
Platinum-Based Nanoformulations for Glioblastoma Treatment: The Resurgence of Platinum Drugs?
 ,
,  ,
,
Abstract
:1. Introduction
2. Current Landscape for GB Treatment
3. Platinum and Glioblastoma: State-of-the-Art
4. Platinum-Based Drugs Limitations and Opportunities
4.1. Factors Related to Brain Uptake
4.2. Narrow Therapeutic Window
4.3. Inappropriate Dosing Schedule
4.4. Extensive Off-Target Toxicity
4.5. Sequestering/Deactivating Reactions
5. Platinum-Based Drugs Limitations and Opportunities
5.1. Cisplatin
5.2. Carboplatin
5.3. Oxaliplatin
5.4. Pt(IV) Prodrugs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt Agent | Nanocarrier & Size | Form | Cells/Animal Models (Administration Mode) | Effect/Mechanism of Action | Ref. |
|---|---|---|---|---|---|
| Cisplatin | Iron oxide NPs in NGO (lateral width of 80–100 nm and thickness of 6.3 nm) | γ-Fe2O3 NPs coated by nanographene oxide (NGO) containing cisplatin | U87 cell line | Superparamagnetic-like behavior but showed little cytotoxicity at 10 μM. | [159] |
| Cisplatin | Au-NPs (7 nm) | Cisplatin conjugated to gold NPs | U251/U87 cell lines, U251 xenografts (intravenous injection) | Inhibited GB cells growth and showed marked synergy with MR-guided Focused Ultrasound (MRgFUS) therapy. In vivo assays demonstrated increased BBB permeability. | [160] |
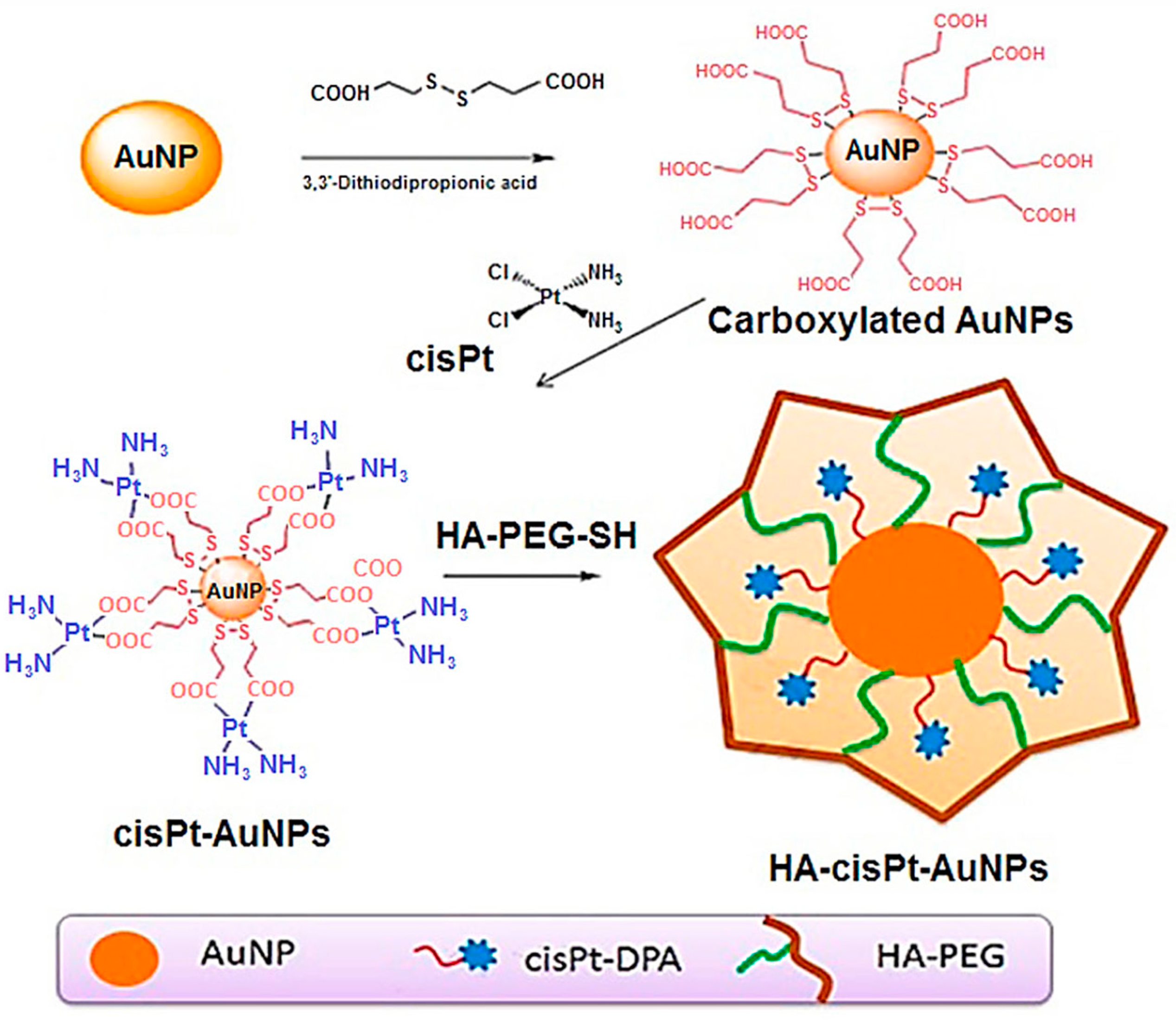
| Cisplatin | Au-NPs (145 nm) | Cisplatinum attached to hyaluronic acid-functionalized gold NPs and coated with PEG | U87 cell line MCF-7 tumour-bearing mice (intravenous injection) | NPs inhibited GB cells growth and showed marked synergy with the thermal effect of applying NIR laser radiation. | [161] |
| Cisplatin | Liposomes (50–60 nm) | LipoplatinTM and novel cisplatin bound to coordination complexes with lipid cholesteryl hemisuccinate (CHEMS) | F98 glioma cell line F98 glioma-bearing rats (convection-enhanced delivery) | Potent in vitro cytotoxicity. High intracerebral retention after CED. CHEMS liposomes were better tolerated than LipoplatinTM and showed increased survival data in vivo. | [165] |
| Cisplatin | Liposomes (130–160 nm) | Cisplatin analogue and antibodies against VEGF or VEGFR2 conjugated on liposome surface | C6, U87 cell lines | Prolonged blood circulation time in C6 glioma-bearing rats. In vitro data confirmed that conjugation with specific antibodies increases the intracellular concentration of the liposomes and improves cytotoxicity. | [167] |
| Cisplatin | Liposomes (160 nm) | Liposomes decorated with OX26 monoclonal antibodies | C6 cell line C6 glioma-bearing rats (stereotactic injection) | Increased cellular uptake and increased mean survival time in vivo with notable reduction in toxicity effects. | [168] |
| Cisplatin | Polymeric NPs (105 nm) | Protamine-functionalized PLGA NPs | U87 cell line | Increased cellular uptake and cytotoxicity in vitro and ability to cross in vitro BBB model, improving therapeutic index. | [169] |
| Cisplatin | Polymeric NPs (50–145 nm) | PLGA-PEG copolymer NPs functionalized with a triphenylphosphonium cation | C6 cell line C6 glioma-bearing rats (intravenous injection) | Nanoparticles below 100 nm diffused within mice brain if densely coated with PEG. | [170] |
| Cisplatin | Polymeric NPs (114 nm) | PLGA NPs | U87 cell line | Significantly higher cytotoxicity than cisplatin, enhanced cellular uptake. | [171] |
| Cisplatin | Polymeric NPs (490 nm) | PBCA NPs | C6 cell line C6 glioma-bearing rats (intraperitoneal injection) | Similar cytotoxicity in comparison to cisplatin. Slightly longer mean survival time and reduced side effects. | [172] |
| Cisplatin | Polymeric NPs (70 nm) | PEGylated-Poly(aspartic acid) NPs | 9L gliosarcoma and F98 glioma lines, orthotopic F98 brain tumour model (convection-enhanced delivery) | Reduction in toxicity associated with cisplatin and increased average survival in vivo. | [173] |
| Cisplatin | Polymeric NPs (9 nm) | Gd-grafted PEO micelles | U87/U251 cell lines, U87 orthotopic xenografts (stereotactic injection) | Hyperintense signal on T2-weighted MRI, 50-fold increased cellular accumulation, and 32-fold Pt-DNA adduct compared to free cisplatin. | [174] |
| Cisplatin | Nanogel (110 nm) | PEG-b-PMAA nanogels functionalized with monoclonal antibody to Cx43 | C6 cells C6 glioma-bearing rats (intravenous injection) | Targeted delivery to C6 glioma. Prolonged the mean survival time of glioma-bearing rats. | [175] |
| Cisplatin + Glutathione Peroxidase | Iron NPs (80–125 nm) | Cisplatin and small interfering RNA (siRNA) targeting glutathione peroxidase attached to IONPs and functionalized with folic acid | U87 cell line, primary glioblastoma cell line (P3#GB), normal human astrocytes (NHAs) U87orthotopic xenografts (stereotactic injection) | Potent ROS and ferroptosis, synergistically improved therapeutic efficacy, low systemic toxicity achieved both in vitro and in vivo. | [86] |
| Cisplatin + Fisetin | Liposomes (173 nm) | Both drugs incorporated to a liposomal formulation composed by DOPC/cholesterol/DODA-GLY-PEG2000 | U87 cell line | Additive effect of cisplatin and fisetin. Effective antitumoural action against GB cells. | [176] |
