossRef]
- Filardo, G.; Previtali, D.; Napoli, F.; Candrian, C.; Zaffagnini, S.; Grassi, A. PRP Injections for the Treatment of Knee Osteoarthritis: A Meta-Analysis of Randomized Controlled Trials. Cartilage 2020. [Google Scholar] [CrossRef]
- De Girolamo, L.; Kon, E.; Filardo, G.; Marmotti, A.G.; Soler, F.; Peretti, G.M.; Vannini, F.; Madry, H.; Chubinskaya, S. Regenerative approaches for the treatment of early OA. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1826–1835. [Google Scholar] [CrossRef]
- Vannini, F.; Spalding, T.; Andriolo, L.; Berruto, M.; Denti, M.; Espregueira-Mendes, J.; Menetrey, J.; Peretti, G.M.; Seil, R.; Filardo, G. Sport and early osteoarthritis: The role of sport in aetiology, progression and treatment of knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1786–1796. [Google Scholar] [CrossRef]
- Felson, D.; Niu, J.; Sack, B.; Aliabadi, P.; McCullough, C.; Nevitt, M.C. Progression of osteoarthritis as a state of inertia. Ann. Rheum. Dis. 2013, 72, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Croft, P.; Porcheret, M.; Peat, G. Managing osteoarthritis in primary care: The GP as public health physician and surgical gatekeeper. Br. J. Gen. Pract. 2011, 61, 485–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losina, E.; Weinstein, A.M.; Reichmann, W.M.; Burbine, S.A.; Solomon, D.H.; Daigle, M.E.; Rome, B.N.; Chen, S.P.; Hunter, D.J.; Suter, L.G.; et al. Lifetime risk and age at diagnosis of symptomatic knee osteoarthritis in the US. Arthritis Care Res. (Hoboken) 2013, 65, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Li, C.S.; Karlsson, J.; Winemaker, M.; Sancheti, P.; Bhandari, M. Orthopedic surgeons feel that there is a treatment gap in management of early OA: International survey. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 363–378. [Google Scholar] [CrossRef] [PubMed]
- Arias-Vazquez, P.I.; Tovilla-Zarate, C.A.; Legorreta-Ramirez, B.G.; Burad Fonz, W.; Magana-Ricardez, D.; Gonzalez-Castro, T.B.; Juarez-Rojop, I.E.; Lopez-Narvaez, M.L. Prolotherapy for knee osteoarthritis using hypertonic dextrose vs other interventional treatments: Systematic review of clinical trials. Adv. Rheumatol. 2019, 59, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohmander, L.S.; Roos, E.M. Disease modification in OA—Will we ever get there? Nat. Rev. Rheumatol. 2019, 15, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, M.; Felson, D.; Lester, G. The osteoarthritis initiative: Protocol for the Cohort Study. OARSI J. 2006. [Google Scholar]
- Jung, T.; Wickrama, K.A. An introduction to latent class growth analysis and growth mixture modeling. Soc. Personal. Psychol. Compass 2008, 2, 302–317. [Google Scholar] [CrossRef]
- Losina, E.; Collins, J.E. Forecasting the future pain in hip OA: Can we rely on pain trajectories? Osteoarthr. Cartil. 2016, 24, 765–767. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Chapter 7: Selecting studies and collecting data. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons Ltd: The Atrium, UK, 2011. [Google Scholar]
- Ioannidis, J.P.; Patsopoulos, N.A.; Rothstein, H.R. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ 2008, 336, 1413–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slavin, R.E. Best evidence synthesis: An intelligent alternative to meta-analysis. J. Clin. Epidemiol. 1995, 48, 9–18. [Google Scholar] [CrossRef]
- van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eijgenraam, S.M.; Reijman, M.; Bierma-Zeinstra, S.M.A.; van Yperen, D.T.; Meuffels, D.E. Can we predict the clinical outcome of arthroscopic partial meniscectomy? A systematic review. Br. J. Sports Med. 2018, 52, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, Z.; Lu, N.; Niu, J.; Felson, D.T.; Zhang, Y. Dietary Fiber Intake in Relation to Knee Pain Trajectory. Arthritis Care Res. (Hoboken) 2017, 69, 1331–1339. [Google Scholar] [CrossRef]