| Cisplatin + TMZ | Biomimetic NPs (171 nm) | pH degradable acetal grated dextran inner core coated with GB cancer cell membrane | U87 or drug-resistant U251R GB tumours (intravenous injection) | Improvement in BBB penetration and targeting of GB tissue/cells. Potent anti-GB activity in mice bearing orthotopic U87 or TMZ resistant U251 (U251R) tumours. | [177] |
| Carboplatin | Polymeric NPs | Polymer poly (ε-caprolactone) NPs | U87 MG | Increase uptake and cytotoxicity in U87 human GB cell line. No haemolytic activity in rat erythrocytes. | [186] |
| Carboplatin | Polymeric NPs (20–100 nm) | Polymer poly (ε-caprolactone) NPs | LN229 human GB cell line | Improved in vitro anti-tumour activity in comparison to free Carboplatin. Better nasal absorption compared to pure carboplatin solution and no severe damage of nasal mucosa. | [190] |
| Carboplatin | Polymeric NPs (365 nm) | Carboplatin-loaded poly (butyl cyanoacrylate) (PBCA) NPs conjugated with monoclonal antibody | C6 glioma cell lines C6 glioma-bearing rats (intraperitoneal injection) | Augmented cytotoxicity compared to free carboplatin. In vivo studies demonstrated an increased survival time and less side effects in the brain, kidney, or liver, compared to free carboplatin. | [187] |
| Carboplatin | Polymeric NPs (200 nm) | PLGA NPs | Primary rat hippocampal cell cultures. Adult male Wistar rats and white pigs (convection-enhanced delivery) | Improved cytotoxicity in vitro. Negligible neurotoxic effects and prolonged tissue half-life in vivo after infusion by CED in small and big animal models. | [188] |
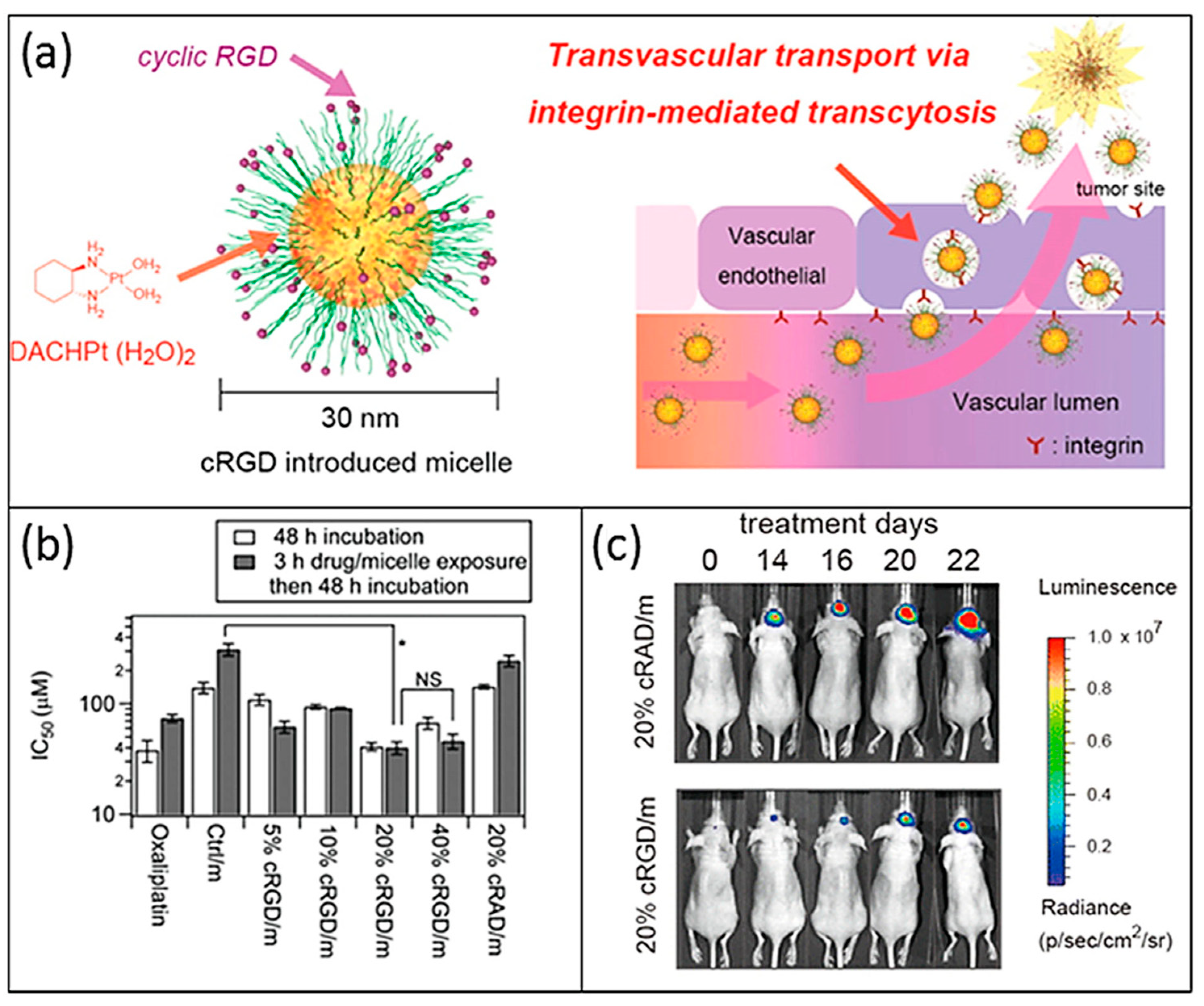
| Oxaliplatin | Polymeric NPs (20–30 nm) | PEG-P(Glu) NPs functionalized with cyclic Arg-Gly-Asp (cRGD) | U87MG cell line | Target GB cells and ability to cross BBB. Tumour growth inhibition in orthotopic model. | [192] |
| Oxaliplatin | Liposomes (57–86 nm) | Liposomal formulation (LipoxalTM) | F98 cell line (convection-enhanced delivery) | Administered by CED, increased tumoural accumulation, and median survival time in F98 glioma-bearing rats. | [193] |
| Oxaliplatin | CNTs (20 nm–several μm) | Multi-walled carbon nanotube functionalized with TAT/Biotin | C6 and CHEM-5 cell lines, C6 orthotopic glioma (intravenous injection) | Improved cytotoxicity of oxaliplatin toward glioma cells. Enhanced BBB penetration, improved brain-targeting selectivity, and excellent anti-tumour activity against orthotopic glioma. | [194] |
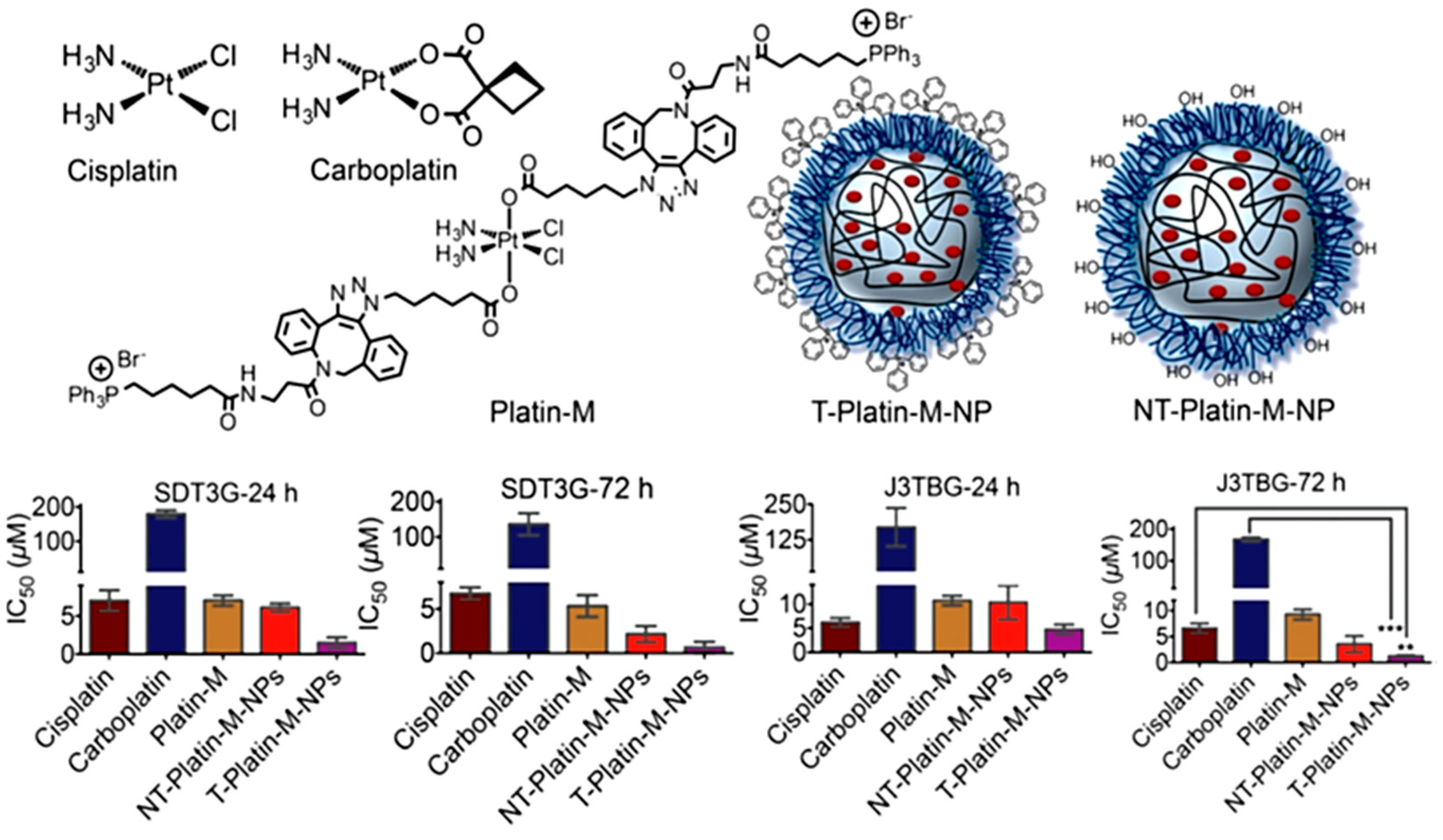
| Pt(IV) prodrug | Polymeric NPs (50–145 nm) | Cisplatin Pt(IV) prodrug in PLGA–PEG NPs | Canine J3TBG glioma and SDT3G glioblastoma cell lines (intravenous injection) | Overall 17 times more effective than cisplatin in vitro. Capable of crossing the canine BBB and accumulating in the brain. | [128] |
| Pt(IV) prodrug | CNTs (20 kDa ̴ 4 nm) | Coil nanotubes | U87, U251, and patient GB cells, human astrocytes, U87 xenografts (subcutaneous injection) | Enhanced in vitro and in vivo tumour cell killing in comparison with free prodrug, activating multiple cell death pathways in GB cells without affecting astrocytes in vitro or causing damage to healthy mouse brain. | [93] |
| Pt(IV) prodrug | Polymeric NPs (105 nm) | Oxaliplatin-derived Pt(IV) complexes attached to a reduction-responsive polymer, (poly(CHTA-co-HD)-PEG) | U87, TMZ-resistant LN229 cell lines and cells from a patient-derived xenograft. In vivo LN229-TR xenografts (convection-enhanced delivery) | Improved cell uptake and cytotoxicity in comparison to TMZ. Lack of toxicity, favorable distribution of drugs into the region of interest, substantial tumour growth inhibition, and increased by 3 the survival time in mice bearing tumours after CED administration in vivo. | [197] |
| Pt(IV) prodrugs | Solid lipid NPs (SLNs) (30–80 nm) | Pt(IV) prodrugs derived from kiteplatin in (SLNs) | U87 human GB cell line, hCMEC/D3 endothelial cells | Enhanced permeability, improved cell uptake compared to free drug. | [198] |
| Pt(IV) prodrugs | Nanostructured Coordination Polymers (NCPs) (70 nm) | Pt(IV) prodrugs obtained from cisplatin as building block in NCPs | HeLa and GL261 cell lines. Orthotopic preclinical GL261 GB tumour-bearing mice (intranasal administration) | In vitro dual pH and redox-mediated control release. Comparable cytotoxicity to cisplatin. In vivo intranasal administration demonstrated increased tumour accumulation of platinum and effective anticancer action. | [199] |
| Pt0 NPs | Metal NPs (2–20 nm) | FePt NPs | U251, U87, and H4 cell lines | Marked cytotoxicity observed in lipophilic coated FePt NPs and low cytotoxicity in the case of hydrophilic FePt NPs. | [200] |
| Pt(0) | Metal NPs (42 nm) | Ag-Pt NPs | U87 cell line | Inhibition of Gram-positive and Gram-negative multi-drug resistant bacteria. Selective and dose-dependent anticancer activity over U87 GB cells without being harmful to healthy human fibroblasts. | [201] |
6. Why Repurpose Platinum Drugs and Use Nanotechnology?
7. Summary and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S.U. Glioblastoma Multiforme: A Review of its Epidemiology and Pathogenesis through Clinical Presentation and Treatment. Asian Pac. J. Cancer Prev. 2017, 18, 3–9. [Google Scholar]
- Ostrom, Q.T.; Cote, D.J.; Ascha, M.; Kruchko, C.; Barnholtz-Sloan, J.S. Adult Glioma Incidence and Survival by Race or Ethnicity in the United States from 2000 to 2014. JAMA Oncol. 2018, 4, 1254–1262. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, M.; Gan, H.; Wang, H.; Lee, J.-H.; Fang, D.; Kitange, G.J.; He, L.; Hu, Z.; Parney, I.F.; et al. A novel enhancer regulates MGMT expression and promotes temozolomide resistance in glioblastoma. Nat. Commun. 2018, 9, 2949. [Google Scholar] [CrossRef]
- Broekman, M.L.; Maas, S.L.N.; Abels, E.R.; Mempel, T.R.; Krichevsky, A.M.; Breakefield, X.O. Multidimensional communication in the microenvirons of glioblastoma. Nat. Rev. Neurol. 2018, 14, 482–495. [Google Scholar] [CrossRef]
- Brown, N.F.; Carter, T.J.; Ottaviani, D.; Mulholland, P. Harnessing the immune system in glioblastoma. Br. J. Cancer. 2018, 119, 1171–1181. [Google Scholar] [CrossRef]
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 9, 1–10. [Google Scholar] [CrossRef]
- Condoluci, A.; Mazzara, C.; Zoccoli, A.; Pezzuto, A.; Tonini, G. Impact of smoking on lung cancer treatment effectiveness: A review. Future Oncol. 2016, 12, 2149–2161. [Google Scholar] [CrossRef]
- Stupp, R.; Warren, P.; Mason, P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Ruge, M.; Kocher, M.; Lucas, C.W.; Galldiks, N.; Grau, S. The Treatment of Gliomas in Adulthood. Dtsch. Arztebl. Int. 2018, 115, 356–364. [Google Scholar] [CrossRef]
- Mowforth, O.D.; Brannigan, J.; El Khoury, M.; Sarathi, C.I.P.; Bestwick, H.; Bhatti, F.; Mair, R. Personalised therapeutic approaches to glioblastoma: A systematic review. Front. Med. 2023, 10, 1166104. [Google Scholar] [CrossRef]
- Messali, A.; Villacorta, R.; Hay, J.W. A Review of the Economic Burden of Glioblastoma and the Cost Effectiveness of Pharmacologic Treatments. PharmacoEconomics 2014, 32, 1201–1212. [Google Scholar] [CrossRef]
- Reid, J.M.; Stevens, D.C.; Rubin, J.; Ames, M.M. Pharmacokinetics of 3-methyl-(triazen-1-yl) imidazole-4-carboximide following administration of temozolomide to patients with advanced cancer. Clin. Cancer Res. 1997, 3, 2393–2398. [Google Scholar]
- Lee, S.Y. Temozolomide resistance in glioblastoma multiforme. Genes Dis. 2016, 3, 198–210. [Google Scholar] [CrossRef]
- Alonso, M.M.; Gomez-Manzano, C.; Bekele, B.N.; Yung, W.A.; Fueyo, J. Adenovirus-based strategies overcome temozolomide resistance by silencing the O6-methylguanine-DNA methyltransferase promoter. Cancer Res. 2007, 67, 11499–11504. [Google Scholar] [CrossRef]
- Montaldi, A.P.; Godoy, P.R.; Sakamoto-Hojo, E.T. APE1/REF-1 down-regulation enhances the cytotoxic effects of temozolomide in a resistant glioblastoma cell line. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2015, 793, 19–29. [Google Scholar] [CrossRef]
- Ramirez, Y.P.; Weatherbee, J.L.; Wheelhouse, R.T.; Ross, A.H. Glioblastoma multiforme therapy and mechanisms of resistance. Pharmaceuticals 2013, 6, 1475–1506. [Google Scholar] [CrossRef]
- Alphandéry, E. Glioblastoma Treatments: An Account of Recent Industrial Developments. Front. Pharmacol. 2018, 9, 879. [Google Scholar] [CrossRef]
- Rominiyi, O.; Vanderlinden, A.; Clenton, S.J.; Bridgewater, C.; Al-Tamimi, Y.; Collis, S.J. Tumour treating fields therapy for glioblastoma: Current advances and future directions. Br. J. Cancer. 2021, 124, 697–709. [Google Scholar] [CrossRef]
- Nam, J.Y.; de Groot, J.F. Treatment of Glioblastoma. J. Oncol. 2017, 13, 629–638. [Google Scholar] [CrossRef]
- Diaz, R.J.; Ali, S.; Qadir, M.G.; De La Fuente, M.I.; Ivan, M.E.; Komotar, R.J. The role of bevacizumab in the treatment of glioblastoma. J. Neurooncol. 2017, 133, 455–467. [Google Scholar] [CrossRef]
- Taylor, T.E.; Furnari, F.B.; Cavenee, W.K. Targeting EGFR for Treatment of Glioblastoma: Molecular Basis to Overcome Resistance. Curr. Cancer Drug Targets 2012, 12, 197–209. [Google Scholar] [CrossRef]
- Kreisl, T.N.; Kotliarova, S.; Butman, J.A.; Albert, P.S.; Kim, L.; Musib, L.; Thornton, D.; Fine, H.A. A phase I/II trial of enzastaurin in patients with recurrent high-grade gliomas. Neuro Oncol. 2010, 12, 181–189. [Google Scholar] [CrossRef]
- Heffron, T.P.; Ndubaku, C.O.; Salphati, L.; Alicke, B.; Cheong, J.; Drobnick, J.; Edgar, K.; Gould, S.E.; Lee, L.B.; Lesnick, J.D.; et al. Discovery of Clinical Development Candidate GDC-0084, a Brain Penetrant Inhibitor of PI3K and mTOR. ACS Med. Chem. Lett. 2016, 7, 351–356. [Google Scholar] [CrossRef]
- Medikonda, R.; Dunn, G.; Rahman, M.; Fecci, P.; Lim, M. A review of glioblastoma immunotherapy. J. Neuro-Oncol. 2021, 151, 41–53. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, W.; Zhang, D.; Sun, Y.; Li, F.; Zheng, M.; Lovejoy, D.B.; Zou, Y.; Shi, B. Brain co-delivery of first-line chemotherapy drug and epigenetic bromodomain inhibitor formultidimensional enhanced synergistic glioblastoma therapy. Exploration 2022, 2, 20210274. [Google Scholar] [CrossRef]
- Weenink, B.; French, P.J.; Sillevis Smitt, P.A.E.; Debets, R.; Geurts, M. Immunotherapy in Glioblastoma: Current Shortcomings and Future Perspectives. Cancers 2020, 12, 751. [Google Scholar] [CrossRef]
- Huang, B.; Yu, Z.; Liang, R. Effect of long-term adjuvant temozolomide chemotherapy on primary glioblastoma patient survival. BMC Neurol. 2021, 21, 424. [Google Scholar] [CrossRef]
- Aliyu, A.; Shaari, M.R.; Sayuti, N.S.A.; Reduan, M.F.H.; Sithambaram, S.; Noordin, M.M.; Shaari, K.; Hamzah, H. N-Ethyl-n-Nitrosourea Induced Leukaemia in a Mouse Model through Upregulation of Vascular Endothelial Growth Factor and Evading Apoptosis. Cancers 2020, 12, 678. [Google Scholar] [CrossRef]
- Jeon, J.; Lee, S.; Kim, H.; Kang, H.; Youn, H.; Jo, S.; Youn, B.; Kim, H.Y. Revisiting Platinum-Based Anticancer Drugs to Overcome Gliomas. Int. J. Mol. Sci. 2021, 22, 5111. [Google Scholar] [CrossRef]
- Ghosh, D.; Nandi, S.; Bhattacharjee, S. Combination therapy to checkmate Glioblastoma: Clinical challenges and advances. Clin. Trans. Med. 2018, 7, 33. [Google Scholar] [CrossRef]
- Kelland, L. The resurgence of platinum-based cancer chemotherapy. Nat. Rev. Cancer 2007, 7, 573–584. [Google Scholar] [CrossRef] [PubMed]
- de Biasi, A.R.; Villena-Vargas, J.; Adusumilli, P.S. Cisplatin-Induced Antitumor Immunomodulation: A Review of Preclinical and Clinical Evidence. Clin. Cancer Res. 2014, 20, 5384–5391. [Google Scholar] [CrossRef] [PubMed]
- Ndagi, U.; Mhlongo, N.; Soliman, M.E. Metal complexes in cancer therapy—An update from drug design perspective. Drug. Des. Devel. Ther. 2017, 11, 599–616. [Google Scholar] [CrossRef]
- Wang, J.L.; Barth, R.F.; Cavaliere, R.; Puduvalli, V.K.; Giglio, P.; Lonser, R.R.; Elder, J.B. Phase I trial of intracerebral convectionenhanced delivery of carboplatin for treatment of recurrent high-grade gliomas. PLoS ONE 2020, 15, e0244383. [Google Scholar] [CrossRef] [PubMed]
- Silvani, A.; Eoli, M.; Salmaggi, A.; Lamperti, E.; Maccagnano, E.; Broggi, G.; Boiardi, A. Phase II trial of cisplatin plus temozolomide, in recurrent and progressive malignant glioma patients. J. Neuro-Oncol. 2004, 66, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; McCully, C.L.; Murphy, R.F.; Bacher, J.; Balis, F.M.; Fox, E. Extracellular fluid concentrations of cisplatin, carboplatin, and oxaliplatin in brain, muscle, and blood measured using microdialysis in nonhuman primates. Cancer Chemother. Pharmacol. 2010, 65, 817–824. [Google Scholar] [CrossRef]
- Johnstone, T.C.; Suntharalingam, K.; Lippard, S.J. The Next Generation of Platinum Drugs: Targeted Pt(II) Agents, Nanoparticle Delivery, and Pt(IV) Prodrugs. Chem. Rev. 2016, 116, 3436–3486. [Google Scholar] [CrossRef] [PubMed]
- Huncharek, M.; Muscat, J. Treatment of recurrent high grade astrocytoma; results of a systematic review of 1415 patients. Anticancer Res. 1998, 18, 1303–1311. [Google Scholar]
- Yung, W.K.A.; Mechtler, L.; Gleason, M.J. Intravenous carboplatin for recurrent malignant glioma: A phase II study. J. Clin. Oncol. 1991, 9, 860–864. [Google Scholar] [CrossRef]
- Posadas, I.; Alonso-Moreno, C.; Bravo, I.; Carrillo-Hermosilla, F.; Garzon, A.; Villaseca, N.; Lopez-Solera, I.; Albaladejo, J.; Cena, V. Synthesis, Characterization, DNA Interactions and Antiproliferative Activity on Glioblastoma of Iminopyridine Platinum(II) Chelate Complexes. J. Inorg. Biochem. 2017, 168, 46–54. [Google Scholar] [CrossRef]
- Mishima, K.; Mazar, A.P.; Gown, A.; Skelly, M.; Ji, X.D.; Wang, X.D.; Jones, T.R.; Cavenee, W.K.; Huang, H.J. A peptide derived from the non-receptor binding region of urokinase plasminogen activator inhibits glioblastoma growth and angiogenesis in vivo in combination with cisplatin. Proc. Natl. Acad. Sci. USA 2000, 97, 8484–8489. [Google Scholar] [CrossRef] [PubMed]
- Spiro, T.P.; Liu, L.; Majka, S.; Haaga, J.; Willson, J.K.V.; Gerson, S.L. Temozolomide: The effect of once- and twice-a-day dosing on tumor tissue levels of the DNA repair protein O6-alkylguanine-DNA-alkyltransferase. Clin. Cancer Res. 2001, 7, 2309–2317. [Google Scholar] [PubMed]
- Zheng, Y.; Hunting, D.J.; Ayotte, P.; Sanche, L. Role of secondary lowenergy electrons in the concomitant chemoradiation therapy of cancer. Phys. Rev. Lett. 2008, 100, 198101. [Google Scholar] [CrossRef] [PubMed]
- Nagane, M.; Narita, Y.; Mishima, K.; Levitzki, A.; Burgess, A.W.; Cavenee, W.K.; Huang, H.J. Human Glioblastoma Xenografts Overexpressing a Tumor-Specific Mutant Epidermal Growth Factor Receptor Sensitized to Cisplatin by the Ag1478 Tyrosine Kinase Inhibitor. J. Neurosurg. 2001, 95, 472–479. [Google Scholar] [CrossRef]