- Halilaj, E.; Le, Y.; Hicks, J.L.; Hastie, T.J.; Delp, S.L. Modeling and predicting osteoarthritis progression: Data from the osteoarthritis initiative. Osteoarthr. Cartil. 2018, 26, 1643–1650. [Google Scholar] [CrossRef] [Green Version]
- Bastick, A.N.; Wesseling, J.; Damen, J.; Verkleij, S.P.; Emans, P.J.; Bindels, P.J.; Bierma-Zeinstra, S.M. Defining knee pain trajectories in early symptomatic knee osteoarthritis in primary care: 5-year results from a nationwide prospective cohort study (CHECK). Br. J. Gen. Pract. 2016, 66, e32–e39. [Google Scholar] [CrossRef] [Green Version]
- Wesseling, J.; Bastick, A.N.; Ten Wolde, S.; Kloppenburg, M.; Lafeber, F.P.; Bierma-Zeinstra, S.M.; Bijlsma, J.W. Identifying Trajectories of Pain Severity in Early Symptomatic Knee Osteoarthritis: A 5-year Followup of the Cohort Hip and Cohort Knee (CHECK) Study. J. Rheumatol. 2015, 42, 1470–1477. [Google Scholar] [CrossRef]
- Nicholls, E.; Thomas, E.; van der Windt, D.A.; Croft, P.R.; Peat, G. Pain trajectory groups in persons with, or at high risk of, knee osteoarthritis: Findings from the Knee Clinical Assessment Study and the Osteoarthritis Initiative. Osteoarthr. Cartil. 2014, 22, 2041–2050. [Google Scholar] [CrossRef] [Green Version]
- Trouvin, A.P.; Marty, M.; Goupille, P.; Perrot, S. Determinants of daily pain trajectories and relationship with pain acceptability in hip and knee osteoarthritis. A national prospective cohort study on 886 patients. Jt. Bone Spine 2019, 86, 245–250. [Google Scholar] [CrossRef]
- Luyten, F.P.; Denti, M.; Filardo, G.; Kon, E.; Engebretsen, L. Definition and classification of early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madry, H.; Kon, E.; Condello, V.; Peretti, G.M.; Steinwachs, M.; Seil, R.; Berruto, M.; Engebretsen, L.; Filardo, G.; Angele, P. Early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Deveza, L.A.; Melo, L.; Yamato, T.P.; Mills, K.; Ravi, V.; Hunter, D.J. Knee osteoarthritis phenotypes and their relevance for outcomes: A systematic review. Osteoarthr. Cartil. 2017, 25, 1926–1941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, W.W., 3rd; Saleh, K.J.; Wilt, T.J.; Kane, R.L. Agreement about indications for total knee arthroplasty. Clin. Orthop. Relat. Res. 2006, 446, 34–39. [Google Scholar] [CrossRef]
- Jain, N.B.; Higgins, L.D.; Ozumba, D.; Guller, U.; Cronin, M.; Pietrobon, R.; Katz, J.N. Trends in epidemiology of knee arthroplasty in the United States, 1990–2000. Arthritis Rheum. 2005, 52, 3928–3933. [Google Scholar] [CrossRef]
- Roemer, F.W.; Kwoh, C.K.; Hannon, M.J.; Hunter, D.J.; Eckstein, F.; Fujii, T.; Boudreau, R.M.; Guermazi, A. What comes first? Multitissue involvement leading to radiographic osteoarthritis: Magnetic resonance imaging-based trajectory analysis over four years in the osteoarthritis initiative. Arthritis Rheumatol. 2015, 67, 2085–2096. [Google Scholar] [CrossRef] [Green Version]
- Scott, C.E.; Oliver, W.M.; MacDonald, D.; Wade, F.A.; Moran, M.; Breusch, S.J. Predicting dissatisfaction following total knee arthroplasty in patients under 55 years of age. Bone Jt. J. 2016, 98, 1625–1634. [Google Scholar] [CrossRef]
- Hawker, G.A.; Badley, E.M.; Borkhoff, C.M.; Croxford, R.; Davis, A.M.; Dunn, S.; Gignac, M.A.; Jaglal, S.B.; Kreder, H.J.; Sale, J.E. Which patients are most likely to benefit from total joint arthroplasty? Arthritis Rheum. 2013, 65, 1243–1252. [Google Scholar] [CrossRef]
- Jones, L.D.; Bottomley, N.; Harris, K.; Jackson, W.; Price, A.J.; Beard, D.J. The clinical symptom profile of early radiographic knee arthritis: A pain and function comparison with advanced disease. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 161–168. [Google Scholar] [CrossRef]