- Brandes, A.A.; Basso, U.; Reni, M.; Vastola, F.; Tosoni, A.; Cavallo, G.; Scopece, L.; Ferreri, A.J.; Panucci, M.G.; Monfardini, S.; et al. First-Line Chemotherapy with Cisplatin Plus Fractionated Temozolomide in Recurrent Glioblastoma Multiforme: A Phase Ii Study of the Gruppo Italiano Cooperativo Di Neuro-Oncologia. J. Clin. Oncol. 2004, 22, 1598–1604. [Google Scholar] [CrossRef]
- Wang, X.; Wang, X.; Jin, S.; Muhammad, N.; Guo, Z. Stimuli-Responsive Therapeutic Metallodrugs. Chem. Rev. 2019, 119, 1138–1192. [Google Scholar] [CrossRef]
- Hess, S.M.; Anderson, J.G.; Bierbach, U. A Non-Crosslinking Platinum-Acridine Hybrid Agent Shows Enhanced Cytotoxicity Compared to Clinical Bcnu and Cisplatin in Glioblastoma Cells. Bioorg. Med. Chem. Lett. 2005, 15, 443–446. [Google Scholar] [CrossRef]
- Gajski, G.; Čimbora-Zovko, T.; Rak, S.; Osmak, M.; Garaj-Vrhovac, V. Antitumour Action on Human Glioblastoma A1235 Cells through Cooperation of Bee Venom and Cisplatin. Cytotechnology 2016, 68, 1197–1205. [Google Scholar] [CrossRef]
- Zhu, T.; Xu, Y.; Dong, B.; Zhang, J.; Wei, Z.; Xu, Y.; Yao, Y. Β-Elemene Inhibits Proliferation of Human Glioblastoma Cells through the Activation of Glia Maturation Factor Β and Induces Sensitization to Cisplatin. Oncol. Rep. 2011, 26, 405–413. [Google Scholar]
- Park, C.K.; Park, S.H.; Lee, S.H.; Kim, C.Y.; Kim, D.W.; Paek, S.H.; Kim, D.G.; Heo, D.S.; Kim, I.H.; Jung, H.W. Methylation Status of the Mgmt Gene Promoter Fails to Predict the Clinical Outcome of Glioblastoma Patients Treated with Acnu Plus Cisplatin. Neuropathology 2009, 29, 443–449. [Google Scholar] [CrossRef]
- Buckner, J.C.; Ballman, K.V.; Michalak, J.C.; Burton, G.V.; Cascino, T.L.; Schomberg, P.J.; Hawkins, R.B.; Scheithauer, B.W.; Sandler, H.M.; Marks, R.S.; et al. Phase Iii Trial of Carmustine and Cisplatin Compared with Carmustine Alone and Standard Radiation Therapy or Accelerated Radiation Therapy in Patients with Glioblastoma Multiforme: North Central Cancer Treatment Group 93-72-52 and Southwest Oncology Group 9503 Trials. J. Clin. Oncol. 2006, 24, 3871–3879. [Google Scholar] [PubMed]
- Barth, R.F.; Wu, G.; Hans Meisen, W.; Nakkula, R.J.; Yang, W.; Huo, T.; Kellough, D.A.; Kaumaya, P.; Turro, C.; Agius, L.M.; et al. Design, synthesis, and evaluation of cisplatincontaining EGFR targeting bioconjugates as potential therapeutic agents for brain tumors. OncoTargets Ther. 2016, 9, 2769–2781. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Wu, Q.; Fang, M.; Huang, W.; Zhu, H. Mir-152-3p Sensitizes Glioblastoma Cells Towards Cisplatin Via Regulation of Sos1. OncoTargets Ther. 2019, 12, 9513–9525. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Song, J.; Guo, F. Mir-186 Reverses Cisplatin Resistance and Inhibits The formation of the Glioblastoma-Initiating Cell phenotype by Degrading Yin Yang 1 in Glioblastoma. Int. J. Mol. Med. 2019, 43, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, R.M.; Garratt-Lalonde, M.; Parolin, D.A.E.; Krzyzanowski, P.M.; Andrade, M.A.; Lorimer, I.A.J. Protection of Glioblastoma Cells from Cisplatin Cytotoxicity Via Protein Kinase Cι-Mediated Attenuation of P38 Map Kinase Signaling. Oncogene 2006, 25, 2909–2919. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Yuan, C.; Wei, F.; Wang, G.; Zhang, J.; Bellail, A.C.; Zhang, Z.; Olson, J.J.; Hao, C. Cisplatin Restores Trail Apoptotic Pathway in Glioblastoma-Derived Stem Cells through up-Regulation of Dr5 and Down-Regulation of C-Flip. Cancer Investig. 2011, 29, 511–520. [Google Scholar] [CrossRef]
- Ferrari, B.; Urselli, F.; Gilodi, M.; Camuso, S.; Priori, E.C.; Rangone, B.; Ravera, M.; Veneroni, P.; Zanellato, I.; Roda, E.; et al. New Platinum-Based Prodrug Pt(Iv)Ac-Poa: Antitumour Effects in Rat C6 Glioblastoma Cells. Neurotox. Res. 2020, 37, 183–197. [Google Scholar] [CrossRef]
- Macieja, A.; Kopa, P.; Galita, G.; Pastwa, E.; Majsterek, I.; Poplawski, T. Comparison of the Effect of Three Different Topoisomerase Ii Inhibitors Combined with Cisplatin in Human Glioblastoma Cells Sensitized with Double Strand Break Repair Inhibitors. Mol. Biol. Rep. 2019, 46, 3625–3636. [Google Scholar] [CrossRef]
- Gwak, H.-S.; Shingu, T.; Chumbalkar, V.; Hwang, Y.-H.; DeJournett, R.; Latha, K.; Koul, D.; Alfred Yung, W.K.; Powis, G.; Farrell, N.P.; et al. Combined Action of the Dinuclear Platinum Compound Bbr3610 with the Pi3-K Inhibitor Px-866 in Glioblastoma. Int. J. Cancer 2011, 128, 787–796. [Google Scholar] [CrossRef]
- Rosa, P.; Catacuzzeno, L.; Sforna, L.; Mangino, G.; Carlomagno, S.; Mincione, G.; Petrozza, V.; Ragona, G.; Franciolini, F.; Calogero, A. Bk Channels Blockage Inhibits Hypoxia-Induced Migration and Chemoresistance to Cisplatin in Human Glioblastoma Cells. J. Cell. Physiol. 2018, 233, 6866–6877. [Google Scholar] [CrossRef]
- Benzina, S.; Fischer, B.; Miternique-Grosse, A.; Dufour, P.; Denis, J.M.; Bergerat, J.P.; Gueulette, J.; Bischoff, P. Cell Death Induced in a Human Glioblastoma Cell Line by P(65)+Be Neutrons Combined with Cisplatin. Life Sci. 2006, 79, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Roci, E.; Cakani, B.; Brace, G.; Bushati, T.; Rroji, A.; Petrela, M.; Kaloshi, G. Platinum-based Chemotherapy in Recurrent High-grade Glioma Patients: Retrospective Study. Med. Arh. 2014, 68, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kong, X.; Guo, Y.; Wang, R.; Ma, W. Continuous Dose-Intense Temozolomide and Cisplatin in Recurrent Glioblastoma Patients. Medicine 2017, 96, e6261. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Setlow, R.B. Inactivation of O-6-alkylguanine-DNA Alkyltransferase in HeLa cells by cisplatin. Carcinogenesis 1989, 10, 1681–1684. [Google Scholar] [CrossRef]
- Piccioni, D.; D’atri, S.; Papa, G.; Caravita, T.; Franchi, A.; Bonmassar, E.; Graziani, G. Cisplatin increases sensitivity of human leukemic blasts to triazene compounds. J. Chemother. 1995, 7, 224–229. [Google Scholar] [CrossRef]
- Britten, C.D.; Rowinsky, E.K.; Baker, S.D.; Agarwala, S.S.; Eckardt, J.R.; Barrington, R.; Diab, S.G.; Hammond, L.A.; Johnson, T.; Villalona-Calero, M.; et al. A phase I and pharmacokinetic study of Temozolomide and cisplatin in patients with advanced solid malignancies. Clin. Cancer Res. 1999, 5, 1629–1637. [Google Scholar]
- Rousseau, J.; Barth, R.F.; Fernandez, M.; Adam, J.-F.; Balosso, J.; Estève, F.; Elleaume, H. Efficacy of Intracerebral Delivery of Cisplatin in Combination with Photon Irradiation for Treatment of Brain Tumors. J. Neurooncol. 2010, 98, 287–295. [Google Scholar] [CrossRef]
- Billecke, C.; Finniss, S.; Tahash, L.; Miller, C.; Mikkelsen, T.; Farrell, N.P.; Bögler, O. Polynuclear platinum anticancer drugs are more potent than cisplatin and induce cell cycle arrest in glioma. Neuro Oncol. 2006, 8, 215–226. [Google Scholar] [CrossRef]
- Newton, H.B.; Page, M.A.; Junck, L.; Greenberg, H.S. Intra-arterial cisplatin for the treatment of malignant gliomas. J Neurooncol. 1989, 7, 39–45. [Google Scholar] [CrossRef]
- Feun, L.G.; Stewart, D.J.; Maor, M.; Leavens, M.; Savaraj, N.; Burgess, M.A.; Yung, W.K.A.; Benjamin, R.S. A pilot study of cis-diamminedichloroplatinum and radiation therapy in patients with high grade astrocytomas. J. Neurooncol. 1983, 1, 109–113. [Google Scholar] [CrossRef]
- Silvani, A.; Gaviani, P.; Lamperti, E.A.; Eoli, M.; Falcone, C.; DiMeco, F.; Milanesi, I.M.; Erbetta, A.; Boiardi, A.; Fariselli, L.; et al. Cisplatinum and BCNU chemotherapy in primary glioblastoma patients. J. Neurooncol. 2009, 94, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Balaña, C.; López-Pousa, A.; Berrocal, A.; Yaya-Tur, R.; Herrero, A.; García, J.L.; Martín-Broto, J.; Benavides, M.; Cerdá-Nicolás, M.; Ballester, R.; et al. Phase II study of temozolomide and cisplatin as primary treatment prior to radiotherapy in newly diagnosed glioblastoma multiforme patients with measurable disease. A study of the Spanish Medical Neuro-Oncology Group (GENOM). J. Neurooncol. 2004, 70, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Chovanec, M.; Abu Zaid, M.; Hanna, N.; El-Kouri, N.; Einhorn, L.H.; Albany, C. Long-term Toxicity of Cisplatin in Germ-Cell Tumor Survivors. Ann. Oncol. 2017, 28, 2670–2679. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Wang, C.; Wang, L.; Chen, Y. A comprehensive review in improving delivery of small-molecule chemotherapeutic agents overcoming the blood-brain/brain tumor barriers for glioblastoma treatment. Drug Deliv. 2019, 26, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, Z.I.; Burks, S.R.; Frank, J.A. Focused ultrasound with microbubbles induces sterile inflammatory response proportional to the blood brain barrier opening: Attention to experimental conditions. Theranostics 2018, 8, 2245–2248. [Google Scholar] [CrossRef]
- Sharabi, S.; Bresler, Y.; Ravid, O.; Shemesh, C.; Atrakchi, D.; Schnaider-Beeri, M.; Gosselet, F.; Dehouck, L.; Last, D.; Guez, D.; et al. Transient blood–brain barrier disruption is induced by low pulsed electrical fields in vitro: An analysis of permeability and trans-endothelial electric resistivity. Drug Deliv. 2019, 26, 459–469. [Google Scholar] [CrossRef]
- Graham-Gurysh, E.; Moore, K.M.; Satterlee, A.B.; Sheets, K.T.; Lin, F.C.; Bachelder, E.M.; Miller, C.R.; Hingtgen, S.D.; Ainslie, K.M. Sustained Delivery of Doxorubicin Via Acetalated Dextran Scaffold Prevents Glioblastoma Recurrence after Surgical Resection. Mol. Pharm. 2018, 15, 1309–1318. [Google Scholar] [CrossRef]
- Tabet, A.; Jensen, M.P.; Parkins, C.C.; Patil, P.G.; Watts, C.; Scherman, O.A. Designing Next-Generation Local Drug Delivery Vehicles for Glioblastoma Adjuvant Chemotherapy: Lessons from the Clinic. Adv. Healthc. Mater. 2019, 8, e1801391. [Google Scholar] [CrossRef]
- Minghan, S.; Sanche, L. Convection-Enhanced Delivery in Malignant Gliomas: A Review of Toxicity and Efficacy. J. Oncol. 2019, 2019, 9342796. [Google Scholar]
- Mathew, E.N.; Berry, B.C.; Yang, H.W.; Carroll, R.S.; Johnson, M.D. Delivering Therapeutics to Glioblastoma: Overcoming Biological Constraints. Int. J. Mol. Sci. 2022, 23, 1711. [Google Scholar] [CrossRef]
- Ruiz-Molina, D.; Mao, X.; Alfonso-Triguero, P.; Lorenzo, J.; Bruna, J.; Yuste, V.J.; Candiota, A.P.; Novio, F. Advances in Preclinical/Clinical Glioblastoma Treatment: Can Nanoparticles Be of Help? Cancers 2022, 14, 4960. [Google Scholar] [CrossRef] [PubMed]
- Harder, B.G.; Blomquist, M.R.; Wang, J.; Kim, A.J.; Woodworth, G.F.; Winkles, J.A.; Loftus, J.C.; Tran, N.L. Developments in Blood-Brain Barrier Penetrance and Drug Repurposing for Improved Treatment of Glioblastoma. Front. Oncol. 2018, 8, 462. [Google Scholar] [CrossRef] [PubMed]
- Hersh, D.; Wadajkar, A.S.; Roberts, N.B.; Perez, J.G.; Connolly, N.P.; Frenkel, V.; Winkles, J.A.; Woodworth, G.F.; Kim, A.J. Evolving Drug Delivery Strategies to Overcome the Blood Brain Barrier. Curr. Pharm. Des. 2016, 22, 1177–1193. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.J.; Malhotra, M.A.; O’Mahony, M.; Cryan, J.F.; O’Driscoll, C.M. Nanoparticles and the Blood-Brain Barrier: Advancing from In-Vitro Models Towards Therapeutic Significance. Pharm. Res. 2015, 32, 1161–1185. [Google Scholar] [CrossRef]
- Saraiva, C.; Praça, C.; Ferreira, R.; Santos, T.; Ferreira, L.; Bernardino, L. Nanoparticle-mediated brain drug delivery: Overcoming blood–brain barrier to treat neurodegenerative diseases. J. Control. Release 2016, 235, 34–47. [Google Scholar] [CrossRef]
- Zhang, Y.; Fu, X.; Jia, J.; Wikerholmen, T.; Xi, K.; Kong, Y.; Wang, J.; Chen, H.; Ma, Y.; Li, Z.; et al. Glioblastoma therapy using codelivery of cisplatin and glutathione peroxidase targeting siRNA from iron oxide nanoparticles. ACS Appl. Mater. Interf. 2020, 12, 43408–43421. [Google Scholar] [CrossRef]
- Wadajkar, A.S.; Dancy, J.G.; Hersha, D.S.; Anastasiadis, P.; Tran, N.L.; Woodworth, G.F.; Winkles, J.A.; Kim, A.J. Tumor-targeted Nanotherapeutics: Overcoming Treatment Barriers for Glioblastoma. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2017, 9, e1439. [Google Scholar] [CrossRef]
- Wang, X.; Guo, Z. Targeting and delivery of platinum-based anticancer drugs. Chem. Soc. Rev. 2013, 42, 202–224. [Google Scholar] [CrossRef]
- Haxton, K.J.; Burt, H.M. Polymeric drug delivery of platinum-based anticancer agents. J. Pharm. Sci. 2009, 98, 2299–2316. [Google Scholar] [CrossRef]
- Wu, H.; Cabral, H.; Toh, K.; Mi, P.; Chen, Y.-C.; Matsumoto, Y.; Yamada, N.; Liu, X.; Kinoh, H.; Miura, Y. Polymeric micelles loaded with platinum anticancer drugs target preangiogenic micrometastatic niches associated with inflammation. J. Control Release 2014, 189, 1–10. [Google Scholar] [CrossRef]
- Kesavan, A.; Ilaiyaraja, P.; Beaula, W.S.; Kumari, V.V.; Lal, J.S.; Arunkumar, C.; Anjana, G.; Srinivas, S.; Ramesh, A.; Rayala, S.K.; et al. Tumor targeting using polyamidoamine dendrimer–cisplatin nanoparticles functionalized with diglycolamic acid and herceptin. Eur. J. Pharm. Biopharm. 2015, 96, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Timbie, K.F.; Afzal, U.; Date, A.; Zhang, C.; Song, J.; Miller, G.W.; Suk, J.S.; Hanes, J.; Price, R.J. MR image-guided delivery of cisplatin-loaded brain-penetrating nanoparticles to invasive glioma with focused ultrasound. J. Control. Release 2017, 263, 120–131. [Google Scholar] [CrossRef]
- Thanasupawat, T.; Bergen, H.; Hombach-Klonisch, S.; Krcek, J.; Ghavami, S.; Del Bigio, M.R.; Krawitz, S.; Stelmack, G.; Halayko, A.; McDougall, M.; et al. Platinum (IV) coiled coil nanotubes selectively kill human glioblastoma cells. Nanomed. Nanotechnol. Biol. Med. 2015, 11, 913–925. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Islas, E.; Sosa-Arróniz, A.; Manríquez-Ramírez, M.E.; Rodríguez-Pérez, C.E.; Tzompantzi, F.; Padilla, J.M. Mesoporous silica nanoparticles functionalized with folic acid for targeted release Cis-Pt to glioblastoma cells. Rev. Adv. Mater. Sci. 2021, 60, 25–37. [Google Scholar] [CrossRef]
- Depciuch, J.; Miszczyk, J.; Maximenko, A.; Zielinski, P.M.; Rawojc, K.; Panek, A.; Olko, P.; Parlinska-Wojtan, M. Gold Nanopeanuts as Prospective Support for Cisplatin in Glioblastoma Nano-Chemo-Radiotherapy. Int. J. Mol. Sci. 2020, 21, 9082. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Calero-Pérez, P.; Montpeyó, D.; Bruna, J.; Yuste, V.J.; Candiota, A.P.; Lorenzo, J.; Novio, F.; Ruiz-Molina, D. Intranasal Administration of Catechol-Based Pt(IV) Coordination Polymer Nanoparticles for Glioblastoma Therapy. Nanomaterials 2022, 12, 1221. [Google Scholar] [CrossRef] [PubMed]
- Charest, G.; Sanche, L.; Fortin, D.; Mathieu, D.; Paquette, B. Glioblastoma Treatment: Bypassing the Toxicity of Platinum Compounds by Using Liposomal Formulation and Increasing Treatment Efficiency with Concomitant, Radiotherapy. Int. J. Radiation Oncol. Biol. Phys. 2012, 84, 244–249. [Google Scholar] [CrossRef]
- Zahednezhad, F.; Zakeri-Milani, P.; Shahbazi Mojarrad, J.; Valizadeh, H. The latest advances of cisplatin liposomal formulations: Essentials for preparation and analysis. Expert Opin. Drug Deliv. 2020, 17, 523–541. [Google Scholar] [CrossRef]
- Liu, L.; Ye, Q.; Lu, M.; Lo, Y.-C.; Hsu, Y.-H.; Wei, M.-C.; Chen, Y.-H.; Lo, S.-C.; Wang, S.-J.; Bain, D.J. A new approach to reduce toxicities and to improve bioavailabilities of platinum-containing anti-cancer nanodrugs. Sci. Rep. 2015, 5, 10881. [Google Scholar] [CrossRef]
- Hernández-Pedro, N.Y.; Rangel-López, E.; Magaña-Maldonado, R.; Pérez de la Cruz, V.; Santamaría del Angel, A.; Pineda, B.; Sotelo, J. Application of Nanoparticles on Diagnosis and Therapy in Gliomas. Biomed. Res. Int. 2013, 2013, 351031. [Google Scholar] [CrossRef]
- Zhao, Y.Z.; Lin, Q.; Wong, H.L.; Shen, X.T.; Yang, W.; Xu, H.L.; Mao, K.L.; Tian, F.R.; Yang, J.J.; Xu, J.; et al. Glioma-targeted therapy using Cilengitide nanoparticles combined with UTMD enhanced delivery. J. Control. Release 2016, 224, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Nainwal, N. Recent advances in transcranial focused ultrasound (FUS) triggered brain delivery. Curr. Drug Targets 2017, 18, 1225–1232. [Google Scholar] [CrossRef] [PubMed]
- Hoadley, K.A.; Yau, C.; Wolf, D.M.; Cherniack, A.D.; Tamborero, D.; Ng, S.; Leiserson, M.D.; Niu, B.; McLellan, M.D.; Uzunangelov, V. Multiplatform analysis of 12 cancer types reveals molecular classification within and across tissues of origin. Cell 2014, 158, 929–944. [Google Scholar] [CrossRef] [PubMed]
- Charest, G.; Sanche, L.; Fortin, D.; Mathieu, D.; Paquette, B. Optimization of the Route of Platinum Drugs Administration to Optimize the Concomitant Treatment with Radiotherapy for Glioblastoma Implanted in the Fischer Rat Brain. J. Neurooncol. 2013, 115, 365–373. [Google Scholar] [CrossRef]
- Rahman, A.A.; Stojanovska, V.; Pilowsky, P.; Nurgali, K. Platinum accumulation in the brain and alteration in the central regulation of cardiovascular and respiratory functions in oxaliplatin-treated rats. Pflugers Arch—Eur. J. Physiol. 2021, 473, 107–120. [Google Scholar] [CrossRef]
- Dermitzakis, E.V.; Kimiskidis, V.K.; Eleftheraki, A.; Lazaridis, G.; Konstantis, A.; Basdanis, G.; Tsiptsios, I.; Georgiadis, G.; Fountzilas, G. The impact of oxaliplatin-based chemotherapy for colorectal cancer on the autonomous nervous system. Eur. J. Neurol. 2014, 21, 1471–1477. [Google Scholar] [CrossRef]
- Tajbakhsh, M.; Houghton, P.J.; Morton, C.L.; Kolb, E.A.; Gorlick, R.; Maris, J.M.; Keir, S.T.; Wu, J.; Reynolds, C.P.; Smith, M.A.; et al. Initial testing of cisplatin by the pediatric preclinical testing program. Pediatr. Blood Cancer 2008, 50, 992–1000. [Google Scholar] [CrossRef]
- Rao, A.A.N.; Wallace, D.J.; Billups, C.; Boyett, J.M.; Gajjar, A.; Packer, R.J. Cumulative cisplatin dose is not associated with event-free or overall survival in children with newly diagnosed average-risk medulloblastoma treated with cisplatin based adjuvant chemotherapy: Report from the Children’s Oncology Group. Pediatr. Blood Cancer 2014, 61, 102–106. [Google Scholar] [CrossRef]
- Enríquez Pérez, J.; Fitzell, S.; Kopecky, J.; Visse, E.; Darabi, A.; Siesjö, P. The effect of locally delivered cisplatin is dependent on an intact immune function in an experimental glioma model. Sci. Rep. 2019, 9, 5632. [Google Scholar] [CrossRef]
- Xue, Y.; Gao, S.; Gou, J.; Yin, T.; He, H.; Wang, Y.; Zhang, Y.; Tang, X.; Wu, R. Platinum-based chemotherapy in combination with PD-1/PD-L1 inhibitors: Preclinical and clinical studies and mechanism of action. Expert Opin. Drug Deliv. 2021, 18, 187–203. [Google Scholar] [CrossRef]
- Park, S.J.; Ye, W.; Xiao, R.; Silvin, C.; Padget, M.; Hodge, J.W.; Van Waes, C.; Schmitt, N.C. Cisplatin and oxaliplatin induce similar immunogenic changes in preclinical models of head and neck cancer. Oral Oncol. 2019, 95, 127–135. [Google Scholar] [CrossRef]
- Eiseman, J.L.; Beumer, J.H.; Rigatti, L.H.; Strychor, S.; Meyers, K.; Dienel, S.; Horn, C.C. Plasma Pharmacokinetics and Tissue and Brain Distribution of Cisplatin in Musk Shrews. Cancer Chemother. Pharmacol. 2015, 75, 143–152. [Google Scholar] [CrossRef]
- McWhinney, S.R.; Goldberg, R.M.; McLeod, H.L. Platinum neurotoxicity pharmacogenetics. Mol. Cancer Ther. 2009, 8, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Rademaker-Lakhai, J.M.; Crul, M.; Zuur, L.; Baas, P.; Beijnen, J.H.; Simis, Y.J.; Van Zandwijk, N.; Schellens, J.H. Relationship between cisplatin administration and the development of ototoxicity. J. Clin. Oncol. 2006, 24, 918–924. [Google Scholar] [CrossRef]