- Baert, I.A.; Staes, F.; Truijen, S.; Mahmoudian, A.; Noppe, N.; Vanderschueren, G.; Luyten, F.P.; Verschueren, S.M. Weak associations between structural changes on MRI and symptoms, function and muscle strength in relation to knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2013–2025. [Google Scholar] [CrossRef] [Green Version]
- Han, H.S.; Lee, J.Y.; Kang, S.B.; Chang, C.B. The relationship between the presence of depressive symptoms and the severity of self-reported knee pain in the middle aged and elderly. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1634–1642. [Google Scholar] [CrossRef] [PubMed]
- Creamer, P.; Hochberg, M.C. The relationship between psychosocial variables and pain reporting in osteoarthritis of the knee. Arthritis Care Res. 1998, 11, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.A.; Gould, R.; Reuben, D.B.; Greendale, G.A.; Carter, M.K.; Zhou, K.; Karlamangla, A. Longitudinal patterns and predictors of alcohol consumption in the United States. Am. J. Public Health 2005, 95, 458–465. [Google Scholar] [CrossRef]
- Giskes, K.; Kunst, A.E.; Benach, J.; Borrell, C.; Costa, G.; Dahl, E.; Dalstra, J.A.; Federico, B.; Helmert, U.; Judge, K.; et al. Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J. Epidemiol. Community Health 2005, 59, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Carlesso, L.C.; Segal, N.A.; Frey-Law, L.; Zhang, Y.; Na, L.; Nevitt, M.; Lewis, C.E.; Neogi, T. Pain Susceptibility Phenotypes in Those Free of Knee Pain with or at Risk of Knee Osteoarthritis: The Multicenter Osteoarthritis Study. Arthritis Rheumatol. 2019, 71, 542–549. [Google Scholar] [CrossRef]
- Hunter, D.J.; Niu, J.; Zhang, Y.; Nevitt, M.C.; Xu, L.; Lui, L.Y.; Yu, W.; Aliabadi, P.; Buchanan, T.S.; Felson, D.T. Knee height, knee pain, and knee osteoarthritis: The Beijing Osteoarthritis Study. Arthritis Rheum. 2005, 52, 1418–1423. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Han, K.; McAlindon, T.E.; Park, Y.G.; Park, S.H. Lower leg muscle mass relates to knee pain in patients with knee osteoarthritis. Int. J. Rheum. Dis. 2018, 21, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Baron, E.; Bass, J.; Murray, S.M.; Schneider, M.; Lund, C. A systematic review of growth curve mixture modelling literature investigating trajectories of perinatal depressive symptoms and associated risk factors. J. Affect. Disord. 2017, 223, 194–208. [Google Scholar] [CrossRef] [PubMed]
- Berlin, K.S.; Parra, G.R.; Williams, N.A. An introduction to latent variable mixture modeling (part 2): Longitudinal latent class growth analysis and growth mixture models. J. Pediatr. Psychol. 2014, 39, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Musliner, K.L.; Munk-Olsen, T.; Eaton, W.W.; Zandi, P.P. Heterogeneity in long-term trajectories of depressive symptoms: Patterns, predictors and outcomes. J. Affect. Disord. 2016, 192, 199–211. [Google Scholar] [CrossRef] [Green Version]
- Stone, A.A.; Schwartz, J.E.; Broderick, J.E.; Shiffman, S.S. Variability of momentary pain predicts recall of weekly pain: A consequence of the peak (or salience) memory heuristic. Pers. Soc. Psychol. Bull. 2005, 31, 1340–1346. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies including patients with symptomatic knee OA | Studies on patients treated with TKA or other surgical and non-surgical treatments |
| Studies assessing pain evolution over time with pain trajectories in patients without treatment | No information on pain evolution or discrete data for patients with knee OA |
| Level of evidence I–IV | Expert opinions (level of evidence V), reviews, systematic reviews and meta-analyses |
| Published in English | Preclinical or ex vivo studies |
| Study | Origin of Data | Included Patients | Patients at Follow-Up | Age (Mean ± SD) | Females (%) | BMI (Mean ± SD) | Follow-Up Length | Baseline KL Grade | Pain Score Used |