- Pardridge, W.M. The blood-brain barrier: Bottleneck in brain drug development. NeuroRx 2005, 2, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Massimino, M.; Spreafico, F.; Riva, D.; Biassoni, V.; Poggi, G.; Solero, C.; Gandola, L.; Genitori, L.; Modena, P.; Simonetti, F.; et al. A lower-dose, lower-toxicity cisplatin-etoposide regimen for childhood progressive low-grade glioma. J. Neurooncol. 2010, 100, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, B.; Roda, E.; Priori, E.C.; De Luca, F.; Facoetti, A.; Ravera, M.; Brandalise, F.; Locatelli, C.A.; Rossi, P.; Bottone, M.G. A New Platinum-Based Prodrug Candidate for Chemotherapy and Its Synergistic Effect with Hadrontherapy: Novel Strategy to Treat Glioblastoma. Front. Neurosci. 2021, 15, 589906. [Google Scholar] [CrossRef]
- Prados, M.D.; Schold, S.C.; Fine, H.A.; Jaeckle, K.; Hochberg, F.; Mechtler, L.; Fetell, M.R.; Phuphanich, S.; Feun, L.; Janus, T.J.; et al. A randomized, double-blind, placebo-controlled, phase 2 study of RMP-7 in combination with carboplatin administered intravenously for the treatment of recurrent malignant glioma. Neuro Oncol. 2003, 5, 96–103. [Google Scholar] [CrossRef]
- Sheleg, S.; Korotkevich, E.; Zhavrid, E.; Muravskaya, G.; Smeyanovich, A.; Shanko, Y.; Yurkshtovich, T.; Bychkovsky, P.; Belyaev, S. Local chemotherapy with cisplatin-depot for glioblastoma multiforme. J. Neurooncol. 2002, 60, 53–59. [Google Scholar] [CrossRef]
- White, E.; Bienemann, A.; Taylor, H.; Hopkins, K.; Cameron, A.; Gill, S. A phase I trial of carboplatin administered by convection-enhanced delivery to patients with recurrent/progressive glioblastoma multiforme. Contemp. Clin. Trials 2012, 33, 320–331. [Google Scholar] [CrossRef]
- Saida, Y.; Watanabe, S.; Tanaka, T.; Baba, J.; Sato, K.; Shoji, S.; Igarashi, N.; Kondo, R.; Okajima, M.; Koshio, J.; et al. Critical roles of chemoresistant effector and regulatory T cells in antitumor immunity after lymphodepleting chemotherapy. J. Immunol. 2015, 195, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Roberts, N.B.; Wadajkar, A.S.; Winkles, J.A.; Davila, E.; Kim, A.J.; Woodworth, G.F. Repurposing platinum-based chemotherapies for multi-modal treatment of glioblastoma. Oncoimmunology 2016, 5, e1208876. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, J. Drug delivery to the central nervous system by polymeric nanoparticles: What do we know? Adv. Drug Deliv. Rev. 2014, 71, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, T.C.; Wilson, J.J.; Lippard, S.J. Monofunctional and Higher-Valent Platinum Anticancer Agents. Inorg. Chem. 2013, 52, 12234–12249. [Google Scholar] [CrossRef]
- Sun, H.; Chen, X.; Chen, D.; Dong, M.; Fu, X.; Li, Q.; Liu, X.; Wu, Q.; Qiu, T.; Wan, T.; et al. Influences of surface coatings and components of FePt nanoparticles on the suppression of glioma cell proliferation. Int. J. Nanomed. 2012, 7, 3295–3307. [Google Scholar]
- Liang, S.; Zhou, Q.; Wang, M.; Zhu, Y.; Wu, Q.; Yang, X. Water-soluble l-cysteine-coated FePt nanoparticles as dual MRI/CT imaging contrast agent for glioma. Int. J. Nanomed. 2015, 10, 2325–2333. [Google Scholar]
- Duan, X.; He, C.; Kron, S.J.; Lin, W. Nanoparticle formulations of cisplatin for cancer therapy. Wiley Interdiscip. Rev. NanomedNanobiotechnol. 2016, 8, 776–791. [Google Scholar] [CrossRef]
- Feldhaeusser, B.; Platt, S.R.; Marrache, S.; Kolishetti, N.; Pathak, R.K.; Montgomery, D.J.; Reno, L.R.; Howerth, E.; Dhar, S. Evaluation of nanoparticle delivered cisplatin in beagles. Nanoscale 2015, 7, 13822–13830. [Google Scholar] [CrossRef]
- Kim, J.-H.; Kim, Y.-S.; Park, K.; Lee, S.; Nam, H.Y.; Min, K.H.; Jo, H.G.; Park, J.H.; Choi, K.; Jeong, S.Y.; et al. Antitumor efficacy of cisplatin-loaded glycol chitosan nanoparticles in tumor-bearing mice. J. Control Release 2008, 127, 41–49. [Google Scholar] [CrossRef]
- Ding, D.; Zhu, Z.; Liu, Q.; Wang, J.; Hu, Y.; Jiang, X.; Liu, B. Cisplatin-loaded gelatin-poly(acrylic acid) nanoparticles: Synthesis, antitumor efficiency in vivo and penetration in tumors. Eur. J. Pharm. Biopharm. 2011, 79, 142–149. [Google Scholar] [CrossRef]
- Mattheolabakis, G.; Taoufik, E.; Haralambous, S.; Roberts, M.L.; Avgoustakis, K. In vivo investigation of tolerance and antitumor activity of cisplatin-loaded PLGA-mPEG nanoparticles. Eur. J. Pharm. Biopharm. 2009, 71, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Li, M.; Tang, Z.; Li, Q.; Yang, Y.; Liu, H.; Duan, T.; Hong, H.; Chen, X. Methoxypoly(ethylene glycol)-block-poly(L-glutamic acid)-loaded cisplatin and a combination with iRGD for the treatment of non-small-cell lung cancers. Macromol. Biosci. 2012, 12, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Plummer, R.; Wilson, R.; Calvert, H.; Boddy, A.; Griffin, M.; Sludden, J.; Tilby, M.; Eatock, M.; Pearson, D.; Ottley, C. A Phase I clinical study of cisplatinincorporated polymeric micelles (NC-6004) in patients with solid tumours. Br. J. Cancer 2011, 104, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, N.; Yokoyama, M.; Aoyagi, T.; Okano, T.; Sakurai, Y.; Kataoka, K. Preparation and characterization of self-assembled polymer-metal complex micelle from cis-dichlorodiammineplatinum (II) and poly (ethylene glycol)-poly (α, β-aspartic acid) block copolymer in an aqueous medium. Langmuir 1999, 15, 377–383. [Google Scholar] [CrossRef]
- Ye, H.; Jin, L.; Hu, R.; Yi, Z.; Li, J.; Wu, Y.; Xi, X.; Wu, Z. Poly (γ, l-glutamic acid)–cisplatin conjugate effectively inhibits human breast tumor xenografted in nude mice. Biomaterials 2006, 27, 5958–5965. [Google Scholar] [CrossRef]
- Feng, Z.; Lai, Y.; Ye, H.; Huang, J.; Xi, X.G.; Wu, Z. Poly (γ, L-glutamic acid)-cisplatin bioconjugate exhibits potent antitumor activity with low toxicity: A comparative study with clinically used platinum derivatives. Cancer Sci. 2010, 101, 2476–2482. [Google Scholar] [CrossRef]
- Kirkpatrick, G.J.; Plumb, J.A.; Sutcliffe, O.B.; Flint, D.J.; Wheate, N.J. Evaluation of anionic half generation 3.5–6.5 poly(amidoamine) dendrimers as delivery vehicles for the active component of the anticancer drug cisplatin. J. Inorg. Biochem. 2011, 105, 1115–1122. [Google Scholar] [CrossRef]
- Yellepeddi, V.K.; Kumar, A.; Maher, D.M.; Chauhan, S.C.; Vangara, K.K.; Palakurthi, S. Biotinylated PAMAM dendrimers for intracellular delivery of cisplatin to ovarian cancer: Role of SMVT. Anticancer Res. 2011, 31, 897–906. [Google Scholar]
- Mallick, A.; More, P.; Ghosh, S.; Chippalkatti, R.; Chopade, B.A.; Lahiri, M.; Basu, S. Dual drug conjugated nanoparticle for simultaneous targeting of mitochondria and nucleus in cancer cells. ACS Appl. Mater. Interf. 2015, 7, 7584–7598. [Google Scholar] [CrossRef]
- Iinuma, H.; Maruyama, K.; Okinaga, K.; Sasaki, K.; Sekine, T.; Ishida, O.; Ogiwara, N.; Johkura, K.; Yonemura, Y. Intracellular targeting therapy of cisplatin-encapsulated transferrin-polyethylene glycol liposome on peritoneal dissemination of gastric cancer. Int. J. Cancer 2002, 99, 130–137. [Google Scholar] [CrossRef]
- Krieger, M.L.; Eckstein, N.; Schneider, V.; Koch, M.; Royer, H.-D.; Jaehde, U.; Bendas, G. Overcoming cisplatin resistance of ovarian cancer cells by targeted liposomes in vitro. Int. J. Pharm. 2010, 389, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Burger, K.N.; Staffhorst, R.W.; de Vijlder, H.C.; Velinova, M.J.; Bomans, P.H.; Frederik, P.M.; de Kruijff, B. Nanocapsules: Lipid-coated aggregates of cisplatin with high cytotoxicity. Nat. Med. 2002, 8, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Hamelers, I.H.; De Kroon, A.I. Nanocapsules: A novel lipid formulation platform for platinum-based anticancer drugs. J. Liposome Res. 2007, 17, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Melanie, K.; Heike, Z.; Sibylle, B.S.; Hartmut, O.; Matthias, Z.; Christian, B.; Rudolf, H.; Karl-Jürgen, H.; Werner, A.K.; Ingrid, H. Characterization of iron oxide nanoparticles adsorbed with cisplatin for biomedical applications. Phys. Med. Biol. 2009, 54, 5109–5121. [Google Scholar]
- Comenge, J.; Romero, F.M.; Sotelo, C.; Domínguez, F.; Puntes, V. Exploring the binding of Pt drugs to gold nanoparticles for controlled passive release of cisplatin. J. Control. Release 2010, 148, e31–e32. [Google Scholar] [CrossRef]
- Craig, G.E.; Brown, S.D.; Lamprou, D.A.; Graham, D.; Wheate, N.J. Cisplatin-tethered gold nanoparticles that exhibit enhanced reproducibility, drug loading, and stability: A step closer to pharmaceutical approval? Inorg. Chem. 2012, 51, 3490–3497. [Google Scholar] [CrossRef]
- Min, Y.; Mao, C.-Q.; Chen, S.; Ma, G.; Wang, J.; Liu, Y. Combating the drug resistance of cisplatin using a platinum prodrug based delivery system. Angew. Chem. Int. Ed. 2012, 51, 6742–6747. [Google Scholar] [CrossRef]
- Lin, C.-H.; Cheng, S.-H.; Liao, W.-N.; Wei, P.-R.; Sung, P.-J.; Weng, C.-F.; Lee, C.-H. Mesoporous silica nanoparticles for the improved anticancer efficacy of cisplatin. Int. J. Pharm. 2012, 429, 138–147. [Google Scholar] [CrossRef]
- Gu, J.; Liu, J.; Li, Y.; Zhao, W.; Shi, J. One-pot synthesis of mesoporous silica nanocarriers with tunable particle sizes and pendent carboxylic groups for cisplatin delivery. Langmuir 2012, 29, 403–410. [Google Scholar] [CrossRef]
- Tao, Z.; Toms, B.; Goodisman, J.; Asefa, T. Mesoporous silica microparticles enhance the cytotoxicity of anticancer platinum drugs. ACS Nano 2010, 4, 789–794. [Google Scholar] [CrossRef]
- Vashist, S.K.; Zheng, D.; Pastorin, G.; Al-Rubeaan, K.; Luong, J.H.; Sheu, F.-S. Delivery of drugs and biomolecules using carbon nanotubes. Carbon 2011, 49, 4077–4097. [Google Scholar] [CrossRef]
- Li, J.; Yap, S.Q.; Yoong, S.L.; Nayak, T.R.; Chandra, G.W.; Ang, W.H.; Panczyk, T.; Ramaprabhu, S.; Vashist, S.K.; Sheu, F.S.; et al. Carbon nanotube bottles for incorporation, release and enhanced cytotoxic effect of cisplatin. Carbon 2012, 50, 1625–1634. [Google Scholar] [CrossRef]
- Guven, A.; Rusakova, I.A.; Lewis, M.T.; Wilson, L.J. Cisplatin@US-tube carbon nanocapsules for enhanced chemotherapeutic delivery. Biomaterials 2012, 33, 1455–1461. [Google Scholar] [CrossRef]
- Dhar, S.; Liu, Z.; Thomale, J.; Dai, H.; Lippard, S.J. Targeted single-wall carbon nanotube-mediated Pt(IV) prodrug delivery using folate as a homing device. J. Am. Chem. Soc. 2008, 130, 11467–11476. [Google Scholar] [CrossRef]
- Rieter, W.J.; Pott, K.M.; Taylor, K.M.L.; Lin, W. Nanoscale coordination polymers for platinum-based anticancer drug delivery. J. Am. Chem. Soc. 2008, 130, 11584–11585. [Google Scholar] [CrossRef]
- He, C.; Liu, D.; Lin, W. Self-assembled nanoscale coordination polymers carrying siRNAs and cisplatin for effective treatment of resistant ovarian cancer. Biomaterials 2015, 36, 124–133. [Google Scholar] [CrossRef]
- Adarsh, N.N.; Frias, C.; Ponnoth Lohidaksh, T.M.; Lorenzo, J.; Novio, F.; Garcia-Pardo, J.; Ruiz-Molina, D. Pt(IV)-based nanoscale coordination polymers: Antitumor activity, cellular uptake and interactions with nuclear DNA. Chem. Eng. J. 2018, 340, 94–102. [Google Scholar] [CrossRef]
- He, C.; Liu, D.; Lin, W. Self-assembled core-shell nanoparticles for combined chemotherapy and photodynamic therapy of resistant head and neck cancers. ACS Nano 2015, 9, 991–1003. [Google Scholar] [CrossRef]
- Makharza, S.A.; Cirillo, G.; Vittorio, O.; Valli, E.; Voli, F.; Farfalla, A.; Curcio, M.; Iemma, F.; Nicoletta, F.P.; El-Gendy, A.A.; et al. Magnetic Graphene Oxide Nanocarrier for Targeted Delivery of Cisplatin: A Perspective for Glioblastoma Treatment. Pharmaceuticals 2019, 12, 76. [Google Scholar] [CrossRef]
- Coluccia, D.; Figueiredo, C.A.; YiJun Wu, M.; Riemenschneider, A.N.; Diaz, R.; Luck, A.; Smith, C.; Das, S.; Ackerley, C.; O’Reilly, M.; et al. Enhancing glioblastoma treatment using cisplatin-gold-nanoparticle conjugates and targeted delivery with magnetic resonance-guided focused ultrasound. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 1137–1148. [Google Scholar] [CrossRef]
- Gotov, O.; Battogtokh, G.; Shin, D.; Ko, J.T. Hyaluronic acid-coated cisplatin conjugated gold nanoparticles for combined cancer treatment. J. Ind. Eng. Chem. 2018, 65, 236–243. [Google Scholar] [CrossRef]
- Kosmas, C.; Angel, J.; Athanasiou, A.; Rapti, A.; Karanikas, C.; Lambaki, S.; Politis, N.; Mylonakis, N. 9088 Phase III study of Lipoplatin plus Gemcitabine versus Cisplatin plus Gemcitabine in advanced NSCLC; interim analysis. Eur. J. Cancer Suppl. 2009, 7, 531. [Google Scholar] [CrossRef]
- Farhat, F.; Kattan, J.; Ibrahim, K.; Bitar, N.; Haddad, N.; Tamraz, S.; Hatoum, H.; Shamseddine, A. 457 Preliminary results of a phase II study of lipoplatin (liposomal cisplatin)–vinorelbine combination as first line treatment in HER2/neu negative metastatic breast cancer (MBC). Eur. J. Cancer Suppl. 2010, 8, 192. [Google Scholar] [CrossRef]
- Koukourakis, M.I.; Giatromanolaki, A.; Pitiakoudis, M.; Kouklakis, G.; Tsoutsou, P.; Abatzoglou, I.; Panteliadou, M.; Sismanidou, K.; Sivridis, E.; Boulikas, T. Concurrent liposomal cisplatin (Lipoplatin), 5-fluorouracil and radiotherapy for the treatment of locally advanced gastric cancer: A phase I/II study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 150–155. [Google Scholar] [CrossRef]
- Huo, T.; Barth, R.F.; Yang, W.; Nakkula, R.J.; Koynova, R.; Tenchov, B.; Chaudhury, A.R.; Agius, L.; Boulikas, T.; Elleaume, H.; et al. Preparation, Biodistribution and Neurotoxicity of Liposomal Cisplatin following Convection Enhanced Delivery in Normal and F98 Glioma Bearing Rats. PLoS ONE 2012, 7, e48752. [Google Scholar] [CrossRef]
- Gonda, A.; Zhao, N.; Shah, J.V.; Calvelli, H.R.; Kantamneni, H.; Francis, N.L.; Ganapathy, V. Engineering Tumor-Targeting Nanoparticles as Vehicles for Precision Nanomedicine. Med. One 2019, 4, e190021. [Google Scholar]
- Shein, S.A.; Kuznetsov, I.I.; Abakumova, T.O.; Chelushkin, P.S.; Melnikov, P.A.; Korchagina, A.A.; Bychkov, D.A.; Seregina, I.F.; Bolshov, M.A.; Kabanov, A.V.; et al. VEGF- and VEGFR2-Targeted Liposomes for Cisplatin Delivery to Glioma Cells. Mol. Pharm. 2016, 13, 3712–3723. [Google Scholar] [CrossRef]
- Ashrafzadeh, M.S.; Akbarzadeh, A.; Heydarinasab, A.; Ardjmand, M. In vivo Glioblastoma Therapy Using Targeted Liposomal Cisplatin. Int. J. Nanomed. 2020, 15, 7035–7049. [Google Scholar] [CrossRef]
- Dhami, N.K.; Pandey, R.S.; Jain, U.K.; Chandra, R.; Madan, J. Non-Aggregated Protamine-Coated Poly(Lactide-Co-Glycolide) Nanoparticles of Cisplatin Crossed Blood-Brain Barrier, Enhanced Drug Delivery and Improved Therapeutic Index in Glioblastoma Cells: In Vitro Studies. J. Microencapsul. 2014, 31, 685–693. [Google Scholar] [CrossRef]
- Marrache, S.; Pathak, R.K.; Dhar, S. Detouring of cisplatin to access mitochondrial genome for overcoming resistance. Proc. Natl. Acad. Sci. USA 2014, 111, 10444–10449. [Google Scholar] [CrossRef]
- Nance, E.A.; Woodworth, G.F.; Sailor, K.A.; Shih, T.Y.; Xu, Q.; Swaminathan, G.; Xiang, D.; Eberhart, C.; Hanes, J. A dense poly(ethylene glycol) coating improves penetration of large polymeric nanoparticles within brain tissue. Sci. Transl. Med. 2012, 4, 149ra119. [Google Scholar] [CrossRef]
- Ebrahimi Shahmabadi, H.; Movahedi, F.; Koohi Moftakhari Esfahani, M.; Alavi, S.E.; Eslamifar, A.; Mohammadi Anaraki, G.; Akbarzadeh, A. Efficacy of Cisplatin-Loaded Polybutyl Cyanoacrylate Nanoparticles on the Glioblastoma. Tumour Biol. 2014, 35, 4799–4806. [Google Scholar] [CrossRef]
- Zhang, C.; Nance, E.A.; Mastorakos, P.; Chisholma, J.; Eberhart, S.B.C.; Tyler, B.; Brem, H.; Suk, J.S.; Hanes, J. Convection enhanced delivery of cisplatin-loaded brain penetrating nanoparticles cures malignant glioma in rats. J. Control. Release 2017, 263, 112–119. [Google Scholar] [CrossRef]
- Lajous, H.; Riva, R.; Lelievre, B.; Tetaud, C.; Avril, S.; Hindre, F.; Boury, F.; Jerome, C.; Lecomte, P.; Garcion, E. Hybrid Gd3+/Cisplatin Cross-Linked Polymer Nanoparticles Enhance Platinum Accumulation and Formation of DNA Adducts in Glioblastoma Cell Lines. Biomater. Sci. 2018, 6, 2386–2409. [Google Scholar] [CrossRef]
- Nukolova, N.V.; Baklaushev, V.P.; Abakumova, T.O.; Mel’nikov, P.A.; Abakumov, M.A.; Yusubalieva, G.M.; Bychkov, D.A.; Kabanov, A.V.; Chekhonin, V.P. Targeted delivery of cisplatin by connexin 43 vector nanogels to the focus of experimental glioma C6. Bull Exp. Biol. Med. 2014, 157, 524–529. [Google Scholar] [CrossRef]
- Renault-Mahieux, M.; Vieillard, V.; Seguin, J.; Espeau, P.; Le, D.T.; Lai-Kuen, R.; Mignet, R.; Paul, M.; Andrieux, K. Co-Encapsulation of Fisetin and Cisplatin into Liposomes for Glioma Therapy: From Formulation to Cell Evaluation. Pharmaceutics 2021, 13, 970. [Google Scholar] [CrossRef]
- Zou, Y.; Wang, Y.; Xu, S.; Liu, Y.; Yin, J.; Lovejoy, D.B.; Zheng, M.; Liang, X.-J.; Park, J.B.; Efremov, Y.M.; et al. Brain Co-Delivery of Temozolomide and Cisplatin for Combinatorial Glioblastoma Chemotherapy. Adv. Mater. 2022, 34, 2203958. [Google Scholar] [CrossRef]
- Straehla, J.P.; Hajal, C.; Safford, H.C.; Offeddu, G.S.; Boehnke, N.; Dacoba, T.C.; Wyckoff, J.; Kamm, R.D.; Hammond, P.T. A predictive microfluidic model of human glioblastoma to assess trafficking of blood-brain barrier penetrant nanoparticles. Proc. Natl. Acad. Sci. USA 2022, 119, e2118697119. [Google Scholar] [CrossRef]
- Yu, H.; Tang, Z.; Zhang, D.; Song, W.; Zhang, Y.; Yang, Y.; Ahmad, Z.; Chen, X. Pharmacokinetics, biodistribution and in vivo efficacy of cisplatin loaded poly(L-glutamic acid)-g-methoxy poly(ethylene glycol) complex nanoparticles for tumor therapy. J. Control Release 2015, 205, 89–97. [Google Scholar] [CrossRef]
- Ho, G.Y.; Woodward, N.; Coward, J.I.G. Cisplatin versus carboplatin: Comparative review of therapeuticmanagement in solid malignancies. Crit. Rev. Oncol./Hematol. 2016, 102, 37–46. [Google Scholar] [CrossRef]
- Colombo, N.; Guthrie, D.; Chiari, S.; Parmar, M.; Qian, W.; Swart, A.M.; Torri, V.; Williams, C.; Lissoni, A.; Bonazzi, C. International Collaborative Ovarian Neoplasm trial 1: A randomized trial of adjuvant chemotherapy in women with early-stage ovarian cancer. J. Natl. Cancer Inst. 2003, 95, 125–132. [Google Scholar] [PubMed]
- Rezaee, M.; Hunting, D.J.; Sanche, L. New insights into the mechanism underlying the synergistic action of ionizing radiation with platinum chemotherapeutic drugs: The role of low-energy electrons. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Gianasi, E.; Buckley, R.G.; Latigo, J.; Wasil, M.; Duncan, R. HPMA copolymers platinates containing dicarboxylato ligands. Preparation, characterisation and in vitro and in vivo evaluation. J. Drug Target. 2002, 10, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Gianasi, E.; Wasil, M.; Evagorou, E.; Keddle, A.; Wilson, G.; Duncan, R. HPMA copolymer platinates as novel antitumour agents: In vitro properties, pharmacokinetics and antitumour activity in vivo. Eur. J. Cancer. 1999, 35, 994–1002. [Google Scholar] [CrossRef]
- Rademaker-Lakhai, J.M.; Terret, C.; Howell, S.B.; Baud, C.M.; de Boer, R.F.; Pluim, D.; Beijnen, J.H.; Schellens, J.H.; Droz, J.-P. A Phase I and pharmacological study of the platinum polymer AP5280 given as an intravenous infusion once every 3 weeks in patients with solid tumors. Clin. Cancer Res. 2004, 10, 3386–3395. [Google Scholar] [CrossRef]
- Karanam, V.; Marslin, G.; Krishnamoorthy, B.; Chellan, V.; Siram, K.; Natarajan, T.; Bhaskar, B.; Franklin, G. Poly (ε -caprolactone) nanoparticles of carboplatin: Preparation, characterization and in vitro cytotoxicity evaluation in U-87 MG cell lines. Colloids Surf B Biointerfaces 2015, 130, 48–52. [Google Scholar] [CrossRef]