|---|---|---|---|---|---|---|---|---|---|
| Bastick et al., 2016 [28] | CHECK database | 743 | 705 | 56 ± 5.1 | 81 | 26.5 ± 4.3 | 5 y | 58% grade 0, 42% grade 1 | NRS 0–10 |
| Collins et al., 2014 [3] | Osteoarthritis Initiative | 1753 | 1448 | 62.2 ± 8.9 | 59 | 30.1 ± 4.9 | 6 y | 52% grade 2, 34% grade 3, 14% grade 4 | WOMAC pain 0–100 |
| Dai et al., 2017 [26] | Osteoarthritis Initiative | 1852 | 1852 | 61.3 ± 9.1 | 58 | NR | 8 y | 56% grade 0–1, 44% grade 2–4 | WOMAC pain 0–20 |
| Halilaj et al., 2018 [27] | Osteoarthritis Initiative | 1243 | 1243 | 62.1 ± 8.8 | 63 | 29 ± 4.8 | 6 y | 100% grade 0–1 | WOMAC pain 0–20 |
| Nicholls et al., 2014 [30] | CAS-K | 819 | 570 | 64 ± 8 | 54 | 29.5 ± 5 | 6 y | 54% grade 0, 9% grade 1, 14% grade 2, 12% grade 3, 10% grade 4 | WOMAC pain (0–20) |
| Trouvin et al., 2018 [31] | French GPs | 632 | 632 | 67.5 ± 9.4 | 58 | 27.9 ± 4.6 | 28 d | NR | NRS 0–10 |
| Wesseling et al., 2015 [29] | CHECK database | 705 | 705 | 56 ± 5.1 | 81 | 26.5 ± 4.3 | 5 y | 61% grade 0, 39% grade 1 | NRS 0–10 |
| Predictor | Number of Studies | Significant Predictor | Non-Significant Predictor | Best Evidence Synthesis |
|---|---|---|---|---|
| Education level | 4 | L L M M | Strong | |
| Comorbidities | 4 | L L M M | Strong | |
| Younger age | 5 | M | L L M M | Strong |
| Alcohol | 2 | L L | Strong | |
| Smoking | 2 | L L | Strong | |
| Depression | 2 | M M | Moderate | |
| Pain medication | 3 | L M M | Moderate | |
| Coping (others) | 2 | L L | Moderate | |
| Diet fibres | 1 | H | Limited | |
| Physical activity | 1 | M | Limited | |
| Diet: meat/diary | 1 | M | Limited | |
| Supplementary Vitamins | 1 | L | Limited | |
| BMI | 5 | L L M | M M | Conflicting |
| Female sex | 5 | M M | L M M | Conflicting |
| Pain ipsilateral hip | 2 | L | L | Conflicting |
| Black ethnicity | 2 | M | L | Conflicting |
| Coping (worrying) | 2 | L | L | Conflicting |
| Predictor | Number of Studies | Significant Predictor | Non-Significant Predictor | Best Evidence Synthesis |
|---|---|---|---|---|
| Knee tenderness | 1 | L | Limited | |
| Joint space width | 1 | M | Limited | |
| Knee warmth | 1 | L | Limited | |
| Bony enlargement | 1 | L | Limited | |
| Crepitus | 1 | L | Limited | |
| Positive re-fill test | 1 | L | Limited | |
| ROM flexion | 1 | L | Limited | |
| ROM extension | 1 | L | Limited | |
| Pain in motion | 1 | L | Limited | |
| Bouchard | 1 | L | Limited | |
| Heberden | 1 | L | Limited | |
| ESR | 1 | L | Limited | |
| Knee alignment | 1 | M | Limited | |
| Problems duration | 1 | M | Limited | |
| Baseline pain | 1 | L | Limited | |
| WOMAC, stiffness | 1 | L | Limited | |
| K-L | 4 | M M | L L | Conflicting |
| WOMAC, pain | 2 | H | L | Conflicting |
| WOMAC, function | 2 | H | L | Conflicting |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Previtali, D.; Andriolo, L.; Di Laura Frattura, G.; Boffa, A.; Candrian, C.; Zaffagnini, S.; Filardo, G. Pain Trajectories in Knee Osteoarthritis—A Systematic Review and Best Evidence Synthesis on Pain Predictors. J. Clin. Med. 2020, 9, 2828. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092828
Previtali D, Andriolo L, Di Laura Frattura G, Boffa A, Candrian C, Zaffagnini S, Filardo G. Pain Trajectories in Knee Osteoarthritis—A Systematic Review and Best Evidence Synthesis on Pain Predictors. Journal of Clinical Medicine. 2020; 9(9):2828. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092828
Chicago/Turabian StylePrevitali, Davide, Luca Andriolo, Giorgio Di Laura Frattura, Angelo Boffa, Christian Candrian, Stefano Zaffagnini, and Giuseppe Filardo. 2020. "Pain Trajectories in Knee Osteoarthritis—A Systematic Review and Best Evidence Synthesis on Pain Predictors" Journal of Clinical Medicine 9, no. 9: 2828. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092828