- Hassanzadeganroudsari, M.; Soltani, M.; Heydarinasab, A.; Apostolopoulos, V.; Akbarzadehkhiyavi, A.; Nurgali, K. Targeted nano-drug delivery system for glioblastoma therapy: In vitro and in vivo study. J. Drug Deliv. Sci. Technol. 2020, 60, 102039. [Google Scholar] [CrossRef]
- Arshad, A.; Yang, B.; Bienemann, A.S.; Barua, N.U.; Wyatt, M.J.; Woolley, M.; Johnson, D.E.; Edler, K.J.; Gill, S.S. Convection-enhanced delivery of carboplatin PLGA nanoparticles for the treatment of glioblastoma. PLoS ONE 2015, 10, e0132266. [Google Scholar] [CrossRef]
- Shi, M.; Anantha, M.; Wehbe, M.; Bally, M.B.; Fortin, D.; Roy, L.-O.; Charest, G.; Richer, M.; Paquette, B.; Sanche, L. Liposomal formulations of carboplatin injected by convection-enhanced delivery increases the median survival time of F98 glioma bearing rats. J. Nanobiotechnol. 2018, 16, 77. [Google Scholar] [CrossRef]
- Alex, A.T.; Joseph, A.; Shavi, G.; Rao, J.V.; Udupa, N. Development and evaluation of carboplatin-loaded PCL nanoparticles for intranasal delivery. Drug Deliv. 2016, 23, 2144–2153. [Google Scholar] [CrossRef]
- Fortin, D.; Desjardins, A.; Benko, A.; Niyonsega, T.; Boudrias, M. Enhanced chemotherapy delivery by intraarterial infusion and blood-brain barrier disruption in malignant brain tumors: The sherbrooke experience. Cancer 2005, 103, 2606–2615. [Google Scholar] [CrossRef] [PubMed]
- Miura, Y.; Takenaka, T.; Toh, K.; Wu, S.; Nishihara, H.; Kano, M.R.; Ino, Y.; Nomoto, T.; Matsumoto, Y.; Koyama, H.; et al. Cyclic Rgd-Linked Polymeric Micelles for Targeted Delivery of Platinum Anticancer Drugs to Glioblastoma through the Blood-Brain Tumor Barrier. ACS Nano 2013, 7, 8583–8592. [Google Scholar] [CrossRef]
- Shi, M.; Fortin, D.; Paquette, B.; Sanche, L. Convection-enhancement delivery of liposomal formulation of oxaliplatin shows less toxicity than oxaliplatin yet maintains a similar median survival time in F98 glioma-bearing rat model. Investig. New Drugs. 2016, 34, 269–276. [Google Scholar] [CrossRef]
- You, Y.; Wang, N.; He, l.; Shi, C.; Zhang, D.; Liu, Y.; Luo, L.; Che, T. Designing dual-functionalized carbon nanotubes with high blood–brain-barrier permeability for precise orthotopic glioma therapy. Dalton Trans. 2019, 48, 1569–1573. [Google Scholar] [CrossRef] [PubMed]
- McCartin, C.; Dussouillez, C.; Bernhard, C.; Mathieu, E.; Blumberger, J.; Dontenwill, M.; Herold-Mende, C.; Idbaih, A.; Lavalle, P.; Bellemin-Laponnaz, S.; et al. Polyethylenimine, an Autophagy-Inducing Platinum-Carbene-Based Drug Carrier with Potent Toxicity towards Glioblastoma Cancer Stem Cells. Cancers 2022, 14, 5057. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Denga, Z.; Zhu, G. Emerging platinum(IV) prodrugs to combat cisplatin resistance: From isolated cancer cells to tumor microenvironment. Dalton Trans. 2019, 48, 2536–2544. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, Y.; Wei, D.; Singh, P.; Yu, Y.; Lee, T.; Zhang, L.; Mandl, H.K.; Piotrowski-Daspit, A.S.; Chen, X.; et al. Nanoparticle-mediated convection-enhanced delivery of a DNA intercalator to gliomas circumvents temozolomide resistance. Nat. Biomed. Eng. 2021, 5, 1048–1058. [Google Scholar] [CrossRef]
- Arduino, I.; Depalo, N.; Re, F.; Dal Magro, R.; Panniello, A.; Margiotta, N.; Fanizza, E.; Lopalco, A.; Laquintana, V.; Cutrignelli, A.; et al. PEGylated solid lipid nanoparticles for brain delivery of lipophilic kiteplatin Pt(IV) prodrugs: An in vitro study. Int. J. Pharm. 2020, 583, 119351. [Google Scholar] [CrossRef]
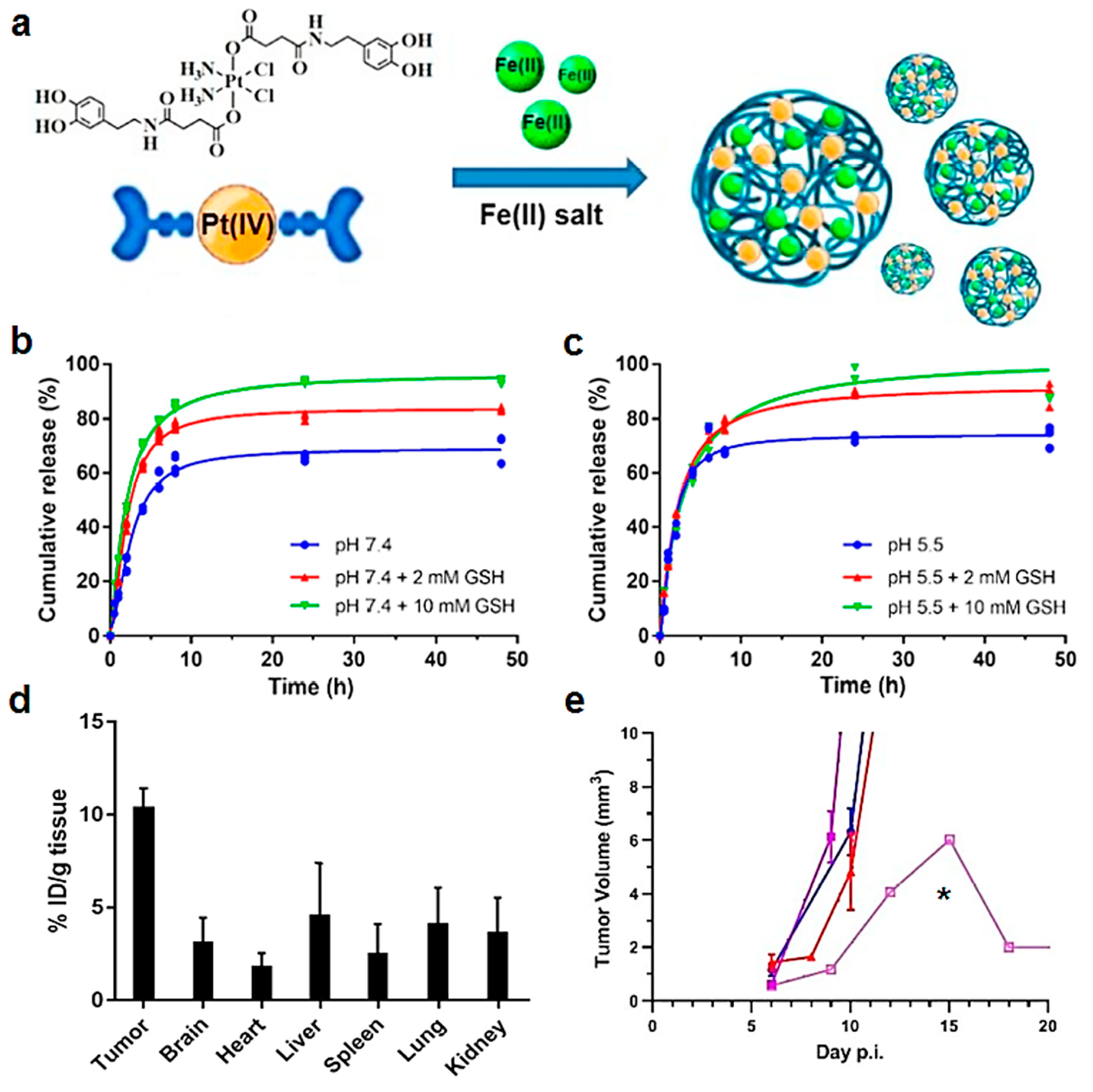
- Mao, X.; Wu, S.; Calero-Pérez, P.; Candiota, A.P.; Alfonso, P.; Bruna, J.; Yuste, V.J.; Lorenzo, J.; Novio, F.; Ruiz-Molina, D. Synthesis and Validation of a Bioinspired Catechol-Functionalized Pt(IV) Prodrug for Preclinical Intranasal Glioblastoma Treatment. Cancers 2022, 14, 410. [Google Scholar] [CrossRef]
- Kutwin, M.; Sawosz, E.; Jaworski, S.; Hinzmann, M.; Wierzbicki, M.; Hotowy, A.; Grodzik, M.; Winnicka, A.; Chwalibog, A. Investigation of Platinum Nanoparticle Properties against U87 Glioblastoma Multiforme. Arch. Med. Sci. 2017, 13, 1322–1334. [Google Scholar] [CrossRef]
- Lopez Ruiz, A.; Bartomeu Garcia, C.; Navarro Gallon, S.; Webster, T.J. Novel Silver-Platinum Nanoparticles for Anticancer and Antimicrobial Applications. Int. J. Nanomed. 2020, 15, 169–179. [Google Scholar] [CrossRef]
- Shi, M.; Fortin, D.; Sanche, L.; Paquette, B. Convection-Enhancement Delivery of Platinum-Based Drugs and Lipoplatintm to Optimize the Concomitant Effect with Radiotherapy in F98 Glioma Rat Model. Investig. New Drugs 2015, 33, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Setua, S.; Ouberai, M.; Piccirillo, S.G.; Watts, C.; Welland, M. Cisplatin-Tethered Gold Nanospheres for Multimodal Chemo-Radiotherapy of Glioblastoma. Nanoscale 2014, 6, 10865–10873. [Google Scholar] [CrossRef] [PubMed]
- Hall, P.E.; Lewis, R.; Syed, N.; Shaffer, R.; Evanson, J.; Ellis, S.; Williams, M.; Feng, X.; Johnston, A.; Thomson, J.A. A phase I study of Pegylated arginine deiminase (Pegargiminase), cisplatin, and Pemetrexed in Argininosuccinate Synthetase 1-deficient recurrent high-grade glioma. Clin. Cancer Res. 2019, 25, 2708–2716. [Google Scholar] [CrossRef]
- Allen, J.; Siffert, J.; Donahue, B.; Nirenberg, A.; Jakacki, R.; Robertson, P.; DaRosso, R.; Thoron, L.; Rosovsky, M.; Pinto, R. A phase I/II study of carboplatin combined with hyperfractionated radiotherapy for brainstem gliomas. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1999, 86, 1064–1069. [Google Scholar] [CrossRef]
- Fouladi, M.; Blaney, S.M.; Poussaint, T.Y.; Freeman III, B.B.; McLendon, R.; Fuller, C.; Adesina, A.M.; Hancock, M.L.; Danks, M.K.; Stewart, C. Phase II study of oxaliplatin in children with recurrent or refractory medulloblastoma, supratentorial primitive neuroectodermal tumors, and atypical teratoid rhabdoid tumors: A pediatric brain tumor consortium study. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2006, 107, 2291–2297. [Google Scholar] [CrossRef]
- Macy, M.E.; Duncan, T.; Whitlock, J.; Hunger, S.P.; Boklan, J.; Narendran, A.; Herzog, C.; Arceci, R.J.; Bagatell, R.; Trippett, T. A multi-center phase Ib study of oxaliplatin (NSC# 266046) in combination with fluorouracil and leucovorin in pediatric patients with advanced solid tumors. Pediatr. Blood Cancer 2013, 60, 230–236. [Google Scholar] [PubMed]
- Chintala, S.; Ali-Osman, F.; Mohanam, S.; Rayford, A.; Go, Y.; Gokaslan, Z.L.; Gagercas, E.; Vekaiah, B.; Sawaya, R.; Nicolson, G.; et al. Effect of cisplatin and BCNU on MMP-2 levels in human glioblastoma cell lines in vitro. Clin. Exp. Metastasis 1997, 14, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Rébé, C.; Demontoux, L.; Pilot, T.; Ghiringhelli, F. Platinum Derivatives Effects on Anticancer Immune Response. Biomolecules 2020, 10, 13. [Google Scholar] [CrossRef]
- Nduom, E.K.; Weller, M.; Heimberger, A.B. Immunosuppressive mechanisms in glioblastoma. Neuro Oncol. 2015, 17, vii9–vii14. [Google Scholar] [CrossRef]
- Hato, S.V.; Khong, A.; de Vries, I.J.; Lesterhuis, W.J. Molecular pathways: The immunogenic effects of platinum-based chemotherapeutics. Clin. Cancer Res. 2014, 20, 2831–2837. [Google Scholar] [CrossRef] [PubMed]
- Lesterhuis, W.J.; Punt, C.J.; Hato, S.V.; Eleveld-Trancikova, D.; Jansen, B.J.; Nierkens, S.; Schreibelt, G.; de Boer, A.; Van Herpen, C.M.; Kaanders, J.H.; et al. Platinum-based drugs disrupt STAT6-mediated suppression of immune responses against cancer in humans and mice. J. Clin. Investig. 2011, 121, 3100–3108. [Google Scholar] [CrossRef]
- Bezu, L.; Gomes-de-Silva, L.C.; Dewitte, H.; Breckpot, K.; Fucikova, J.; Spisek, R.; Galluzzi, L.; Kepp, O.; Kroemer, G. Combinatorial strategies for the induction of immunogenic cell death. Front. Immunol. 2015, 6, 187. [Google Scholar] [CrossRef]
- Kang, L.; Gao, Z.; Huang, W.; Jin, M.; Wang, Q. Nanocarrier-mediated codelivery of chemotherapeutic drugs and gene agents for cancer treatment. Acta Pharm. Sin. B 2015, 5, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Field, K.M.; Simes, J.; Nowak, A.K.; Cher, L.; Wheeler, H.; Hovey, E.J.; Brown, C.S.; Barnes, E.H.; Sawkins, K.; Livingstone, A.; et al. Randomized phase 2 study of carboplatin and bevacizumab in recurrent glioblastoma. Neuro Oncol. 2015, 17, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Bruinsmann, F.A.; Richter Vaz, G.; de Cristo Soares Alves, A.; Aguirre, T.; Raffin Pohlmann, A.; Stanisçuaski Guterres, S.; Sonvico, F. Nasal Drug Delivery of Anticancer Drugs for the Treatment of Glioblastoma: Preclinical and Clinical Trials. Molecules 2019, 24, 4312. [Google Scholar] [CrossRef]
- Sandbhor, P.; Goda, J.; Mohanty, B.; Gera, P.; Yadav, S.; Chekuri, G.; Chaudhari, P.; Dutt, S.; Banerjee, R. Targeted nano-delivery of chemotherapy via intranasal route suppresses in vivo glioblastoma growth and prolongs survival in the intracranial mouse model. Drug Deliv. Transl. 2023, 13, 608–626. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfonso-Triguero, P.; Lorenzo, J.; Candiota, A.P.; Arús, C.; Ruiz-Molina, D.; Novio, F. Platinum-Based Nanoformulations for Glioblastoma Treatment: The Resurgence of Platinum Drugs? Nanomaterials 2023, 13, 1619. https://0-doi-org.brum.beds.ac.uk/10.3390/nano13101619
Alfonso-Triguero P, Lorenzo J, Candiota AP, Arús C, Ruiz-Molina D, Novio F. Platinum-Based Nanoformulations for Glioblastoma Treatment: The Resurgence of Platinum Drugs? Nanomaterials. 2023; 13(10):1619. https://0-doi-org.brum.beds.ac.uk/10.3390/nano13101619
Chicago/Turabian StyleAlfonso-Triguero, Paula, Julia Lorenzo, Ana Paula Candiota, Carles Arús, Daniel Ruiz-Molina, and Fernando Novio. 2023. "Platinum-Based Nanoformulations for Glioblastoma Treatment: The Resurgence of Platinum Drugs?" Nanomaterials 13, no. 10: 1619. https://0-doi-org.brum.beds.ac.uk/10.3390/nano13101619